
Abstract
Background:
Patients with transient ischemic attack (TIA) or ischemic stroke demonstrate an increased risk of cognitive dysfunction. Accumulating evidence indicates that ischemic cerebrovascular disease (ICVD) may interact with the amyloid/tau/neurodegeneration (AT[N]) biomarkers to promote dementia. However, the precise pathological mechanisms remain to be fully characterized.
Objective:
To elucidate the interrelationships among ICVD, ATN biomarkers in cerebrospinal fluid (CSF), and cognition.
Methods:
A total of 2524 participants were recruited from the CABLE study. ICVD referred to TIA/ischemic stroke. Cognitive performance was assessed by China Modified Mini-Mental State Examination (CM-MMSE) and Montreal Cognitive Assessment-b (MoCA-b). Multivariate linear regression analyses were performed to evaluate the associations of ICVD with CSF ATN biomarkers and cognition. Causal mediation analyses were used to identify whether the association was mediated by ATN biomarkers.
Results:
ICVD was associated with higher total-tau (t-tau) (p = 2.828×10–2) and poorer cognition (CM-MMSE: p = 1.539×10–5, MoCA-b: p = 4.552×10–6). Additionally, no discernible correlation surfaced between ICVD and amyloid-β (Aβ) 42 (p = 6.910×10–1) or phosphorylated tau (p-tau) (p = 4.324×10–1). The influence of ICVD on cognitive function was partially mediated by CSF t-tau (CM-MMSE: proportion: 2.74%, MoCA-b: proportion: 2.51%). Subgroup analyses revealed the influences of t-tau were especially evident in male (CM-MMSE: proportion: 5.45%, MoCA-b: proportion: 5.38%) and mid-life group (CM-MMSE: proportion: 9.83%, MoCA-b: proportion: 5.31%).
Conclusions:
These results delineated t-tau as a potential mediator for the influence of ICVD on cognition. Targeting brain ischemia and alleviating neuronal injury induced by ischemia may be a promising approach for preventing cognitive decline.
INTRODUCTION
The incidence of cerebrovascular disease has increased in recent years, and the most frequent subtype is ischemic cerebrovascular disease (ICVD) [1]. As estimated in China, over 20 million people may have suffered transient ischemic attack (TIA) [2], and over 100 million suffered ischemic stroke [3]. Globally, stroke remained one of the leading causes of death [4]. ICVD was found to be subsequentially associated with cognitive decline or even dementia. By harmonizing data from 13 studies based in 8 countries, studies found that cognitive impairment after stroke or TIA was common and evident [5]. Ischemic stroke could lead to an elevated risk of dementia over time, and bring forward the occurrence of dementia [6].
Estimations from the World Alzheimer Report 2015 suggested over 40 million people worldwide have dementia, with expectations to increase to 70 million by 2030 and 130 million by 2050 [7]. Among the subtypes of dementia, Alzheimer’s disease (AD) covers the largest part, and the typical pathological alterations lie in amyloid-β (Aβ) deposition and intracellular tau accumulation [8]. Brain ischemia could contribute to AD pathology, with the manifestation of pathological alterations in amyloid and tau protein [9]. However, the relationship between brain ischemia and amyloid/tau/neurodegeneration (AT[N]) biomarkers in cerebrospinal fluid (CSF) remains controversial. It has been suggested that CSF Aβ42 showed no significant changes after ischemic stroke, whereas CSF tau increased remarkably and was well correlated with the size of the infarct [10]. In contrast, another study pointed out that the patients with ischemic vascular pathology had significantly lower levels of CSF Aβ42 levels than the controls [11]. Besides, although ICVD as well as ATN biomarkers have been revealed to drive cognitive decline independently [12–14], it is also disputed whether the way TIA/ischemic stroke contributes to cognitive decline is through the pathway of ATN biomarkers [15–18].
Motivated by these prior findings, we performed this study, with the following aims: 1) to investigate the associations between ICVD and cognitive performance; 2) to examine the relationships between ICVD and CSF ATN biomarkers; and 3) to elucidate whether the effect of ICVD on cognition is mediated through ATN biomarkers.
METHODS
Participants
The study was conducted based on the Chinese Alzheimer’s Biomarker and LifestylE (CABLE) study. CABLE, an ongoing and in-depth study, has been conducted since the wave of 2017. It aims to investigate the modifiers and biomarkers of AD in the northern Chinese Han population between 40 to 90 years. Participants who completed comprehensive assessments across clinical, neuropsychological, psychosocial, and psychiatric domains and provided blood and CSF samples were enrolled in this study. China Modified Mini-Mental State Examination (CM-MMSE) and Montreal Cognitive Assessment-b (MoCA-b) were used as the measurements to assess global cognitive performance. The study only included the qualified data with complete assessments. All the assessments and bio-sample collection were undergone by experienced doctors with previously standard training. This study was approved by the Institutional Review Board of Qingdao Municipal Hospital and adhered to the principles of the Helsinki Declaration. Written consents were obtained by the patients themselves or their close relatives.
The exclusion criteria were as follows: 1) epilepsy, multiple sclerosis, central nervous system infection, and other major neurological disorders, 2) severe psychological disorders (e.g., major depressive disorder or generalized anxiety disorders), 3) advanced cancers, and 4) genetic diseases. Finally, 2,524 adults were enrolled in this cross-sectional study. Participants were categorized into mid-life (<65 years: n = 1350) and late-life (≥65 years: n = 1174) groups based on a cut-off age of 65 years (Fig. 1).

Flowchart of the study. Flowchart depicting the step-by-step selection and data analyses of the study. AD, Alzheimer’s disease; APOE, apolipoprotein E; Aβ, amyloid-β; ICVD, ischemic cerebrovascular disease; CM-MMSE, China-Modified Mini-Mental State Examination; MoCA-b, Montreal cognitive assessment – basic; p-tau, phosphorylated tau; t-tau, total tau.
Information of ICVD
ICVD (TIA or ischemic stroke) diagnosis was based on electronic medical records from the hospital and face-to-face interviews using a structured questionnaire. The initial diagnoses were then confirmed by two experienced clinical neurologists. The diagnosis identified from the hospital records was followed by the International Classification of Diseases (ICD)-10 coding. TIA was defined as a transient episode of neurological dysfunction caused by focal brain ischemia less than 24 h without acute infarction. Ischemic stroke was defined as an episode of neurological dysfunction caused by focal cerebral infarction persisting for more than 24 h [19]. The questionnaire asked for detailed information on whether the participants ever suffered ICVD, the exact diagnosed years, and the treatments of the disease.
CSF ATN biomarkers assessments
CSF samples were collected by lumbar puncture into 10-ml polypropylene tubes and transported to the laboratory within 2 h. Upon arrival, samples were centrifuged at 2000 g for 10 min. The thaw/freezing cycles were restricted to no more than two times. Levels of Aβ42, p-tau, and t-tau in CSF were determined with the enzyme-linked immunosorbent assay lit (Innotest; Fujirebio, Ghent, Belgium) on the microplate reader (Multiskan MK3; Thermo Fisher Scientific, Waltham, MA). All biochemical assays were performed in duplicate by trained technicians blinded to clinical information. Precision values of within-batch were < 5% and the inter-batch coefficients of variation were < 15%.
APOE ɛ4 genotyping
Genomic DNA was extracted from peripheral blood samples obtained after overnight fasting using the QIAamp DNA Blood Mini Kit (250). APOE ɛ4 genotyping was performed by PCR amplification using primers 50-ACGGCTGTCCAAGGAGCTG-30 (rs429358) and 50-CTCCGCGATGCCGATGAC-30 (rs7412) followed by restriction fragment length polymorphism (RFLP) analysis.
Covariates
Age and sex were obtained from the medical record system. Height and weight were measured by experienced nurses to calculate body mass index (BMI). The information on vascular risk factors was obtained by structured questionnaire and medical records, and it included diabetes mellitus (plasma glucose levels [fasting glucose level≥7.0 mmol/L or postprandial glucose level≥11.1 mmol/L], or a 75-g oral glucose tolerance test according the 1998 World Health Organization criteria, or by the use of oral hypoglycemic agents or insulin), hyperlipidemia (i.e., total cholesterol≥5.6 mmol/L or low-density lipoprotein cholesterol≥3.1 mmol/L, or high-density lipoprotein cholesterol < 0.8 mmol/L, or triglyceride≥1.9 mmol/L, or the use of lipid-regulating drugs), coronary heart disease (coronary atherosclerosis, angina, or acute coronary syndrome), and atrial fibrillation (based on electrocardiogram). Smoking and drinking status were determined based on previous or current tobacco and alcohol use, respectively.
Statistical analysis
First, for the comparison of the difference in basic characteristics between ICVD and non-ICVD groups, categorical variables were compared using the χ2 test or Fisher’s exact test, while continuous variables were compared using the Mann-Whitney U test.
Then, we used multiple linear regression (MLR) models to test the associations of ICVD, CSF ATN biomarkers, and cognitive performance. Adjusted covariates included age, sex (female = 0, male = 1), BMI, smoking (yes = 1), drinking (yes = 1), APOE ɛ4 status (“rs429358” or “rs7412” = 1, other genotypes = 0), and years of education. Subgroup analyses stratified by age, sex, and APOE ɛ4 status were conducted for sensitivity analyses.
Further, to identify whether the association between ICVD and cognitive performance was mediated by ATN biomarkers, we conducted mediation analyses with the methods set by Baron and Kenny [20]. In the first equation, CSF ATN biomarkers were modeled as the mediator and ICVD as the independent variable. In the second equation, cognitive test scores were modeled as the dependent variable and ICVD as the independent variable. In the third equation, cognitive test scores were modeled as the dependent variable, ICVD as the independent variable, and CSF ATN biomarkers as the mediator. Mediation effects were established only if it simultaneously met the following criteria: 1) ICVD was significantly associated with CSF ATN biomarkers; 2) ICVD was significantly associated with cognitive test scores; 3) CSF ATN biomarkers were significantly associated with cognitive test scores; and 4) The association between ICVD and cognition was weakened when CSF ATN biomarkers (the mediator) were added in the regression model. Additionally, the attenuation or indirect effect was evaluated, using 10,000 bootstrapped iterations. The above-mentioned regression models were controlled for age, sex, BMI, drinking, smoking, APOE ɛ4 status, and years of education. MLR models were all z-scored. The “lm”, “mediate”, and “car” packages in R version 4.2.0 software (R Project for Statistical Computing; http://www.r-project.org) were used to accomplish the analyses conducted in the study. All figures were created using the “pheatmap” package in R version 4.2.0 and GraphPad Prism 9.0.
RESULTS
Participant characteristics
The characteristics of the study participants were summarized in Table 1. Among the 2,524 individuals included in the study, a total of 1,522 (60.3%) participants were male, and 347 (15.98%) were APOE ɛ4 carriers. The mean age was 62.97 years and the mean years of education were 9.26. Regarding cognitive performance, the mean score of CM-MMSE was 27.01 with a range from 0 to 30, and the mean score of MoCA-b was 22.38 with a range from 0 to 30. Besides, a total of 1296 participants were cognitively normal, whereas 1,228 were diagnosed with mild cognitive impairment. Of all the participants, 176 individuals had ICVD, with 27 classified as TIA and 149 as ischemic stroke. The ICVD group tended to be older (p < 0.0001), and had a higher prevalence of vascular risk diseases (hyperlipidemia [p < 0.0001], hypertension [p < 0.0001], diabetes mellitus [p < 0.0001], coronary heart disease [p < 0.0001], and atrial fibrillation [p = 0.0336]) compared to the no-ICVD group.
Characteristics of participants
Bold p values indicated the results were significant between groups. Aβ, amyloid-β; APOE, apolipoprotein E; BMI, body mass index; CHD, coronary heart disease; CM-MMSE, China-Modified Mini-Mental State Examination; ICVD, ischemic cerebrovascular disease; MoCA-b, Montreal cognitive assessment – basic; p-tau, phosphorylated tau; SD, standard deviation; t-tau, total tau.*The significance of difference among groups was examined by the Mann-Whitney U test.✢ The significance of difference among groups was examined by the Pearson’s χ2 test.✧ The significance of difference among groups was examined by the Fisher’s exact test.
The associations of ICVD, CSF ATN biomarkers, and cognition
Participants with ICVD had poorer performance on cognitive tests (Fig. 2: CM-MMSE, p < 0.0001; MoCA-b, p < 0.0001) than no-ICVD individuals. Mean CM-MMSE score was 25.63 in the ICVD group versus 27.11 in the no-ICVD group. Similarly, the ICVD cohort achieved lower mean MoCA-b score relative to the no-ICVD participants (20.33 versus 22.53). Besides, the ICVD group exhibited elevated t-tau levels (Fig. 2, p = 0.0063). However, CSF Aβ42 and p-tau did not significantly differ between the two groups (p > 0.05 for both comparisons) (Fig. 2).
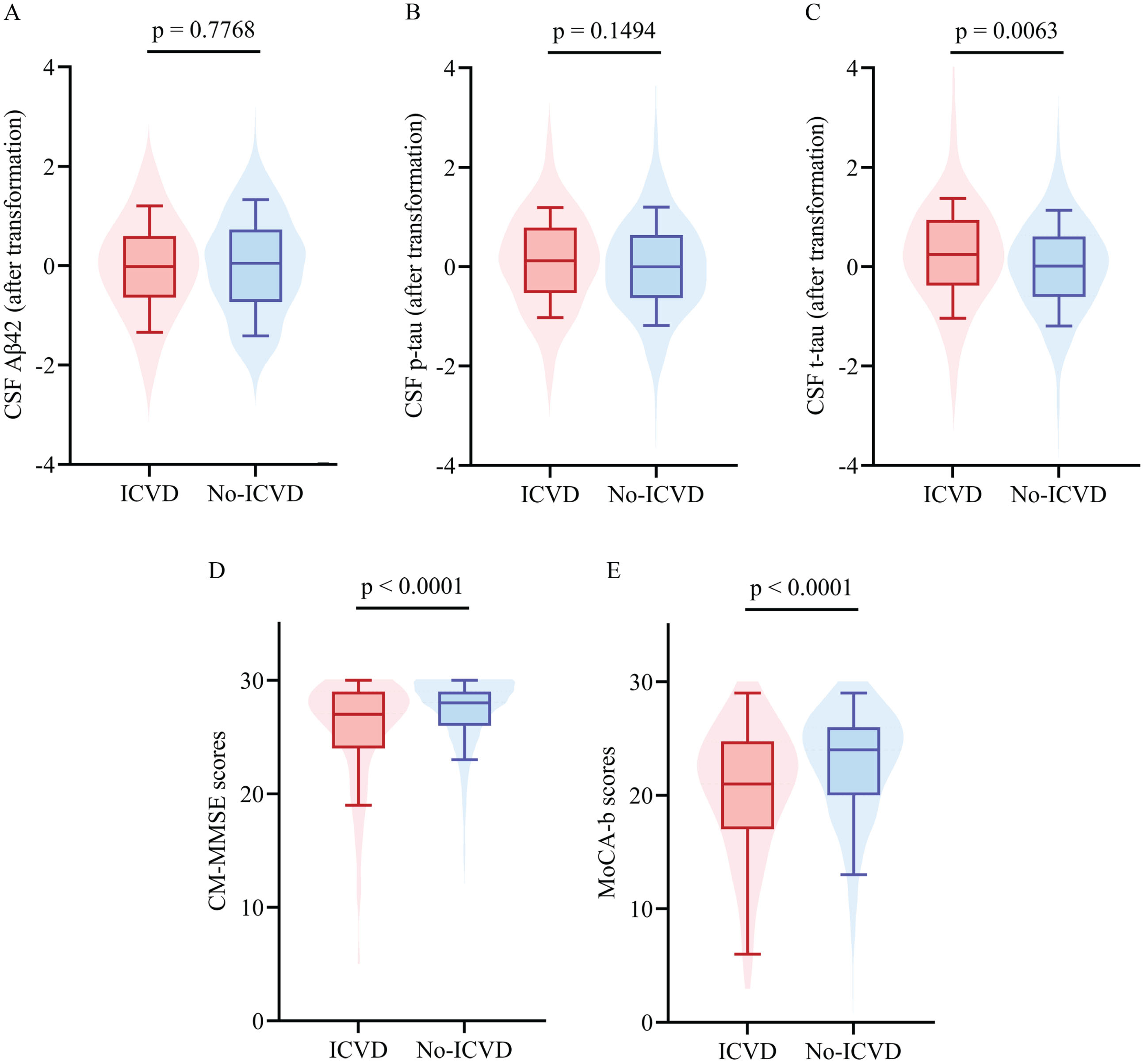
Associations of ICVD with CSF ATN biomarkers and cognition. Differences in AD biomarker levels and cognitive performance were examined by the Mann-Whitney U test. Compared with the no-ICVD group, ICVD participants had higher levels of t-tau and poorer cognitive performance. Aβ, amyloid-β; CM-MMSE, China-Modified Mini-Mental State Examination; IS, ischemic stroke; MoCA-b, Montreal cognitive assessment-basic; p-tau, phosphorylated tau protein; TIA, transient ischemic attack; t-tau, total tau protein.
MLR models demonstrated associations between ICVD and t-tau (β= 0.205, p = 2.828×10–2) as well as cognitive performance (CM-MMSE: β= –0.299, p = 1.539×10–5; MoCA-b: β= –0.324, p = 4.552×10–6) (Fig. 3). However, there was no associations between ICVD and CSF Aβ42 (p = 6.910×10–1) or p-tau (p = 4.324×10–1). To examine whether these findings could be observed in specific subgroups, we conducted stratified analyses categorized by age, sex, and APOE ɛ4 carrier status. It turned out that the associations between ICVD and higher levels of CSF t-tau were only found in the subgroup of males (β= 0.340, p = 5.094×10–3), mid-life (β= 0.776, p = 4.699×10–5), and APOE ɛ4 carriers (β= 0.457, p = 2.901×10–2). However, ICVD conferred significantly poorer cognitive performance across all subgroups examined (Fig. 4, Supplementary Table 1). Moreover, results of interaction analyses on these unmodifiable factors were all insignificant (p > 0.05, Supplementary Table 2).
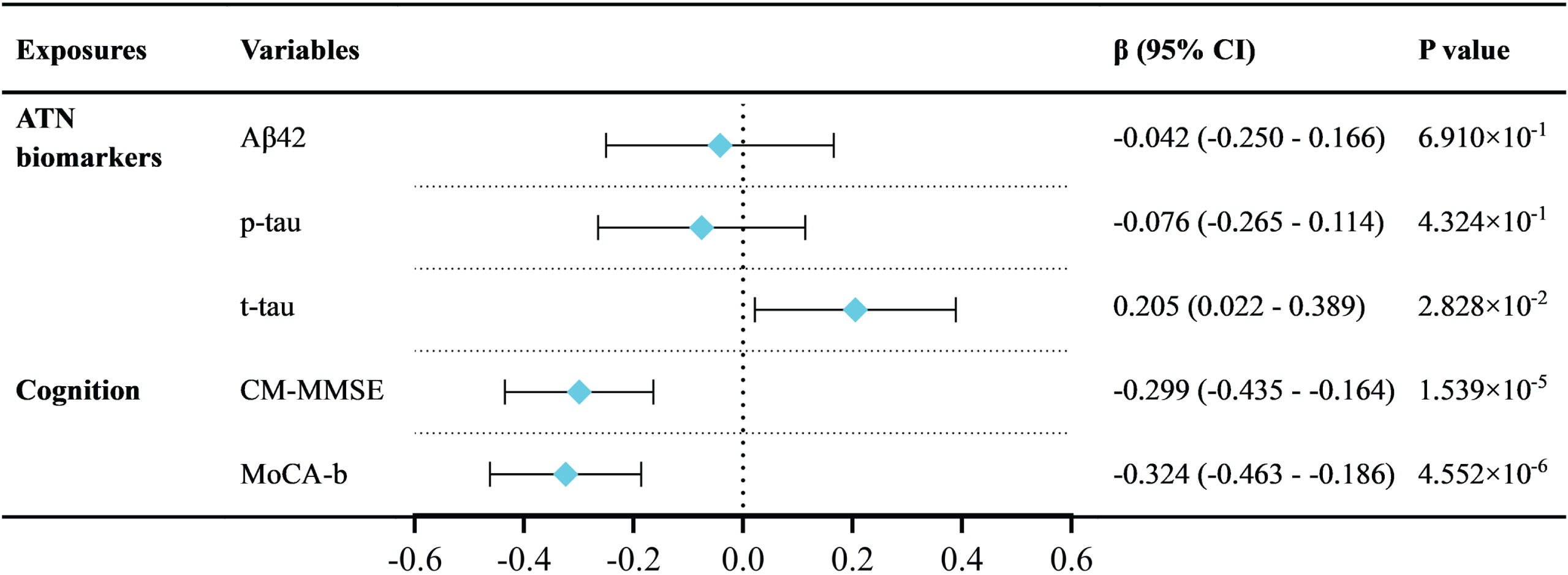
The linear relationships among ICVD, CSF ATN biomarkers, and cognition. Adjusted for age, sex, BMI, APOE ɛ4 status, drinking, smoking, and years of education. ICVD was associated with higher levels of CSF t-tau and poorer cognitive performance. The patchwork patterns by rhombus represent the β value, and the horizontal lines across the spot represent 95% CI of the β. Aβ, amyloid-β; ICVD: ischemic cerebrovascular disease; CM-MMSE, China-Modified Mini-Mental State Examination; MoCA-b, Montreal cognitive assessment – basic; p-tau, phosphorylated tau protein; t-tau, total tau protein.
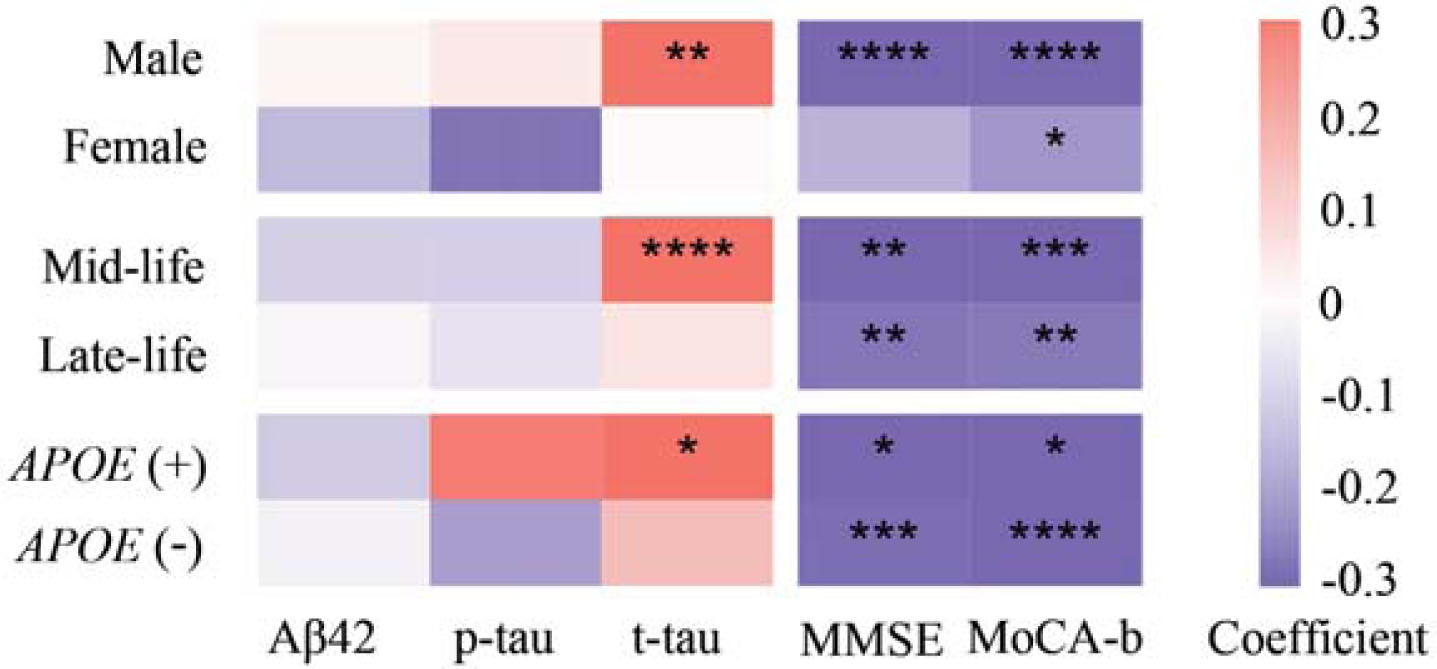
Heatmap for subgroup analyses of the relationships among ICVD, CSF ATN biomarkers, and cognition. CSF t-tau showed significant or suggestive associations with ICVD in subgroups of male, mid-life, and APOE ɛ4 carriers. Adjusting for age, sex, APOE ɛ4 status, drinking, smoking, and years of education. The associations between ICVD and higher levels of CSF t-tau were only found in the subgroup of male, mid-life, and APOE ɛ4 carriers. ICVD was significantly associated with cognitive performance in all subgroups. Aβ, amyloid-β; APOE, apolipoprotein E; ICVD, ischemic cerebrovascular disease; CM-MMSE, China-Modified Mini-Mental State Examination; MoCA-b, Montreal cognitive assessment-basic; p-tau, phosphorylated tau protein; t-tau, total tau protein.*p < 0.05;**p < 0.01;***p < 0.001;****p < 0.0001.
Causal mediation analyses
Collectively, the results showed that ICVD was not only significantly associated with cognition, but also related CSF t-tau. Thus, we further examined whether ICVD could lead to cognitive decline by modulating CSF t-tau. We found that t-tau partially mediated the association between ICVD and cognition, and the mediation proportion was 2.74% when measured by CM-MMSE (p = 0.030) and 2.51% when measured by MoCA-b (p = 0.037) (Fig. 5A). Moreover, consistent results were observed in the subgroups of male (CM-MMSE: proportion = 5.45%, p = 0.006; MoCA-b: proportion = 5.38%, p = 0.015) (Fig. 5B) and mid-life (CM-MMSE: proportion = 9.83%, p = 0.006; MoCA-b: proportion = 5.31%, p = 0.051) (Fig. 5C). Upon excluding participants with a cognitive test score of 0, the consistency of the results was maintained (Supplementary Figure 1).

CSF t-tau mediated association between ICVD and cognitive decline. Mediation effects of CSF t-tau are shown in total (A), male (B), and mid-life (C). Adjusting for age, sex, years of education, drinking, smoking, and APOE ɛ4 status. IE, indirect effect, ICVD, ischemic cerebrovascular disease; CM-MMSE, China-Modified Mini-Mental State Examination; MoCA-b, Montreal cognitive assessment-basic; p-tau, phosphorylated tau protein; t-tau, total tau protein.
DISCUSSION
In this large-scale study, we made three key observations. First, ICVD was significantly related to cognitive impairment. Second, ICVD was associated with a higher CSF t-tau. Third, the association between ICVD and cognitive decline was partially mediated by t-tau. Notably, these results were pronounced in the subgroup of male and mid-life participants. Taken together, our results indicated that ICVD was not significantly associated with hallmarks of AD pathological changes, as assessed by CSF Aβ42 and CSF p-tau. However, ICVD correlated closely with elevations in total tau, a marker of neuronal injury, which in turn contributed to cognitive decline.
Numerous studies have demonstrated that ICVD is associated with cognitive decline. Micro-infarctions in the brain could contribute to the likelihood of dementia [21], one or more infarctions lead to increased odds of dementia by 2.80-fold [18], while another study showed that persons with one or more infarctions had poor cognitive performance in multiple cognitive domains [22]. Besides, animal experiments also showed strong evidence of this viewpoint. Cerebral ischemia in mice can induce spatial learning and memory impairment [23].
In line with previous studies, we found that ICVD was associated with a heavier t-tau in CSF, and this finding was consistent with multiple previous studies. Furthermore, one investigation delineated a substantial correlation between ICVD and neurodegeneration linked to total tau [24]. Brain ischemia induced by mechanical resuscitation in hypothermic brain hypoxia was accompanied by a prompt release of tau protein [25]. Current evidence suggests several potential mechanisms that may underlie ICVD-related tau accumulation, including increased serum gelatinase activity leading to release of tau into the serum [26], blood-brain barrier disruption allowing influx of plasma tau [27], upregulation of tau gene expression [28], as well as other ischemic changes such as inflammation and impaired autophagy [29, 30]. However, further studies are still needed to fully elucidate the intricate interplays between ischemic cerebrovascular changes and t-tau.
We further found that the association between ICVD and CSF t-tau was more pronounced in APOE ɛ4 carriers. APOE ɛ4, the strongest genetic risk factor for AD, has also been associated with ICVD [31]. Besides, after acute ischemic stroke, APOE ɛ4 status was significantly related to cognitive decline [32]. There appears to be a synergistic effect between ischemic stroke and APOE ɛ4, stroke patients with APOE ɛ4 were more prone to dementia [33]. However, the underlying mechanism still needed to be clarified the phenomenon that APOE ɛ4 gene is found to be involved in tau-induced neurodegeneration [34]. Research has found that it accelerated the accumulation of tau in the entorhinal cortex [35]. In this way, it is postulated that ICVD may unmask pre-existing APOE ɛ4-related tau pathology by exhausting compensatory reserves in the vulnerable brain, thereby accelerating the manifestation of tau abnormalities.
Importantly, we found that t-tau may mediate the link between ICVD and cognitive decline. Besides, our results suggest that this mediation effect was more evident in males and middle-aged adults. Recent studies have revealed that the gender differences in stroke-related cognitive impairment and dementia may be attributable to the protective role of estrogen, which could persist for three decades after menopause. Besides, we also summarized the relationship between sex-related reproductive factors and dementia in a review, identifying that higher lifetime estrogen exposure was associated with lower risk of cognitive decline or dementia [36]. Additionally, in aged mice models, gonadal complement was shown to have protective effects [37]. Furthermore, among individuals with stroke or TIA, males demonstrate poorer baseline vascular risk profiles compared to females, which could further predispose them to dementia [38]. Taken together, this sex-specific difference may stem from the protective hormonal influences in women compared to men, coupled with the greater vulnerability of men to various vascular risk factors over the lifespan.
In contrast to our initial hypothesis, the effects were more pronounced in middle-aged adults. However, prior studies have indicated age-dependent differences in responses to ischemic injury [39]. As reported by an experiment exploring an ischemic stroke model, age could alter the immunological response after brain ischemia [40]. Notably, the younger mice exhibited more severe cerebral atrophy than the aging mice after brain ischemia, which may be owing to the pro-inflammatory milieu of the aging brain and the formation of glial scar [41]. Moreover, as indicated by a pilot study, age inversely interacted with the pathology induced by brain ischemia, which showed increased collateral recruitment with age, further representing better cerebrovascular reserve [42]. It is shown that aging could increase the resilience of the brain to stand against ischemic injury, in detail, researchers identified a profile that included the upregulation of glycogen degradation-related pathways and the downregulation of mitochondrial dysfunction-related pathways, separating the responses against post-ischemic injury of late-life and mid-life [43]. In summary, inflammation, glycogen metabolism, and mitochondrial function may underlie the age-related variances in ischemic outcomes and associated tau pathology [44, 45].
Several strengths of this study ensured the reliability of the findings, including a robust sample size which enabled analysis of associations among ICVD, CSF ATN biomarkers, and cognition. Stringent quality control and statistical adjustment for potential confounders further bolstered confidence in the results. However, some limitations exist. First, the cross-sectional design and lack of pathological ICVD verification preclude causal inferences, longitudinal assessments paired with autopsy or neuroimaging data could elucidate causal pathways. Second, hospital-based recruitment may introduce selection bias. Third, the restriction to Chinese Han ethnicity necessitates validation across diverse populations. Fourthly, given the relatively modest mediated proportion, further studies are required to validate the mediation effects. Finally, cognitive assessments were conducted using the CM-MMSE and MoCA-b, recognized as screening instruments for cognition but may be deemed insufficiently precise. Moving forward, research should delineate whether ICVD impacts cognition through mechanisms beyond neuronal injury alone.
In summary, this study demonstrated associations between ICVD and both elevated CSF t-tau, indicating neuronal injury, as well as poorer cognitive performance. However, hallmark AD pathological changes, reflected by Aβ42 and p-tau in CSF, were not significantly associated with ICVD. Notably, CSF t-tau was found to partially mediate the relationship between ICVD status and cognitive decline. These novel findings provide insight into the mechanisms linking ICVD to dementia and could inform priorities for preventing cognitive impairment by alleviating ischemia-related neuronal damage. Future studies validating our results in diverse populations and exploring subtype-specific effects are warranted.
AUTHOR CONTRIBUTIONS
Shuang-Ling Han (Visualization; Writing – original draft); Ya-Nan Ou (Writing – review & editing); Bao-Lin Han, MD (Data curation); Hai-Hua Guo (Methodology); Hao-Chen Chi (Visualization); Yi-Ming Huang (Data curation); Hui-Fu Wang (Conceptualization; Funding acquisition); Lan Tan (Funding acquisition; Supervision).
Footnotes
ACKNOWLEDGMENTS
The authors thank all colleagues who have made an effort to build the CABLE cohort.
FUNDING
This study was supported by grants from the Science and Technology Innovation 2030 Major Projects (2022ZD0211600), the National Natural Science Foundation of China (81971032), and the Taishan Scholars Program of Shandong Province (tsqn201812157).
CONFLICT OF INTEREST
Lan Tan is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
The authors have no conflict of interest to report.
DATA AVAILABILITY
The datasets utilized in the study are available from the corresponding authors upon reasonable request. The data are not publicly available due to privacy or ethical restrictions.