
Abstract
Background:
Elevated amyloid-β (Aβ) on positron emission tomography (PET) scan is used to aid diagnosis of Alzheimer’s disease (AD), but many prior studies have focused on patients with a typical AD phenotype such as amnestic mild cognitive impairment (MCI). Little is known about whether elevated Aβ on PET scan predicts rate of cognitive and functional decline among those with MCI or dementia that is clinically less typical of early AD, thus leading to etiologic uncertainty.
Objective:
We aimed to investigate whether elevated Aβ on PET scan predicts cognitive and functional decline over an 18-month period in those with MCI or dementia of uncertain etiology.
Methods:
In 1,028 individuals with MCI or dementia of uncertain etiology, we evaluated the association between elevated Aβ on PET scan and change on a telephone cognitive status measure administered to the participant and change in everyday function as reported by their care partner.
Results:
Individuals with either MCI or dementia and elevated Aβ (66.6% of the sample) showed greater cognitive decline compared to those without elevated Aβ on PET scan, whose cognition was relatively stable over 18 months. Those with either MCI or dementia and elevated Aβ were also reported to have greater functional decline compared to those without elevated Aβ, even though the latter group showed significant care partner-reported functional decline over time.
Conclusions:
Elevated Aβ on PET scan can be helpful in predicting rates of both cognitive and functional decline, even among cognitively impaired individuals with atypical presentations of AD.
Keywords
INTRODUCTION
Amyloid-β (Aβ) positron emission tomography (PET) scans have demonstrated significant empirical benefits in identifying individuals likely to have Alzheimer’s disease (AD) pathology [1], improving diagnostic accuracy of recruitment for clinical trials [2], and evaluating effects of anti-amyloid therapies [3]. Yet, until recently, Aβ PET scans have not been used routinely for clinical diagnostics because they lacked coverage under Medicare. The US Food and Drug Administration (FDA) has recently expanded their coverage of Aβ PET scans, which may lead to increased use of the technology in the clinical setting. The clinical value of these scans would be enhanced if their results demonstrated good prognostic value in predicting cognitive and functional decline.
The variability in rates of progression of cognitive and functional decline from the early symptomatic phase of mild cognitive impairment (MCI) through the full course of dementia make it difficult to identify single key predictors of decline. Studies examining the association between elevated Aβ on PET scan and cognition have generally found that, among those with normal cognition or MCI, elevated Aβ on PET scan is associated with greater cognitive decline compared with those without elevated Aβ [4–7]. However, the number of individuals with MCI in these studies was relatively small (n < 60). The prognostic value of Aβ PET scans among individuals with dementia is less clear, likely because Aβ deposition plateaus as AD progresses [8, 9]. To date, few studies have examined rates of cognitive decline in relationship to Aβ PET scan results in this group. One study reported that among 31 individuals with clinically diagnosed AD dementia, those with elevated Aβ on PET scan showed faster cognitive decline than those without elevated Aβ [10]. In contrast, another study of 36 patients with AD based on biomarkers and clinical signs of MCI or mild dementia showed no association between rates of cognitive decline and levels of Aβ [11]. In addition to inconsistent results and use of small sample sizes, the majority of studies examining the association between elevated Aβ and cognitive decline had fairly homogeneous participants whose clinical presentations were often consistent with an etiology of AD, such as amnestic MCI [12]. Therefore, it is not clear whether the association between Aβ level on PET and rate of cognitive decline is the same for individuals with MCI or dementia presentations less typical of AD, a group that accounts for a substantial portion of patients in the clinical setting.
Along with cognition, everyday function is important as it impacts level of independence and in turn, caregiver burden [13, 14]. Cognition and everyday function are related, but their rates of change may differ in relation to Aβ PET scan results [15]. The very limited research assessing functional decline in relation to Aβ on PET scan indicates that rate of decline of everyday function does not differ in relation to Aβ level on PET scan for those with either MCI or dementia over 18 months [7] or 36 months [10]. Combined, this evidence highlights the need for further examination of the longitudinal association between Aβ PET and clinically meaningful measures of cognitive and functional decline for those with MCI or dementia of uncertain etiology.
Therefore, we conducted the Caregiver’s Reactions and Experience Study, a supplemental study of the Imaging Dementia—Evidence for Amyloid Scanning (CARE-IDEAS) Study [1], a study designed to assess if use of Aβ PET scans as part of the diagnostic process is associated with subsequent changes in the medical management of individuals with MCI or dementia of uncertain etiology. The CARE-IDEAS Study provides a unique opportunity to understand the clinical trajectories of individuals with MCI or dementia with presentation atypical for AD, including those without elevated Aβ on PET scan. To better understand the prognostic value of Aβ PET scans, we investigated whether elevated Aβ on PET scan predicts cognitive and functional decline over an 18-month period in those with MCI or dementia of uncertain etiology. Findings from this study can help fill gaps in our understanding of the prognostic value offered by Aβ PET scans in potentially identifying individuals with MCI or dementia who are most likely to decline more rapidly to guide clinical diagnosis and treatment planning.
MATERIALS AND METHODS
Participants and setting
The study population was from the parent IDEAS Study, a cohort study examining how Aβ PET scans influence clinical management among 18,295 Medicare beneficiaries aged≥65 with MCI or dementia [1]. Details of the IDEAS Study are described elsewhere [1]. Briefly, IDEAS participants were recruited by dementia specialists from their clinical practices. Participants were required to meet appropriate use criteria for Aβ PET, which included: 1) the etiology of cognitive impairment was uncertain after a comprehensive evaluation by the dementia specialist, 2) AD was among the possible differential diagnoses, and 3) knowledge of Aβ PET status was expected to alter diagnosis and management. Diagnoses of MCI and dementia were based on the experienced clinical judgment of the dementia specialists, and they were not restricted by research or consensus criteria in providing their diagnoses.
The IDEAS Study transferred the contact information of all IDEAS patients who agreed to be contacted for supplemental studies (n = 12,474) to TrialMatch ®, the Alzheimer’s Association’s clinical studies matching service. Trained TrialMatch ® agents called these participants and described the approved IDEAS supplemental studies, including CARE-IDEAS. Of the 3,717 IDEAS study participants who initially agreed to be contacted for the CARE-IDEAS Study, 2,228 of them and 1,872 of their care partners completed the Time 1 (T1) telephone interview a median of 4.5 months post Aβ PET scans. Of these, 1,028 participants with MCI or dementia and their care partners completed the Time 2 (T2) telephone interview about 18 months after the T1 interview. Dyads were excluded if the participant with MCI or dementia was missing the modified Telephone Interview Cognitive Status (TICS-m) [16] (n = 23) or the Everyday Cognition-12 (ECog-12) [17] (n = 10) scale at either time point, or had an uninterpretable Aβ PET scan result (n = 3). The resulting sample consisted of 992 dyads. This study was conducted in accordance with the Helsinki Declaration of 1975. The Brown University and Duke University Institutional Review Boards (IRB) approved the CARE-IDEAS study (#1606001534, #00076890). The Brown University IRB required participants to correctly answer 2 of 3 content questions about the informed consent text at Time 1 or Time 2 to be eligible to participate in that phase of the study.
Measures
The dependent variables were collected at T1 and T2 interviews. Cognitive status of the individual with cognitive impairment and the care partner was measured using an abbreviated version of the TICS-m. The TICS-m is one of the most frequently used telephone cognitive screening instruments to detect cognitive change and dementia [16, 18]. It has been shown to be sensitive to detecting change over time [19–21]. The version of the TICS-m used in this study had a score range of 0 to 41 and included items of immediate (score range 0–10) and delayed 10-noun (score range 0–10) free recall; serial 7 subtraction; counting backwards; orientation to date; naming the president and the vice-president; and naming common items. Higher scores on the TICS-m indicate better cognitive function.
Functional ability of the individuals with cognitive impairment was assessed using the Everyday Cognition-12 (ECog) scale [17] administered to the care partners. The ECog was designed to assess cognitive and functional performance compared to 10 years ago. It has been shown to be sensitive to assessing change over time [22]. The version used in this study consists of 12 questions that ask the care partner to report change compared to 10 years ago on various daily tasks including multitasking, balancing a checkbook, remembering objects and dates, communicating, understanding directions, reading a map, navigating, anticipating and planning, and staying organized. The response options were 1) performs better or no change = 1 point; 2) questionable change or occasionally worse = 2 points; 3) performs consistently a little worse = 3 points; and 4) performs consistently much worse = 4 points. To allow for missing data and ‘don’t know’ responses, the total score was calculated by summing the score for all completed items and dividing by the number of items completed.
The two primary predictors of interest were the Aβ PET scan result (elevated, not elevated) and baseline diagnosis (dementia, MCI). As part of the IDEAS Study, Aβ PET was completed at accredited imaging facilities using 1 of 3 FDA–approved Aβ ligands following published practice guidelines [23]. Participating imaging specialists interpreted the scans using approved reading methodologies for each tracer [24–26]. Based on FDA guidelines, scans were interpreted dichotomously as “negative” (white matter retention only) or “positive” (cortical tracer retention), indicative of either non-elevated or elevated levels of amyloid, respectively. The diagnoses were assigned by the IDEAS dementia specialist study physicians and were based on standard criteria (DSM-IV and/or National Institutes of Aging-Alzheimer’s Association criteria [27–29]).
Both members of the dyad reported sociodemographic characteristics, including age (years), sex, race, ethnicity, and educational attainment. Race and ethnicity were recoded into a dichotomous variable, non-Hispanic white versus other, due to the homogenous nature of the study sample. Using standardized mean differences to evaluate group differences in sex, race, and ethnicity by our main predictors, we determined that these variables did not differ significantly and thus they were not included as covariates in the models. Education level was categorized as: high school graduate or less, some college, bachelor’s degree, and graduate degree or higher. We included both education and age as covariates in all of our analytic models because both differed by our main predictors, and therefore were anticipated to be potentially important confounders.
Data analysis
Group differences in demographic characteristics based on scan result (elevated versus not elevated) and diagnosis (MCI versus dementia), were evaluated using standardized mean differences. Standardized mean differences of less than 20% in absolute value indicate reasonable covariate balance and are not sensitive to sample size [30]. For categorical characteristics with more than two levels (e.g., education), we calculated the mean difference for each category relative to a reference category. To test the association between Aβ scan results, diagnosis, and our outcomes (TICS-m, ECog), we regressed the change in scores from T1 to T2 on the TICS-m and ECog in separate multivariable linear regressions with scan results (elevated, not elevated) and diagnosis (MCI, dementia) and their interaction entered in as predictors, and age and education as covariates.
We expected that as a group the TICS-m scores at T1 would be lower for those with dementia compared to those with MCI; however, we also expected that there would be overlap between the distribution of the TICS-m scores for the different diagnostic groups. Therefore, we conducted analyses to determine if future cognitive decline is associated with TICS-m score at T1 rather than the diagnosis of MCI or dementia. Thus, to determine if Aβ PET scan results and T1 TICS-m scores predicted cognitive decline, we regressed T1 to T2 TICS-m change scores in a multivariable model with scan results (elevated, not elevated) and T1 TICS-m score (median-split TICS-m score: high versus low) and their interaction serving as predictors, and included participant age and education as covariates. Rather than using clinical cut points that were likely less relevant in an already impaired population, we divided T1 TICS-m scores using a median split method. We included the interaction term (scan×T1 TICS-m score) to test the hypothesis that an elevated Aβ scan result would be associated with a greater decline in cognitive function for those with lower T1 TICS-m scores. We conducted parallel analyses using ECog scores and dividing the T1 ECog scores using a median split method.
Finally, we regressed change in immediate and delayed recall scores on the TICS-m in separate multivariable models to test the effect of scan result and diagnosis on memory score components of the TICS-m scale. To generate model-implied means for scan by diagnosis by time for all models, we repeated the analyses utilizing linear models fit via generalized estimating equations clustered by individual, by modeling the outcome variables at both time points, and including time point (T1, T2) as additional predictors.
RESULTS
Participant and care partner characteristics at T1 are presented in Table 1. The average time between T1 and T2 did not differ significantly (p = 0.61) for those with elevated Aβ scan results (mean = 531.8 days; SD = 29.1) compared to the non-elevated scan result group (mean = 532.9 days; SD = 33.5). A total of 496 of the 760 with MCI had elevated Aβ scan results, while 178 of the 232 with dementia had elevated Aβ scan results. Among those with elevated Aβ, 83 (5.7%) of those who completed T1 interviews did not complete T2 because they did not answer questions demonstrating cognitive capacity to give informed consent. In contrast, only 22 (2.9%) of those with non-elevated Aβ scan results did not complete the T2 interview for the same reason.
Time 1 characteristics of participants, by scan result and diagnosis, and care-partner characteristics
SMD, standard mean difference. Values of less than 20% in SMD absolute value indicate reasonable covariate balance. SD, standard deviation. *For Participants, ‘Other’ was comprised of American Indian or Alaska Native (n = 3), Asian (n = 4), Hispanic white (n = 19), mixed race (n = 15), Non-Hispanic Black or African American (n = 15) and Missing (n = 7). For Care Partners, ‘Other’ was comprised of American Indian or Alaska Native (n = 6), Asian (n = 6), Hispanic white (n = 17), mixed race (n = 16), Non-Hispanic Black or African American (n = 11) and Missing (n = 4).
The multivariable regression models examining the effect of the scan results and diagnosis on change on the TICS-m from T1 to T2, while controlling for participant age and education, yielded no significant interaction effect between scan result and diagnosis (p = 0.140). Averaging the effect of scan results for those with dementia and those with MCI, we found elevated Aβ was associated with greater decline on the TICS-m [β= –1.84 (–2.62, –1.07)] compared to those without elevated Aβ. Similarly, for change in ECog scores, we found no evidence of an interaction effect between scan result and diagnosis (p = 0.711). Averaging the effect of scan results for those with dementia and those with MCI, we found that people with elevated Aβ had significantly greater increase in ECog scores (more impairment) from T1 to T2 [β= 0.13 (0.05, 0.22)] compared to those without elevated Aβ. Table 2 presents the model-implied means for the TICS-m and ECog at both time points and the change from T1 to T2. Those with dementia scored lower on the TICS-m and had a higher mean score on the ECog (more impairment) compared to participants with MCI. Matching the change score models, the model-implied means from the mixed models demonstrate that individuals with elevated Aβ on the PET scan had lower mean TICS-m scores and higher ECog scores at T2 versus T1 across diagnoses.
Model-implied means for TICS-m and ECOG scores at Time 1 and Time 2 and change over time
Models controlled for participant age and education. Higher TICS-m scores reflect better cognition and lower ECog scores reflect better function. Values under Time 1 and Time 2 are model-implied means (95% Confidence Intervals). *Change from Time 1 to Time 2 was significantly different from 0 (p < 0.05).
To examine whether the association between elevated Aβ and change in the TICS-m score from T1 to T2 was influenced by the TICS-m score at T1, we used the median split of the TICS-m at T1 to define high and low levels. The median score was 22. Among those with MCI, 56% had scores above the median and 20% of those with dementia had scores above the median. We found that the T1 TICS-m score significantly moderated the association between Aβ scan results and change in TICS-m score (p = 0.02; Fig. 1a). Among those with higher T1 TICS-m scores, elevated Aβ scan was associated with a 1.19 greater point decline in TICS-m at T2 [β= –1.19 (–2.02, –0.37)] compared to those without elevated Aβ. Among those with lower than median T1 TICS-m score, the difference in decline associated with elevated Aβ was greater [β= –2.63 (–3.55, –1.71)], though this greater difference in decline is explained in part by an increase in TICS-m scores among those with lower than median T1 TICS-m scores and non-elevated Aβ. As shown in Fig. 1a, scores declined for those with high T1 TICS-m scores in both the elevated and non-elevated Aβ scan groups. Those with low T1 TICS-m scores and elevated scan results declined on the TICS-m, but scores did not decline and may have slightly increased for participants with low T1 TICS-m scores and non-elevated Aβ.
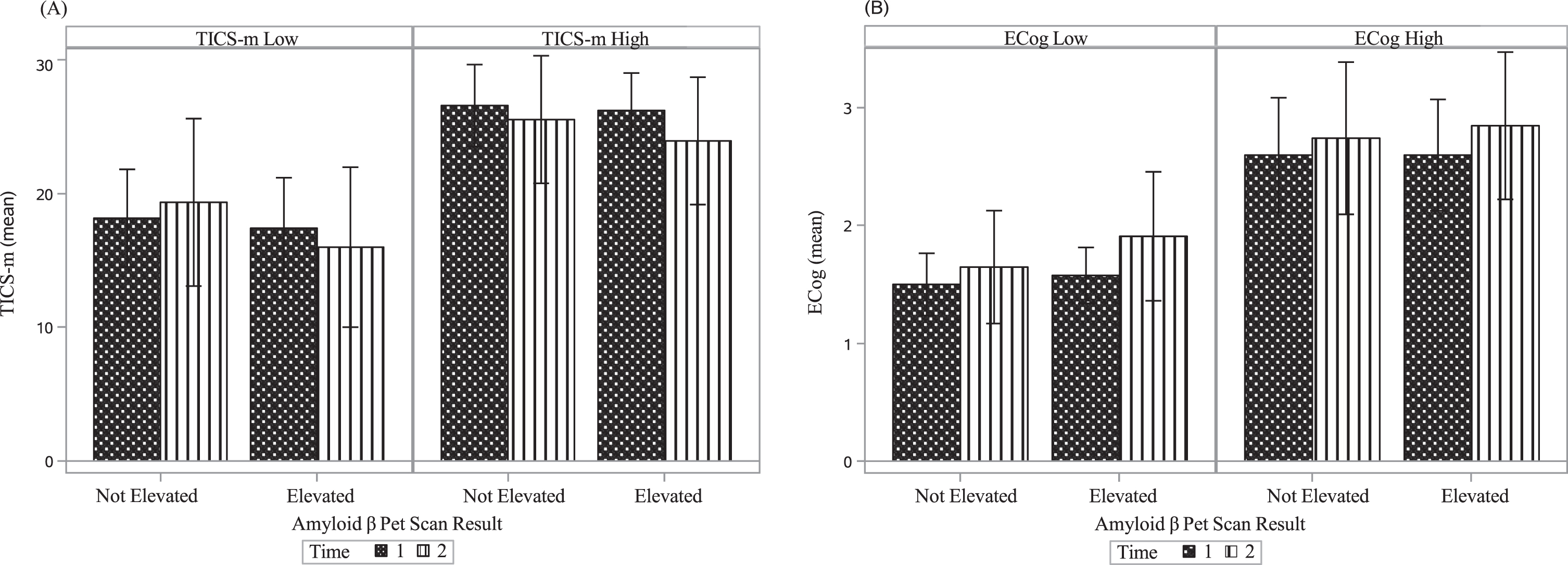
TICS-m and Ecog scores, by time and scan result. A) Left panel shows group with baseline scores below the median TICS-m baseline score. Right panel shows group with baseline scores above the median TICS-m baseline score. Higher scores on the TICS-m indicate better cognitive function. B) Left panel shows group with baseline scores below the median ECog baseline score. Right panel shows group with baseline scores above the median ECog baseline score. Higher scores on the ECog indicate worse function. The error bars represent standard deviations.
To examine whether the association between elevated Aβ and change in the ECog score from T1 to T2 was influenced by the ECog score at T1, we used the median split of the ECog at T1 to define high and low levels. The median score was 2. Among those with MCI, 51% had scores above the median (i.e., greater impairment) and 69% percent of those with dementia had scores below the median. We found that the T1 ECog score did not significantly moderate the association between Aβ scan results and change in ECog score (p = 0.25; Fig. 1b). Lower T1 scores indicating less functional impairment showed that elevated Aβ was associated with a 0.18 greater increase (worsening of function) in ECog scores at T2 [β= 0.18 (0.08, 0.27)] compared to those without elevated Aβ. But among those with higher than median T1 ECog scores, the change in ECog score for those with elevated Aβ did not differ from those without elevated Aβ [β= 0.09 (–0.00, 0.19)].
In exploratory analyses probing the relationship between Aβ scan results, diagnosis, and changes in the immediate and delayed recall score components of the TICS-m, we found no evidence of interaction effects between scan result and diagnosis on changes for either immediate or delayed recall [immediate: p = 0.24; delayed: p = 0.82]. We found that only changes in immediate recall scores were associated with Aβ scan results. Specifically, averaging over diagnosis, those with elevated Aβ had significantly greater declines in immediate recall scores [β= –0.46 (–0.76, –0.16)], but not in delayed recall [β= –0.10 (–0.36, 0.16). Table 3 shows model-implied mean scores for immediate and delayed verbal recall by diagnosis, scan result, and each time point and change in scores over time.
Model-implied means for Immediate and Delayed recall task at Time 1 and Time 2 and change over time
Models controlled for participant age and education. Values under Time 1 and Time 2 are model-implied means (95% Confidence Intervals). *Change from Time 1 to Time 2 was significantly different from 0 (p < 0.05).
DISCUSSION
We investigated whether rate of cognitive and functional decline was associated with level of Aβ on PET scan among individuals with MCI or dementia with presentations atypical for AD. Our findings show that individuals with a diagnosis of MCI or dementia of uncertain etiology and elevated Aβ on PET scan declined more rapidly on an objective global cognitive status measure (i.e., TICS-m) compared to those without elevated Aβ. Most prior studies have focused on the association between elevated Aβ on PET scan and cognitive decline among those who have a more typical AD phenotype, such as amnestic MCI [4–7, 11]. Elevated Aβ is included in the research framework on the biological definition of AD [31] and is a criterion for a pathologic clinical diagnosis of AD. But elevated Aβ is also found as a coexisting pathology in dementias with primary pathology attributed to another etiology such as dementia with Lewy bodies [32]. Our results indicate that elevated Aβ on PET scan is associated with greater cognitive decline even in circumstances where clinicians have uncertainty about the etiology. Such diagnostic dilemmas are well known to dementia experts due to a range of factors including mixed pathologies and confounding factors such as depression, medications, and cardiovascular or other medical conditions. The majority of individuals with a clinical diagnosis of AD have mixed pathology postmortem [33], and this may explain the varied level of accuracy of clinical AD diagnoses even among dementia specialists [34]. The actual effect of elevated Aβ on PET scan may be greater than estimated by our results because a greater proportion of individuals in our study with elevated Aβ were unable to give informed consent at Time 2 due to cognitive decline (N = 89, 5.7%) compared to those without elevated Aβ (N = 22, 2.9%).
When comparing rate of decline on the TICS-m based on T1 score, we found that, overall, those with higher cognitive function at T1 declined regardless of Aβ status. In contrast, those with lower cognitive function at T1 and elevated Aβ declined on the TICS-m, but those with lower cognition at T1 without elevated Aβ did not decline. It is possible that the stable to mildly improved scores of those without elevated Aβ with low cognition at T1 reflect a practice effect, regression to the mean, or that they did not have AD but potentially a reversible cause for their cognitive impairment. In contrast, participants with elevated Aβ (i.e., biomarker evidence of AD) showed cognitive decline. These findings suggest that elevated Aβ may be associated with cognitive change over a fairly broad range of TICS-m scores at least through mild dementia. Thus, although tau biomarkers have typically been more closely tied to rate of cognitive decline [11], identifying Aβ as a reliable marker of cognitive decline would strengthen the justification of its use in clinical settings and provide additional markers to predict cognitive change. In exploratory analyses, we found that elevated Aβ was associated with greater decline of immediate memory recall scores but not with rates of decline of delayed recall. This may be due to the low scores and limited range of scores for delayed recall, which is likely attributable to the TICS-m having only one learning trial, while other word list memory tests have more than one learning trial.
Although small changes in performance on cognitive status measures may not be directly aligned with observable changes in everyday functional ability, importantly, we found that care partners also reported greater decline in function as measured by the ECog scale for those with elevated Aβ on PET scan, thus mirroring the results for the TICS-m. Two other studies assessed change in function using a different instrument than that used in our study and found that elevated Aβ on PET scan was not associated with greater decline in everyday function over both an 18-month [7] and a three-year period [10]. Another study reported that greater Aβ deposition on PET scan was associated with more impairment reported on the ECog by informants for those with more advanced MCI, but not for those with less advanced MCI or dementia, but this study did not assess change in function over time [35]. The effect sizes for the present study results were relatively small for both cognition and everyday function. This may help to explain why our findings are discrepant from some prior studies, especially those for rate of cognitive decline in dementia and rate of functional decline in MCI and dementia. Some other studies may have been underpowered to find significant small differences in cognitive and functional outcomes. It is difficult to map effect size of cognitive and functional measures to clinical significance. To provide some context in this regard, we note that on average those with dementia and elevated amyloid declined 14% on the TICS-m over 18 months, while those with dementia and non-elevated amyloid declined 0.02% over this time period. In addition, although the actual change in ECog scores over time is small due to the restricted range for these scores (between 1 and 4, reflecting averaged scores over 12 items in various domains of functioning), these changes reflect decline in daily functioning observed by care partners, thus suggesting their importance in everyday life.
There is growing interest in individuals with diagnosed cognitive impairment who do not have elevated Aβ on PET scan. These cases are often labeled “suspected non-Alzheimer’s disease pathology,” or SNAP. Although we lacked the data to evaluate all SNAP criteria, namely neurodegeneration, CARE-IDEAS does provide a unique opportunity to assess those without elevated Aβ, a group that represented about one-third of the present sample. The clinical trajectory of individuals with SNAP is unclear, with some studies demonstrating decline in cognition or everyday function over time [36–38], but others showing no change [39, 40]. We found that although individuals with elevated Aβ showed greater cognitive and functional decline over the 18-month study period compared with those with non-elevated scans, even individuals with non-elevated Aβ showed worsening caregiver-reported function (though no significant change in cognition) over time. It is noted that physicians of the parent study, IDEAS, reported making treatment decisions based on results of Aβ PET imaging, including discontinuing anti-dementia medications for some participants without elevated Aβ. It is unclear whether these medications would be effective in delaying functional decline among those with non-elevated Aβ and thus influence the results of our study. Future investigation of IDEAS data may provide important insights regarding the potential impact of such treatment decisions on the overall cognitive and functional decline trajectories demonstrated in our report.
Limitations
Limitations include a lack of diversity with respect to race, ethnicity, and years of education in the present sample. Sample heterogeneity is particularly important when examining cognitive change over time, as several of these sociodemographic variables are important contributors to cognitive reserve [41]. In addition, the IRB required eligibility be dependent on the participant correctly answering questions about the consent language to demonstrate capacity to give informed consent. As such, individuals who completed the T1 interview but had greater cognitive impairment were ineligible to participate at the follow-up interview. However, twice as many individuals with elevated Aβ were ineligible at T2 for this reason compared to those without elevated Aβ (5.7% versus 2.7%). Thus, our results likely underestimate the association between elevated Aβ and cognitive and functional decline. Altogether, this suggests the results may not be generalizable to groups unrepresented in the sample.
Conclusions
As previously reported [1], the results of Aβ PET scans allow greater confidence in identifying the etiology of MCI or dementia for individuals with atypical presentations of AD and this impacts patient management decisions. Our data showing prognostic implications of decline over time provide additional support justifying the utilization of Aβ PET scans in clinical decision-making. The results of Aβ PET scans allow greater confidence in the diagnosis of MCI or dementia with atypical presentations of AD. In addition, the finding that elevated Aβ on PET is associated with more rapid cognitive and functional decline may lead to better identification of those more likely to need access to health care resources, earlier treatment, and assist families with future planning even among individuals with cognitive impairment due to uncertain etiology.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgements to report.
FUNDING
This work was supported by the National Institute on Aging of the National Institutes of Health under award number R01AG053934, and by the American College of Radiology Imaging and Alzheimer’s Association. The content is solely the responsibility of the authors and does not necessarily represent views of the National Institutes of Health, the American College of Radiology or the Alzheimer’s Association.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.