
Abstract
Background:
Alzheimer’s disease (AD) stands as the prevailing type of dementia, marked by gradual memory loss and cognitive decline. Transcranial direct current stimulation (tDCS) is a non-invasive method used to regulate cortical brain function and has been explored as a potential treatment for cognitive impairment.
Objective:
This study aimed to compare the effects of daily home-based active or sham tDCS on cognitive function in patients with early-stage AD and its follow-up after one month.
Methods:
The study involved a randomized, blinded, and controlled-placebo design, with 18 participants enrolled. The primary outcome measures were general cognitive function, immediate, and delayed recall, and executive function. Participants included in the study were randomly assigned to the anodal and sham tDCS groups. Participants were assessed before and after the intervention and one month after the end of treatment. The home-based intervention was applied for 5 consecutive days, daily.
Results:
The results showed a significant interaction between the active and sham groups; in particular, improvements in MMSE scores, immediate memory and delayed recall were observed at one-month follow-up in the active group.
Conclusions:
The positive effects of tDCS on cognitive function in AD patients observed suggest that tDCS may induce long-term neuroplastic changes, leading to sustained improvements in cognitive abilities.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) stands as the most common form of dementia. It is primarily distinguished by progressive memory loss, although as the disease advances, other cognitive domains and executive functions are often affected [1]. Despite its rising prevalence, existing therapeutic approaches, though enhanced, exhibit restricted effectiveness in preventing, slowing, or stopping the progression of the disease. Anti-amyloid therapies are a type of treatment for AD that target the protein fragments that build up in the brain and form plaques, which is a defining feature of the disease [2]. The anti-amyloid antibody drug aducanumab was the first approved therapy to show that clearing amyloid-β from the brain lessens cognitive decline in individuals with early AD [3, 4]. These therapies are potentially effective, with a reduction in cognitive impairment of around 30%. However, their long-term effect is still unknown, and they have high economic costs. Although they constitute a promising avenue of research for the treatment of AD, many questions remain to be answered.
Transcranial direct current stimulation (tDCS) is a non-invasive method that involves applying a mild electrical current to the brain through electrodes placed on the scalp. Its primary goal is to regulate cortical brain function by inducing alterations in cortical excitability and synaptic plasticity [5, 6]. Compared to other methods of brain stimulation, tDCS is relatively safe, straightforward, and cost-effective to administer.
The application of the technique has focused primarily on the dorsolateral prefrontal cortex (DLPFC) because the DLPFC possesses widespread reciprocal connections with nearly all cortical and subcortical brain structures, enabling it to effectively coordinate and integrate the functioning of various other brain regions [7]. The DLPFC performs a crucial function in tasks associated with executive control and memory. Specifically, the left DLPFC seems to play a role in self-initiated memory strategy utilization, and research has revealed that individuals may engage distinct neural networks based on their adoption of encoding strategies [8]; furthermore, the crucial role of the left DLPFC in encoding, and its involvement in memory trace formation, consolidation, and maintenance, has been confirmed [9].
Results in healthy and cognitively impaired older adults point mainly to beneficial effects, but results remain mixed. In healthy older adults, tDCS has shown promise as a technique to improve cognitive function [10] particularly in the areas of learning [11, 12], working memory [13, 14], and memory encoding, retrieval, and recognition [15, 16]. However, the effects may be small or partial, and the short- and long-term effects of tDCS depend on baseline cognitive status, especially benefiting older adults who may need help [17]. Overall, studies suggest that tDCS has the potential to improve cognitive function in patients with mild cognitive impairment (MCI) and may be a meaningful treatment alternative for these patients. Research results point to improvements in episodic memory with effects lasting 4 weeks [18], in immediate and delayed memory [19, 20] and slightly significant benefits of stimulation for executive functions have also been found [21].
Studies exploring the effects of tDCS in patients with early AD have yielded mixed results. While some studies have indicated no significant effects, an increasing body of evidence supports the potential benefits and therapeutic role of tDCS in enhancing or postponing cognitive decline in AD [22]. It has been demonstrated that in AD patients there is a consistent alteration of cortical plasticity, being tDCS a technique that could facilitate the synaptic plasticity of the circuits [23]. Enhancing memory and learning is especially relevant for patients seeking to improve their capacity to recall information and establish associations between memories. The impact of daily home-based tDCS targeting the DLPFC over a 6-month period was examined in patients with early-stage AD, and an enhancement in global cognitive performance, as assessed by the MMSE, was observed following active tDCS. [24]. Considering the anticipated annual decline in MMSE scores, the study proposes that repeated tDCS not only halts the deterioration of global cognitive functioning in patients with early AD but also yields improvements. Furthermore, research indicates that individuals with milder AD demonstrate more favorable responses to tDCS, while its efficacy diminishes in advanced stages with reduced neuroplasticity [25]. The findings reveal enhancements in various cognitive functions, including temporal and spatial orientation, reversal learning or verbal intelligence. Additionally, there were observed changes in the beta band with an increase and a decrease in P300 latency. A meta-analysis showed that tDCS was effective in improving cognition in AD patients, with anodal stimulation being more effective [26]. Furthermore, another meta-analysis [27] reinforces the notion that tDCS protocols yield positive effects in ameliorating cognitive impairment induced by AD, particularly in the domains of memory and global cognitive function. However, changes in the attention domain did not achieve statistical significance.
The objective of this study was to compare the effects of daily home-based sessions of active or sham tDCS targeting the DLPFC for 5 days on cognitive function in patients with early-stage AD. Additionally, the study assessed the follow-up one month after completion.
MATERIALS AND METHODS
Study design and participants
We conducted a randomized, blinded, and placebo-controlled study involving five sessions of active anodal tDCS on the DLPFC, which was compared to a sham or placebo group. Participants were assessed before for baseline and after the intervention and followed up one month later.
Eligible patients were aged >65 years, meeting the criteria for probable AD dementia as per the National Institute on Aging-Alzheimer’s Association workgroup (NIA-AA) [1], and obtained a Mini-Mental State Examination (MMSE) [28] score ranging from 16 to 22 during screening. Patients were considered eligible for enrollment in the study if they scored 4 on the Global Deterioration Scale (GDS) [29] and obtained a score lower than 28 on the Memory Alteration Test (M@T) [30].
Patients with any of the following conditions were excluded from the study: neurodegenerative diseases other than AD dementia or severe psychiatric symptoms; individuals with low (dependent) or high (independent) function on the Lawton Instrumental Activities of Daily Living (IADL) assessment [31]; subjects with contraindications to tDCS, such as intracranial metallic implants or intracranial hypertension; and lastly, participants had to reside in the community, with no current or anticipated residence in a nursing home during the study.
Participants were recruited from the Neurology department of the Consorcio Hospital General Universitario de Valencia. Initially, 31 patients were contacted, of which thirteen were excluded: five with an MMSE < 15, three with an MMSE < 15 and GDS = 5, two with an MMSE > 22 and GDS = 3, and three declined. The final sample comprised 18 subjects, including 7 men and 9 women, accounting for 38.9% and 61.1% of the total, respectively. The participants’ ages ranged from 65 to 87 years, with a mean age of 74.06 (SD = 5). All subjects provided their informed consent at the outset of the study. The research received approval from the Ethics Committee of Research in Humans of the Ethics Commission in Experimental Research of University of Valencia with register code 2601758.
Once the inclusion/exclusion criteria were verified, patients were allocated to either the active tDCS or sham groups through stratified block randomization, with a 1:1 ratio and sex as the stratum. Participants remained unaware of their assigned group until the end of the intervention, as the study followed a single-blind design. A flowchart of the study is shown in Fig. 1.
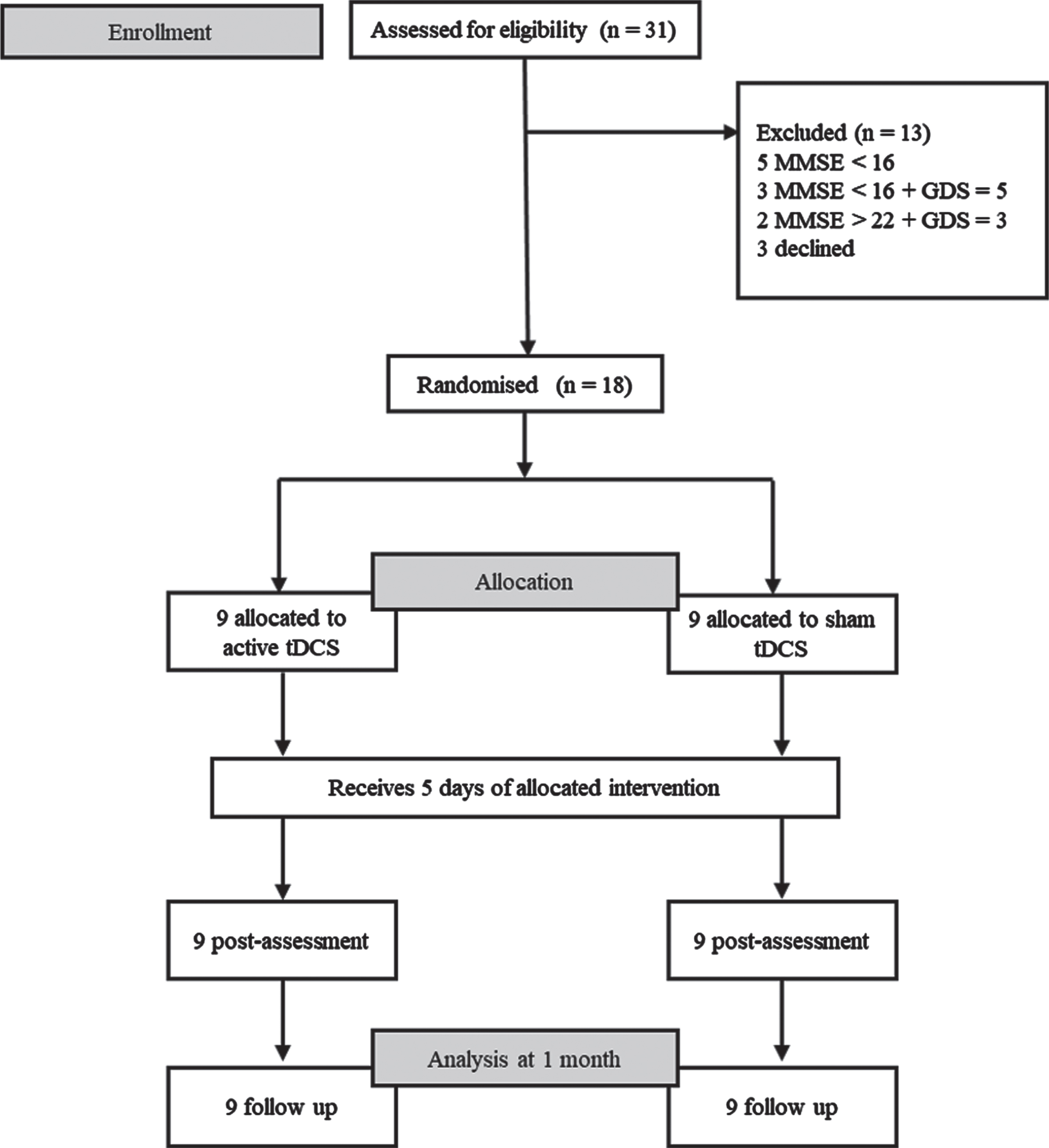
Flow diagram of trial profile.
The active anodal tDCS group comprised 9 participants, while the sham or placebo group consisted of 9 participants as well. Table 1 below displays the primary data and the comparison tests conducted between the two groups. Both groups were well-matched in their characteristics.
Means (and SD) of demographics indices comparing active and sham groups
Measures
The primary outcome measures included general cognitive function, immediate and delayed recall, while executive function was evaluated as a secondary outcome measure. These measures were chosen based on the significance of memory impairment in characterizing the pathology. The objective was to analyze potential changes in these variables. Additionally, considering the typical decline in executive control as the disease progresses, we aimed to investigate changes in this variable as a secondary outcome.
The MMSE [28] is arguably the most commonly utilized screening test for dementia, serving as a concise and quantitative assessment of overall cognitive function. The highest achievable MMSE score is 30.
Test Aprendizaje Verbal Complutense (TAVEC) [32]. This test is based on a list of 16 words that are read aloud, and the participant is asked to repeat them at the end of the list. The first trial assesses immediate memory. The procedure is repeated five times (trials) in order to obtain the total number of words remembered after having tried the list five times. After 20 min, the participant is asked to recall all 16 words (delayed memory).
The Digit Span subtest of the Wechsler Intelligence Scale for Adults-III [33] evaluates working memory and mental flexibility. In this task, the subject is required to repeat a series of digits presented by the examiner but in reverse order. A score of one point is awarded for each correct item, with a maximum achievable score of 16.
The Memory Alteration Test [30] offers rapid and effective screening with excellent discriminative properties for amnestic MCI (aMCI) and early-stage AD within the general primary care population. The test assesses various abilities, including encoding, orientation, semantic memory, and free recall. It features oral questions with only one possible answer, and the maximum score achievable is 50 points. A cut-score of 28 was found to distinguish between aMCI and early AD (sensitivity 0.91; specificity 0.78).
Finally, to assess the independence of older adults Lawton’s Instrumental Activities of Daily Living scale was applied [31]. Scale provides information about functional skills necessary to live independently in the community and includes 8 activities: the ability to use a telephone, shopping, meal preparation, housekeeping, laundry, model of transportation, responsibility for own medication, and ability to manage finances. The rating scale is zero and one, and the sum of the scores ranges from 0 (low functioning, dependence) to 8 (high functioning, independence).
Intervention
Stimulation was performed with an HDC stimulator (Newronika TM, Milan, Italy), which delivers direct current.
The current intensity used for tDCS was set at 2 mA, and each stimulation session lasted for 20 min. Prior to the initiation of stimulation, a 30-s current ramp was delivered, and the same procedure was repeated at the end of stimulation. In the tDCS placebo condition, the current was automatically turned off between the ramps. For electrode placement, 25 cm2 rubber electrodes were positioned on a neoprene headcap, with predefined and clearly annotated positions based on a subset of the international 10-10 EEG system. The anode was placed in F3, targeting the left dorsolateral prefrontal cortex, and the cathode was placed in the right frontal lobe (Fp2). Both the active tDCS and placebo conditions had identical electrode placement and session duration.
Procedure
The Neurology department recruited patients with an initial diagnosis of AD. An appointment was made to explain the research procedure, obtain informed consent and check eligibility criteria. Baseline data was obtained from the participants. Participants included in the study were randomly assigned to the anodal and sham tDCS groups. Two technicians (psychologists) with specialized training in the technique conducted and supervised the home-based intervention consistently for 5 consecutive days. The HDCstim® stimulator was connected to the HDCprog to guarantee the accurate application of stimulations. The HDCprog’s menu included a “treatment report” to verify the correct impedance and treatment results. On the final day, after completing the stimulation sessions, the evaluation was conducted once again. A follow-up evaluation was performed one month after the end of the treatment.
Data analysis
A mixed factorial ANOVA 2 (groups)×3 (time) was performed for each dependent variable; p values of ≤0.05 were considered statistically significant. Significant interactions were analyzed using Bonferroni tests to compare the means of the two groups at each assessment point (pre-intervention, post-intervention, and follow-up), as well as simple effects tests to analyze whether there were significant differences between the different assessment points of each group.
RESULTS
We analyzed the data by means of mixed ANOVAs 2 groups (active versus sham; between-subjects)×3 assessments (pre-intervention, post-intervention and follow-up; within-subjects). The efficacy of tDCS should be observed by finding a significant interaction between these two independent variables. Table 2 shows these main and interaction effects.
Regarding the significant interaction of the MMSE (Table 2), Bonferroni t-tests showed there was no a significant difference between groups at either pre-test (p = 0.349) or post-test (p = 0.299), but at follow up the treatment group mean was significantly higher (p = 0.035) than the sham group mean (Table 3). Regarding to the treatment group data, a simple effects test showed the effect of the three assessments to be significant (F(2, 16) = 10.91; p = 0.001, λ2 = 0.577). Bonferroni t-tests showed that there was no significant difference within pre-test and post-test means (p = 0.259), the difference within post-test and follow-up was marginally significant (p = 0.064), and the difference within pre-test and follow-up means was significant (p = 0.006). As for the sham group data, a simple effects test showed that the effect of the three assessments was not significant (F(2, 16) = 2.16, p = 0.148, λ2 = 0.213), meaning that there was no significant differences between the three assessments means.
Main and interaction effects
With respect to the significant interaction of the TAVEC trial 1, which asses immediate memory, Bonferroni t-tests showed there was no a significant difference between the groups at pre-test (p = 0.349), but both at post-test (p = 0.049) and follow-up (p = 0.006) the treatment group mean was significantly higher than the sham group mean (Table 3). Regarding to the treatment group data, a simple effects test showed the effect of the three assessments to be significant (F(2, 16) = 10.48; p = 0.002, λ2 = 0.552). Bonferroni t-tests showed that there was significant difference within pre-test and post-test means (p = 0.008) and within post-test and follow-up (p = 0.026), but there was not a significant difference within pre-test and follow-up (p = 0.585). As for the sham group data, a simple effects test showed that the effect of the three assessments was not significant (F(2, 16) = 0.01, p = 0.999, λ2 = 0.001), meaning that there was no significant differences between the three assessments means.
Means and standard deviations (SD) of the significant interactions
Finally, concerning the significant interaction of the TAVEC delayed recall (Table 2), Bonferroni t-tests showed there was no significant difference between groups at either pre-test (p = 0.332) or post-test (p = 0.095), but at follow-up the treatment group mean was significantly higher (p = 0.012) than the sham group mean (Table 3). Regarding to the treatment group data, a simple effects test showed the effect of the three assessments to be significant (F(2, 16) = 6.11; p = 0.011, λ2 = 0.433). Bonferroni t-tests showed that there was no significant difference within pre-test and post-test means (p = 0.416), the difference within pre-test and follow-up was significant (p = 0.040), and the difference within post-test and follow-up means was no significant (p = 0.186). As for the sham group data, a simple effects test showed that the effect of the three assessments was not significant (F(2, 16) = 2.0, p = 0.168, λ2 = 0.201), meaning that there was no significant differences between these three means.
DISCUSSION
The results obtained in this research suggest that the application of active stimulation using tDCS had a positive impact on cognitive function compared to the sham group, as demonstrated by improvements in MMSE scores, immediate memory and delayed recall at one-month follow-up.
The significant interactions observed between the active and sham groups provide evidence that active tDCS stimulation has a positive impact on cognitive function in patients with early AD. The improvements in MMSE scores, immediate memory (TAVEC Trial 1), and delayed recall (TAVEC Delayed) at the one-month follow-up in the active group suggest that tDCS may be beneficial for enhancing cognitive abilities in this population. These findings are consistent with previous research supporting the potential positive effects of tDCS on cognitive function in AD patients.
It has been demonstrated the efficacy of tDCS in enhancing cognitive performance in individuals with MCI and AD [34]. Several meta-analyses [26, 27] analyzing the effects of tDCS on cognitive function in patients with AD concluded that tDCS appears to improve cognitive function in AD. These studies provide support for the notion that tDCS can have positive effects on cognitive function in AD. However, unlike other research that reported significant improvements in working memory in AD patients after active tDCS on the left DLPFC, other research reports that the results of the interaction were not significant so that the intervention had no effect on executive function [35].
Importantly, no significant differences were observed between the active and sham groups in MMSE and delayed recall scores at both pretest and posttest. This consistent finding aligns with a previous study [36], which also reported similar results in AD patients receiving either active or sham tDCS. The lack of immediate differences suggests that the immediate effects of tDCS on cognitive function may not be readily detectable. However, the significant differences observed at the one-month follow-up indicate that the effects of tDCS may require time to manifest and become detectable. These findings imply that tDCS may induce long-term neuroplastic changes, leading to sustained improvements in cognitive abilities. Further research with longer follow-up periods is necessary to fully understand the duration and stability of the observed effects and their impact on cognitive impairment in individuals with early AD.
These long-term effects may be attributed to neuroplastic changes induced by tDCS. Previous research has shown that tDCS can modulate neuronal activity and promote synaptic plasticity [37]. By enhancing neural connectivity and facilitating neuronal networks involved in memory and cognition, tDCS may lead to sustained improvements in cognitive abilities.
Nevertheless, it is worth noting that certain studies [38] have indicated a correlation between intellectual inactivity and a lower level of education (typically defined as less than 8 years of schooling) with an increased risk of AD. Furthermore, a meta-analytic study [39] has corroborated the role of low education as a potential risk factor for dementia, particularly in the case of AD. These findings underscore the significance of accounting for patients’ cognitive reserves and advocating for combined treatment strategies. Such strategies should not only involve electrical stimulation but also incorporate training and cognitive stimulation to bolster the cognitive functions that patients can still maintain [40, 41].
While the findings of this study are promising, it is important to acknowledge some limitations and future directions. The sample size appears to be relatively small, which may limit the generalizability of the findings. Additionally, the follow-up period was limited to one month, and it would be valuable to investigate the longer-term effects of tDCS. Future studies could consider expanding the sample size, extending the follow-up period, and exploring other cognitive domains to gain a more comprehensive understanding of the effects of tDCS in AD patients. In addition, it is important to consider the variability in individual responses to tDCS. While the overall group analysis showed significant effects, it is possible that some individuals within the active group experienced greater improvements in cognitive function compared to others. Exploring individual differences in response to tDCS could help identify potential predictors of treatment efficacy and personalize interventions for AD patients.
In summary, the study provides evidence that active tDCS stimulation has the potential to positively influence cognitive function in patients with early AD. The findings suggest that tDCS may have long-term effects on cognitive abilities, emphasizing the importance of exploring the underlying mechanisms and optimizing stimulation protocols. Continued research in this area may contribute to the development of effective non-invasive interventions for cognitive enhancement in individuals with AD.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This work was supported by MCIN/AEI [Grant PID2022-136798OB-I00].
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.