
Abstract
Background:
Concomitant cerebrovascular diseases (CeVD) have been identified as an important determinant of Alzheimer’s disease (AD) progression. Development of robust blood-based biomarkers will provide critical tools to evaluate prognosis and potential interventional strategies for AD with CeVD.
Objective:
This study investigated circulating placental growth factor (PlGF), a potent pro-angiogenic factor related to endothelial dysfunction and vascular inflammation, in an Asian memory clinic cohort of non-demented individuals as well as AD, including its associations with neuroimaging markers of CeVD.
Methods:
109 patients with AD, 76 cognitively impaired with no dementia (CIND), and 56 non-cognitively impaired (NCI) were included in this cross-sectional study. All subjects underwent 3T brain magnetic resonance imaging to assess white matter hyperintensities (WMH), lacunes, cortical infarcts, and cerebral microbleeds (CMBs). Serum PlGF concentrations were measured by electrochemiluminescence immunoassays.
Results:
Serum PlGF was elevated in AD, but not CIND, compared to the NCI controls. Adjusted concentrations of PlGF were associated with AD only in the presence of significant CeVD. Elevated PlGF was significantly associated with higher burden of WMH and with CMBs in AD patients.
Conclusions:
Serum PlGF has potential utility as a biomarker for the presence of CeVD, specifically WMH and CMBs, in AD. Further studies are needed to elucidate the underlying pathophysiological mechanisms linking PlGF to CeVD, as well as to further assess PlGF’s clinical utility.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the most common type of neurodegenerative dementia affecting the elderly population and constitutes a significant socioeconomic and healthcare burden worldwide [1]. While the underlying causes of AD remain incompletely understood, it is widely believed to be associated with neurodegenerative processes involving dysregulated neuroinflammation together with accumulation of amyloid plaques and neurofibrillary tangles [2, 3]. Moreover, recent evidence from epidemiological, clinical, and experimental studies has highlighted the role of cerebrovascular disease (CeVD) in contributing to cognitive deficits [4], and has revealed a considerable overlap between CeVD and AD [5–7], suggesting that the two conditions may be intimately connected at a pathophysiological level. Apart from direct contribution to vascular dementia and related conditions within the spectrum of vascular cognitive impairment (VCI), CeVD is also found concomitantly in approximately 50% of clinically diagnosed AD patients, and as high as 75% in post-mortem AD studies [8]. The accumulation of CeVD in AD can have a profound impact on disease progression and severity, resulting in poorer prognosis due to additive or synergistic effects of AD and concurrent microvascular lesions [9–11]. As such, early, accessible detection of CeVD is essential for prognosis and potential treatment. Recent advances in the performance of detection platforms have made blood-based biomarkers an increasingly feasible approach [12]. However, the complex clinical presentation of AD with CeVD, compounded by variability in CeVD severity and subtypes as well as the overlap of cognitive phenotypes, poses a significant challenge in its diagnosis and characterization [7]. Therefore, there is an unmet need for identifying reliable biomarkers to assess the burden of CeVD in AD. While we have reported several inflammation or vascular disease-associated markers with potential clinical utility [13–17], the complex nature of CeVD pathogenesis imply involvement of a wide range of biomolecules, thus supporting continued efforts into uncovering novel biomarkers.
Placental growth factor (PlGF), which belongs to the vascular endothelial growth factor family, plays a crucial role in regulating endothelial signaling and vascular function [18]. It is predominantly produced by activated endothelial cells in response to vascular damage and is intrinsic to initiation of angiogenic/repair processes [19]. Studies have reported that PlGF promotes neurogenesis and angiogenesis, which are essential processes for repairing damaged tissue and restoring vascular integrity following ischemic injury [20–23]. Conversely, PlGF deficiency in mice leads to severe defects in brain vascularization which result in compromised cerebral blood flow and brain function [24]. While the multiple functions of PlGF in the brain are still being actively studied, an increasing body of evidence indicates its potential involvement in CeVD and related disorders. For instance, elevated levels of PlGF in the cerebrospinal fluid (CSF) of individuals with Parkinson’s disease were associated with a higher CSF/plasma albumin ratio, increased white matter hyperintensities (WMH) burden, and the presence of cerebral microbleeds (CMBs) [25]. Increased PlGF levels in the CSF were also found to be associated with WMH in non-dementia subjects [26]. Additionally, an important recent study has found that plasma PlGF levels were elevated in patients with WMH-associated cognitive impairment and were linked to poorer executive function and memory performance [27]. In this context, circulating PlGF has been proposed as a promising biomarker for VCI [27, 28]. However, there is at present no study examining peripheral blood PlGF levels in AD, either with or without concomitant CeVD. In this context, we measured serum PlGF in a cohort of participants with cognitive impairment or AD dementia who underwent neuroimaging assessments for CeVD and investigated associations between serum PlGF levels and magnetic resonance imaging (MRI) markers of four specific CeVD subtypes: cortical infarcts, WMH, lacunes, and CMBs.
METHODS
Study population
This cross-sectional pilot study consisted of participants who attended memory clinics at the National University Hospital and St. Luke’s Hospital in Singapore between August 2010 to February 2020. The selection and assessment of subjects for this retrospective case-control study have previously been described [29]. Briefly, important demographic and medical characteristics, as well as exclusion factors (such as previous head trauma, psychiatric illnesses, thyroid disease, and non-dementia neurodegenerative conditions), were collected through detailed questionnaires and reviews of medical records. The inclusion criteria of this study were as follows: 1) patients diagnosed as no cognitive impairment (NCI), cognitive impairment no dementia (CIND), or AD, 2) had gradable MRI scans, and 3) sufficient serum samples for PlGF measurement. The demographic and disease profiles of the 241 subjects included in the analysis were presented in Table 1, demonstrating a resemblance to the population from which they were drawn [16]. Patient diagnoses were discussed and confirmed at weekly consensus meetings during which detailed clinical features, neuropsychological testing and brain imaging were reviewed by study clinicians and neuropsychologists. NCI was defined as those who had no objective cognitive impairment on formal neuropsychological test battery or functional loss. Details of the component tests used for the six cognitive domains assessed are listed in Supplementary Table 1. CIND was defined as impairment in at least one domain of the neuropsychological test (that is, scored 1.5 SDs below the established education-adjusted cut-off values on any test) but did not meet the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSMIV) criteria for dementia. Diagnosis of AD follows the criteria of the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) [30].
Demographic and disease characteristics of the study cohort (n = 241)
CIND, cognitive impairment no dementia; CeVD, cerebrovascular disease; NCI, no cognitive impairment; no., number of cases; SD, standard deviation; IQR, interquartile range; CMB, cerebral microbleed; ARWMC, age-related white matter changes. Hypertension was missing for 1 CIND patients; Complete neuroimaging data were available for 228 subjects. ¶Significant CeVD burden are defined by cortical infarct count≥1, and/or ARWMC score≥8, and/or lacune count≥2, and/or cerebral microbleed count≥2, as previously described [36].
All subjects underwent standard physical, clinical, blood tests, and neuropsychological assessments as well as neuroimaging scans at the National University of Singapore. The study received ethics approval from National Healthcare Group Domain-Specific Review Board (reference 2010/00017; study protocol DEM4233) and was conducted in compliance with the guidelines in the Declaration of Helsinki. Written informed consent was obtained from all participants or their next-of-kin, in their preferred language, prior to enrolment.
Demographics and risk factors assessments
A detailed questionnaire was administered to all participants to collect information on age, sex, race, and educational level. Education status was categorized as low (not exceeding primary school education) or high (beyond primary school education). Physical examination included height, weight, and blood pressure. Risk factors, such as hypertension, hyperlipidemia, diabetes mellitus, and cardiovascular diseases were ascertained from clinical interview and medical records and classified as present or absent, as previously described [16] (see Supplementary Material: Risk factors assessments for details). Apolipoprotein E (APOE) genotyping was performed as described previously [31], and APOE ɛ4 carrier status was defined as having at least one ɛ4 allele.
Neuroimaging
MRI scans were performed on a 3-Tesla Siemens Magnetom Trio Tim scanner, using a 32-channel head coil, at the Clinical Imaging Research Centre, National University of Singapore. Subjects with claustrophobia, contraindications for MRI, or those who were unable to tolerate the procedure were excluded. All MRIs were graded by one radiologist and two clinicians blinded to the neuropsychological and clinical data, with good-to-excellent intra- and inter-rater reliability [32]. The sequences included T1-weighted Magnetization Prepared Rapid Gradient Recalled Echo, Fluid Attenuated Inversion Recovery, T2-weighted, and Susceptibility Weighted Imaging sequences. MRI markers of CeVD were defined based on the Standards for Reporting Vascular Changes on Neuroimaging (STRIVE) criteria [33]: 1) Cortical infarcts were defined as hypodense lesions interrupting the cortex grey/white junction. 2) Lacunes were defined by the presence of hypodense focal lesions measuring≥3 mm and < 15 mm. 3) WMH were defined as lesions which were hyperintense on T2 and FLAIR sequences and hypointense on T1 weighted images and were graded using the Age-Related White Matter Changes (ARWMC) scale [34]. 4) CMBs were defined as focal, punctate areas (2 to 10 mm in diameter) associated with blooming on Susceptibility weighted images and were graded according to the Microbleed Anatomical Rating Scale [35]. Diagnoses of NCI, CIND, and AD were divided into presence of significant CeVD, defined according to our previously reported operationalized criteria, which take into account the presence of cortical infarcts, and/or≥2 lacunes, and/or≥2 CMBs, and/or confluent WMH in two regions of the brain (ARWMC score≥8) [14, 36].
Serum PLGF measurements
Non-fasting blood samples were drawn from study participants into serum-separating tubes and processed by centrifugation at 2000×g for 10 min at 4°C, after which aliquots of serum were mixed well and stored at –80°C until use. The PlGF concentrations were measured by electrochemiluminescence immunoassays using the Elecsys PlGF assay on an automated Cobas e411 analyzer (Roche Diagnostics GmbH, Vienna, Austria) according to the manufacturer’s instructions. The minimal detectable dose in the assay for serum PlGF was 3 pg/ml; the intra-assay and inter-assay coefficients of variation were 0.7–1.0% and 2.7–4.1%, respectively.
Statistical analyses
Statistical analyses were performed using software IBM SPSS Statistics (version 26, IBM Corp., Armonk, NY, USA) and R (version 4.1.1, The R Foundation). One-way analyses of variance (ANOVA) with Bonferroni post hoc tests, Kruskal–Wallis test with Dunn’s post hoc tests and Chi-square tests were used to detect group differences for normally distributed continuous variables (age), skewed continuous variables (educational year and PlGF), and binary variables (gender, APOE4 status, education level, hypertension, hyperlipidemia, diabetes mellitus, cardiovascular diseases and MRI markers of CeVD), respectively. Binary logistic regression models were constructed with odds ratios (OR) and 95% confidence intervals (CI) to determine the association between blood biomarkers with subtypes of CIND and AD dementia stratified by significant CeVD defined by MRI (Table 2). Models were first assessed unadjusted (Model 1) with subsequent adjustment for age, gender, and cardiovascular disease (Model 2). To examine the relationship between PlGF and CeVD subtypes, negative binomial regression models with rate ratios (RR) and 95% CI were constructed for the count of CMBs; linear regression models with mean differences (β) and 95% CI were used for the ARWMC visual scores (Table 3). Here the models were unadjusted (Model 1); adjusted for covariates including age, gender, and cardiovascular diseases (Model 2) and lastly, additionally adjusted for relative CeVD markers (Model 3). All regression analyses were conducted without applying multiple comparison correction, and a significance level of p < 0.05 was considered statistically significant.
Associations with serum PlGF and concomitant CeVD in cognitive impairment and dementia
Model 1: unadjusted. Model 2: adjusted for age, gender, diabetes mellitus, and cardiovascular diseases. Absence and presence of significant cerebrovascular disease indicated as “CeVD-” and “CeVD+” respectively.
Associations of serum PlGF with WMH and CMBs
ARWMC, age-related white matter changes; β, mean difference; CI, confidence interval; MRI, magnetic resonance imaging; WMH, white matter hyperintensities; RR, rate ratio. Model 1: unadjusted. Model 2: adjusted for age, gender, diabetes mellitus, and cardiovascular diseases. Model 3: further adjusted for †CMBs or
RESULTS
Group description
Table 1 presents the demographic and clinical characteristics of the study cohort. Among the 241 participants, 56 (23.2%) were NCI, 76 (31.5%) were CIND and 109 (45.2%) had AD. The groups differed significantly in age, gender distribution, years of education, and the prevalence of diabetes mellitus (Table 1). Post hoc analyses revealed that age was significantly higher in the CIND and AD groups compared to NCI (p < 0.001 for both). Additionally, the AD group showed a higher female to male ratio than CIND (p = 0.002), and their education level was significantly lower compared to both NCI and CIND (p < 0.001 for both). Moreover, the prevalence of diabetes mellitus was significantly higher in the CIND and AD groups compared to NCI (p = 0.011 and p < 0.001, respectively). However, among the groups, there were no significant differences observed in APOE ɛ4 carrier frequency and the prevalence of other vascular risk factors, including hypertension, hyperlipidemia, and cardiovascular diseases. Circulating concentrations of PlGF were higher in AD patients compared to NCI controls (Fig. 1A, p = 0.042) and were also elevated in the presence of cardiovascular diseases (Mann-Whitney, p = 0.016). PlGF levels correlated with age across the full study population (Spearman correlation coefficient rho = 0.239, p < 0.001).

Serum PlGF levels across (A) diagnostic groups and (B) subgroups stratified by CeVD status. AD, Alzheimer’s disease; CeVD, cerebrovascular disease; CIND, cognitive impairment no dementia; NCI, no cognitive impairment. In the scatter plots the central horizontal lines show the median concentrations, and the error bars show the 25th and 75th percentiles, respectively. *p < 0.05, **p < 0.01, ***p < 0.001 indicate significant pairwise comparisons using Kruskal-Wallis ANOVA with Dunn’s post hoc tests.
Serum levels of PlGF in diagnostic groups
To investigate whether the increase in PlGF levels in AD was primarily driven by CeVD, we further stratified the diagnostic groups based on the presence or absence of significant CeVD (as shown in Fig. 1B). Our results revealed a significant elevation in serum PlGF levels in the AD with CeVD subgroup as compared to both NCI without CeVD subgroup (p < 0.001) and AD without CeVD subgroup (p = 0.007). In multivariable logistic regression analyses (Table 2), with covariates taken into account, a significant association was only observed between higher serum levels of PlGF and AD with CeVD (odds ratio [OR], 1.2; 95% confidence interval [CI], 1.0 –1.5; p = 0.024). No association was found between PlGF and CIND or AD in the absence of CeVD, nor in CIND with CeVD.
Association of PlGF with CeVD burden
We then conducted separate subgroup analyses to examine the association between PlGF and specific types of CeVD markers graded on MRI scans, including WMH, cortical infarcts, lacunes, and CMBs. We found that subjects with multiple CMBs (Fig. 2C, p = 0.016) and confluent WMH (Fig. 2D, p < 0.001) had significantly higher serum PlGF concentrations, while no significant associations were observed with cortical infarcts or lacunes (Fig. 2A, B). Furthermore, in multivariate regression analyses, these associations remained significant only in AD subgroup, where elevated PlGF levels were independently associated with higher WMH burden (β, 0.2; 95% CI, 0.1–0.4; p = 0.006) and an increased number of CMBs (RR, 1.1; 95% CI, 1.0–1.1; p = 0.047), even after adjusting for covariates and relevant CeVD markers (Table 3). In contrast, we did not observe any significant associations between PlGF and MRI markers of CeVD among CIND subjects.
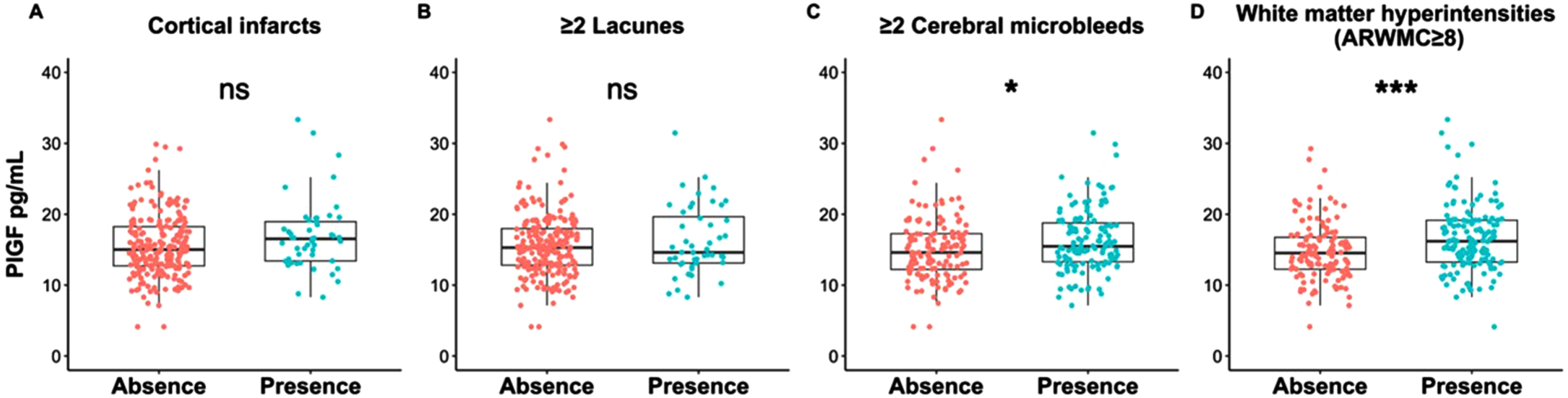
Serum PlGF levels in subjects stratified by presence of specific CeVD markers. ARWMC, age-related white matter changes; ns, not significant. Cut-offs of counts / scores for definitions of significant CeVD have been previously described [36]. Bar graphs show medians and interquartile ranges (IQR). Mann-Whitney U tests were performed, with p values indicated with asterisks: *p < 0.05, ***p < 0.001.
DISCUSSION
Our study builds upon previous research reporting elevated peripheral PlGF in patients with VCI [27] by showing increased PlGF is also found in a cohort of AD subjects with concomitant CeVD. Furthermore, significant associations were uncovered between peripheral circulating PlGF and two specific CeVD subtypes, namely WMH and CMB, both of which well-established predictors of cognitive decline and dementia in older adults [27, 37–39].
PlGF is a well-studied proangiogenic cytokine that signals through the Flt-1 receptor, and its importance lies in its ability to drive tissue vascularization and maintain vascular homeostasis [40]. It has also been linked to the pathogenesis of multiple vascular diseases and has emerged as a promising biomarker for endothelial dysfunction and vascular injury [41, 42]. The presence of cardiovascular risk factors known to predispose to vascular injury has been reported to be associated with elevated circulating PlGF [43, 44]. Similar findings were observed in our cohort where individuals with cardiovascular disease showed higher levels of PlGF in the serum. However, we identified an independent association between PlGF and CeVD in AD patients, which remains significant even after correcting for vascular risk factors. The exact mechanisms that lead to upregulated PlGF in AD with CeVD are not yet fully elucidated, but it is likely that they reflect activation of vascular repair processes. It is hypothesized that endothelial dysfunction plays a major role in initiating the pathological cascade that eventually leads to frank CeVD and VCI [45]. PlGF has been shown to be primarily released by activated endothelial cells and smooth muscle cells in response to injury and inflammatory stimuli that cause endothelial stress [18, 46]. While its ability to promote endothelial cell proliferation may play a protective role in maintaining endothelial integrity [20, 47], some experimental studies suggest a pro-atherogenic and disease-provoking role of PlGF during the early stages of plaque formation [48, 49], presumably through the activation of endothelial adhesion molecule expression, thereby facilitating the recruitment of monocytes to the arterial wall and contributing to downstream atherosclerotic plaque formation processes [50]. Although the exact role of PlGF in vascular diseases remains incompletely understood, several epidemiological studies have shown associations between elevated blood PlGF levels and an increased risk of cardiovascular events and stroke [51, 52], and it is possible that serum PlGF levels in AD patients with CeVD reflect common processes linking heart and brain vascular disease [53, 54].
The presence of CeVD is clearly linked to lower cognitive performance and an increased risk of cognitive decline and AD, contributing to disease progression and severity [7, 55]. One of the most common brain-imaging features of CeVD is WMH, which are histologically characterized by demyelination, gliosis, and axonal loss [56]. Post-mortem studies have shown a higher burden of WMH in AD brains, with WMH volume approximately three times larger than in controls [57]. Although the pathogenesis of WMH remains incompletely understood and may be multifactorial, WMH is strongly associated with hypoxic/ischemic brain injury [58], which may also induce PlGF expression. Studies performed in experimental animal models have shown an upregulation of PlGF in astrocytes and endothelial cells following cerebral ischemia, supporting a key role of PlGF in ischemic CeVD [23, 59]. Elevated levels of PlGF in both CSF and plasma have been found to be associated with WMH in non-demented subjects [26, 27]. However, in our study, we did not observe any association between PlGF and WMH in CIND patients. This disparity could be attributed to differences in cohort characteristics, sample size, definition of CeVD, and assessment methods. Further investigation is needed to elucidate the underlying factors contributing to the divergent results. In addition to WMH, we found that PlGF was also associated with CMBs, which are small or microscopic subclinical intracerebral hemorrhages believed to be linked to cerebral amyloid angiopathy and hypertensive microangiopathy, which are major pathological mechanisms for CMBs in AD [60]. These cerebrovascular pathologies are likely associated with structural alterations and increased permeability of small vessels, potentially leading to the development of CMBs [61]. Our findings raise the possibility that PlGF-induced endothelial cell repair responses are involved in the pathogenesis of CMBs. Furthermore, the differential relationship between PlGF and CeVD in AD patients and nondemented individuals in our cohort highlights the complex relationship between CeVD and AD neuropathological processes. This may be due to the generally higher burden of CeVD found in our AD patients, which may have significantly shifted the balance between protein production and clearance, leading to increased serum PlGF. Nevertheless, further research is needed to validate these findings and to better understand the role of PlGF in CeVD, as well as in cognitive impairment and dementia.
Study limitations
The current study has several limitations that should be considered while interpreting the study findings. Firstly, due to the cross-sectional and observational nature of the study, it is difficult to ascertain the causal nature of the links between PIGF and CeVD in AD. Therefore, further longitudinal analyses are required to determine the relative effect of elevated serum PlGF levels on CeVD progression in both AD and nondemented subjects. Secondly, this study was conducted predominantly in a memory clinic with a relatively small sample size, and a higher prevalence of vascular risk factors among the participants. This might introduce selection bias and potentially limit the generalizability of the study findings to the broader population. Furthermore, the relatively limited number of cases with infarct and lacunes may have restricted our ability to detect any significant associations between PlGF with these specific conditions. Lastly, although we did not observe any alterations in PlGF level among AD without CeVD subgroup, it might be of interest to further investigate the potential association between PlGF levels and established biomarkers for AD pathologies, such as amyloid burden, in order to gain a more holistic understanding of the intricate interplay between PlGF, CeVD, and AD pathologies. With larger follow-up studies, it would also be of interest to study amnesic vs. non-amnesic subgroups of minimally cognitively impaired (MCI, similar to CIND) individuals, to measure PlGF changes across the AD spectrum, as well as to better characterize PlGF associations with both cognitive impairment as well as with functional loss.
Conclusion
The findings of our study provide evidence that elevated serum levels of PlGF may serve as a biomarker for detecting the presence of CeVD, specifically WMH and CMBs, in AD patients. This has prognostic implications as significant CeVD is known to exacerbate AD progression. Furthermore, these findings add to current understanding of the links between angiogenic factors and cerebrovascular diseases and may inform the development of directed therapeutic interventions. However, further mechanistic studies are needed to elucidate the role of PlGF in CeVD pathogenesis. In addition, larger, prospective studies are required to validate our findings in larger and more diverse populations, as well as to investigate the sensitivity and specificity of PlGF as a diagnostic or prognostic biomarker of CeVD and VCI.
Footnotes
ACKNOWLEDGMENTS
We acknowledge the coordinators at the Memory Aging & Cognition Centre, National University Hospital for their contribution to recruitment and data acquisition.
FUNDING
This work was supported by the Singapore National Medical Research Council (MOH-000707-01) and the Yong Loo Lin School of Medicine Healthy Longevity Translational Research Programme (grant HLTRP/2022/PS-01).
CONFLICT OF INTEREST
Mitchell Lai and Saima Hilal are Editorial Board Members of this journal but were not involved in the peer-review process nor had access to any information regarding its peer-review. All other authors have no conflict of interest to report.
DATA AVAILABILITY
Anonymized data analyzed in the current study is available on reasonable request from the corresponding author.