
Abstract
Background:
Loneliness and social isolation are considered public health problems among older individuals. In addition, both increase the risk of developing cognitive impairment and dementia. The Social Loneliness construct has been proposed to refer to these harmful social interaction-related factors.
Objective:
To define the risk factors of Social Loneliness in individuals with mild cognitive impairment (MCI) and to analyze cognitive, emotional, and functional differences according to the participant’s degree of Social Loneliness.
Methods:
Through convenience sampling, 105 participants over 60 diagnosed with MCI were selected. The evaluation consisted of anamnesis and a comprehensive neuropsychological examination. The ESTE-II questionnaire was used to assess Social Loneliness and its three factors: perceived social support, social participation, and use of communication technologies. Personality was measured with the NEO-FFI questionnaire.
Results:
The predictors of the Social Loneliness factors were as follows; 1) perceived social support (R2 = 0.33): Neuroticism (β= 0.353), depression (β= 0.205), and perceived health (β= 0.133); 2) social participation (R2 = 0.24): Conscientiousness (β= –0.344) and Extraversion (β= –0.263); 3) use of communication technologies (R2 = 0.44): age (β= 0.409), type of cohabitation (β= 0.331), cognitive reserve (β= –0.303), and Conscientiousness (β= –0.247); all p < 0.05. The participants with a higher degree of Social Loneliness showed more depressive symptoms (R2 = 0.133), more memory complaints (R2 = 0.086), worse perceived health (R2 = 0.147), lower attentional performance/processing speed (R2 = 0.094), and more naming difficulties (R2 = 0.132); all p < 0.05.
Conclusions:
This research represents an advance in detecting individuals with MCI and an increased risk of developing Social Loneliness, which influences the configuration of the clinical profile of MCI.
Keywords
INTRODUCTION
Neurodegenerative diseases are the leading cause of disability in older people, Alzheimer’s disease being the most prevalent, accounting for approximately 60% of diagnoses [1]. The estimated global prevalence of dementias or major neurocognitive disorders is 82 million in 2030 and 152 million in 2050 [2].
Mild cognitive impairment (MCI) or minor neurocognitive disorder is considered a prodromal stage and less disabling than dementia [1, 3], and its early detection is relevant to start preventive treatments as quickly as possible. A large body of research has focused on the study of MCI risk factors under the premise that the etiology of this clinical profile can be as varied as its possible outcomes [4]. In addition to well-established risk factors such as genetics (e.g., presence of the APOE4 gene) [5] or vascular (e.g., arterial hypertension) [6], a close relationship has been found between the appearance of cognitive impairment and psychological factors such as mood disorders [7], stress [8], unhealthy habits [9], and even the presence of unwanted loneliness [10]. Focusing on the latter, we can define loneliness as an unpleasant feeling derived from the discrepancy between available social relationships and those desired [11], both in terms of quantity and quality [12]. In this context, it is essential to differentiate it from related, but not equivalent, factors, such as desired solitude within the framework of active and healthy aging [13], living alone or social isolation, the last being defined as the objective lack of social contacts [14]. Although it has a synergistic relationship with the feeling of loneliness [14], social isolation is not an equivalent concept. Indeed, some authors consider that the differentiation of the mentioned subjective and objective components of social relationships would be important both at a conceptual level and to establish valid conclusions that will allow the development of effective intervention strategies [14, 15].
On the one hand, social isolation is a highly prevalent problem among older individuals [16]. It is related to multiple health issues in this population, both mental (e.g., depression, cognitive impairment) [17, 18] and physical (e.g., cardiovascular disease, infectious illness) [19, 20], leading to a more rapid worsening of symptomatology in individuals with established cognitive impairment [21]. Social isolation is partly derived from factors commonly related to later phases of life, such as the loss of significant people and usual roles, or health issues, such as reduced mobility and limitations to hearing and vision [16]. In MCI patients, the risk of social isolation is increased since avoiding social engagement is recognized as a coping mechanism in this population [22], with evidence of a smaller social network and reduced community participation in these individuals compared to the general population of older adults [23]. Psychological factors also have a crucial role, with mood disorders like depression increasing the risk of social isolation in the older population [24].
On the other hand, loneliness is a highly prevalent subjective phenomenon in our environment and is considered a public health problem [25], with significant repercussions at the aging stage [26]. Among older individuals, higher levels are observed in people with MCI compared to healthy controls [27]. Various studies show a positive correlation between loneliness and physical and emotional health problems and a negative correlation with cognitive performance [28–31]. In addition, its presence could increase the risk of developing MCI or dementia in the future [10, 32] through mechanisms that are not yet clearly established. Among these, the alterations in stress responses and increased cortisol with harmful effects on brain function have been postulated [28, 33]. However, some studies show decreased cortisol levels in lonely older adults [34], existing conflicting results. Other mechanisms postulated are the presence of cardiovascular events (e.g., atherosclerosis or elevated blood pressure) or other chronic diseases like diabetes, derived from the brain dysfunction described above [35, 36], increased amyloid burden [37–39], or the presence of unhealthy habits between people suffering from loneliness and social isolation [11]. However, some authors find no evidence of loneliness as a risk factor for long-term cognitive decline [40]. In the specific field of MCI, Kwon et al. [41] found no association between cognitive performance and loneliness, although the neuropsychological evaluation consisted only of the application of screening tests. Despite the existing controversies, recent meta-analyses [42] and cross-cultural studies [43] confirm the relevance of loneliness as a possible risk factor for cognitive impairment and its association with MCI, thus justifying efforts to reduce the appearance of this feeling with a preventive purpose.
Regarding the possible risk factors of loneliness, to the best of our knowledge, there are no previous studies on the specific population of people with MCI. In the general population, similar to social isolation, sociodemographic characteristics such as advanced age, living alone, or being a woman are associated with a greater risk of experiencing loneliness [44, 45], with some studies evidencing conflicting results regarding sex and age [46, 47]. The effects often attributed to age and sex are probably not independent but derive from other variables with which they are frequently associated, such as living alone or depressive symptoms. Additionally, in a population-based study with older people from the city of Madrid, Montejo et al. [48] found that the effect size of psychological predictors like perceived mental health (R2 = 0.24) was more significant than that of classically considered objective and sociodemographic variables, such as living alone (R2 = 0.07). Other loneliness predictors and associated factors evidenced in the specific context of aging are the presence of life stressors [49], physical health problems such as chronic diseases [11], mental health disorders such as anxiety or depression [50], and psychological constructs such as personality traits [51–53].
Concerning the last factor mentioned, multiple stable character traits could increase the risk of experiencing loneliness. Buecker et al. [51], in a meta-analysis of 113 studies with individuals of different ages, studied the association between loneliness and the five personality factors according to the model of Costa and McCrae [54]. They determined that higher levels of Neuroticism and lower levels of Extraversion were associated with a higher degree of loneliness, observing significant negative relationships with Conscientiousness and Agreeableness, although of lesser magnitude. In addition, they found that age played a mediating role in the strength of the associations since traits such as Extraversion decreased in relevance at advanced ages compared to younger individuals, with no differences being observed for the rest of the traits. Hensley et al. [52, 53] found that a higher degree of Neuroticism and lower levels of Extraversion and Competence (a facet of the Conscientiousness trait) were associated with greater perceived loneliness in older individuals without cognitive impairment. On the contrary, Cacioppo et al. [55], in a 5-year longitudinal study concluded that traits such as Neuroticism do not influence the appearance of loneliness over time, so there are discrepant results.
At this point, it is clear that both social interaction-related factors, loneliness and social isolation, negatively impact older people’s physical and mental health. The Social Loneliness construct has been proposed by authors like Rubio et al. [56] to refer to the binomy loneliness/social isolation that, taken together, reflects the dissatisfaction and adaptation difficulties of older people to their social environment, characterized by changes in terms of new technologies, new forms of residence or family structures. Some authors support the convenience of studying both factors together to capture a complete picture of the individual’s social context and adaptation [57]. It is essential to clarify that the Social Loneliness concept defined here differs slightly from the concept proposed by authors like Weiss [12], which refers only to the individual’s perception of not being part of an engaging community. Through factorial analysis, Rubio et al. [56] proposed three factors as part of this Social Loneliness construct: perceived social support –closely related to the loneliness concept presented by Weiss [12]; social participation; and communication technologies use –both closely related to the concept of social isolation. From this model, they created the Social Loneliness Scale ESTE-II [56], which allows researchers to measure, both separately and in a whole way, these harmful social interaction-related factors in older people. This instrument follows the path initiated by others concerning measuring the loneliness phenomenon entirely and comprehensively, like the UCLA quantitative scales [58], SESLA-S [59], and de Jong Gierveld Loneliness Scale [60].
In conclusion, and based on the reviewed literature, the complexity of the loneliness and social isolation phenomena is evident in terms of their conceptualization, the risk factors for their appearance, and their multiple adverse effects on the aging process. Additionally, we highlight the scarcity of studies analyzing the predictive factors of both phenomena in people with MCI. Given the impossibility of extrapolating conclusions obtained from non-clinical populations to populations with mental or neurocognitive disorders, this scarcity is relevant. Likewise, there is a lack of research that addresses the association of loneliness and social isolation taken together with the configuration of MCI, analyzing their relationship with specific cognitive domains and functional or emotional aspects.
Therefore, the objectives of this study are: First, to analyze the predictive variables of subjective (perceived social support) and objective (social participation and use of communication technologies) social interaction-related factors across individuals with MCI. The hypothesis is that both sociodemographic and psychological variables will be strongly associated with them. In a complementary way, we hypothesize that psychological variables will be the most significantly associated with perceived social support and social participation. Secondly, the differences in objective (cognitive and functional performance) and subjective variables (mood, memory complaints, and perceived health) will be analyzed between patients with MCI and different degrees of Social Loneliness, as defined by Rubio et al. [56]. The hypothesis is that individuals with a higher degree of Social Loneliness will show lower cognitive and functional performance, more mood disturbances, and a more negative self-perception, translated into more subjective memory complaints and worse perceived health. That is, we expect to find differential MCI characteristics based on the Social Loneliness level.
METHOD
Participants and design
This study is part of the DECI (Digital Environments for Cognitive Inclusion) project, aimed at evaluating the effectiveness of a comprehensive home health program that combines different intervention modalities with digital support (cognitive training, physical exercise, and other healthy habits guidelines) in improving cognitive performance, functional ability, and quality of life in people with MCI. This project, in turn, is part of the Horizon 2020 plan (H2020-PHC-2014-2015/H2020-PHC-2014-single-stage), financed by the European Commission (Grant N°. 643588), and aimed at promoting active and healthy aging through information and communication technologies. In the context of the DECI project, several pilot studies have been carried out in Israel, Italy, Sweden, and Spain. The sample analyzed belongs to the pilot study conducted in Spain through the collaboration of the Getafe University Hospital and the Center for the Prevention of Cognitive Impairment (CPCI) of the Madrid City Council.
A convenience sampling was performed. Participants were initially attended at the CPCI for memory problems. During the 2-month recruitment phase, all patients diagnosed with MCI were offered to participate in the study. A total of 105 individuals interested in participating and who met the following inclusion criteria were finally selected: diagnosis of MCI (Petersen criteria) [3], over 60 years of age, absence of institutionalization, and sufficient reading and writing skills to collaborate in the general assessment. The exclusion criteria were the presence of depression, operationalized as a score greater than 6 on the 15-item Yesavage Geriatric Depression Scale [61], the presence of other severe mental disorders (e.g., alcoholism, manic-depressive psychosis, schizophrenia), present or past severe neurological diseases (e.g., Parkinson’s disease, stroke), taking psychotropic drugs (e.g., neuroleptics, anticholinesterases, benzodiazepines, antidepressants) in high doses, according to the assessment of the healthcare professional, the presence of significant sensory or motor alterations that could compromise performance of the assessment tests and the presence of any factor that could prevent full participation in the study (e.g., expected hospital admission).
Procedure
The variables of interest were measured throughout three consecutive assessment sessions. First, the participants were informed about the characteristics of the study and signed a consent form approved by the DECI ethics committee (A02/17 January 2017). Subsequently, the CPCI health personnel (3 neuropsychologists and a psychiatrist) conducted an initial interview and a comprehensive neuropsychological assessment. After this assessment, a geriatrician from the Getafe Hospital evaluated the participants at the geriatric level. However, the measures taken in this last assessment were not considered in the present study.
Assessment
The exploration of the sociodemographic variables of interest and the collection of data for the complete anamnesis of each participant was carried out through a semi-structured interview that is part of the CPCI assessment protocol.
The neuropsychological assessment was carried out by applying different tests to assess multiple cognitive domains. The Mini-Mental State Examination [62] and the 7 Minute Test [63] were used to assess general cognitive performance. Verbal and visual episodic memory was assessed using the Logical Memory Test of the Wechsler Memory Scale-III [64] and the Rey-B Complex Figure test [65], respectively. Attentional ability, processing speed, and executive functions were measured using the Trail Making Test (TMT), forms A and B [66]. Verbal fluency was assessed using the Phonological and Semantic Fluency Test [67, 68]. Naming ability by visual confrontation was measured using the Boston Naming Test [69].
The Memory Failures of Everyday questionnaire [70] was used to assess subjective memory complaints. The 15-item Yesavage Geriatric Depression Scale [61] and the Goldberg Anxiety Scale (Goldberg-A) [71] were used to measure the emotional variables. Perceived health was assessed with the Nottingham General Health questionnaire [72]. The Pfeffer Functional Activity questionnaire [73] was used to measure the functional ability of the participants. Cognitive reserve was assessed using the Rami questionnaire [74], which explores eight aspects related to reserve: the patient’s schooling, completion of training courses, parental schooling, lifetime occupation, musical training, language proficiency, reading activity, and cognitively stimulating activities performed throughout life. The score is obtained from the sum of the eight items and lies in the interval between 0 (minimum reserve) and 25 (maximum reserve). Finally, the personality profile was assessed using the Reduced Five-Factor Personality Inventory [54], which measures Neuroticism, Extraversion, Conscientiousness, Agreeableness, and Openness to experience.
The questionnaire used to assess the subjective and objective social interaction-related variables was the ESTE-II scale of Social Loneliness [56], which is composed of 15 items with three response options, defined as always (2 points), sometimes (1 point), and never (0 points). This scale, in turn, is composed of three subscales or factors. Factor 1, called perceived social support, is comprised of eight items that assess different aspects of the subjective feeling of loneliness through different questions (e.g., Do you feel lonely? Do you have friends or family when you need them? Do you have someone to talk to about your problems?). These questions are similar to those in other scales, like the de Jong Gierveld Loneliness Scale [60, 75]. Factor 2, called use of communication technologies (items 9–11), measures the individual’s use of different communication technologies like telephone or computer. Factor 3, called social participation index (items 12–15), measures the objective aspect of greater or lesser participation with people close to the individual (e.g., Do you go to a park, an association, or a retirement home where you socialize with other older people? During the week and at weekends, do other people call you to go out?). The scale’s total score is obtained through the sum of each item and is between 0 and 30 points, so a higher score implies a greater degree of Social Loneliness. This interpretation can be extended to the three subscales of the test, such that a higher score on the perceived social support subscale implies less perceived support, a higher score on the use of communication technologies subscale implies less use of these technologies, and a higher score on the social participation subscale implies less social participation by the individual. The scale has been validated in older Spanish individuals, shows an adequate internal consistency (Cronbach’s alpha = 0.72), and the three factors extracted by factorial analysis explain 42.86 % of the variance [56].
Data analyses
The statistical analyses were carried out using the SPSS (Statistical Package Social Sciences) program in its version 24, considering a significance level of p < 0.05.
The study of the association between Social Loneliness and its three factors with sociodemographic variables was performed through an analysis of variance (ANOVA), using the R2 statistic to consider the effect size (R2 0.01 = small effect, 0.06 = medium effect, 0.14 = large effect) [76]. The association between quantitative variables was analyzed using the Pearson correlation statistic. A stepwise multiple linear regression analysis was carried out to study the predictors of Social Loneliness, considering the ESTE-II global score and the three subscales partial scores as the criteria variables. It is important to emphasize that, given the transversal nature of the present study, no longitudinal or causal relationships between the variables can be established, so the term predictor refers to a cross-sectional association between predictors and criteria variables. Other authors use this terminology similarly in cross-sectional studies, as evidenced in meta-analyses on predictors of loneliness by authors such as Cohen-Mansfield et al. [77]. The R2 statistic was used to determine the proportion of variance of the criterion variable explained by each predictive model, considering the values proposed by Cohen [76]: 0.02 ‘small,’ 0.13 ‘medium,’ and 0.26 ‘large.’ The VIF statistic (variance inflation factor) was used to analyze collinearity in the regression studies. According to the Montgomery, Peck, and Vining criteria [78], it is considered that coefficients associated with the regression equation are not estimated correctly with VIF values greater than 5 due to collinearity.
The differences between the groups of participants with different degrees of Social Loneliness were analyzed using an ANOVA and an analysis of covariance (ANCOVA) when there were covariates whose influence on the dependent variable was interesting to isolate. In these last two cases, the effect sizes were determined with the R2 statistic, following the considerations of Cohen [76]. Post-hoc analyses were performed using the LSD statistic (least significant difference), considering a significance level of p < 0.05. In certain variables, there were missing cases corresponding to participants who did not complete all assessment tests, in which case, they were eliminated from the specific analysis.
RESULTS
Bivariate study: Association of social loneliness and its factors with qualitative and quantitative variables
First, the association of Social Loneliness with sociodemographic variables was studied. For this, an ANOVA was performed, considering the sociodemographic variables as independent variables and the different scores in the ESTE-II as dependent variables, both from the global test and from the three factors. The results of this analysis and the sociodemographic characteristics of the sample are detailed in Table 1.
Socio-demographic characteristics of the sample, number of participants and percentage of the total sample. ANOVA results: mean, standard deviation, F statistic and effect size of Social Loneliness and the three factors
*p < 0.05; **p < 0.01. ANOVA, Analysis of Variance; SD, Standard Deviation; R2, effect size; ESTE-II, Social Loneliness Scale; Factor 1, perceived social support; Factor 2, use of communication technologies; Factor 3, social participation index.
The group of older individuals scored higher on the Social Loneliness scale and on the subscales of perceived social support (that is, on average, they perceived less social support than younger individuals) and use of communication technologies (that is, they reported using these technologies less). However, age was not significantly associated with the social participation subscale. Regarding the gender variable, women showed a higher mean score in Social Loneliness and the perceived social support subscale, with no significant differences between men and women in the use of communication technologies and social participation subscales. About the educational level, a lower mean score was observed in the use of communication technology subscale in the higher-level group (that is, they reported using these technologies more). Lastly, individuals who live with others showed a higher mean score on the Social Loneliness scale, as well as on the social participation subscale (that is, they reported less participation) than individuals who live alone.
Next, the association of Social Loneliness (global ESTE-II and subscales) with the quantitative variables of interest was studied. The results of the Pearson correlations are shown in Table 2.
Association among Social Loneliness (total and factors) and quantitative variables
*p < 0.05; **p < 0.01; ***p < 0.001. GDS, Geriatric Depression Scale; Goldberg-A, Goldberg Anxiety scale; FAQ, Functional Activities Questionnaire; NEO-FFI, Reduced Five-Factor Personality Inventory; ESTE-II, Social Loneliness Scale; Factor 1, perceived social support; Factor 2, use of communication technologies; Factor 3, social participation index. R2, percentage of variance explained by predictors. VIF, variance inflation factor.
The direction of the correlations shows us that higher scores on the tests that measure anxiety, depression, and perceived health were related to higher scores on the Social Loneliness global scale and the perceived social support and social participation subscales. In contrast, functionality was not associated with any Social Loneliness factors studied. Regarding cognitive reserve, it is observed that a lower score on the Rami questionnaire was associated with a higher score on the use of communication technologies subscale (this indicates a lower reported use of these technologies). Finally, Conscientiousness correlated negatively with all the scales, Extraversion correlated negatively with social participation, and Neuroticism showed a positive correlation mainly with the Social Loneliness global scale and the perceived social support subscale.
Multivariate study: Predictors of social loneliness
A stepwise multiple linear regression analysis was conducted to study the predictors of Social Loneliness and its three factors. Considering the results of the previous bivariate study, sociodemographic variables (age, gender, and type of cohabitation), cognitive reserve, health variables (anxiety, depression, and perceived health), and personality variables (Neuroticism, Extraversion, Conscientiousness, Agreeableness, and Openness to experience) were included as possible predictors.
The final models obtained are detailed in Table 3.
Predictors of Social Loneliness and its factors. Multiple Lineal Regression. Final models
All models: p < 0.001. ESTE-II, Social Loneliness Scale; Factor 1, perceived social support; Factor 2, use of communication technologies; Factor 3, social participation index. R2, percentage of variance explained by predictors.
In all models, the value of the Durbin-Watson statistic was close to 2 (for Social Loneliness and Factor 1, 2, and 3 = 1.786, 2.173, 2.042, and 2.336 respectively), which indicates that the residuals are not correlated. Similarly, in all models, the VIF value was less than 5 (all values between 1.005 and 1.904), which implies a lack of multicollinearity between predictors.
The Conscientiousness trait stood out as the most important predictor of both Social Loneliness and social participation, being the fourth most relevant predictor of the use of communication technologies. Neuroticism was the most relevant predictor of perceived social support. Sociodemographic variables such as age and type of cohabitation, together with cognitive reserve, were particularly relevant as predictors of the use of communication technologies.
Differences according to the degree of social loneliness
Finally, an ANOVA was performed to study the differences in the variables of interest between participants with MCI and different degrees of Social Loneliness, considering the covariate age, given the close relationship between age and cognitive, emotional, and functional variables. For this purpose, the sample was subdivided into three groups based on the ESTE-II score, considering the mean score and the standard deviation (SD). The first group consisted of participants with a low level of Social Loneliness, with scores ranging between 0 and 6 (n = 14; scores below the mean minus one SD). The second group comprised those with a medium level of Social Loneliness, with scores between 7 and 14 (n = 78; scores in the range between the mean minus one SD and the mean plus one SD). The third group had a high level of Social Loneliness, with scores between 15 and 20 (n = 12; scores above the mean plus one SD). It should be noted that the maximum score obtained in this sample was 20 points.
Figures 1 and 2 show the results of this analysis and the graphical representation of the mean scores and SDs of the three groups of individuals in each of the variables in which statistically significant differences were observed.
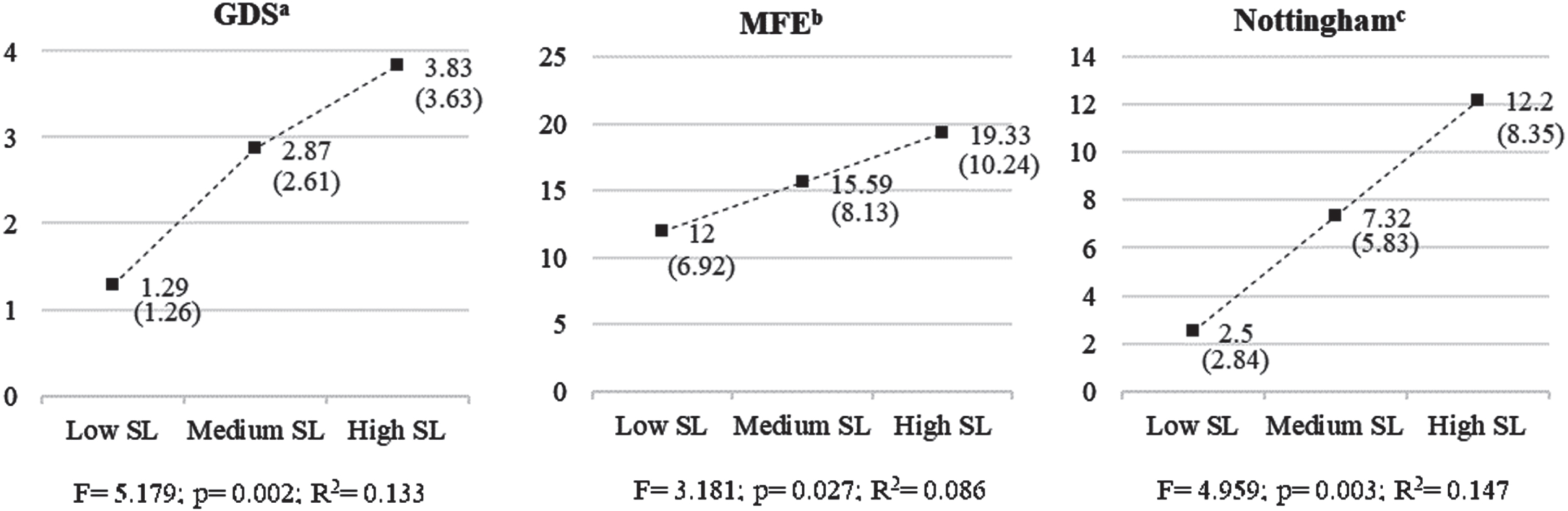
Statistically significant differences in subjective variables between groups with different degrees of Social Loneliness. Means (standard deviations) and ANCOVA results. SL, Social Loneliness. aPost-hoc LSD (least significant difference): low SL < medium SL, p = 0.039; low SL < high SL, p = 0.015. bPost-hoc LSD: low SL < high SL, p = 0.026. cPost-hoc LSD: low SL < medium SL, p = 0.010; low SL < high SL, p = 0.000; medium SL < high SL, p = 0.016. GDS, Geriatric Depression Scale; MFE, Memory Failures of Everyday Questionnaire.

Statistically significant differences in objective variables between groups with different degrees of Social Loneliness. Means (standard deviations) and ANCOVA results. * covariable “age” is the significant one. SL, Social Loneliness. aPost-hoc LSD (least significant difference): low SL < high SL, p = 0.005; medium SL < high SL, p = 0.005. bPost-hoc LSD: no significant differences were found between the pairs of means. cPost-hoc LSD: no significant differences were found between the pairs of means. dPost-hoc LSD: low SL > medium SL, p = 0.040; low SL > high SL, p = 0.003. TMT, Trail Making Test.
Figure 1 shows how the individuals with a low level of Social Loneliness showed a significantly lower mean score in the tests that assess depressive symptoms, memory complaints, and perceived health compared to individuals with medium and high levels. However, concerning the last two groups mentioned, the post-hoc analyses revealed significant differences only in the mean score of the Nottingham test. Similarly, Fig. 2 shows a shorter TMT-A execution time in the groups of individuals with a low and medium level of Social Loneliness. On the other hand, there was a higher score on the Boston test in the group of individuals with a low level of Social Loneliness compared to individuals with medium and high levels. Finally, the differences observed in the mean execution time in the TMT-B and the copy of the Rey-B figure were attributable to age (TMT-B: F = 16.702; p = 0.000; R2 = 0.142. Rey-B copy time: F = 6.462; p = 0.013; R2 = 0.066) and not to the degree of Social Loneliness (TMT-B: F = 1.473; p = 0.234; R2 = 0.028. Rey-B copy time: F = 0.763; p = 0.469; R2 = 0.016), as evidenced in the analysis of covariance.
Table 4 shows the variables in which no statistically significant differences were observed based on the degree of participant’s Social Loneliness.
Variables in which no differences were found between groups with different degrees of Social Loneliness. Means (standard deviations) and ANCOVA results
SL, Social Loneliness; M, mean; SD, standard deviation; Goldberg-A, Goldberg Anxiety scale; MMSE, Mini-Mental State Examination; WMS, Wechsler Memory Scale; LM, logical memory; FAQ, Functional Activities Questionnaire.
DISCUSSION
The objective of the present research was, firstly, to study the predictors of subjective (perceived social support) and objective (social participation and use of communication technologies) Social Loneliness factors in individuals with MCI. The results confirm the proposed hypothesis, as both the sociodemographic and psychological variables are significant predictors of the different factors of Social Loneliness studied. In addition, psychological variables, such as personality traits, are the most relevant when it comes to predicting social participation and perceived social support. Secondly, the association of Social Loneliness with the configuration of the clinical profile of the participants was analyzed. The initial hypothesis is confirmed, observing differential characteristics depending on the level of Social Loneliness. Individuals with a higher degree of Social Loneliness show more depressive symptoms and memory complaints, worse perceived health, lower attentional/processing speed performance, and more naming difficulties than individuals with a lower degree.
Predictors of social loneliness in individuals with MCI
Sociodemographic variables, cognitive reserve, and functionality
The association between loneliness and multiple sociodemographic variables is in line with the findings of other authors [44–46, 79]. The older and female participants in the sample showed a greater degree of Social Loneliness and perceived less social support, confirming the relevance of these factors in individuals with MCI, in congruence with other research on older people without cognitive impairment [45, 80].
However, in the multivariate study, sociodemographic variables lose significance, mainly gender, with personality variables becoming more relevant in predicting the different factors of Social Loneliness. Nevertheless, certain sociodemographic factors maintain a determining weight as predictors regarding the use of communication technologies. It is observed how older age, less cognitive reserve, and living with others are associated with less use of these technologies. This evidence would be in line with the studies that show technology underuse by individuals with a lower educational level and older ages [80, 81]. Given the evidence on the protective role of using these technologies in loneliness [82], these results support encouraging their use among older individuals with MCI and lower cognitive reserve, which is congruent with digital literacy plans for older adults [83].
On the other hand, although living alone is a documented risk factor [57], in this sample, it can be considered a protective factor regarding both global Social Loneliness and the use of communication technologies. Authors such as Hawkley and Kocherginsky [80] suggest that among older adults who live alone, there could be a higher level of socialization that would offset the adverse effects of an “a priori” unfavorable cohabitation status, which could lead to better mental health and a lower feeling of loneliness. Given the results obtained, this could be extended to individuals with MCI.
Finally, it is worth mentioning that the functional ability measured with the Pfeffer questionnaire is not associated with Social Loneliness or any of its factors individually. However, among the defining characteristics of MCI is the preservation to a great extent of functionality, which would explain the observed findings.
Personality variables
Stable personality traits have been shown in the literature as crucial factors in loneliness among older adults without cognitive impairments. Specifically, some studies show that high levels of Neuroticism and low levels of Extraversion increase the risk of loneliness appearing [52, 53]. Additionally, a recent meta-analysis evidenced a strong loneliness association with Neuroticism and Extraversion and a significant but weaker association with traits like Conscientiousness and Agreeableness [51]. The results of the present study confirm the relevance of this personality pattern among older individuals with MCI but also provide relevant data regarding the differential role of specific traits in objective and subjective factors of Social Loneliness. To our knowledge, this last aspect has not yet been explored in the literature.
Neuroticism is the main predictor of the subjective component of Social Loneliness, so a higher level of this factor is associated with a lower perceived social support. We can hypothesize a possible influence of specific characteristics of this trait (e.g., lower stress tolerance or greater emotional instability) on interpersonal interactions. Studies show an association between Neuroticism and a greater sensitivity to social rejection [84], greater reactivity to social stressors [85], and more dysfunctional interpersonal behavior that could be associated with greater dissatisfaction about relationships with others [86]. All this could contribute to the development of an exacerbated feeling of loneliness.
Conscientiousness, characterized by the tendency towards self-discipline, organization, and impulse control [54], is one of the main predictors of Social Loneliness and its non-subjective factors, that is, social participation and the use of communication technologies. Analyzing the sign of the associations, we hypothesize that individuals with a higher level of this trait will likely maintain social contacts to a greater extent [87], which could be extended to the higher use of technologies that favor communication. Consequently, they would have a lower risk of feeling lonely. However, the association with Social Loneliness seems to be explained by the predictive power of Conscientiousness on the more objective components of Social Loneliness analyzed. These results are congruent with those observed in other investigations. Hensley et al. [53] found that the Competence facet of the Conscientiousness trait significantly predicts loneliness in older people (β= –0.29). The sign of the relationship between the variables was the same as that observed in the present study, such that a lower level of Competence was associated with a higher level of loneliness.
Concerning Extraversion, a factor characterized by a tendency to seek and enjoy interpersonal relationships [54], is related to greater social participation being one of its main predictors in the regression analysis, in line with other findings in the literature in individuals without cognitive impairment [88, 89]. The fact that both Extraversion and Conscientiousness are strongly associated with social participation would be especially relevant in people with MCI since it supports the hypothesis that factors that protect against cognitive impairment and that enhance cognitive reserve, such as frequent interpersonal relationships [90], are significantly related to stable personality traits.
Agreeableness and Openness are the traits that show a lower relationship with Social Loneliness and its different factors in the bivariate study, highlighting only the negative association between Agreeableness and Social Loneliness. In the multivariate study, their significance is minimal, and they are not considered predictors. These results would be in line with findings such as those of Buecker et al. [51], in which it is observed that Agreeableness shows a significant but weak association with loneliness compared to the other traits, with no significant association with Openness.
Characterization of MCI based on the degree of social loneliness
The ESTE-II Social Loneliness scale utilized in the present investigation allows for the study of the association of subjective and objective social interaction-related harmful factors, taken together, with the clinical profile of patients with MCI. We observe that the group of patients with MCI that reported greater Social Loneliness shows a characteristic clinical profile at multiple levels, significantly differentiating them from those with less Social Loneliness. From the cognitive point of view, they present a lower mean performance in domains such as attention and information processing speed (TMT-A), results consistent with those found by authors such as O’Luanaigh et al. [91] or Gow et al. [92] among the general population of older people. There is also evidence of lower performance in linguistic processes such as access to the lexicon (Boston test), in line with the results of Shankar et al. [18] with a non-clinical population. In contrast, Kwon et al. [41] found no association between cognitive performance and loneliness in individuals with MCI. However, it should be noted that the type of screening assessment used in this study limits the scope of the conclusions. In line with our results, social isolation showed a negative association with attentional and linguistic task performance in other studies within the older general population [10].
The explanatory mechanisms of the negative influence of loneliness and social isolation on cognition are multiple. Among these, there is an alteration in the organism’s stress responses, materializing in prolonged activation of the Hypothalamic-Pituitary-Adrenal axis and higher cortisol levels in individuals with greater loneliness [93] and social isolation [94], which could be associated with cellular damage at the brain level and worsening of cognitive function [95]. Nevertheless, other authors found contrary results, evidencing lower cortisol levels in lonely older people [34]. Other mechanisms related to stress are the dysregulation of inflammatory responses in individuals who feel lonely [96], a relevant aspect if we consider that the alteration of inflammatory processes is involved in pathologies such as Alzheimer’s disease and other dementias [97]. Regarding Alzheimer’s biomarkers, an increased amyloid burden in lonely older people has been reported [37, 39]. Furthermore, behavioral aspects like unhealthy habits (e.g., smoking, absence of exercise routines) or the lack of daily social stimulation in older individuals with loneliness and social isolation have been proposed as possible mechanisms [11]. However, not all the cognitive domains evaluated seem negatively influenced by Social Loneliness. The lower performance in tests that measure executive processes (TMT-B) or visual-constructive speed (Rey-copy time) in individuals with greater Social Loneliness seems to be mainly influenced by age, as shown by the analysis of covariance. In addition, no group differences are observed in tests that evaluate visual and verbal episodic memory processes or amplitude and attentional control. The absence of an association between memory or executive functions with loneliness and social isolation is consistent with studies such as that of Schnittger et al. [98] and Lara et al. [10]. However, other authors show contrary results [91, 92], and there is no agreement on this matter.
Additionally, patients with MCI and greater Social Loneliness show specific characteristics in subjective variables. They exhibit a more significant number of depressive symptoms, a greater number of subjective memory complaints, and a lower perceived health, which confirms the hypothesis initially raised, evidencing a more negative self-perception in this group of individuals. A bidirectional relationship between mood and Social Loneliness could be considered, such that a higher social isolation and feeling of loneliness could lead to depressive symptoms, an interpretation consistent with longitudinal studies that show how loneliness predicts depression [99, 100] and with studies that link depression with a low level of social participation [17]. In turn, a depressed mood would negatively influence the perception of the individual’s ties and the predisposition to begin social contacts [24, 101].
Regarding memory complaints, some studies have documented their relationship with loneliness in the general population of older people [102–104]. We can hypothesize the existence of several mechanisms underlying this association: On the one hand, at the physiological level, a relationship has been found between loneliness and increased activity of the hypothalamic-pituitary-adrenal axis, as well as greater hypervigilance towards external threats [33]. This fact could contribute to a worsening of attentional processes that are already altered in patients with MCI in the sample, which could contribute towards an increase in the frequency of daily forgetfulness. The hypothesis would be reinforced by the results of the present study, which show lower attentional performance in the group of individuals with a higher degree of Social Loneliness. On the other hand, a relationship between social isolation, loneliness and a lower self-concept has been documented [55, 105], which could increase self-monitoring and self-criticism towards one’s daily performance [106], manifesting as a greater number of memory complaints.
Finally, the mechanisms that explain the association between perceived health with loneliness and social isolation have not been clearly established to date, which would require further investigation. However, a two-way process could again be considered through which the perception of worse health by individuals would have an objective (more physical and mental health problems) and subjective (worse associated mood) basis, which could be related to a higher feeling of loneliness and social isolation in these individuals [16, 24]. In turn, the depressive mood associated with loneliness [99] and social isolation [17] could impact individuals’ perceived health.
In summary, these results support the hypothesis that Social Loneliness, conceptualized as the concurrency of subjective and objective social interaction factors that reflect the dissatisfaction and adaptation difficulties of older people to their social environment, is a risk factor that could be associated with the very configuration of the clinical profile of individuals with MCI.
Limitations
Firstly, the incidental sampling affects the generalization of the results, limiting them to the individuals of the sample studied, that is, volunteer older people with MCI who attend a center to prevent cognitive impairment. On the other hand, among the risk factors for loneliness and social isolation evidenced in the literature, there are multiple variables associated with aging that have not been analyzed in this study, such as sensory alterations [107], life stressors [49], or physical health problems [11], which would aid to understand the percentage of Social Loneliness variance not explained by the predictive models obtained. In future research, it would be relevant to analyze whether the influence of Social Loneliness in the configuration of MCI is due to mediational risk variables, such as unhealthy habits among individuals with higher social isolation and greater reported loneliness, as some studies point out [9]. Finally, the cross-sectional nature of this research limits the conclusions that could be established in a longitudinal study. For example, it is not possible to determine if the health status of the participants is a consequence, a cause, or just a correlate of Social Loneliness. In this sense, it would be interesting to propose a long-term follow-up of Social Loneliness, its relationship with personality traits, and its effects on the clinical profile of the patients. This study has already begun at the CPCI.
Conclusions
The present study represents an advance in detecting individuals with MCI and an increased risk of developing unwanted loneliness and social isolation. Moreover, these results show that Social Loneliness understood as a binomial of loneliness/social isolation, is a variable that can influence the very configuration of the clinical profile of MCI. Therefore, in preventing cognitive impairment protocols, it is essential to assess both loneliness and social isolation and intervene directly in them, complementary to the rest of the non-pharmacological strategies traditionally implemented, such as behavioral-cognitive interventions or the establishment of healthy habits.
Additionally, it is convenient to differentiate between subjective loneliness or perceived social support from the objective reality of a greater or lesser degree of social participation. Both variables show a synergistic relationship. However, as observed in the present study, their predictive personality factors are different; therefore, the potential approach should also differ.
In short, as authors such as Forjaz et al. suggest [25], the health effects of unwanted loneliness and social isolation are comparable to those of obesity, physical inactivity, or tobacco use, three of the health problems that entail the most health expenditure. This reality highlights the importance of considering these risk factors in general health action protocols and preventing cognitive impairment.
Footnotes
ACKNOWLEDGMENTS
The authors are grateful to the patients and families for supporting our research. We want to thank Elena Iuga for her assistance with participant testing. Finally, the authors wish to acknowledge the CPCI staff for their precious contribution.
FUNDING
This work was partially financed by the European Commission (Grant N°. 643588).
CONFLICT OF INTEREST
The authors have no conflict of interest to declare.
DATA AVAILABILITY
The data that support the findings of this study are available from the corresponding author on reasonable request.