
Abstract
Background:
Neuropsychiatric symptoms (NPS) are distressing for patients with dementia, often accelerating functional decline and nursing home placement. Medications such as quetiapine are used to alleviate NPS, but their side effects require cautious use. Liquid formulations such as quetiapine oral suspension suit specific populations; however, real-world data on their use in patients with dementia are limited.
Objective:
The purpose of this retrospective, naturalistic study was to provide preliminary data on the effects of treatment with quetiapine oral suspension on behavioral and psychiatric disturbances in Alzheimer’s disease (AD) outpatients in Taiwan.
Methods:
Between January 2022 and June 2023, data were collected from outpatients with a diagnosis of probable AD who received treatment with Qting® (quetiapine oral solution 25 mg/ml). Primary outcome measures were changes in Neuropsychiatric Inventory (NPI) total score and its sub-items from baseline to the endpoint.
Results:
We recruited 66 AD patients with a mean age of 72.1±7.6 years, most of whom were female (69.7%). Twenty-three patients had data on neuropsychological test and NPI scores before and after quetiapine treatment. There was no significant change in global cognitive function from baseline to the endpoint. A significant reduction in NPI total score after quetiapine treatment was noted, while the effect on NPI sub-items was limited. The average maintenance dose was 1.5±0.6 ml.
Conclusions:
We demonstrated our clinical experience of the use of quetiapine oral solution in AD patients with NPS. Our results showed that quetiapine oral solution treatment significantly improved these symptoms at a relatively low dose.
INTRODUCTION
Neuropsychiatric symptoms (NPS) in patients with dementia such as agitation, aggression, delusions, hallucinations, and sleep disturbances are very common and often more distressing than cognitive issues [1]. NPS have been reported to occur in up to 90% of dementia patients, with a higher prevalence in severe cases [2, 3]. These symptoms worsen functional decline and are linked to nursing home placement due to their impact on the patients’ well-being and cognitive functioning.
Although non-pharmacological interventions are recommended as first-line treatments for NPS in patients with dementia, medications are commonly initiated to alleviate caregiver burden and improve NPS [4–6]. Quetiapine is an atypical antipsychotic frequently used in an off-label manner to control the behavioral and psychological symptoms of dementia, although the use of antipsychotics has been associated with serious side effects such as extrapyramidal syndrome and major cardiovascular events [7]. It is therefore important to use antipsychotics briefly and at the lowest possible dosage when managing NPS in patients with dementia. It is therefore important to use antipsychotics for short periods and at the lowest possible dosage when managing NPS in patients with dementia. In Taiwan, quetiapine is not approved for the treatment of NPS and treatment is off-label; however, the use of quetiapine is still promoted by clinical practice guidelines [8, 9].
Liquid formulations are an alternative treatment option for specific populations such as children, older adults, and individuals with dysphagia. These formulations are easy to swallow, offer flexibility and ensure accurate dosing [10, 11]. Qting® oral suspension (Center Laboratories, Inc.) contains 25 mg of quetiapine per milliliter. Few studies have reported real-world clinical experience of the use of quetiapine oral solution for behavioral/psychological symptoms in patients with dementia. Therefore, the aim of this study was to assess the effectiveness of quetiapine oral suspension in managing these symptoms through a retrospective analysis of patients with Alzheimer’s disease (AD) before and after treatment with quetiapine in Taiwan.
MATERIALS AND METHODS
Data source
Data for this chart review study were derived from the Kaohsiung Municipal Ta-Tung Hospital (KMTTH) Dementia Cohort study. The KMTTH Dementia Cohort is a hospital-based, observational study of elderly Taiwanese outpatients with cognitive impairment that has been conducted at KMTTH in southern Taiwan since January 2022. Most of these outpatients undergo a series of comprehensive evaluations, including detailed medical history assessments, tests for neurological and psychiatric symptoms, blood analysis, and imaging scans to determine the type of dementia. Regular neuropsychological test results are also recorded. Consequently, we conducted this retrospective study using these data to identify patients with dementia who were either using or had used quetiapine oral suspension. This study was approved by the Kaohsiung Medical University Hospital Institutional Review Board (KMUHIRB-SV(I)-20210067).
Inclusive cases
A total of 592 patients with dementia due to AD were enrolled in the KMTTH Dementia Cohort, with an age ranging from 55 to 100 years. The diagnosis of AD was made according to the 2011 National Institute on Aging and Alzheimer’s Association criteria for “probable AD” [12]. We reviewed their chart records from January 2022 to June 2023, and identified 70 patients who had taken quetiapine oral suspension during this period. All 70 patients had also received a series of neuropsychological screening tests, including the Clinical Dementia Rating (CDR) scale with CDR-Sum of Boxes (CDR-SB) [13], and Cognitive Abilities Screening Instrument (CASI) to corroborate the diagnosis of cognitive dysfunction [14]. Mini-Mental State Examination (MMSE) scores were derived from the CASI scores (i.e., the estimated MMSE scores) [14, 15].
Patients were excluded if they: 1) had taken other antipsychotic agents either immediately, preceding or concurrently with the use of quetiapine oral suspension; and 2) lacked MMSE, CDR, CASI, or Neuropsychiatric Inventory (NPI) scores 3 months before the use of quetiapine oral suspension.
Outcomes measures
The primary outcome measures were NPS of dementia, as assessed by the NPI. The NPI is a commonly used caregiver-informant interview that evaluates 12 behavioral changes (NPI frequency x severity) along with the caregiver’s burden associated with these changes (NPI Distress) [16]. The NPI total score is calculated as the sum of the frequency multiplied by severity scores for each domain. The total score ranges from 0 to 144, with a higher score suggesting more severe or distressing NPS [17, 18].
Data collection
Sociodemographic data including gender, age, education, and the severity of dementia were collected. We obtained patterns of treatment with quetiapine oral suspension by reviewing medical records, including information about the dose and duration. The “starting dose” of quetiapine was defined as the administration dose at the first day of prescription. The “maintenance dose” was defined as the consistent dose throughout a specific timeframe meeting the following criteria: 1) two clinical visits spaced more than 4 weeks apart; and 2) continuous administration of an unchanging quetiapine dose during this duration. We also recorded the use of adjunctive medicines during quetiapine treatment, including antidementia drugs, antidepressants, benzodiazepine and antiseizure medications, all of which are commonly used in dementia patients.
Statistical analysis
Data are presented as the mean±standard deviation or proportion. Pearson correlation analysis was used to evaluate the correlations of age, gender, education, severity of cognitive impairment, severity of NPS, and the pattern of treatment with quetiapine. The Wilcoxon signed-rank test was used to compare NPI scores before and after quetiapine treatment. All analyses were conducted using SPSS version 20.0 software for Windows (IBM Inc., Armonk, NY). Data were visualized using MedCalc Statistical Software version 19.2.6 (MedCalc Software bv, Ostend, Belgium). Statistical significance was set at p < 0.05 for all tests.
RESULTS
A total of 66 patients were recruited in this study, and their characteristics are shown in Table 1. The mean age of the patients was 82.1±7.6 years, most were female (69.7%), most had mild dementia (67.1%), and more than 90% were community-dwelling. The baseline mean estimated MMSE and CASI scores were 11.0 and 39.3, respectively. The mean NPI score before quetiapine treatment was 24.8. Most of the patients (51/66) were concurrently using cholinesterase inhibitors, and 50% (33/66) were concurrently taking at least one of the following types of medications: antidepressants, benzodiazepines, antiparkinsonian drugs, and antiseizure medications. The duration and dose of quetiapine oral suspension treatment are reported in Table 2. The mean duration of quetiapine usage was 204.0±193.2 days (range 14 days to 542 days), and the average maintenance quetiapine dose was 1.5 ml per day. There was a significant correlation between baseline NPI total score with baseline CDR-SB score (r = 0.41, p < 0.01). However, there were no significant correlations between quetiapine dose or total duration of use with age, baseline estimated MMSE, CASI, CDR-SB, or NPI total scores (Table 3). There were also no significant correlations between NPI sub-item scores and pattens of quetiapine use (data not shown in the table).
Among the 66 patients, 23 had data on neuropsychological test and NPI scores before and after quetiapine treatment. Cognitive and behavioral/psychological test data were also available for these patients, as shown in Table 4. The estimated MMSE score remained stable from baseline to the endpoint after quetiapine treatment. Although there was a decline in CASI score, the difference was not significant. Elation/euphoria was a rare presentation in these patients. Following quetiapine treatment, a notable reduction in NPI total score was observed (p = 0.04) (Fig. 1). Nonetheless, there were no significant changes in individual sub-item scores of the NPI before and after quetiapine treatment.
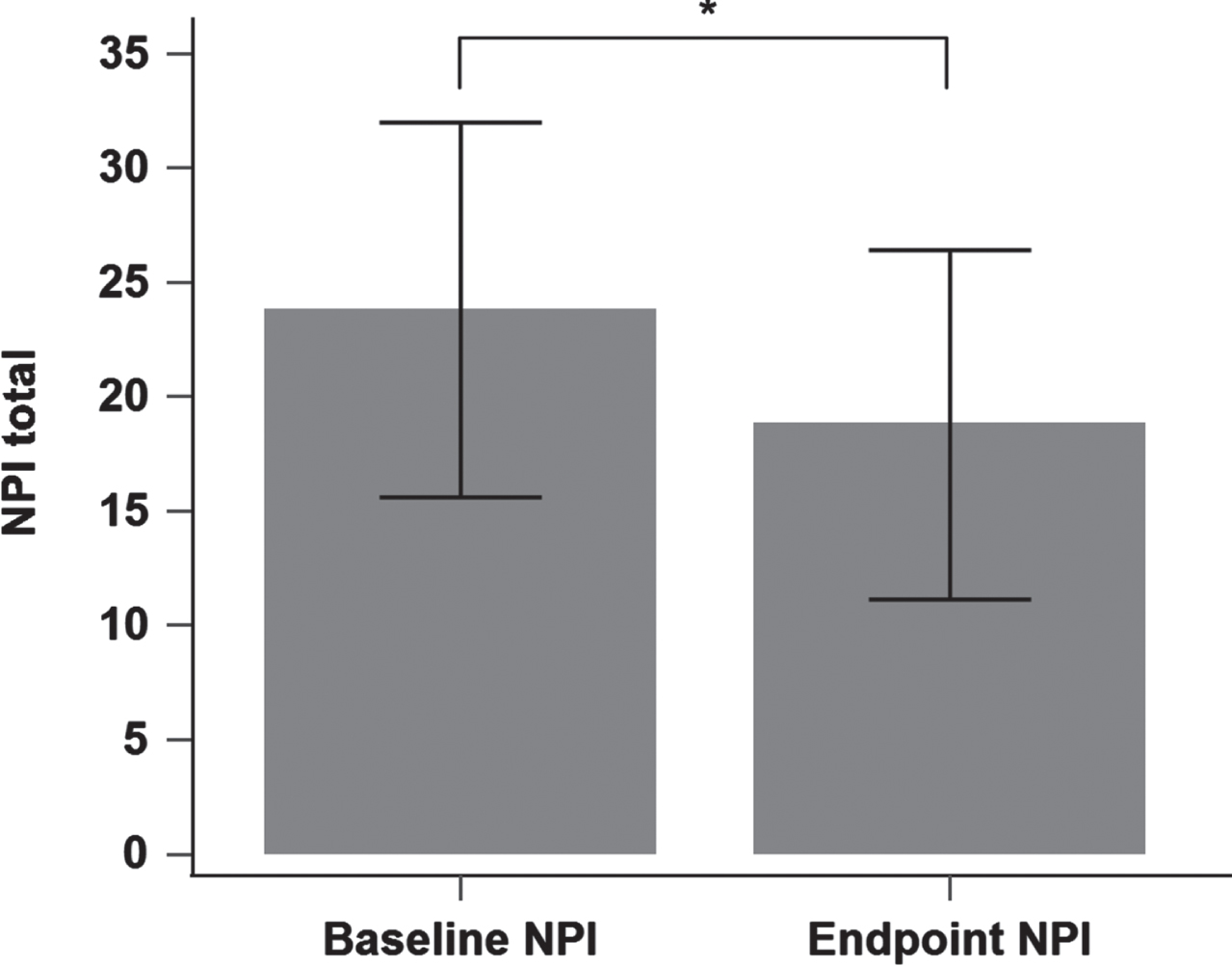
Changes of Neuropsychiatric Inventory (NPI) score from baseline to the endpoint. *p < 0.05.
Demographic data and baseline scores (N = 66)
MMSE, Mini-Mental State Examination; CASI, Cognitive Abilities Screening Instrument; CDR-SB, Clinical Dementia Rating-Sum of Boxes; ChEI, cholinesterase inhibitor; NPI, Neuropsychiatric Inventory.
Quetiapine dose and total using days (N = 66)
Quetiapine oral suspension contains 25 mg of quetiapine per mL.
Correlation of quetiapine prescriptions pattern with demographic variables (N = 66)
MMSE, Mini-Mental State Examination; CASI, Cognitive Abilities Screening Instrument; CDR-SB, Clinical Dementia Rating-Sum of Boxes; NPI, Neuropsychiatric Inventory.
NPI scores difference before and after quetiapine treatment (N = 23)
*p < 0.05, FxS, frequency times severity; NPI, neuropsychiatric inventory.
DISCUSSION
We conducted this retrospective chart-review study of AD patients to examine the effect and average dose of quetiapine oral suspension on NPS in an outpatient setting. The baseline mean estimated MMSE score in our patients was 11.0, indicating moderate cognitive impairment [19]. Our results showed that quetiapine oral suspension treatment with an average dose of 1.5 ml/day led to noteworthy improvements in behavioral symptoms, as evidenced by a significant reduction in NPI total score compared to baseline. However, there were no significant improvements in NPI sub-items, including agitation and psychosis, and there was no association between quetiapine dose or total duration of treatment with the severity of NPS. Of note, assessments of global cognitive function showed that treatment with quetiapine did not have a detrimental effect on cognitive performance. We also found that the severity of behavioral symptoms was correlated with the severity of dementia, which is consistent with previous studies [20, 21].
Quetiapine is one of the most commonly used antipsychotic drugs for elderly patients in Taiwan due to its minimal anticholinergic activity, and lower rates of extrapyramidal adverse effects and mortality compared to other antipsychotics [7, 23]. The currently available evidence suggests that quetiapine can modestly improve NPI total score but has limited efficacy in treating agitation and psychosis [7], and this is consistent with our findings.
The daily dose of quetiapine in our study is much lower compared to previous studies [24–26]. In a meta-analysis of randomized placebo-controlled trials [26], the average quetiapine daily dose ranged from 56.5 to 200 mg, compared to a mean starting dose of 1.3 mL/day (equivalent to 32.5 mg/day) and mean maintenance dose of 1.5 mL/day (equivalent to 37.5 mg/day) in our study. With regards to the participants, the mean MMSE score of the dementia patients in the previous studies ranged from 12.4 to 19.2, indicating moderate severity, which is similar to our participants. In addition, the mean baseline NPI total score in the other studies ranged from 25.1 to 43.3, which is slightly higher than in our participants. There are several possible explanations for the lower quetiapine daily dose in our study compared to the other studies. First, differences in disease characteristics and demographic factors between the study populations may play a role. Most of our patients came from the community, and the NPI total score was slightly lower in our participants. In addition, our data were sourced solely from a neurology outpatient department, and we excluded inpatients and those under psychiatric care, who often exhibit more severe symptoms and may require higher dosages. Second, we exclusively analyzed patients using quetiapine oral suspension, which generally implies a lower dosage. This is because liquid formulations allow for the precise administration of small doses without the need for splitting a tablet, a characteristic more suitable for patients on smaller doses. Patients on higher dosages can opt for tablet forms. Moreover, racial or ethnic differences in the metabolic patterns of antipsychotics may have led to variations in tolerable or efficient dosages between our study and the others [27].
Clinical guidelines generally recommend that antipsychotics should only be used for short periods of time, with a requirement to reassess their risks, benefits, indications, and dosage at least every 3 months due to considerations of safety [28, 29]. The overall duration of quetiapine treatment in our study was relatively long (mean 204 days), and more than half of the patients used quetiapine solution for more than 3 months. Several reasons could explain the long duration of use, such as suboptimal therapeutic effects of quetiapine, the lack of effectiveness or availability of non-pharmacological interventions, and insufficient family support.
To the best of our knowledge, this study is the first to report real-world experience and investigate the effectiveness of treatment with quetiapine oral suspension in managing NPS in patients with AD. This study has several limitations. First, it is a retrospective chart review study, and certain important information was unavailable. For example, the timing of medication use, discontinuation, and adjustments were solely based on the judgment of individual physicians, and this information was not available in the charts. Consequently, we could not address why physicians chose quetiapine oral suspension instead of tablets, or analyze medication adherence or self-dosage adjustments. In addition, the clinical and medical records may have been incomplete or inaccurate, and there were no reliable records of medication compliance and side effects. Retrospective chart reviews provide valuable initial insights but have limitations in assessing these crucial aspects, which should be acknowledged [30, 31]. Second, the study design involved pre- and post-intervention tests in a single group, which makes it challenging to control for confounding factors such as concomitant medications including antidepressants and cholinesterase inhibitors. Additionally, the study sample size was relatively small to effectively examine the potential effects of the pharmacological intervention on NPS. Moreover, the data were sourced solely from one hospital and only included individuals with AD, therefore limiting the generalizability of the results to all dementia patients.
In summary, the results of this study demonstrated an improvement in NPS among outpatients with AD during treatment with quetiapine oral suspension at a low daily dose. However, the effect on reducing agitation and psychosis was not statistically significant. Further research involving a larger sample size and prospective, controlled study design is necessary to confirm the efficacy, safety, and tolerability aspects of quetiapine oral suspension.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This study was supported by National Health Research Institutes (NHRI-11A1-CG-CO-06-2225-1, NHRI-12A1-CG-CO-06-2225-1), Kaohsiung Medical University Research Center (KMU-TC112B02), Department of Neurology, Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung, Taiwan (KMTTH-111-004).
CONFLICT OF INTEREST
Yuan-Han Yang is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
All other authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article.