
Abstract
Background:
Sleep is a potentially modifiable factor associated with dementia, including Alzheimer’s disease, but current evidence supporting this is insufficient.
Objective:
This study aimed to determine whether sleep duration and bedtime patterns are associated with the risk of dementia among middle-aged and older people.
Methods:
This cohort study had an eight-year follow-up period. Participants were 13,601 community-dwelling people aged 40–74 years living in Murakami (Niigata, Japan). Data were collected using a self-administered questionnaire. Predictors were self-reported sleep duration and bedtime, and the outcome was newly-diagnosed dementia determined using the long-term care insurance database. Covariates were demographic characteristics, body mass index, smoking, alcohol consumption, total physical activity, insomnia symptoms, disease history, and either bedtime or sleep duration. Cox proportional hazard models were used to calculate hazard ratios (HRs).
Results:
The mean age of participants at baseline was 59.2 years. Over a mean follow-up period of 8.0 years, 319 cases of dementia were observed. A long self-reported sleep duration relative to the reference sleep duration (7 hours) was associated with increased dementia risk, with the “8 hours” group (adjusted HR = 1.30, 95% CI:0.99–1.73) and “≥9 hours” group (adjusted HR = 1.46, 95% CI:1.00–2.15) having an increased risk (marginally significant) relative to the reference group. Early bedtime was associated with increased dementia risk (adjusted p for trend = 0.0010), with the “21 : 00 or earlier” group (adjusted HR = 1.61, 95% CI:1.14–2.28) having an increased risk relative to the reference (“23 : 00”).
Conclusions:
A long self-reported sleep duration and early bedtime are both associated with increased dementia risk in middle-aged and older people
INTRODUCTION
Dementia is a global public health concern, with the number of affected individuals projected to rise significantly in the near future [1]. In Japan, the prevalence of dementia is significantly increasing due to the aging population; the projected number of people living with dementia was estimated to be 4.1 million in 2019, and the estimated change in all-age dementia prevalence between 2019 and 2050 is reported to be 27% [2]. Costs associated with dementia, both medical and care-related, can be significant and place a tremendous burden on individuals, families, and healthcare systems. Costs for people aged ≥60 years with dementia in Japan are projected to reach approximately $125 billion by 2043 [3].
One of the specific strategic action areas of the World Health Organization focuses on the reduction of dementia risk [4]. In addition to risk factors already identified [1], other factors are being investigated and may emerge as promising targets for reducing the risk of dementia. Sleep plays an important role in the regulation of brain activity, encompassing a wide range of processes from tissue repair to brain metabolite clearance [5]. Therefore, sleep is a potentially modifiable factor that can have an impact on the prevention of dementia. Sleep duration—either short or long—has been reported to be associated with changes in cerebral spinal fluid biomarkers of Alzheimer’s disease (AD), greater amyloid pathology, and cortical atrophy [6, 7]. Dysregulations in sleep-wake behavior, which serve as the most well-established and widely recognized indicators of the circadian system, have been proposed to be associated with neurodegenerative disorders, including AD [8].
Over the past decade, several epidemiologic studies have been conducted to elucidate the association between different sleep patterns and dementia. Recently, observational studies examined the association between sleep duration and the occurrence of dementia, observing an approximately U-shaped dose-response relationship with the lowest point located at 7–8 hours per day [9–12]. In addition to sleep duration, bedtime is also a factor associated with dementia. A number of longitudinal studies found an early bedtime to be associated with an increased risk of dementia [13–15]. However, previous studies rarely assessed whether bedtime is associated with dementia risk independent of sleep duration. Only one cohort study [14] reported that early bedtime is associated with an increased risk of dementia, after adjusting for sleep duration (which was not associated with dementia risk probably due to the limited sample size). Consequently, that study did not clearly show both early bedtime and sleep duration to each be associated with dementia risk. For these reasons, large-scale, high-quality cohort studies on this topic are needed.
Since 2011, we have been conducting a cohort study involving 14,364 participants aged 40–74 years at baseline [16]. One of the target diseases of the cohort study is dementia. The present study aimed to examine associations of sleep duration and bedtime patterns with the risk of dementia among middle-aged and older Japanese people.
METHODS
Participants
The present cohort study had an eight-year follow-up period. The Murakami cohort study is a population-based cohort study of people aged 40–74 years living in Murakami city, Sekikawa village, and Awashimaura village (Niigata Prefecture, Japan) aimed at determining risk factors for multiple outcomes of age- and lifestyle-related chronic diseases [16]. The age range is wide (40–74 years) because the Murakami cohort study covers multiple outcomes. Of the total of 34,802 residents, 14,364 voluntarily participated in the baseline survey conducted in 2011–2013. After excluding 23 participants who were covered by long-term care insurance (LTCI) [17] at baseline (i.e., suspected of having mild cognitive decline or dementia) and 390 people with missing data on body mass index (BMI), height, weight, education, smoking, alcohol drinking, physical activity (PA), sleep duration, and bedtime, 13,974 (97.3%) were enrolled in the present study. Of these, 318 with irregular bedtime patterns (due to shift work, etc.) and 55 outliers for BMI were excluded, resulting in a final study population of 13,601 people (94.7%). Written informed consent was obtained from all participants. The protocol of the Murakami Cohort Study was approved by the Ethics Committee of Niigata University (Nos. 1324 and 2018-0417).
Baseline survey
The baseline survey was conducted using a self-administered questionnaire in 2011–2013. Data on sex, age, body weight, height, marital status, education level, occupation, lifestyle factors (including sleep-related information), use of sleep medication, and disease history (myocardial infarction, stroke, diabetes mellitus, and depression) were collected by a self-report questionnaire. BMI was calculated by dividing weight in kilograms (kg) by height in meters squared (m2).
Questions on self-reported sleep duration and bedtime were based on the Pittsburgh Sleep Quality Index (PSQI) [18]. Sleep duration was asked as “How much nighttime sleep did you usually get during the last year?”, with response options given at one-hour intervals, as follows: ≤5, 6, 7, 8, 9, and≥10 hours/day. Bedtime was asked as “What time did you usually go to bed during the last year”, with response options given at one-hour intervals, as follows: 19 : 00 or earlier, 20 : 00, 21 : 00, 22 : 00, 23 : 00, 00 : 00, 01 : 00, 02 : 00, 03 : 00, 04 : 00, and “irregular bedtime due to night shifts, etc.” The distributions of self-reported sleep duration and bedtime of participants are shown in Fig. 1a and 1b, respectively. Due to the limited number of participants with sleep duration≥10 hours/day (Fig. 1a), self-reported sleep duration was grouped into five categories: (1) ≤5, (2) 6, (3) 7, (4) 8, and (5) ≥9 hours/day. Similarly, due to the limited number of participants with bedtimes of 19 : 00 and after 0 : 00 (Fig. 1b), bedtime was grouped into five categories: (1) 20 : 00 or earlier, (2) 21 : 00, (3) 22 : 00, (4) 23 : 00, and (5) 00 : 00 or later. Participants were defined as having insomnia if their responses to either of the following two questions were “3 days or more”: “Have you ever been unable to fall asleep within 30 minutes of going to bed?” (3 days or more/other), and “Have you ever woken up at night or early in the morning?” (3 days or more/other). Non-refreshing sleep (morning fatigue) was asked as “Did you feel terribly tired when you woke up in the morning during the last year?” (3 days or more/other). We also asked about the use of sleeping pills (at least once a week). Codes for demographic variables, smoking, and drinking are shown in Supplementary Table 1. Alcohol consumption was assessed by obtaining the frequency, usual amount, and type of alcohol consumed, and weekly ethanol consumption was calculated based on the amount of ethanol per day and the frequency per week [19]. Total PA levels were assessed by calculating the metabolic equivalents (METs) score (MET-hours per day [MET-h/d]). The questionnaire elicited the number of hours spent at each level of intensity for sitting, standing, walking, and strenuous work for non-leisure-time PA; frequency and the number of hours spent at each level of intensity for walking slowly, walking quickly, light to moderate exercise, and strenuous exercise for leisure-time PA; sleep; and other activities. The intensity of each PA is shown in Supplementary Table 1. To determine MET-h/d values, activity duration per day was multiplied by the respective MET level. This method of measuring PA has previously been reported [20] and validated [21]. The protocol of the Murakami Cohort Study has been described in detail elsewhere [16].
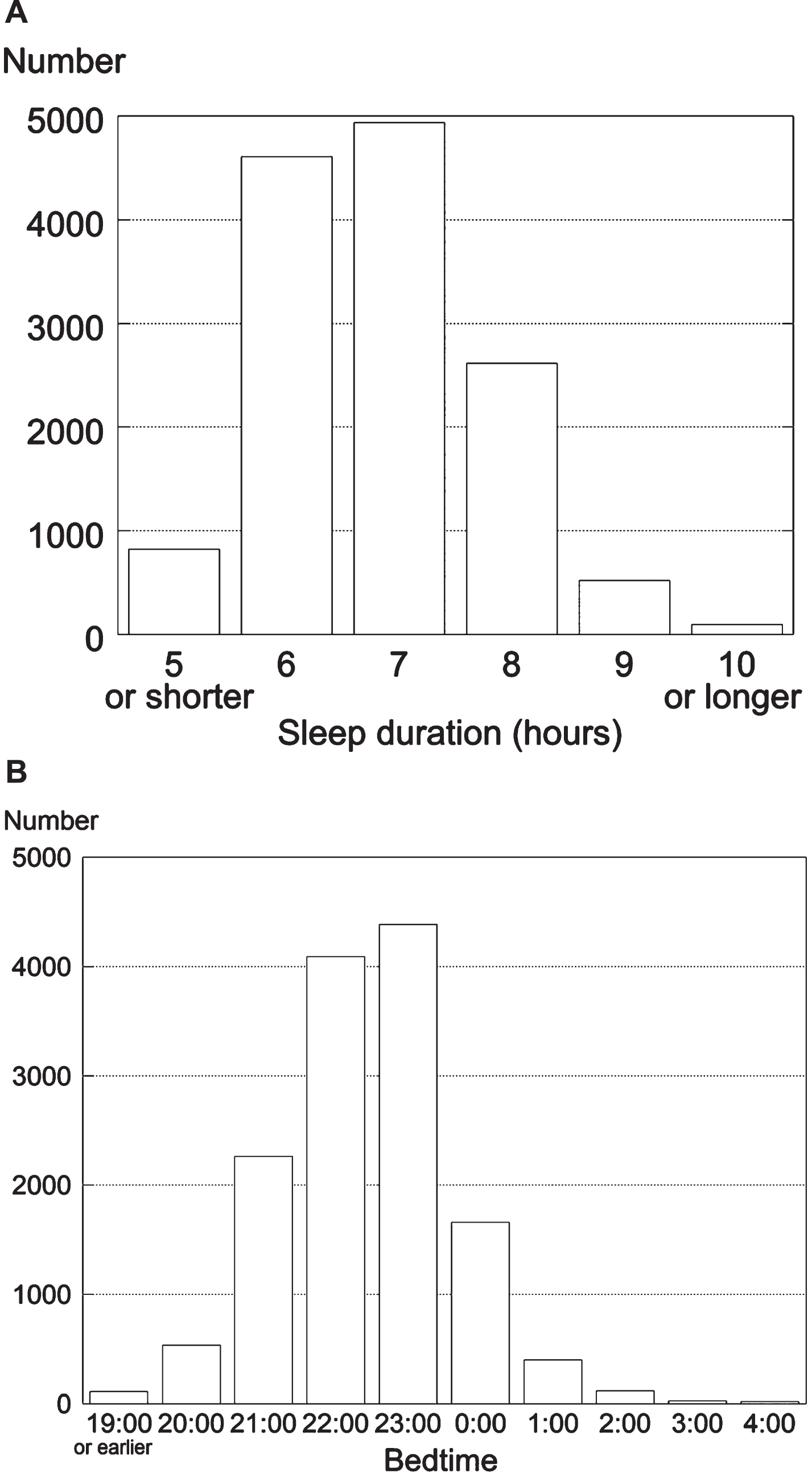
Distributions of self-reported sleep duration (A) and bedtime (B).
Case finding
Cases of incident dementia (up to March 31, 2020) were determined using the LTCI database over eight years of follow-up. As indicated by the LTCI dementia scale [22], disabling dementia is classified into six grades from 0 (no dementia) to V (severe dementia-related behavioral disturbance and cognitive impairment requiring medical treatment) according to the Doctor’s Opinion Paper of a physician in charge. Incident dementia cases correspond to grade II (moderate dementia-related behavioral disturbance and cognitive impairment with slight dependence) or higher [23]. This method of dementia determination has been reported to be highly specific (94–97%) [22]. Details of this case-finding method have previously been described [23]. Person-years of observation were determined using data on moving out and death from residency registration and death registration records in accordance with the Basic Residential Registry Law and the Family Registry Law.
Statistical analysis
Baseline characteristics of participants by sex were reported, with continuous variables presented as median and interquartile range and categorical variables as number and percent. To determine the incidence rate of dementia, the number of dementia cases was divided by person-years of observation. We used the Cox proportional hazards model, which is widely used in the analysis of time-to-event data in cohort studies (Supplementary Figure 1) [24]. Using this model, hazard ratios (HRs) of dementia were calculated according to self-reported sleep duration and bedtime categories. The modes of distribution of self-reported sleep duration and bedtime in our study population were set as the reference groups of each category, i.e., the “7 hours” group and the “23 : 00” group, respectively. This mode-based choice aimed to capture the prevailing sleep pattern in our cohort, providing a representative reference point for our analysis and ensuring the relevance of the findings to the majority of the studied population. We included in the analysis as covariates demographics, lifestyle factors such as total PA [20], smoking, and drinking [19], BMI [25], insomnia and insomnia-related symptoms [26], histories of diseases that are considered important, and potential risk factors for dementia. Covariates in multivariable model 1 included age, sex, BMI, marital status (dummy variable), education level, occupation (dummy variable), smoking, alcohol drinking (coded as 1, 0 or ≥450 g ethanol/week, and 0, other categories; dementia risk is reportedly higher in the 0 and ≥450 groups than in other groups [19]), total PA level, insomnia (dummy variable), morning fatigue (dummy variable), use of sleeping pills (dummy variable), and history of myocardial infarction, stroke, diabetes, and depression (dummy variables). The variable “insomnia” was identified using the criteria for diagnosing insomnia disorder, which included the inability to fall asleep or experiencing sleep difficulty with nocturnal awakenings for at least three nights per week and a period of at least three months, in accordance with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [27]. Multivariable model 2 was additionally adjusted for the bedtime group in the analysis of sleep duration/dementia, and the sleep duration group in the analysis of bedtime/dementia. Given the wide age range of participants in this study (40–74 years), the possibility of participants (e.g., middle-aged adults) developing early-onset dementia during the follow-up period was taken into consideration, and the association between sleep duration/bedtime and dementia was also examined by limiting the analysis to those aged ≥60 years (sensitivity analysis) to focus on late-onset dementia, which accounts for the majority of cases.
In subgroup analyses, HRs of dementia were calculated stratified by sex and age groups. Subsequently, HRs of sleep duration were calculated stratified by bedtime and vice versa to determine a potential interaction between the two variables. Finally, HRs at 2, 4, 6, and 8 years of follow-up were calculated, and the association of sleep duration and bedtime with dementia risk was analyzed in the cohort that excluded cases of dementia that occurred within the first four years of follow-up (sensitivity analysis) to assess the possibility of reverse causation (i.e., having dementia may cause individuals to change sleep patterns). Multicollinearity was checked for predictor variables. The correlation between sleep duration and bedtime was moderate (Spearman’s correlation coefficient, –0.500, p < 0.0001), and agreement between them was low (weighted Kappa, –0.22, 95% CI: –0.23,–0.21) (Supplementary Table 2). The cumulative incidence of dementia stratified by predictor variables was determined by the Kaplan–Meier method. SAS version 9.4 software (SAS Institute Inc., Cary, NC, USA) was used for statistical analysis. p < 0.05 was considered statistically significant.
RESULTS
The mean age of participants at baseline was 59.2 years (standard deviation [SD] 9.3), and the mean follow-up period was 8.0 years (SD 1.3). During the follow-up period, a total of 319 people developed dementia; five in their 40 s, 22 in their 50 s, 126 in their 60 s, and 166 in their 70 s. Participant characteristics at baseline according to self-reported sleep duration and bedtime groups are presented in Table 1. Sleep duration was significantly associated with age, total PA levels, sex, marital status, education levels, occupation, alcohol drinking, difficulty in falling asleep, morning fatigue, and all of the four disease histories. Bedtime was significantly associated with age, total PA levels, sex, marital status, education levels, occupation, smoking, alcohol drinking, nocturnal awakening, morning fatigue, use of sleeping pills, and disease histories of myocardial infarction, stroke, and diabetes.
Baseline participant characteristics by groups of self-reported sleep duration and bedtime
Data are shown as median with interquartile range in parentheses or number with percent in parentheses. MET, metabolic equivalent; PA, physical activity; MI, myocardial infarction. *Experiencing difficulty falling asleep within 30 minutes of bedtime three or more times a week. †Experiencing nocturnal awakening three or more times a week. ‡Experiencing fatigue upon waking up three or more times a week. **Use of sleeping pills at least once a week.
Incidence rates and HRs for dementia according to self-reported sleep duration are shown in Table 2. Overall, a long self-reported sleep duration relative to the reference sleep duration (7 hours) was associated with increased dementia risk, with the “8 hours” group (HR = 1.30, 95% confidence interval [CI]: 0.99–1.73 [p = 0.0641]) and “≥9 hours” group (HR = 1.46, 95% CI: 1.00–2.15 [p = 0.0519]) having a marginally higher risk than the reference group. A long self-reported sleep duration relative to the reference sleep duration (7 hours) was associated with increased dementia risk in males and females, with the “≥9 hours” group (HR = 1.58, 95% CI: 0.95–2.62 [p = 0.0783]) in males having a marginally higher risk than the reference group. Short sleep duration groups of “≤5 hours” and “6 hours” did not have a significantly increased risk of dementia. The cumulative incidence of dementia as determined by the Kaplan–Meier method stratified by sleep duration groups is shown in Supplementary Figure 2. The results of the sensitivity analysis, in which participants were limited to those aged ≥60 years, are shown in Supplementary Table 3.
Incidence rates and hazard ratios (HRs) for dementia according to self-reported sleep duration
*Adjusted for age, sex, body mass index, marital status, education, occupation, smoking, alcohol drinking, total physical activity levels, insomnia, morning fatigue, use of sleeping pills, and disease history (myocardial infarction, stroke, diabetes mellitus, depression). †Further adjusted for bedtime in addition to covariates in multivariable-adjusted Model 1.
Incidence rates and HRs for dementia according to self-reported bedtime are shown in Table 3. Overall, early bedtime was associated with higher dementia risk, with the “20 : 00 or earlier” group (multivariable-adjusted Model 2 HR = 1.56, 95% CI: 1.00–2.46 [p = 0.0523]) and “21 : 00” group (multivariable-adjusted Model 2 HR = 1.61, 95% CI: 1.14–2.28 [p = 0.0075]) having a higher risk than the reference (“23 : 00”) group. In the sex-stratified analysis, bedtime was associated with the risk of dementia in males (multivariable-adjusted Model 2 p for trend = 0.0400) and females (multivariable-adjusted Model 2 p for trend = 0.0045), with the “00 : 00 or later” group (HR = 0.25, 95% CI: 0.06–1.06 [p = 0.0598]) in males having a lower risk, and the “20 : 00 or earlier” group (HR = 2.13, 95% CI: 1.05–4.31 [p = 0.0357]) and “21 : 00” group (HR = 1.76, 95% CI: 1.07–2.88 [p = 0.0255]) in females having a higher risk than the reference group. The cumulative incidence of dementia as determined by the Kaplan–Meier method stratified by bedtime group is shown in Supplementary Figure 3. The results of the sensitivity analysis are shown in Supplementary Table 4.
Incidence rates and hazard ratios (HRs) for dementia according to self-reported bedtime
*Adjusted for age, sex, body mass index, marital status, education, occupation, smoking, alcohol drinking, total physical activity levels, insomnia, morning fatigue, use of sleeping pills, and disease history (myocardial infarction, stroke, diabetes mellitus, depression). †Further adjusted for sleep duration in addition to covariates in multivariable-adjusted Model 1.
Incidence rates and HRs for dementia according to self-reported sleep duration and bedtime were also analyzed by age group (<65 versus ≥65 years; Table 4). Long sleep hours were associated with a higher dementia risk (multivariable-adjusted Model 2 p for trend = 0.0180), with the “≥9 hours” group having a higher risk (HR = 3.13, 95% CI: 1.48–6.64 [p = 0.0029]) than the reference (7 hours) for individuals aged <65 years, while the association between long sleep duration and higher dementia risk was not significant (multivariable-adjusted Model 2 p for trend = 0.0987) for those aged≥65 years. Bedtime was not associated with dementia risk for individuals aged < 65 years (multivariable-adjusted Model 2 p for trend = 0.1716), while early bedtime was associated with a higher dementia risk (multivariable-adjusted Model 2 p for trend = 0.0063) for those aged≥65 years, with the “20 : 00 or earlier” (HR = 1.58, 95% CI: 0.96–2.63 [p = 0.0748]) and “21 : 00” (HR = 1.60, 95% CI: 1.07–2.39 [p = 0.0222]) groups having a higher dementia risk than the reference.
Incidence rates and hazard ratios (HRs) for dementia according to self-reported sleep duration and bedtime stratified by age group
*Adjusted for age, sex, body mass index, marital status, education, occupation, smoking, alcohol drinking, total physical activity levels, insomnia, morning fatigue, use of sleeping pills, and disease history (myocardial infarction, stroke, diabetes mellitus, depression). †Further adjusted for bedtime or sleep duration in addition to covariates in multivariable-adjusted Model 1.
Incidence rates and HRs for dementia according to self-reported sleep duration and bedtime stratified by two groups of bedtime and sleep duration, respectively, are shown in Supplementary Table 5. There was no interaction between bedtime and sleep duration on dementia risk (multivariable-adjusted Model 2 p for interaction = 0.9199).
Unadjusted HRs for dementia at 2, 4, 6, and 8 years of follow-up are shown in Supplementary Table 6. HRs of long self-reported sleep duration and early bedtime groups at 2 years of follow-up were apparently higher than in the other follow-up periods. Incidence rates and HRs for dementia according to sleep duration and bedtime in males and females combined, after excluding dementia cases occurring within four years of follow-up, are shown in Supplementary Table 7. Long sleep duration was not associated with a higher risk of dementia (multivariable-adjusted Model 2 p for trend = 0.0605). Early bedtime was associated with a higher risk of dementia (multivariable-adjusted Model 2 p for trend = 0.0138), with the “21 : 00” group having a higher dementia risk (HR = 1.58, 95% CI: 1.06–2.37) than the reference.
DISCUSSION
The present study yielded the following findings: 1) self-reported sleep duration and bedtime were each associated with increased dementia risk, 2) long self-reported sleep duration (≥9 hours) was associated with increased dementia risk, but short sleep duration was not, 3) early bedtime (21 : 00 or earlier) was associated with increased dementia risk, 4) the association between long self-reported sleep duration (≥9 hours) and high dementia risk was stronger in middle-aged people than in older people, and 5) the association between early bedtime and high dementia risk was observed in older people but not in middle-aged people.
The present study showed that a long self-reported sleep duration relative to the reference sleep duration of 7 hours was associated with increased dementia risk. Several longitudinal studies have reported consistent results [9, 29]. In contrast to our findings, however, some studies [30, 31] have reported no significant association between self-reported sleep duration and the risk of cognitive decline. This discrepancy may be attributed to the use of different outcomes or follow-up periods. Studies using a decline in cognitive function as an outcome typically had a short follow-up period, and in fact, the follow-up period of the two studies with null associations [30, 31] was four years or less. Mechanisms underlying the association between long sleep duration and dementia are not well understood, but some hypotheses may help explain it. Long sleep duration is suggested to be associated with global brain atrophy [28] and may also be associated with sleep disorder or sleep fragmentation [15], which may decrease the deep sleep phase [32] for efficient clearance of brain toxins [33] and is hence associated with dementia [34]. Long sleep duration is also associated with the risk of non-communicable chronic diseases, including diabetes, stroke, heart disease, obesity, and depression [35], which are established risk factors for dementia [1]. Using objective sleep measures, Basta et al. [36] showed that long sleep duration is associated with cognitive decline. Although both objective and subjective studies suggest that long sleep duration is a predictor of dementia/cognitive decline, since the causality of the association between long sleep duration and dementia risk has not been fully elucidated, further studies are warranted.
In the present study, the estimated overall relative risk (RR) of ≥9 hours of sleep for dementia was 1.46, which is not necessarily high. According to a meta-analysis conducted by Wu et al. [9], the risk of the longest category (versus middle category) for dementia was low (RR = 1.22, 95% CI: 0.97–1.54), whereas the risk for AD was high (RR = 2.19, 95% CI: 1.08–4.46). In light of this, the potential effect of long sleep duration on AD may be higher than the estimated RR of 1.46 in the present study.
The present study showed that a long self-reported sleep duration of≥9 hours was strongly associated with an increased risk of dementia (HR = 3.13) in the middle-aged subgroup (<65 years). While reasons for this finding are unclear, patients with early-onset AD were reported to have more severe sleep alterations than those with late-onset AD [36], due probably to a more compromised arousal system, which may be associated with elevated levels of hormones such as interleukin-6 and cortisol [37]. Long sleep duration is suggested to be a more sensitive predictor of early-onset dementia. On the other hand, a sleep duration of≥9 hours was not significantly associated with an increased risk of dementia in the older subgroup (≥65 years). This may be explained by misclassification bias due to inaccuracies in their self-reported sleep duration among older people [38].
Although meta-analyses have found that a short sleep duration of <7 hours is associated with an increased risk of dementia [9, 10], we did not observe such an association, consistent with the findings of recent studies that also used self-reported sleep duration as an outcome [13, 15]. Meanwhile, some studies using objective sleep duration reported an association between short sleep duration and high dementia risk [39, 40]. The lack of association between short self-reported sleep duration and high dementia risk may be explained by the fact that, unlike studies using objective measures of sleep duration [41], the studies using self-reported sleep duration simply assessed sleep quantity and did not assess the impact of sleep quality (e.g., insomnia).
The present study found a robust association between early bedtime and an increased risk of dementia, independent of sleep duration, with high risk being observed for a bedtime of 21 : 00 or earlier (Model 1 HRs = 1.82 and 1.83; Model 2 HRs = 1.61 and 1.56) (Table 3). Recent cohort studies have reported similar results [13–15]: Liu et al. [13] reported a high risk (adjusted RR = 2.17 [95% CI: 1.22–3.87], versus 22 : 00 or later) of bedtime 21 : 00 or earlier, and Li et al. [14] reported an RR of 2.00 (95% CI: 0.94–4.29, versus 21 : 00–23 : 00) of bedtime 21 : 00 or earlier. The HRs of 1.61 and 1.56 for Model 2 (sleep duration included as a covariate) in the preset study appear to be low relative to those reported by the two previous studies (2.17 and 2.00, respectively) [13, 14]; however, the HRs for Model 1 (sleep duration not included as a covariate) were 1.82 and 1.83, which are comparable to those of the two studies. While the mechanism underlying this finding is unclear, one probable explanation is that early bedtime is driven by circadian dysfunction [42] which is associated with AD [43]. Circadian dysfunction contributes to the risk of dementia; thus, an early bedtime may be a modifiable factor for AD [43, 44]. Early bedtime may also be a consequence of AD because once amyloid-β plaques have formed, sleep-wake functions and circadian rhythms are disrupted [44], suggesting that the association is robust and bidirectional.
We also detected an association between early bedtime and an increased risk of dementia in older people (≥65 years), but not in middle-aged people (<65 years). This finding is in line with current knowledge that dysregulation in the circadian system, which has been suggested to be linked with neurodegenerative disorders, is typically observed in older individuals [8, 42]. Aging contributes to the degeneration of the suprachiasmatic nucleus and a reduction in melatonin synthesis, disrupting circadian regulation and establishing a bidirectional relationship with neurodegenerative diseases, including AD, where changes in circadian amplitude may precede AD symptoms [42]. Also, the lack of such an association in middle-aged people may partly be explained by the fact that early bedtime is not common among middle-aged people due to various life demands (e.g., work, social life, family responsibilities).
The strength of the present study is the large number of participants and a high follow-up rate that enabled us to determine associations of self-reported sleep duration and bedtime with dementia risk. In addition, the target sample included a relatively young population, which allowed us to assess the effects of sleep patterns in midlife and late life separately.
There are some limitations in the present study. First and most importantly, we used self-reported sleep duration as a predictor, which may have led to misclassification. According to Van Den Berg et al. [38], self-reported duration deviated from actigraphically measured sleep duration by more than 1 hour in 34% of older individuals. The second and another important limitation is the failure to take into account multimorbidity, which we did not assess in our study cohort. Multimorbidity has been reported to be associated with sleep duration and sleep quality [45], as well as the progression of AD [46]. Thus, multimorbidity is a potential confounder and might have affected the HRs obtained in the present study. Third, data on sociodemographic characteristics, lifestyle factors, and disease history were obtained from a self-administered questionnaire, which may have introduced misclassification. Fourth, Spearman’s correlation coefficient between the predictors of ‘sleep duration (≤5, 6, 7, 8, ≥9 hours)’ and ‘bedtime (-20 : 00, 21 : 00, 22 : 00, 23 : 00, 00 : 00-)’ was –0.50, which may have affected HRs. A previous simulation study [47] showed that, when two predictor variables are correlated with each other, their parameter estimates are smoothly affected by the degree of correlation until the degree of correlation reaches±0.9. This suggests that the HRs of sleep duration and bedtime in the present study may have been modified by the relatively high correlation (Spearman’s r=–0.50). Fifth, incident dementia cases were identified using the LTCI database. As some of these cases might not have been diagnosed by neurologists, misclassification of dementia cases could have attenuated the association between sleep patterns and the risk of dementia. Although the specificity of the method used to determine dementia is reportedly high (94–97%), sensitivity is limited (73%) [22]. This may have resulted in a selection bias for dementia cases. Sixth, dementia subtypes were not determined. Given that AD accounts for roughly two-thirds of dementia cases [48], our findings may be primarily relevant to AD cases. Seventh, changes in sleep patterns and confounding variables during the follow-up period could not be analyzed. Eighth, although associations between self-reported sleep duration/bedtime and dementia risk were detected, these associations may be explained by reverse causation. For example, early-stage AD may have affected sleep duration and/or bedtime. Longer follow-up studies are needed to confirm the causality of these associations. Finally, our results were not adjusted for all potential confounders and their changes over the follow-up period, including other sleep parameters (e.g., time in bed, sleep quality), genetic factors (e.g., APOE polymorphisms), family history, and dietary factors. Because sleep duration and bedtime share many confounders, caution should be exercised in interpreting their independence with respect to dementia risk.
Despite these limitations, the present study has some clinical implications. In general practice, incorporating self-reported sleep duration and bedtime assessment in addition to known risk factors may improve risk assessment for dementia. Moreover, monitoring self-reported sleep patterns may be a useful indicator of early dementia. Furthermore, our findings may provide a rationale for interventions to determine whether optimizing sleep duration and bedtime can reduce dementia risk. Taken together, the present study underscores the pivotal role of health professionals in not only detecting the early signs of dementia but also developing preventive care strategies for dementia.
Conclusions
The present study found that self-reported long sleep duration and early bedtime are both associated with an increased risk of dementia in middle-aged and older Japanese people. This suggests that mechanisms by which these two sleep characteristics may be associated with dementia differ. Although the causality of the associations is unclear, sleep-related lifestyle interventions might help reduce the risk of dementia. Further investigation is warranted to elucidate the role of different sleep patterns in the etiology of dementia.
AUTHOR CONTRIBUTIONS
Irina Bulycheva (Conceptualization; Formal analysis; Writing – original draft); Yumi Watanabe (Writing – review & editing); Kaori Kitamura (Investigation; Writing – review & editing); Keiko Kabasawa (Writing – review & editing); Toshiko Saito (Investigation); Akemi Takahashi (Investigation); Ryosaku Kobayashi (Investigation); Rieko Oshiki (Investigation); Ribeka Takachi (Investigation; Writing – review & editing); Shoichiro Tsugane (Funding acquisition; Writing – review & editing); Osamu Yamazaki (Resources); Kei Watanabe (Writing – review & editing); Kazutoshi Nakamura (Conceptualization; Data curation; Formal analysis; Funding; acquisition; Investigation; Project administration; Supervision; Writing – original draft).
Footnotes
ACKNOWLEDGMENTS
The authors thank the Murakami Public Health Center, Murakami city, Sekikawa village, and Awashimaura village for their valuable support in data collection, and Professor Kohei Akazawa (Department of Medical Informatics, Niigata University Medical and Dental Hospital) for his advice on statistical analysis.
FUNDING
This work was supported by JSPS KAKENHI Grants (Grant Nos. JP23249035, JP15H04782) and the National Cancer Center Research and Development Fund [23-A31(toku) (since 2010)]. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are not publicly available due to privacy restrictions.