
Abstract
Background:
Financial capacity is vital for the elderly, who possess a substantial share of global wealth but are vulnerable to financial fraud.
Objective:
We explored the link between small vessel disease (SVD) and financial capacity in cognitively unimpaired (CU) older adults via both cross-sectional and longitudinal analyses.
Methods:
414 CU participants underwent MRI and completed the Financial Capacity Instrument-Short Form (FCI-SF). Subsequent longitudinal FCI-SF data were obtained from 104, 240, and 141 participants at one, two, and four years, respectively. SVD imaging markers, encompassing white matter hyperintensities (WMH), cerebral microbleeds (CMB), and lacune were evaluated. We used linear regression analyses to cross-sectionally explore the association between FCI-SF and SVD severity, and linear mixed models to assess how baseline SVD severity impacted longitudinal FCI-SF change. The false discovery rate method was used to adjust multiple comparisons.
Results:
Cross-sectional analysis revealed a significant association between baseline WMH and Bank Statement (BANK, β=-0.194), as well as between lacune number and Financial Conceptual Knowledge (FC, β= –0.171). These associations were stronger in APOE ɛ4 carriers, with β= –0.282 for WMH and BANK, and β= –0.366 for lacune number and FC. Longitudinally, higher baseline SVD total score was associated with severe FCI-SF total score decrease (β= –0.335). Additionally, baseline WMH burden predicted future decreases in Single Checkbook/Register Task (SNG, β= –0.137) and FC (β= –0.052). Notably, the association between baseline WMH and SNG changes was amplified in APOE ɛ4 carriers (β= –0.187).
Conclusions:
Severe SVD was associated with worse FCI-SF and could predict the decline of financial capacity in CU older adults.
Keywords
INTRODUCTION
Financial scams often target older adults, who suffer from brain aging and related diseases and have less financial capacity to make informed decisions [1, 2]. Financial capacity has been found declined in mild cognitive impairment (MCI) [3, 4], and became more pronounced in Alzheimer’s disease (AD) patients [5]. The Financial Capacity Instrument Short Form (FCI-SF) efficiently assesses financial abilities, distinguishing cognitively unimpaired (CU) individuals from MCI or AD patients, and tracks changes longitudinally [3, 7]. Recently, imaging studies have uncovered connections between financial capacity and brain alterations. Both financial capacity and white matter integrity declined in relation to the severity of the disease, showing minimal to no impact in healthy elderly individuals, notable effects in MCI, and more pronounced effects in AD patients [5]. In MCI, performance on the FCI-SF is linked to angular gyri and precunei volumes [8]. Further, FCI-SF performance and processing speed in CU adults also relate to AD pathologies [9, 10].
Cerebral small vessel disease (SVD) is a common occurrence in older adults. The imaging characteristics of SVD include white matter hyperintensities (WMH), lacunes, dilated perivascular spaces (dPVS), and cerebral microbleeds (CMB) observed on MRI scans [11, 12]. Studies have linked the presence and extent of SVD to impaired daily living activities, cognitive decline, and dementia [13]. However, SVD’s connection to financial capacity is underexplored, especially in CU individuals. Additionally, the apolipoprotein E (APOE) allele is a well-known genetic risk factor for sporadic AD, and individuals carrying the APOE ɛ4 allele have an increased risk of cognitive decline and more severe SVD burden and progression [14–16]. Given the high prevalence of SVD and the importance of financial capacity, the association between them needs to be investigated.
This study pursued two goals: 1) assessing links between SVD imaging markers and changes in financial capacity among CU older individuals over time, and 2) investigating whether the presence of the APOE ɛ4 allele enhances the association between SVD and financial capacity. SVD markers were visually assessed, resulting in a total severity score [17, 18]. Additionally, WMH volume was quantified using automated segmentation. PET-based amyloid, tau, and hippocampal volume were covariates, considering their connections to financial capacity and AD pathologies [9, 19].
METHODS
Alzheimer’s Disease Neuroimaging Initiative (ADNI)
The study utilized data from the ADNI database, initiated in 2003 and expanded with ADNI3 from 2016. ADNI aims to explore connections between genetics, biomarkers, imaging, cognition, and AD across its stages. ADNI-3 spans 59 North American sites, enrolling participants from NC, MCI, and AD cohorts. Comprehensive protocols are available online in the study manual and ADNI-3 protocol.
Participants
Cognitively unimpaired (CU) older adults, aged 55-90 years old, were recruited at baseline. Participants were confirmed to have no impaired cognitive function based on informant reports, neuropsychiatric test results, laboratory tests, physical examination, Clinical Dementia Rating (CDR), and comprehensive physician evaluation. Specific inclusion criteria included a Mini-Mental State Examination (MMSE) score between 25-30, a CDR score of 0, and higher Wechsler Memory Scale Logical Memory (WMS-LM) delay scores than predefined cutoff values based on education level. Participants with a Geriatric Depression Scale (GDS) score higher than 6 were excluded, as were individuals with a history of head trauma, other neurological or major psychiatric disorders, and alcohol or drug abuse. Vascular risk factors (VRFs) were recorded based on medical history, including hypertension, hyperlipidemia, diabetes, smoking history, and cardiovascular history. If each item is positive, it will be recorded as 1 point, and the total VRFs score (0-5 points) will be obtained. Out of the 414 participants, 104 (25.1%), 240 (57.9%), and 141 (34.0%) had follow-up visits with the FCI-SF at one, two, and four years after baseline imaging.
APOE genotyping for all participants was performed as previously described [20]. Briefly, APOE genotyping for all subjects was performed using the DNA extracted from peripheral blood cells. The cells were collected in single EDTA plastic tubes (10 ml) and were sent via overnight delivery, at room temperature, to the University of Pennsylvania AD Biofluid Bank Laboratory. At baseline, among the 414 participants, there were 124 carriers of the APOE ɛ4 allele and 268 non-carriers, as not everyone had blood samples. Follow-up processes at 1, 2, and 4 years included 46 carriers and 57 non-carriers at the first year, 77 carriers and 161 non-carriers at the second year, and 50 carriers and 90 non-carriers at the fourth year, respectively.
Financial capacity instrument-short form
The Financial Capacity Instrument –Short Form (FCI-SF) is described as comprising 37 items, further categorized into five domain scores: Mental Calculation (MC), Financial Conceptual Knowledge (FC), Single Checkbook/Register Task (SNG), Complex Checkbook/Register Task (COM), and Bank Statement (BANK). The total score on the FCI-SF ranges from 0 to 74, with each sub-domain score having its own specific range: MC (0-4), FC (0-8), SNG (0-20), COM (0-28), and BANK (0-14). Higher scores on the FCI-SF indicate better financial capacity. Additionally, the FCI-SF considers the time required to complete specific tasks. The maximum time for the overall timing score (total composite time, TIME) is 720 s (12 min). In this analysis, we utilized the FCI-SF (total score and sub-domain score) as well as TIME.
MRI acquisition
MRI data were acquired using 3T scanners from various sites with the following parameters: 1) 3D T1-weighted imaging (T1WI): TR (Repetition Time)=7.36 ms; TE (Echo Time)=3.05 ms; TI (Inversion Time)=400 ms; Flip angle = 11°; Voxel size = 1×1×1 mm3; Field of view = 256; Number of slices = 196. 2) 3D fluid-attenuated inversion-recovery (FLAIR): Repetition time = 4800 ms; Echo time = 441 ms; Inversion time = 1650 ms; Voxel size = 1.2×1×1 mm3; 3) 2D Axial T2* acquired using a gradient recalled echo (GRE): Repetition time = 650 ms; Echo time = 20 ms; Voxel size = 0.85×0.85×4 mm3; For MRI standardization details, visit http://www.adni-info.org.
Core AD biomarkers
As per NIA-AA Alzheimer’s research criteria, AD diagnosis involves abnormal core AD biomarkers like fluid Aβ42/40, ptau, amyloid PET, or neocortical tau PET [21]. Hippocampus volume holds significance despite its non-specificity in AD pathogenesis. In this study, considering the relationship between financial capacity and the three identified pathologies from previous research, the positive status of amyloid and tau proteins, as well as hippocampal volume, were included as covariates in the analysis [9, 19].
Data for tau PET and amyloid PET were obtained from the ADNI3 database. Specifically, amyloid PET was acquired using two radiotracers (Florbetapir or Florbetaben), while tau PET was conducted using flortaucipir. The ADNI PET processing pipeline, as previously described [22], was employed for PET data correction, involving the following steps: 1) collecting pre-processed PET and MR data and co-registering PET to MRI images; 2) defining regions of interest and reference regions through FreeSurfer; 3) extracting volume-weighted means from cortical summary regions; 4) calculating the summary amyloid SUVR by dividing cortical summary regions by the whole cerebellum, and calculating the summary tau SUVR by dividing MetaTemporal regions (Freesurfer-defined bilateral entorhinal, amygdala, fusiform, inferior, and middle temporal cortices) by the inferior cerebellar grey matter. Amyloid positivity was determined by a summary amyloid SUVR greater than 1.08 and 1.11, respectively. Positive tau status was defined as a summary tau SUVR greater than 1.27 [23, 24]. In the study, 384 participants (92.8%) and 364 participants (87.9%) out of 414 completed the baseline amyloid and tau PET scans, respectively.
Hippocampus volume (HV) and total intracranial volume (TIV) data were obtained [25]. Bilateral HV averaged and divided by TIV to derive corrected HV (tHV) for subsequent analyses.
WMH quantification
WMH were quantified using an established segmentation method [15]. Lesion maps were auto-generated from T1-weighted and FLAIR images via the Lesion Segmentation Toolbox (https://www.{}applied-statistics.de/lst.html). An expert radiologist manually improved mask accuracy. These masks and T1, FLAIR images were co-registered to the UNC adult brain atlas template (http://www.nitrc.org). Due to TIV and WMH distribution skewness, TIV-corrected WMH underwent a log transformation (lgtWMH) for analysis.∥
Rating of dPVS, lacune, and CMB
To assess dilated perivascular spaces (dPVS), high-resolution 3D-T1WI was utilized due to the absence of T2-weighted images in the ADNI3 database. dPVS were identified as <3 mm diameter, CSF-like signal lesions. They were round, oval, or linear, aligned perpendicularly to brain surface and parallel to vessels. The severity of dPVS was rated based on their numbers, and separately for those in the basal ganglia (BG-dPVS) and centrum semiovale (CSO-dPVS) as previously [15].∥In FLAIR data, lacune were defined as CSF-like hypointensity with surrounding hyperintensity rim, 3–15 mm diameter. Lacune presence was recorded. CMB referred to hypointense foci, 2–5 mm diameter, on T2*-weighted images [26]. CMB presence was recorded.∥
Total SVD burden score
We calculated SVD burden using a point system based on four markers [18]. The total MRI burden of SVD was rated on an ordinal scale ranging from 0 to 4, determined by the presence of each of the 4 MRI features of SVD. We defined the presence of lacunes and CMB as the presence of one or more lacunes (1 point if present) or any CMB (1 point if present). The presence of PVS was counted if there were moderate to severe (grade 2–4) PVS in the basal ganglia (1 point if present). The presence of WMH was defined as either (early) confluent deep WMH (Fazekas score 2 or 3) or irregular periventricular WMH extending into the deep white matter (Fazekas score 3) (1 point if present).∥
Inter-rater agreement on SVD markers
Two trained radiologists, blinded to clinical data, evaluated SVD scores. Inter-rater consistency was assessed using Cohen’s kappa coefficient, yielding strong agreements for WMH (Kappa = 0.81), dPVS (Kappa = 0.83), lacune (Kappa = 0.88), and CMB (Kappa = 0.87). Discrepancies were resolved through discussion.∥
Statistical analysis
All statistical analyses were performed using R software (R Foundation for Statistical Computing, V4.2.1).∥
Association between SVD and FCI-SF at baseline
To examine the relationship between SVD and FCI-SF performance, we employed a linear regression analysis while controlling for various covariates including age, sex, education, amyloid, tau, tHV, and VRFs. Each SVD imaging marker (SVD total scores, lgtWMH, BG-dPVS, CSO-dPVS, CMB number, and lacune number) was individually designated as an independent variable. The dependent variables consisted of both the FCI-SF and 6 subdomains (i.e., MC, FC, SNG, COM, BANK, TIME). To address the issue of inflated Type I error due to multiple comparisons across the seven different FCI-SF metrics, we applied the False Discovery Rate (FDR) method for multiple correction. We set p-values below 0.05 following this correction as statistically significant. To investigate whether APOE ɛ4 allele carriers could strengthen the effect of SVD on financial capacity, additional linear regression models were performed for APOE ɛ4 allele carriers to assess the association between SVD and FCI-SF performance in APOE ɛ4 allele carriers.∥
Association between SVD and longitudinal changes of FCI-SF
We examined the impact of SVD severity on longitudinal trajectories of FCI-SF scores using linear mixed-effects models (LMM; R, “lmerTest”). LMM can effectively handle the hierarchical nature of longitudinal, repeated-measures data, with missing data accounted for using maximum likelihood estimation. We modeled changes in FCI-SF total score and each FCI-SF subdomain over the 4-year follow-up period. Due to the limited number of participants followed at 3 years from baseline, we only included the time points at 1 year, 2 years and 4 years from baseline.∥FCI-SF total score and each FCI-SF subdomain (i.e., MC, FC, SNG, COM, BANK, TIME) were set as dependent variables separately. SVD severity, including the total SVD score and SVD indicators (log-transformed tWMH, dPVS-BG, dPVS-CSO, lacune and CMB number), was fed into the model. Follow-up time point (i.e., the number of years from baseline) was modelled as a random effect (random intercepts and slopes) for each participant. The interaction between SVD and follow-up time point (years from the SVD assessment) was modelled to determine if these metrics were associated with FCI-SF changes over the follow-up period (e.g., time×SVD metrics).
Initially, we established a model incorporating age (at the time of SVD assessment), sex, and education as fixed effects. Subsequently, to account for multiple comparisons, we applied the FDR method and considered p-values below 0.05 post-correction as statistically significant. For the identified significant results, we extended our analysis by introducing AD-related pathologies (including amyloid and tau status, and tHV measured at time 0) as well as VRFs as additional covariates.
RESULTS
Demographics
Demographics, cerebral vessel disease, and AD pathologies in all cognitive unimpaired participants, APOE ɛ4 carriers, and non-carriers
SVD, small vessel disease; WMH, white matter hyperintensities; BG and CSO dPVS, basal ganglia and centrum semiovale dilated perivascular space; CMB, cerebral microbleeds; AD, Alzheimer’s disease; TIV, total intracranial volume. *p < 0.05 represents the significant difference between cognitive unimpaired APOE ɛ4 carriers and non-carriers. In the study, 384 (92.8%) and 364 (87.9%) out of 414 participants completed the amyloid and tau PET scans, respectively.
Cross sectional relationship between SVD and FCI-SF scores
After adjusting for age, sex, education, VRFs, and AD pathologies, no significant correlation was found between SVD total score and FCI-SF scores (total and sub-items) or composite time in the overall participants or APOE ɛ4 carriers (p > 0.05).
Regarding individual SVD markers, baseline WMH was associated with BANK (standardized β= –0.194, FDR-p = 0.004), and lacune number was associated with FC (standardized β= –0.171, FDR-p = 0.010). Notably, these associations exhibited increased strength in APOE ɛ4 carriers, with standardized β= –0.282 for the relationship between WMH and BANK (FDR-p = 0.031), and standardized β= –0.366 for the correlation between lacune number and FC (FDR-p = 0.001). While we didn’t find an association of cerebral microbleeds (CMB) with all FCI-SF scores, a significant association was observed between CMB number and BANK in APOE ɛ4 carriers (standardized β= –0.257, FDR-p = 0.019). More details in Supplementary Table 2.
Longitudinal FCI scores changes and its association with baseline SVD burden
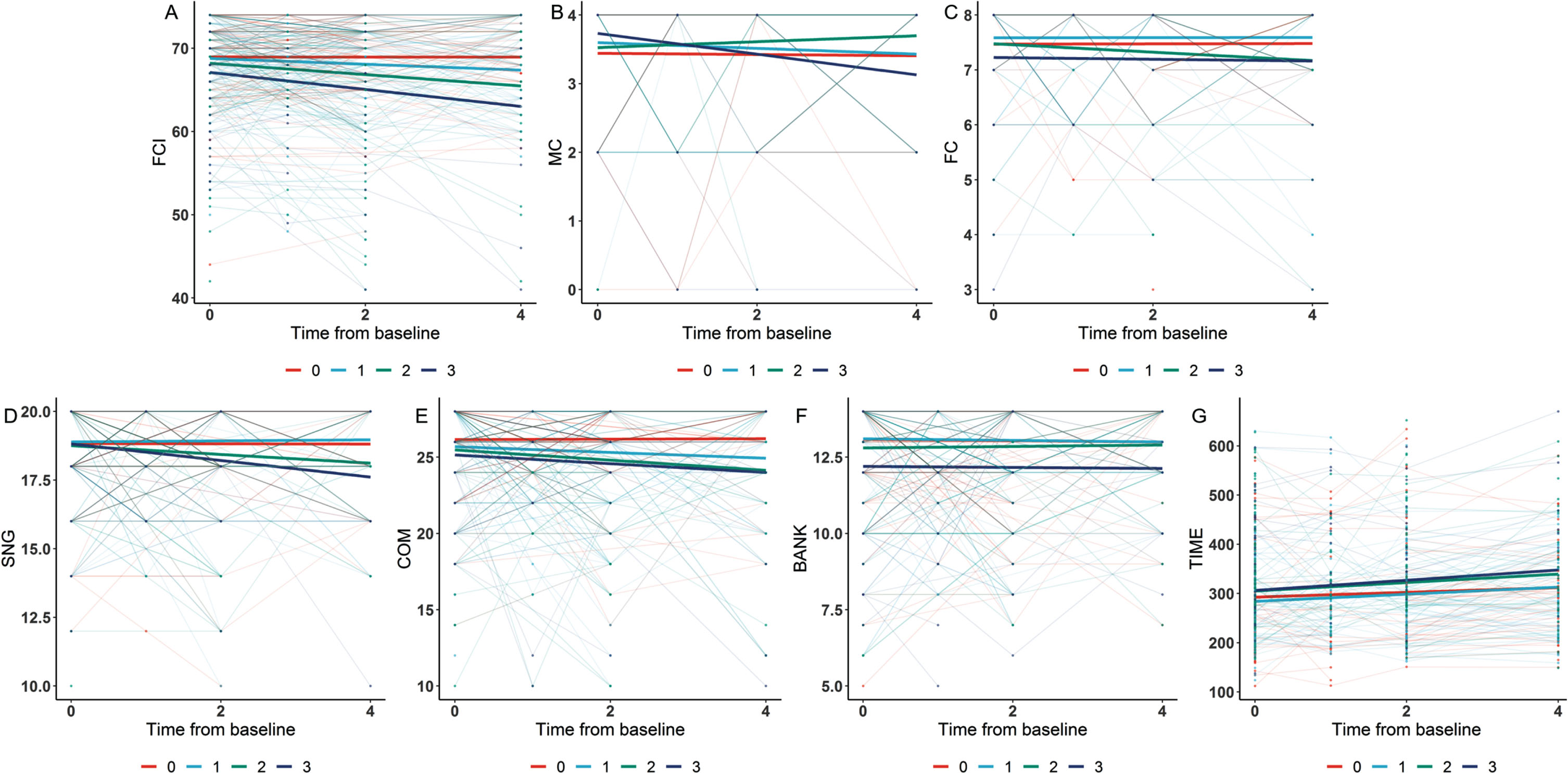
Longitudinally, a higher SVD total score at baseline was associated with a greater decline in FCI-SF total score (standardized β= –0.335, FDR-p = 0.007). A more severe WMH burden at baseline was associated with a greater decline in SNG (standardized β= –0.137, FDR-p = 0.007) and FC (standardized β= –0.052, FDR-p = 0.028). Notably, the association between baseline WMH and SNG changes was amplified in APOE ɛ4 carriers (standardized β= –0.187, FDR-p = 0.029). Figure 1 demonstrates a more pronounced decline in CU financial capacity among those with a higher SVD severity. The results were adjusted for age, sex, education, VRFs, and AD pathologies. More details in Supplementary Table 3.
DISCUSSION
We investigated the impact of SVD on financial capacity in CU older adults and found that participants with higher baseline SVD severity were associated with poorer baseline and long-term FCI-SF performance. In the presence of the APOE ɛ4 allele, these correlations were intensified. Our study suggests that strategies addressing SVD may preserve financial capacity for CU older adults, particularly for APOE ɛ4 carriers.
At the baseline level, we observed that the overall SVD score was not associated with any FCI-SF. However, at the longitudinal level, participants with lower baseline scores on the SVD severity scale exhibited a correlation with poorer future FCI-SF. Previous studies have indicated that SVD primarily affects executive function and information processing speed [27, 28]. Unexpectedly, we did not find a relationship between SVD total score and FCI-SF completion time at cross-sectional and longitudinal levels. However, previous studies in CU old adults reported that cortical amyloid burden was adversely associated with financial quickness, and mean cortical thickness is also associated with increased long-term financial complement time [9, 19]. We hypothesize that the ADNI database might have excluded individuals with severe SVD, potentially leading to a weakening of statistical results. Further diverse population validation is needed for confirmation.
Then we examined the link between individual SVD markers and financial capacity. Specifically, higher baseline WMH was independently associated with poor bank statement management. Interestingly, bank statement management has been identified as one of the most sensitive sub-domains of the FCI-SF in individuals with mild AD and MCI patients [10, 19]. Further, higher baseline WMH was associated with declining SNG performance. WMH is common in older adults’ MRI scans (prevalence 39–96%) [11]. WMH could damage long-distance fiber connections and disrupt the coordination among brain regions [29]. Accumulating studies demonstrated that WMH was associated with substantially increased risks of long-term cognitive impairment and daily living activities, particularly related to reduced information processing speed and executive dysfunction [30–33]. Our study emphasizes WMH prevention strategies. These include managing hypertension, obesity, diabetes, and hypercholesterolemia to protect financial and cognitive abilities in older adults.
Our study found that baseline CMB and lacune number were linked to FC and BANK, respectively. CMBs and lacune were traditionally considered “silent lesions” that did not manifest clinical symptoms. However, accumulating studies have shown that CMB and lacune are strongly associated with cognitive decline, especially in participants with three or more CMBs, or lacune occurs in strategic areas [12, 34]. Evidence from population-based studies supports that CMB and lacunes may have an important role in developing cognitive decline, especially executive function [31, 35–37]. Our research uniquely establishes the connection between CMBs, lacunes, and older adults’ financial capacity. We hypothesized that CMB and lacune might have a direct lesional effect by disrupting strategic brain networks [38] or an indirect effect through underlying diffuse microangiopathy [39].
Notably, we did not find any relationship between dPVS and financial capacity. The perivascular space is a fluid-filled space surrounding blood vessel that course from the subarachnoid space through the brain parenchyma. When perivascular space is visible in vivo on MRI, they are considered dPVS, widely used to reflect glymphatic dysfunction [40]. Many studies demonstrated that ePVS were associated with worse information processing, executive function, and visuospatial ability [41]. Thus, ePVS-related glymphatic dysfunction may contribute directly to the progressive decline in a financial capacity. The visual assessment of dPVS may have a floor effect in CU participants, masking any potential relationship with financial capacity. Future automated dPVS volume assessment may require additional validation to explore this connection [42].
The APOE ɛ4 allele is the most robust genetic risk factor for sporadic AD and is associated with cognitive decline in older adults [43]. In line with previous research, we observed that among APOE ɛ4 carriers, SVD had a more pronounced negative long-term impact on financial capacity. There are two plausible explanations for these findings. On the one hand, our previous work showed that APOE ɛ4 was associated with more severe SVD in CU older participants and might accelerate the progression of SVD, especially WMH [15]. Additionally, APOE ɛ4 carriers experience accelerated AD-related pathology progression, such as amyloid burden and hippocampal atrophy, previously tied to financial capacity decline [9, 19].
We acknowledge several study limitations. Firstly, our sample consisted of highly educated individuals (mean education: 16.8±2.3 years), potentially limiting the generalizability of findings to diverse educational backgrounds. Secondly, while the FCI-SF is relevant for the baby boomer generation, its applicability might diminish with the evolution of electronic payment systems and financial technology. Additionally, the focus of our study was primarily on the effects of baseline SVD and AD pathologies on future changes in financial capacity. As SVD progresses slowly over a span of four years, validation with longer follow-up databases is needed for stronger results.
AUTHOR CONTRIBUTIONS
Xiao Luo (Conceptualization; Data curation; Funding acquisition; Investigation; Writing – original draft; Writing – review & editing); Hui Hong (Data curation; Formal analysis; Methodology; Writing – original draft; Writing – review & editing); Kaicheng Li (Data curation; Formal analysis; Validation); Qingze Zeng (Methodology; Validation; Writing – review & editing); Xiaocao Liu (Data curation; Investigation; Methodology); Luwei Hong (Data curation; Formal analysis; Writing – original draft); Jixuan Li (Data curation; Resources; Software); Xinyi Zhang (Data curation; Software; Validation); Siyan Zhong (Data curation; Formal analysis; Writing – review & editing); Xiaopei Xu (Conceptualization; Data curation; Visualization); Yanxing Chen (Conceptualization; Data curation; Software; Writing – original draft; Writing – review & editing); Minming Zhang (Project administration; Writing – original draft; Writing – review & editing); Peiyu Huang (Conceptualization; Data curation; Formal analysis; Methodology; Project administration; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
We extend our heartfelt gratitude to the patients, researchers, and clinicians who generously contributed to the ADNI database. Your invaluable support greatly facilitated this research. Thank you for your dedicated participation in advancing scientific knowledge in this field.
FUNDING
This work was made possible with the support of the National Natural Science Foundation of China (grant numbers 82271936, 82371907) and the Zhejiang Natural Science Foundation (grant number 2021RC060, Z24H180011). Furthermore, we acknowledge the funding received from the Zhejiang Province Traditional Chinese Medicine Youth Talent project (grant number 2022ZQ057).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
Data are available upon reasonable request. The data sets generated for this study are available on request to the senior author, for non-commercial academic studies, but may be subject to some restrictions according to consent and confidentiality.