
Abstract
Background:
Alzheimer’s disease (AD) is a complex condition that affects various aspects of a patient’s life. Music therapy may be considered a beneficial supplementary tool to traditional therapies, that not fully address the range of AD manifestations.
Objective:
The purpose of this systematic review is to investigate whether music therapy can have a positive impact on AD patients and on which symptoms.
Methods:
The main research databases employed have been PubMed and Cochrane, using the keywords “dementia”, “music therapy”, “Alzheimer”, “fMRI”, “music”, and “EEG”.
Results:
After removing duplicates and irrelevant studies, 23 were screened using set criteria, resulting in the final inclusion of 15 studies. The total number of participants included in these studies has been of 1,196 patients. For the fMRI analysis the search resulted in 28 studies on PubMed, two of which were included in the research; the total number of participants was of 124 individuals. The studies conducted with EEG were found using PubMed. The initial search resulted in 15 studies, but after a more accurate evaluation only 2 have been included in the analysis.
Conclusions:
Even though the data currently available is not sufficient to draw conclusions supported by robust statistical power, the impact of music therapy on AD neuropsychiatric symptoms deserves great interest. Further research should be ushered, possibly multicentric studies, led with neuroimaging and other recent techniques, which can eventually open views on the music role in improving the cognitive status in AD.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) was estimated to have a prevalence of approximately 50 million people in global population by the Alzheimer’s Disease International in 2018 [1]. It was also reported, based on a US-based study, that the average survival of patients with AD dementia after receiving the diagnosis is of 6 years [1]. AD dementia is a medical condition characterized by a progressive cognitive impairment associated with neurobehavioral symptoms, witch significatively influence daily life [1].
Currently, even if the etiopathology of AD is not entirely understood, it is widely accepted that the underlying causes of the disease include the accumulation of amyloid plaques and tau tangles, neuroinflammation, damage to blood vessels, and shrinkage of brain tissue [2, 3]. These changes disrupt normal neuron function, lead to the loss of connections between neurons, and ultimately result in neuronal death [3]. Furthermore, it has been demonstrated that the brain structure of AD patients is characterized by changes in the synapses of the neurons implicated in memory and learning; these changes include alterations in the balance between excitation and inhibition, and the increase of multi-innervated spines in the transentorhinal cortex, which has been considered as an attempt to compensate the loss of connectivity [4].
It is relevant to emphasize that these alterations take place in areas such as the hippocampus and the entorhinal cortex, which are crucial hubs implicated in the strategical representation of objects and in spatial information, as well as direction and orientation [5]. These areas have shown remarkable signs of neurodegeneration and atrophy in subjects affected by AD [5–7]. Together, these alterations affect the function that these areas play in episodic memory encoding and behavioral planning [8]. It is also important to remark the possibility of using the degree of atrophy in the entorhinal cortex as a biomarker to predict the evolution of the pathology [9]. Progressively, as the damage spreads, more and more brain regions are involved, and this results in an escalating cognitive impairment, predicted by the shrinking of the hippocampal portion of the entorhinal cortex [10].
The evolvement of the pathology could be traced by measuring several biomarkers, different for each phase of the disease [11]. The first to undergo modifications are the amyloid-β biomarkers, followed by the increasing of the cerebrospinal fluid tau and by cerebral atrophy spotted on the MRI, that correlates with neuronal injury and neurodegeneration [11].
The overarching complexity of the etiopathogenetic players involved in AD makes exceedingly challenging to design and to eventually develop effective treatment methods. Experts believe that a combination of drug and non-drug interventions (i.e., behavioral methods) is the most promising approach in treating AD [1]. Drug interventions include treatments that have different targets, such as cognitive function (cholinesterase inhibitors and memantine), neuropsychiatric symptoms (pimavanserin, brexpiprazole, citalopram, nabilone, and suvorexant), and monoclonal antibodies that have been shown to be promising as disease-modifying therapies [1, 12]. These include for example aducanumab and gantenerumab, that target amyloid-β plaques, but also oligomannate, that acts on neuroinflammation [1, 13]. Finally, a recent study published on the New England Journal of Medicine has shown the efficacy of a new monoclonal antibody in reducing markers of amyloid-β and in lessening cognitive decline of patients with AD [14]. Non-pharmacological interventions include lifestyle changes (interruption of tobacco and alcohol exposition, physical exercise, etc.), treatment of hypertension and diabetes, but also cognitive stimulation, that has been shown to improve cognitive function in people with mild dementia [15], and social activities [1, 16].
Music therapy is one of the therapeutical options that are thought to play a potential role in contributing to the treatment of mild forms of dementia correlated to AD [15]. Indeed, several observations prove such a potential contribution; firstly, research has shown that music can positively impact the process of neuroplasticity [17], which in its turn can impact, and eventually improve, functions like speaking, learning, attention, and memory [18, 19]. Additionally, it has been observed that music can have a positive influence on behavior, emotions, and cognitive processes, potentially due to its ability to enhance parallel activation of different brain areas [19]. Some of these areas include cortical-subcortical circuits, the limbic system, and the amygdale-centered emotional reward system [15].
There are many different types of music therapy interventions. Some of them include Group Music Therapy (GMT) [20], Recreational Choir Singing (RCS) [21], Music & Memory (M&M) [22], Active Music Intervention (AMI) [23], and Receptive Music Intervention (RMI) [24]. Among them, there are methods that need active participation from the patients involved, such as GMT, that is done in small groups of 8–10 participants that share activities like singing familiar songs or improvise melodies on instruments like the drums [20], and AMI, also an intervention received by small groups of people, that sing and dance together and do rhythmic exercises [23]. Instead, M&M and RMI are mainly passive [22, 24]. In fact, M&M consists of listening to a personalized music playlist [22] and RMI consists of listening to songs together with another small group of patients, and to share feelings or memories after each song [24]. Passive interventions are known for their ability to impact emotions and behaviors [23], so that they can be considered some of the main approaches also in the therapy of subjects affected by autism [25] or epilepsy [26]. Active interventions employ an approach that is often shared with other patients or with family members, and that consists of “making” music [20]; in this sense, we can say that whoever receives the intervention plays an active role in their therapy, and is subjected not only to auditory stimuli, but also to active movements and creativity reasoning [20]. Active music interventions (but also RMI) often include discussions and emotion sharing, and for this reason they are very useful to improve social abilities and communication [24].
The potential of music as a therapeutic intervention for various neurological disorders is supported by a wide range of neurobiological factors [27, 28]. One example of research on the use of music as a therapeutic intervention for neurological disorders is a study that showed an increase in the release of dopamine in the ventral striatum and ventral tegmental area of subjects listening to pleasant music [27]. Other chemicals involved in the body’s response to music include endorphins, endocannabinoids, and nitric oxide [27, 30].
A recent study also shows the implication of the brain-derived neurotrophic factor (BDNF), in musical stimuli [31]. This molecule, along with other neurotrophic factors (as NGF, neurotrophins, etc.), plays a key role in regulating several processes, including neurogenesis and synaptogenesis [32, 33]. Particularly, BDNF is produced by the entorhinal cortex and plays a pivotal role in regulating memory circuits, such as the complex neocortical entorhinal hippocampal circuitries [32, 34]. All these networks are affected in AD, as BDNF and NGF-mediated signals decline in the damaged regions [31, 33]. Moreover, it is of interest that music increases the levels of BDNF in animal models, with consequences on neurogenesis modulation [31].
Despite the amount of evidence in support of music therapy (MT), there is an important gap in literature, concerning the methodological aspect of MT clinical trials [27]. Indeed, there is a lack of guidelines and evidence on how to undertake a study that has the main goal of objectivating and evaluating the efficacy of MT.
The aim of this research is to highlight the similarities and differences among clinical studies dealing with the role of MT in supporting treatments for cognitive impairment. We dare to provide an overall evaluation of MT’s efficacy, based on a critical update of the available studies.
MATERIALS AND METHODS
This systematic review of the literature was conducted according to the Preferred Reporting Items for Systemic Reviews and Meta-Analyses (PRISMA) guidelines. The search question was formulated using the PICO template: the condition of which the patients included are affected is AD dementia; the type of intervention on which the study concentrates is a potential complementary treatment to AD, music therapy; the study compares classic pharmacological treatments for AD with and without the association with music therapy; the relevant outcomes evaluated are the effects on cognition and neuropsychiatric behaviors.
322 studies were found on PubMed and 91 on Cochrane. Further refinement was done by applying filters such as “Randomized controlled trial” and limiting publication date range from 2013 to 2023. This time frame was chosen with the purpose of including more recent research, considering 10 years from the start of this study a good compromise for adding a sufficient number of contemporary studies. The selection process was completed by excluding studies that were not focused on evaluating the efficacy or effects of music therapy, those with biased results, and duplicates. The primary search yielded 31 studies to include in the review. After removing duplicates and irrelevant studies, 23 were screened using set criteria, resulting in the final inclusion of 15 studies (Fig. 1).
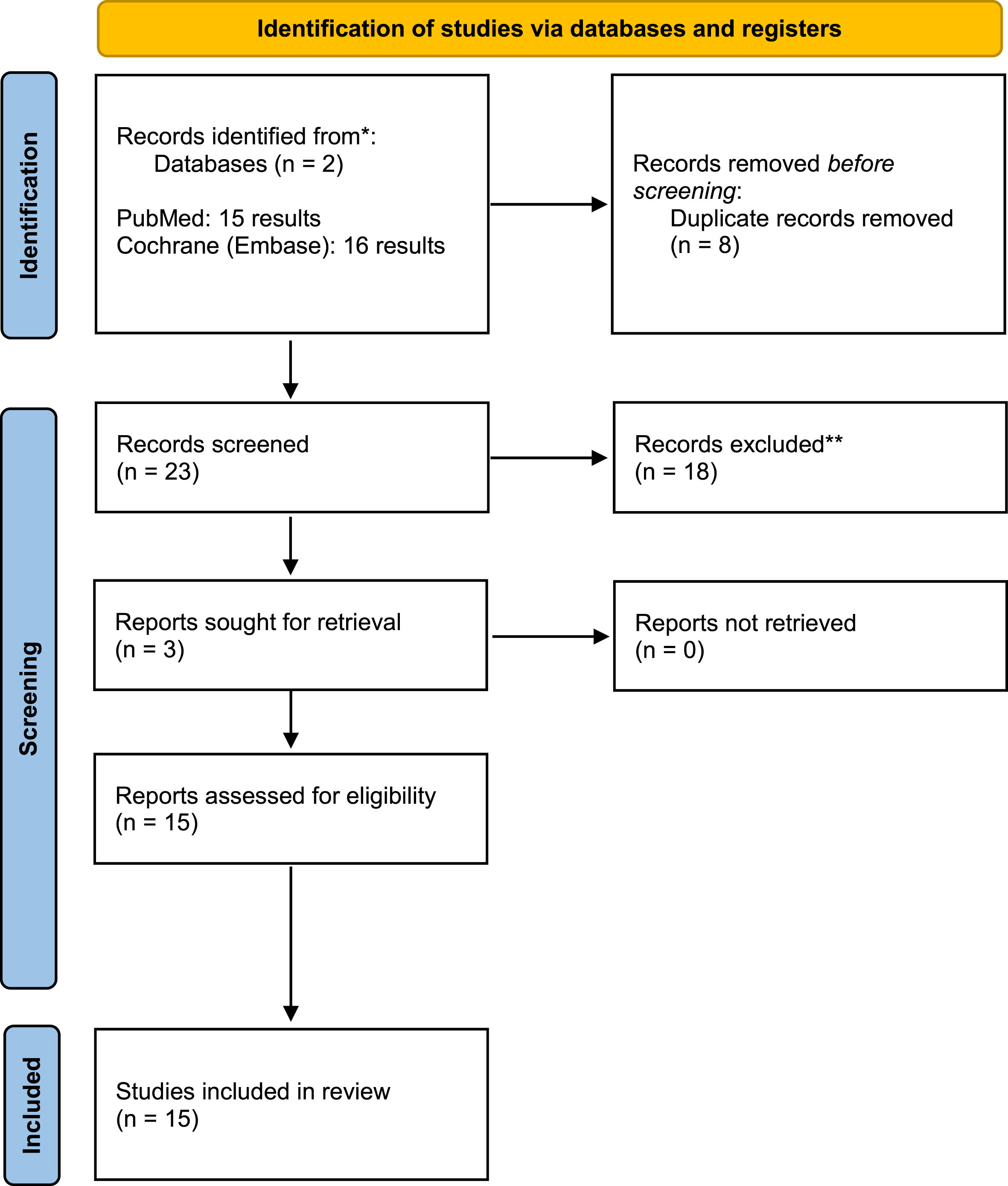
Graphic chart of the process of selection and exclusion of studies.
The research was performed by one person, while the review and the quality evaluation was done by two of the authors.
Search strategy
The literature search was conducted in December 2023, using two different computerized databases: PubMed and Cochrane (Embase). The initial search used the keywords “dementia” and “music therapy”, and later added “Alzheimer”. Then the keywords were switched to “dementia”, “music therapy”, and “MCI”. It was also selected a time frame from 2013 to 2023.
For the selection of fMRI studies, the keywords that have been employed are “fMRI”, “music”, and “Alzheimer”, with a publication date selected in the website filters from 2013 to 2023. The search retrieved 28 studies mentioned on PubMed; after further assessment, five of them fulfilled the criteria of our survey (Fig. 2). Another search was conducted with PubMed and Cochrane (Embase), by using the keywords “EEG”, “music”, and “Alzheimer”. Of the two studies found with Cochrane (Embase), none was considered eligible to be included in the present research, while of the 15 studies found with PubMed, 5 were analyzed, and 2 of them were selected (Fig. 3).

Graphic chart of the process of selection and exclusion of fMRI studies.
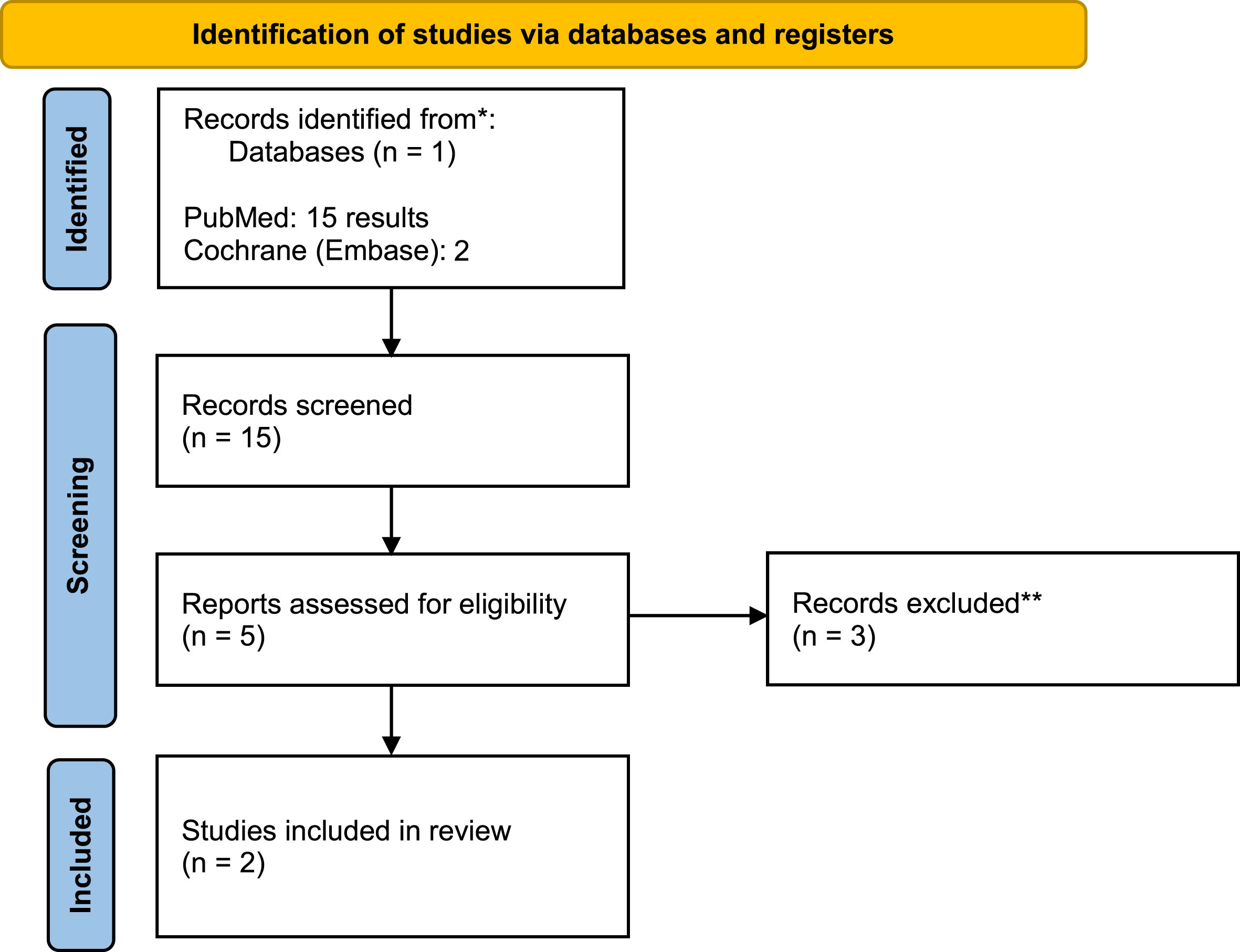
Graphic chart of the process of selection and exclusion of EEG studies.
Finally, another research was conducted with PubMed and Cochrane (Embase), to find studies on music therapy done with magnetoencephalography, using the keywords “MEG”, “music”, and “Alzheimer”. The research unfortunately didn’t bring any study that was eligible to be included in the present article.
Study selection
After duplicates and not pertaining studies removal, the initial selection was based on the presence of search terms in abstract and title, and on the subsequent retrieval of the full text of the possibly eligible studies. Eligibility for this systematic review regarded two inclusion criteria: English as a language and studies conducted with music therapy. Exclusion criteria were: studies that did not include evaluation on people with dementia correlated with AD, language other than English, review articles, studies that had a different purpose than of evaluating the efficacy of music therapy, and studies that have not been concluded yet.
Quality assessment
The presence of relevant biases in the included studies was evaluated by two readers according to QUADAS-2 criteria [35]. The performed quality assessment included 4 domains: 1) patient selection, 2) index test, 3) reference standard, 4) flow and timing. We used the proposed signaling questions to determine the risk of bias and concerns regarding the applicability, grading them as low, high, or unclear in case of insufficient data (Fig. 3).
RESULTS
The data from each study is summarized in Table 1, including details on: the type of music therapy used, number of participants, frequency and duration of therapy, evaluation time frame, and cognitive tests/parameters used to measure results. The total number of participants that were included in these studies has been of 1,196 patients. This systematic review does not include a meta-analysis, since the studies that have been included were too heterogeneous in methodological methods and clinical outcome evaluations to allow to draw out bias-free conclusions.
Graphic chart of the process of the quality assessment according to QUADAS-2 criteria

The techniques of music therapy employed in the studies were various and included listening to personalized music playlists [36–38], singing [39], RMI and AMI [36], GMT [40], “music with movement” [41], and Active Music Therapy [42].
Also, the time intervals between interventions and evaluations, as well as the duration of the MT sessions, were disparate, as reported in Table 2.
Characteristics of the studies conducted with music therapy
AD, Alzheimer’s disease; ADAS-Cog, Alzheimer’s Disease Assessment Scale Cognitive Subscale; ADL, activities of daily living; AMI, active music intervention; AMT, active music therapy; AVLT, Auditory Verbal Learning Test; BANS-S, Bedford Alzheimer Nursing Severity scale; CDR, Clinical Dementia Rating; CMAI, Cohen-Mansfield Agitation Inventory; CSDD, Cornell Scale for Depression in Dementia; GAI, Geriatric Anxiety Inventory; GDS, Geriatric Depression Scale; GMT, group music therapy; HADS, Hospital Anxiety and Depression Scale; IADL, instrumental activities of daily living; MADRS, Montgomery–Åsberg Depression Rating Scale; MCET, multimodal cognitive enhancement therapy; MCI, mild cognitive impairment; MDS-ABS, Minimum Data Set-Aggressive Behavior Scale; ML, music listening; MM, music with movement; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; MRA, music reminiscence activity; MT, music therapy; NPI, Neuropsychiatric Inventory; NPI-NH, Neuropsychiatric Inventory Nursing Home Version; NPI-Q, Neuropsychiatric Inventory–Questionnaire; OERC, Observed Emotion Rating Scale; PCTB scale, Professional Care Team Burden scale; PHQ-9, Patient Health Questionnaire-9; QoL-AD, Quality of Life in Alzheimer Disease; RAID, rating anxiety in dementia; RAVLT, Rey auditory verbal learning test; RCS, recreational choir singing; RMBPC, Revised Memory and Behavior Problems Checklist; RMI, receptive music intervention; RMT, receptive music therapy; SA, social activities; SIB, Severe Impairment Battery; SIB-l, Severe Impairment Battery-Language; SMMSE, Standardized Mini-Mental State Examination; VAS, visual analog scale; WAIS, Wechsler Adult Intelligence Scale.
The outcome measures vary from Mini-Mental State Examination (MMSE) [36, 43], to Neuropsychiatric Inventory [36–39, 42], Barthel Index [36, 39], Cohen-Mansfield Agitation Inventory [37, 41], and activities of daily living [40, 42]. Other studies, instead, utilized other more specific questioners, that are shown in Table 2.
From the analysis emerges that music therapy has many effects on different sides of the pathology; in fact, in all the studies it was found that music therapy seems to stabilize and to reduce neuropsychiatric symptoms, such as agitation, irritability and disinhibition. Also, it was shown to reduce depression symptoms in AD patients, as well as caregivers’ stress.
Lyu et al. pointed out how music therapy can enhance memory and language in patients with mild dementia [39]. This evidence was also supported by Gallego et al., that showed how AMI might be more cognitively stimulating than RMI [36]. Lyu et al.’s study resulted in an improvement in participants’ memory and language [39]. Giovagnoli et al. highlighted how music therapy associated to memantine has a better outcome on psychiatric health and depression symptoms than memantine alone [42]. According to Cheung et al.’s study, there are no significative differences between the effects of different intervention techniques, and more specifically between music with movement and music listening [41]. McCreedy at al.’s study draws to the conclusion that music interventions decrease patients’ behaviors [38]; Gold et al. pointed out a reduction in caregivers’ distress and in participants’ depression symptoms after music therapy [40]. This was also shown by Kwak et al., that have also highlighted a significant impact on irritability and disinhibition [37]. Garrido et al.’s results focalize on the improvement in patients’ quality of life, with increases in parameters such as Interest, Responsiveness, Initiation, Involvement, and Enjoyment [43]. Strong et al.’s study supported the hypothesis that a combination of interventions, including physical and social activities, combined with musical agency, improve attention and short-term memory [44]. Narme et al. and Wang et al. added evidence on the positive effects of music therapy on mental behavior and agitation [45, 46]. Agitation of patients was reduced by MT also in Sànchez et al.’s study [47]. Finally, Mahendran et al., Han et al., and Xue et al. pointed out the important impact that MT interventions have on cognition [48–50].
Overall, the results of these studies show that music therapy is able to enhance memory and language [36, 39], and to increase the efficacy of memantine on psychiatric symptoms and depression [42]. Furthermore, it is important to underline the improvement in cognitive functions, such as attention, memory, and executive functions, that music therapy has shown to induce [48–50].
Results of fMRI studies
The total number of participants to the present study was of 124 individuals. The data from each study is summarized in Table 2, including details on: the type of music therapy used, number of participants, frequency and duration of therapy, evaluation time frame, and cognitive tests/parameters used to measure results.
After the first investigation, [51] selected 34 subjects diagnosed with AD or posterior cortical atrophy (PCA) and 19 age-matched healthy individuals to evaluate their functional connectivity when exposed to different musical stimuli. Specifically, the objective of the study was to evaluate the networks engaged in musical semantic memory and in incidental musical episodic memory [51].
The interventions methods were exposition to two different musical stimuli (widely known tunes and unfamiliar melodies) [51] and listening to personalized music playlists [52, 53]. Satoh et al.’s intervention method was singing training, Shimizu et al.’s was Multitask Movement Music Therapy (MMT) [54, 55].
The outcome measures were evaluated before and after the task [51], and after the intervention [52–55], and consisted of the fMRI and the simultaneous administration of various questioners reported in Table 3, including the MMSE [51, 54].
Characteristics of the studies conducted with music therapy and fMRI
AD, Alzheimer’s disease; DAD, Disability Assessment for Dementia; DSMT, Digit Symbol Modalities Test; FAB, Frontal Assessment Battery; fNIRS, functional near-infrared spectroscopy; GDA, Graded Difficulty Arithmetic; GDST, Graded Difficulty Spelling Test; GNT, Graded naming test; IADL, instrumental activities of daily living; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; MMT, Multitask Movement Music Therapy; MoCA, Montreal Cognitive Assessment; NART, National Adult Reading Test; NPI, Neuropsychiatric Inventory; PCA, posterior cortical atrophy; RBMT, Rivermead Behavioral Memory Test; RCPM, Raven’s Colored Progressive Matrices; RMT, Recognition Memory Test; VOSP, Visual Object and Spatial Perception battery; WASI, Wechsler Abbreviated Scale of Intelligence; WF, word fluency; WMS-R, Wechsler Memory Scale Revised; ZBI, Zarit Burden Interview.
AD and PCA patients showed impaired functioning of the posteromedial cortical regions during incidental episodic processing of repeated melodies [51]. The activation of the inferior frontal cortex during semantic processing of familiar melodies was altered in AD patients, as well as the function of the precuneus during the first presentation of various melodies (implicit melody encoding) [51]. PCA patients were found to have an abnormal increase of the activation of the posterior cingulate cortex during the second presentation of melodies (implicit melody recollection) [51]. The right precuneus aroused when listening to previously unfamiliar melodies and the inferior frontal cortex during semantic processing of familiar melody [51]. These brain regions didn’t arouse properly in the cohort of patients with dementia [51]. Moreover, it was shown a general increase of the functional connectivity of different brain areas, such as the visual network [52], and the activation of the supplementary motor area when listening to preferred musical selections [52]. After listening to favorite musical selections, fMRI allowed to highlight an increase in brain connectivity in sensory and attentional networks that involved corticocortical and corticocerebellar connections [52].
Satoh et al. pointed out the positive effects of MT on cognition, and particularly in psychomotor speed [54]. Also, in support of this, the angular gyrus, which is an important site of multimodal sensory integration, was found to increase its activation [54]. Shimitzu et al.’s study associated the exposure to MT with improvements in functional connectivity in the prefrontal area of individuals with mild cognitive impairment (MCI) [55]. Finally, Fischer et al. confirmed the increased cognitive functioning by detecting the activation of specific regions of the brain, such as the basal ganglia and the right inferior frontal gyrus [53].
The results of the qualitative analysis on the studies taken into consideration in this review are resumed in Tables 3 and 6.
Results of EEG studies
The total number of participants to the present study was of 68 individuals. The data from each study is summarized in Table 4, including details on: the type of music therapy used, number of participants, frequency and duration of therapy, evaluation time frame, and cognitive tests/parameters used to measure results.
In Byrns et al.’s study the number of patients with cognitive decline included in the study was of 19 participants [56]. Wu et al. selected 49 patients, that were evaluated with MMSE and behavioral and psychological symptoms of dementia, and that have been inserted in three groups: a mild-to-moderate AD group (n = 17), a severe AD group (n = 16), and a control group (n = 16) [57].
Byrns et al. used EEG and other outcome measures (PANAS Scale, Cyber-sickness, and AttrakDiff 2, as well as attention and memory exercises) before and after the music stimulus [56]. Wu et al. evaluated the participants’ responses to the music stimulus before, during and after the stimulus with EEG [57].
Byrns et al. found that the emotional state of the patients examined was improved after the music stimulation [56]. More specifically, frustration and negative emotions were reduced, while memory and attention were significantly enhanced, as demonstrated by the attention and memory exercises, although a more important effect was measured in memory performances [56].
Wu et al. pointed out the effects of music stimulation on different lobes of the brain [57]. Particularly, the parietal lobe and the temporal lobe responded in a significant way in patients with mild-to-moderate dementia [57]. The parietal areas of the brain are involved in cognition, while the temporal region is important for emotion regulation [57]. Patients with severe dementia showed responses to music stimulation only in the medial temporal lobes [57]. This is thought to be due to the fact that severe AD patients have the parietal and lateral temporal lobes completely atrophied [57]. For this reason, it has been hypothesized that these individuals have a lower potential response to music therapy [57].
The results of the qualitative analysis on the studies taken into consideration in this review are resumed in Tables 4 and 7.
Characteristics of the studies conducted with music therapy and EEG
Effects of music therapy on behaviors and cognition
AD, Alzheimer’s disease; AMI, active music intervention; GMT, group music therapy; MCET, multimodal cognitive enhancement therapy; MCI, mild cognitive impairment; MSSE, Multisensory Stimulation Environment; MT, music therapy; RCS, recreational choir singing; RMI, receptive music intervention.
Effects of music therapy on brain connectivity and activation of specific areas in the brain
AD, Alzheimer’s disease; MCI, mild cognitive impairment; MMT, Multitask Movement Music Therapy; PCA, posterior cortical atrophy.
Effects of music therapy evaluated with EEG
DISCUSSION
The purpose of this study was to point out the behavioral and cognitive effects of music therapy on patients with AD dementia and with MCI. An evaluation of these effects based on neuroimaging studies that used fMRI and on EEG studies was also included in the study. From the analysis emerges that MT has many effects on different aspects of the clinical features of AD dementia; in fact, in all the studies it was found that MT seems to stabilize and to reduce neuropsychiatric symptoms, such as agitation, irritability and disinhibition. Also, it was shown that MT reduces depressive symptoms in AD patients, as well as caregivers’ stress. fMRI studies allowed to draw out conclusions on the ability of music therapy to enhance brain connectivity, and more specifically to activate areas that are involved in memory processing and cognition. EEG studies pointed out the important effects of music stimulation on cognitive functions and emotion regulation. This fact makes it possible to formulate stronger hypothesis on the ability of music therapy to impact on cognition. Unfortunately, neuroimaging studies and EEG studies on this matter are very limited; therefore, the evidence that was collected during this analysis is based on the scores of several rating scales used in evaluating the quality of life (QoL), though for a more detailed evaluation more multicentric studies led with standardized methods are needed to collect reliable data.
Overall, these studies assessed that music therapy is effective in improving psychiatric behaviors and QoL in patients with AD dementia, especially when the music therapy intervention consists of listening to personalized music pieces. Gòmez-Gallego proposes that personalized music may have a positive impact due to its mnemonic connection to life events [36]. Further studies are required to confirm this hypothesis by comparing the effects of familiar and unfamiliar music on mood and behavior.
The efficacy of music therapy on mood, behaviors, and psychiatric symptoms could be explained by the impact of listening to music on the reward system [58, 59]. In fact, studies have shown how listening to music is associated with an enhancement of the release of neurotransmitters, and more specifically dopamine, endocannabinoids, and endorphins [27, 30]. These molecules are known to impact pleasure and reward stimuli [58–61] and could thus explain the reduction of depression and neuropsychiatric symptoms, including irritability and agitation [27, 45–50].
Another interesting argument is that the association of music listening and body movements or, in general, some type of action is effective in increasing cognitive functions in these patients [36, 49]. This was shown in [36, 49] and could be attributed to a putative effect of music acting as a memory enhancer when played in the background during various activities [62]. It is worth considering that in another neurodegenerative conditions, such as Parkinson’s disease, the combination of music with rhythmic movements, as occurring in folk dance, result in improved outcome for both motor and non-motor symptoms [63].
It is also important to cite the effects demonstrated by [39] and [40] on caregivers’ stress. The relevance of this observation is of paramount importance, as caregivers working with demented subjects often find themselves surrounded by a very stressful environment, potentially backfiring on their health and quality of life [64, 65]. Music therapy could be a powerful tool, potentially able to reduce such consequences on patients’ families and healthcare staff, with an impact on multifarious aspects, which encompass affective, economic and interindividual relationships [64], with an overall fallout on society and on the general management of medical health in the population [66]. Therefore, it would be beneficial to carefully assess the positive impact of music therapy also as a tool in handling caregivers’ stress and improving familiar and social ties in the community.
The effects of music on memory and language, as well as on reflexes and attention, were already carefully investigated [39, 49–51], and received further support by other studies [36]; together, these trials proposed a possible explanation for the cognitive effects of music, suggesting that these could be related to the fact that the use of preferred musical genres might be able to stimulate autobiographical memories [36]. In consideration of the possible relevance of the therapeutic role of musical approaches, more investigations are needed to confirm and to characterize the possible impact of music therapy on cognitive impairment.
The selected fMRI and EEG studies have been taken into consideration despite the limited number and the small population analyzed, with the purpose of associating the evidence of the effects of music therapy on both behavioral and cognitive aspects with the effects on brain connectivity and brain responses, and so attempting to hypothesize a significative link between music therapy and cognitive enhancement [51]. The brain areas that were found to play a role in these results, though sparsely located in several brain areas, are largely acknowledged for their function in regulating cognitive processes [67]. These regions include the posteromedial cortical regions which, along with the posterior cingulate cortex, play a crucial role in regulating the access to the autobiographical memory [67, 68]. Furthermore, the right precuneus has been thoroughly investigated as the main brain hub which integrates within episodic memory several instances processed in parietal, occipital and temporal areas [69, 70], that become eventually activated during the listening of unfamiliar music in healthy subjects. This observation is particularly pertinent as AD patients were found to have an impaired activation of this area [44]. Moreover, it seems worth considering the possible implication of the hippocampus and of its upstream connections with temporoparietal circuits in decoding items of musical novelty [44]. Indeed, this observation could support the use of personalized music playlists which include familiar music pieces, resulting in a noticeable benefit in these patients and suggesting that it would be preferable not only to refer to the patient’s personal musical taste when planning the therapy sessions, but also to include music pieces that are connected to significant life events of the subject.
In addition to the areas mentioned, other brain networks are found to be involved in the effects of music therapy, such as the inferior frontal cortex and as the anterior frontotemporal cortical network [51], both largely acknowledged for modulating the abstract content of cognitive processes [71, 72].
Another aspect of the evaluation of musical listening is represented by the activation of the supplementary motor area when preferred musical selections are played [52]; moreover, this observation is of further relevance as this region is considered part of the networks that regulate the timetable of cognitive tasks [72].
EEG studies contribute to confirm the hypothesis of the effects of music therapy in enhancing cognitive functions. Especially Wu et al. draw out interesting conclusions on the effects of music stimulation in increasing brain activity of the parietal lobes, indispensable for memory and attention [57].
In commenting these results, it is important to mention a recent study led in post-comatose patients presenting some residual form of consciousness; listening to their favorite music was able to activate several areas, including some of the ones mentioned to have activated in cognitive impaired subjects in the present study [73]. This supports the hypothesis that music can generate an increase in brain connectivity [73]. In addition to that, it has been suggested that the functional brain architecture underlying the qualitative content of life experiences, such as the perception of sounds or colors, known in pyscho-philosophical jargon as “qualia”, may derive from the bioelectrical networking embedded in neural circuits which are plastically involved in the octave tonal structure of music perception, according to the Weber-Fechner logarithmic order [74]. Together, these observations suggest that music not only could activate or reinstate interarea connectivity, but also, that it is able to modulate a proper architecture of brain circuitries involved in temporal dynamics which supervise the access to a proper temporal frame of memory and “feelings” [5, 75].
The reason for emphasizing studies conducted with fMRI over techniques such as PET imaging is that fMRI offers unparalleled insights into minute changes in brain activity. Variations identified using PET typically emerge after significant alterations in brain activity and morphology. In contrast, the fMRI, with its sophisticated techniques and methodology, permits the examination of the finest shifts in brain functionality. It is noteworthy that the impacts of interventions like music therapy might initially manifest as microscopic changes in brain function, eventually leading to macroscopic morphological alterations.
Conclusions
This study deserves several critical observations: first, music therapy methodologies, and in general the protocols employed during these studies were neither homogeneous nor standardized; secondly, more accuracy is needed in order to get a previous frame on the effects of simple acoustic features of music played versus its semantic aspects.
Beside these critical weaknesses, this study attempts to add evidence to the efficacy of music therapy in various aspects of cognitively impaired subjects, in support to other non-drug interventions currently employed in the treatment of AD dementia. The data available in the current scientific literature is unfortunately not sufficient to draw definitive conclusions on the cognitive impact of this approach, though they seem to sustain the hypothesis that music could play a role in improving mild forms of cognitive impairment. This study highlights the interest to support new research projects conducted with neuroimaging and other combined supports (e.g., electrophysiological co-registrations) integrated with the data obtained by questionnaires that aim to assess neuropsychiatric symptoms and general cognitive functions, with the purpose of expanding the points of view on the role that music potentially deserves in the study of neurodegenerative diseases.
AUTHOR CONTRIBUTIONS
Eleonora Rossi (Conceptualization; Data curation; Formal analysis; Investigation; Project administration; Writing – original draft; Writing – review & editing); Francesco Marrosu (Visualization; Writing – original draft); Luca Saba (Conceptualization; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article.