
Abstract
Background:
Mild cognitive impairment (MCI) is considered a prodromal state of dementia. Abnormal values of cerebrospinal fluid Alzheimer’s disease biomarkers (CSF-AD-b) have been associated with a higher risk of conversion to dementia (due to Alzheimer’s disease), but studies evaluating the ability of Montreal Cognitive Assessment (MoCA) in this task are lacking.
Objective:
This study aims to investigate the relationship between MoCA and CSF-AD-b, as well as the ability of those tools to predict conversion to dementia.
Methods:
Taking advantage of our MCI cohort with biological characterization on longitudinal follow-up (180 patients followed for 62.6 months during which 41.3% converted), we computed MoCA and MMSE z-scores, using Portuguese normative data. The performance in MoCA z-score was correlated with CSF-AD-b and the relative time to conversion and risk according to baseline characteristics were analyzed using Kaplan-Meier analysis and Cox regression models.
Results:
MoCA z-scores were correlated with Aβ42 (p = 0.026), t-tau (p = 0.033), and p-tau (p = 0.01). Impaired MMSE (p < 0.001) and MoCA z-scores (p = 0.019), decreased Aβ42 (p < 0.001) and increased t-tau (p < 0.001) and p-tau (p < 0.001) were associated with shorter estimated time of conversion. Aβ42 (p < 0.001) and MMSE z-scores (p = 0.029) were independent predictors of conversion. For those with at least 9 years of education, MoCA z-score (p = 0.004) (but not MMSE) was an independent predictor of conversion as well as Aβ42.
Conclusions:
This study confirms the role of CSF-AD-b, namely Aβ42, in predicting conversion from MCI to dementia and suggests the utility of MoCA in predicting conversion in highly educated subjects, supporting its use in the evaluation of MCI patients.
Keywords
INTRODUCTION
Mild cognitive impairment (MCI) is defined as an intermediate stage between healthy aging and dementia. Despite being recognized as a prodromal phase of dementia, not all those identified will develop it [1]. Depending on the clinical setting, a proportion of these individuals has cognitive decline due to other causes than neurodegeneration [1] and may remain cognitively stable or even revert to normal [2, 3]. In a memory clinical setting, studies have shown an annual conversion rate from MCI to dementia around 10–15% [4, 5] with MCI non-progressors even after 10 years of follow-up [6, 7].
Since the introduction of the concept of MCI, predictors of conversion to dementia have been intensively investigated [8]. In patients with MCI, cerebrospinal (CSF) Alzheimer’s disease (AD) biomarkers [amyloid β1-42 (Aβ42), total tau (t-tau), and phosphorylated tau (p-tau)] can identify patients in risk of progression to AD dementia [9–12]. Neuropsychological measures have also been suggested as good predictors of conversion from MCI to AD dementia [9, 14]. Although CSF biomarkers and neuropsychological measures may have a comparable accuracy [15], combining them may increase the prediction ability [15, 16].
The Montreal Cognitive Assessment (MoCA) is a 10-min neuropsychological test with a maximum score of 30 points that assesses eight cognitive domains: executive functions, visuospatial abilities, short-term memory, language, attention, concentration, working memory, and temporal and spatial orientation. It was first designed as a cognitive screening tool to assist physicians in detecting MCI [17]. This test was already adapted and validated in multiple countries, including for Portuguese population [18], and due to considerable differences in education level between original study and Portuguese population, a normative study was performed with cut-offs calculated and stratified according to the different age and educational levels [19].
Identifying individuals with MCI at higher risk of conversion to dementia is of utmost importance not only to clinicians but also for patients and their families. Besides allowing an accurate selection of patients to enroll disease modifying therapeutic trials and providing an appropriate allocation of early treatment when these drugs are approved, it empowers patients and their families to prepare for the future.
To our knowledge, only few studies have evaluated MoCA’s ability to predict conversion from MCI to dementia [20, 21] and no previous studies have evaluated the predictive value of MoCA in patients with known CSF biomarkers in MCI condition. This study aims to assess the relationship between the performance in MoCA and CSF biomarkers, as well as MoCA’s ability to predict conversion to dementia in individuals with MCI.
METHODS
Subjects and procedures
We included patients from a cohort of MCI patients with CSF AD biomarkers assessment longitudinally followed at the Dementia Clinic, Neurology Department of Coimbra University Hospital Centre, Portugal. This cohort included 180 patients that were followed during 62.6±42.0 months, 41.3% of which converted to dementia: 63 to AD, 2 to Lewy body dementia, 6 to vascular dementia, 5 to frontotemporal dementia.
As previously published [22], at baseline, all patients undergo a thorough diagnostic investigation including standard clinical evaluation, neuropsychological assessment, blood analysis (including complete blood count, chemistry profile, thyroid function, vitamin B12, folic acid), apolipoprotein E (APOE) genotyping, CSF analysis (including cytochemical analysis and AD biomarkers), and imaging studies –structural [brain computed tomography (CT) or magnetic resonance imaging (MRI)] and/or functional [single-photon emission computed tomography or Pittsburgh compound B positron emission tomography (PiB-PET)].
Additionally, all patients undergo longitudinal assessment with a biannual clinical and an annual neuropsychological evaluation to detect objective evidence of progressive decline and establish a conversion to dementia.
Patient files were reviewed and demographic, neuropsychological, laboratorial, and genetic variables were collected.
Neuropsychological baseline assessment and classification
At baseline, each patient was submitted to a structured clinical interview, physical and neurological examination performed by a neurologist, followed by a comprehensive and holistic cognitive, functional, and psychological evaluation carried out by a team of trained neuropsychologists, comprising a standard battery of tests and scales, adapted, and validated to the Portuguese population. Age at onset of symptoms was estimated from subject and caregiver information using a standard questionnaire, as well as family history. The assessment battery included: cognitive instruments, including the Mini-Mental State Examination (MMSE) [23], MoCA [24], the Alzheimer Disease Assessment Scale-Cognitive (ADAS-Cog) [25], and the Battery of Lisbon for Assessment of Dementia [26]; staging scales, including the Clinical Dementia Rating (CDR) [27] for global staging, and the Disability Assessment for Dementia [28] and the Activities of Daily Living [29] for functional status assessment; and psychiatry scales, including the Neuropsychiatric Inventory [30] to assess concomitant psychiatry disorders and the Geriatric Depression Scale [31] to exclude major depression.
MCI diagnosis was established by a multidisciplinary team based on this initial investigation and in accordance with the criteria defined by Petersen et al. [1], as the following: a subjective complaint of cognitive decline (reported by the subject or an informant); objective cognitive impairment (assessed by the previously described comprehensive neuropsychological battery); preserved independence in functional abilities (confirmed by aforementioned functional assessment scales); and absence of dementia (established by the score of 0.5 on CDR global scale).
Because in this study MMSE and MoCA were the focus of investigation and to obviate circularity, its results were not considered for the clinical classification. Moreover, considering the verified effect of age and education on MoCA and MMSE performances, z-scores were obtained following Portuguese normative data. [19, 23] Z-score was calculated by subtracting tests scores from the reference mean and dividing it by the standard deviation.
Follow-up assessment and conversion
Longitudinal assessment comprised biannual clinical observation and annual cognitive and functional reassessment to detect progression to dementia. Annual reassessment included a brief neuropsychological reassessment with MMSE, MoCA, ADAS-Cog, and the CDR. Conversion to dementia was established according to the Diagnostic and Statistical Manual of Mental Disorders V [32] supported by switching in CDR global rating to at least 1 confirming loss of autonomy. Dementia subtype classification was done according to the recommendations from the respective international working groups [33–36]. Follow-up time was considered from the date of baseline assessment until the last clinical and neuropsychological evaluation for non-converters or until conversion for converters.
Biomarkers assessment
For APOE genotyping, DNA was isolated from whole EDTA-blood using a commercial kit (Roche Diagnostics GmbH, Manheim, Germany) and APOE genotype was determined by polymerase chain reaction-restriction fragment length polymorphisms assay [37]. CSF was obtained by lumbar puncture and biomarkers (Aβ42, t-tau, and p-tau) measurements were performed as previously reported by Baldeiras et al. [22] Briefly, CSF samples were collected in sterile polypropylene tubes, immediately centrifuged at 1,800 g for 10 min at 4°C, aliquoted into polypropylene tubes and stored at –80°C until analysis. CSF Aβ42, t-Tau, and p-Tau were measured separately by commercially available ELISA kits (Innotest, Fujirebio, Japan). Pre-analytical and analytical procedures were done in accordance with the Alzheimer’s Association guidelines for CSF biomarkers determination. External quality control of the assays was performed under the scope of the Alzheimer’s Association quality control program for CSF biomarkers [38]. CSF biomarkers were classified as normal/abnormal according to previously reported laboratory reference values [39].
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics software version 28. Subjects were divided into two groups: those who progressed to dementia (converters) and those who did not progress to dementia (non-converters). Normality was ascertained using the Kolmogorov-Smirnov test. Categorical variables are represented using frequencies and were compared through chi-square tests. Ordinal or discrete variables are reported as means as they are better perceived but were studied using median values and were compared through Mann-Whitney U tests. For further analysis, MMSE and MoCA z-scores, instead of absolute values, were used. Correlations between MoCA z-scores and CSF biomarkers were measured using Spearman correlation. Kaplan-Meier survival analysis was used to assess the rates of conversion to dementia in the different MCI groups according to their baseline characteristics. To assess for independent predictors of conversion, a Cox regression was performed, adjusted for the collected variables preconsidered to be predictors of dementia (age at onset, baseline MMSE z-score, APOE genotype, and CSF biomarkers levels) and the studied variable (baseline MoCA z-score). Considering the relevance of educational level in MoCA performance, we proceeded to a subsequent analysis organized by education levels (4 –primary school, 5-6 –2nd cycle, 7-9 –3rd cycle, 10-12 –high school,≥13 –university school). All the assumptions of these models were verified.
Ethics
The present research complied with the ethical guidelines for human experimentation stated in the Declaration of Helsinki and was approved by the Ethics Board of Coimbra University Hospital Centre. An informed consent was obtained from all the participants after the aims and procedures of investigation were fully explained by a member of the study group.
RESULTS
Baseline characteristics of participants by cognitive status at follow-up (converters and non-converters) are reported in Table 1. Individuals who developed dementia were older, had a lower baseline MMSE and MoCA scores and z-scores, and lower CSF levels of Aβ42 and higher levels of t-tau and p-tau. Converters carried APOE ɛ4 alleles more frequently. They did not differ in sex, family history, and education. Concerning time of follow-up, non-converters had a higher follow-up time (Table 1).
Demographic and clinical data of patients by cognitive status at follow-up (converters and non-converters)
Bold data indicates p < 0.05. LP, lumbar puncture; SD, standard deviation; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; APOE, apolipoprotein E; CSF, cerebrospinal fluid; Aβ42, amyloid β1-42; P-tau, phosphorylated tau; T-tau, total tau; A+, decreased CSF amyloid-β; T+, increased CSF hyperphosphorylated tau; N+, increased CSF total tau.
MoCA z-scores were significantly correlated with CSF Aβ42 (r = 0.167, p = 0.026), t-tau (r = –0.159, p = 0.033), and p-tau (r = –0.191, p = 0.01).
In Kaplan-Meier analysis, carrying an APOE ɛ4 allele, having a MMSE or MoCA z-score ≤ –1.5 and having decreased CSF Aβ42 or increased CSF t-tau and p-tau according to laboratory reference values was associated with a lower estimated time of conversion (Table 2). Figure 1 illustrates Kaplan-Meier curves according to MoCA z-score.
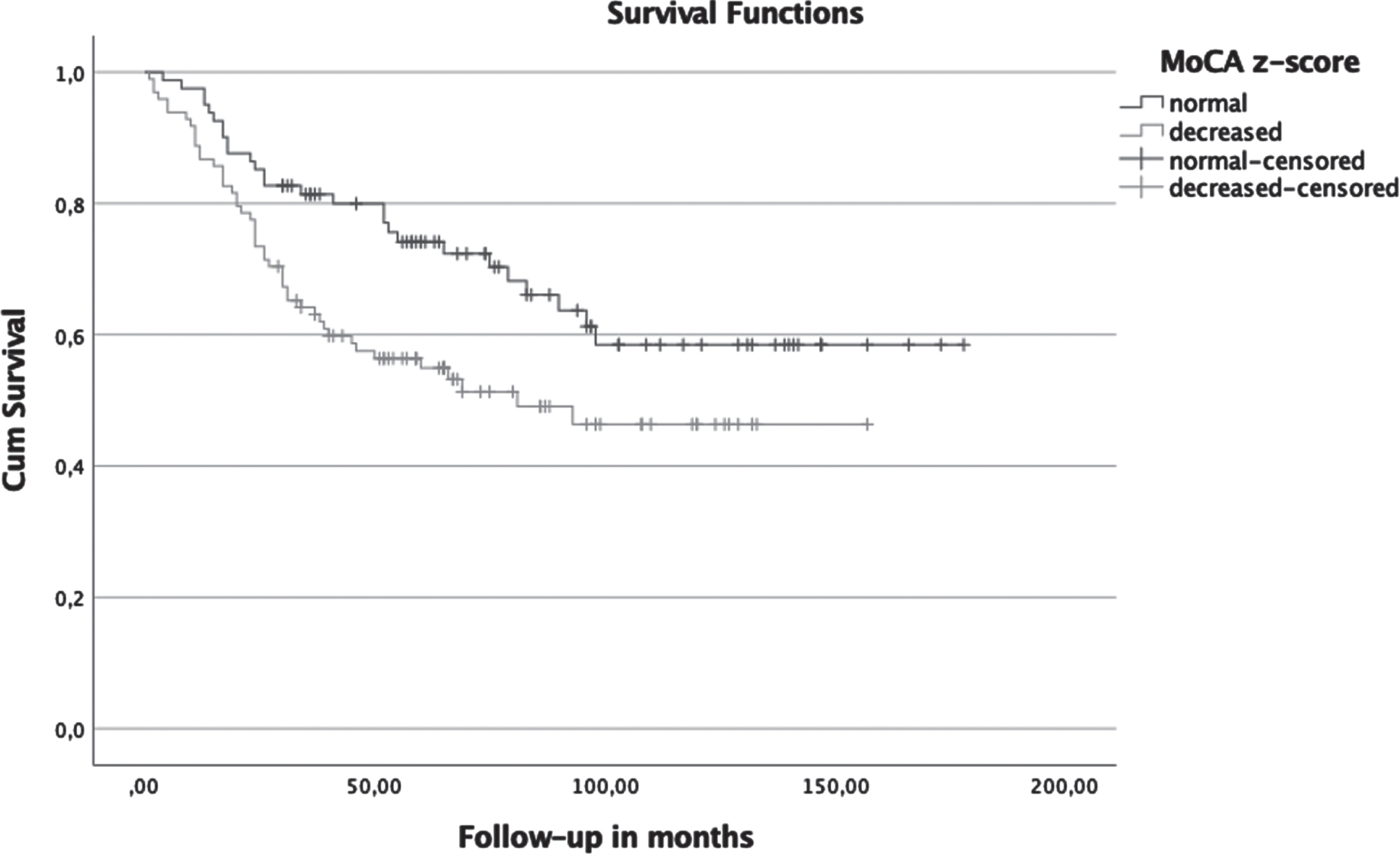
Kaplan-Meier curves according to MoCA z-score –normal (> –1.5) or decreased (≤ –1.5).
Kaplan-Meier analysis
Bold data indicates p < 0.05. †≤ – 1.5 (according to normative data for Portuguese population). †† according to laboratory reference values. SD, standard deviation; HR, hazard ratio; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; APOE, apolipoprotein E; CSF, cerebrospinal fluid; Aβ42, amyloid β1-42; T-tau, total tau; P-tau, phosphorylated tau.
In Cox regression models with potential confounding variables taken into account, including age at onset, baseline MMSE z-score, APOE genotype, and CSF biomarkers levels, we found that higher age at onset (HR = 1.057, 95% CI = [1.024, 1.092], p < 0.001), lower baseline MMSE z-score (HR = 0.837, 95% CI = [0.713, 0.982], p = 0.029), and lower CSF Aβ42 (HR = 0.998, 95% CI = [0.997, 0.999], p < 0.001), but not MoCA, were significant independent predictors of conversion (Table 3).
Cox regression results (-2log likelihood = 601.076, χ-squared = 115.922, p < 0.001, degrees of freedom (df) = 7)
Bold data indicates p < 0.05. HR, hazard ratio; CI, confidence interval; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; APOE, apolipoprotein E; CSF, cerebrospinal fluid; Aβ42, amyloid β1-42; T-tau, total tau; P-tau, phosphorylated tau.
Considering the relevance of educational level in MoCA performance, we proceeded to a subsequent analysis organized by education levels. No differences in baseline MoCA z-scores were found between those who converted and those who remained stable in patients under 10 years of education. Conversely, individuals with more than 9 years of education that developed dementia presented lower baseline MoCA z-scores than their counterparts (Table 4).
Baseline MMSE and MoCA z-scores according to education level and cognitive status at follow-up (converters and non-converters)
Bold data indicates p < 0.05. MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; SD, standard deviation.
Considering these results, we proceeded to a Cox regression subanalysis including only those with 9 or more years of education (3rd cycle) (n = 71), showing that lower baseline MoCA z-score (HR = 0.652, 95% CI = [0.490, 0.869], p = 0.004) as well as higher age at onset and lower CSF Aβ42, but not MMSE, were significant independent predictors of conversion (Table 5).
Cox regression results for patients with 9 or more years of education (n = 71) (-2log likelihood = 111.859, χ-squared = 48.791, p < 0.001, degrees of freedom (df) = 7)
Bold data indicates p < 0.05. HR, hazard ratio; CI, confidence interval; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; APOE, apolipoprotein E; CSF, cerebrospinal fluid; Aβ42, amyloid β1-42; T-tau, total tau; P-tau, phosphorylated tau.
Multivariate Cox regression analysis was replicated post-hoc, excluding the patients who converted to other forms of dementia than AD, and results were similar (results not presented).
DISCUSSION
Our findings suggest MoCA as a potential predictor of progression from MCI to dementia and support its use in clinical practice in the evaluation of patients with MCI, namely those with higher education where the MMSE fails to detect cognitive decline.
The outcome for any patient with MCI is uncertain: some patients remain stable or even revert to a normal state, while others progress to dementia [1–3]. Early and accurate identification of individuals at a higher risk of developing dementia in the near future is crucial for the successful development of disease-modifying treatments. Most diagnostics and prognostics instruments [11, 41] are expensive and require equipment only available in tertiary care centers, with some of them requiring invasive procedures.
MoCA was first designed as a cognitive screening tool to assist physicians in the detection of early cases of cognitive decline. In the continuum of AD, MoCA showed high sensitivity in the early identification of patients with MCI (90%) and high specificity in excluding elderly normal controls (87%) [17]. Due to linguistic, cultural, and educational differences, transcultural adaptation and validation studies were needed and MoCA is currently available in over 100 languages and dialects (http://www.mocatest.org). Portuguese population presents a lower educational level compared to the original one of Nasreddine et al. [17] which might impact in the adapted normative scores. This was confirmed in the Portuguese normative study by Freitas et al. [19], where education and age explained 49% of the variance. Based on these results, different cut-offs were calculated for the Portuguese population and stratified according to the different age and educational levels. The choice of the normality cut-off score for MoCA was also considered critical in patients with stroke by Chiti and Pantoni [42]. Other studies discussed this crucial methodological issue in other settings, emphasizing that the proposed addition of 1 point to North America patients with < 12 years of education could not be adequate to patients with different social background [43]. Accordingly, several normative studies around the world confirmed the importance of age and education-related norms for MoCA to avoid misdiagnosis of cognitive decline [44–46].
In our cohort, MoCA z-score correlated significantly with all CSF AD biomarkers. Although significant, correlations were weak, possibly because we had patients progressing to other types of dementia, where these biomarkers do not show marked changes. This finding is consistent with another study that found a correlation between MoCA and amyloid deposition on PET imaging in subjects with MCI [47].
Individuals who exhibited a MoCA z-score < –1.5, an MMSE z-score < –1.5, had decreased CSF Aβ42, or increased CSF t-tau or p-tau levels, as per laboratory reference values, or carried an APOE ɛ4 allele, demonstrated a significantly accelerated rate of conversion. On average, these individuals converted in approximately half to two-thirds of the time compared with their counterparts without these detrimental factors. Moreover, as we could see in Fig. 1, Kaplan-Meier curves diverged right from the baseline, meaning that patients with MoCA z-score ≤ –1.5 have a greater conversion rate than those who score on the normal range both on the short and long term. In our sample, MMSE seemed to be overall better in identifying patients at risk of conversion. However, an analysis including only patients with basic education (9 or more years of education), demonstrated MoCA’s superiority to MMSE in conversion prediction in patients with higher education. Being more demanding, MoCA overcomes the known insufficiencies of MMSE that score highly literate MCI subjects in the normal range. This stresses the importance of MoCA in the present and near future, with patients having increasingly higher levels of education namely in developing countries. In fact, MoCA is already considered to be better than MMSE in the early identification of cognitive decline, having a higher sensitivity (though a lower specificity) in the detection of MCI [17], particularly for MCI with multiple cognitive domains involvement [48].
MoCA’s ability to predict MCI progression have been already observed in previous studies [20, 21]. However, to our knowledge, none has evaluated the predictive value of MoCA in patients with known CSF biomarkers in MCI condition. In this study, MoCA showed to have an additional conversion predictive value to CSF Aβ42, an established predictor of conversion [9, 10], further supporting its performance in the prognosis of MCI patients.
Dementia disorders place a huge burden on clinical care and are set to bulge up due to an aging population in the near and foreseeable future [49]. For that reason, most patients will need to be evaluated on a primary care setting, highlighting the importance of simple and reliable tools to help clinicians assess dementia risk, so that they can refer those who need more specialized evaluation and closer monitoring. Unlike the other diagnostic instruments, cognitive tests may be performed everywhere, are cheap and are well tolerated by patients.
Although our cohort does not have pathological confirmation of the diagnosis, we support the study with biological markers of disease and considering that we focus on conversion rather on the pathological process, this issue is not so relevant. Nowadays, it is well known that Aβ42/Aβ40 ratio is a better indicator of an underlying AD pathology compared to Aβ42. However, at the time most of these patients were assessed, Aβ40 measurement was not available in our center. Other challenge of the study was that we included patients who converted to other forms of dementia other than AD. In our perspective, this enriches the results, as they are more valid to the clinical setting, where patients may progress to different forms of dementia, despite the low number of non-AD patients in our cohort. Nevertheless, we replicated the multivariate Cox regression analysis post-hoc, excluding the patients who converted to other forms, and results were similar. A thorough initial and longitudinal examination and the extensive follow-up of these patients also strengthens our results, as well as the use of z-scores based on different cut-offs adapted for the Portuguese population and stratified according to the different age and educational levels
In conclusion, our results confirm the key role of CSF biomarkers, namely Aβ42, in predicting patient conversion from MCI to dementia, and suggest that neuropsychological assessment with MoCA could help predict which MCI patients will convert to dementia in highly educated populations. Its relatively low cost and availability could spread its use in clinical practice.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
A.S-S. was supported by FCT –Fundação para a Ciência e a Tecnologia, I.P. (DFA/BD/6393/2020). The funding agency had no role in the study design, sample collection, data analysis or the writing of the manuscript.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.