
Abstract
Background:
Frailty is a vulnerability state increasing the risk of many adverse health outcomes, but little is known about the effects of frailty on neuropsychiatric health.
Objective:
To explore the associations between frailty and the risk of neuropsychiatric symptoms (NPSs) in Alzheimer’s disease (AD), especially in its different clinical stages.
Methods:
We included 2,155 individuals assessed using modified frailty index-11 (mFI-11), Neuropsychiatric Inventory (NPI) and Neuropsychiatric Inventory Questionnaire (NPI-Q) in the Alzheimer’s Disease Neuroimaging Initiative (ADNI). The relationships between frailty and NPSs were explored with logistic regression models and Cox proportional hazard regression models. Causal mediation analyses were conducted to explore the mediation factors between frailty and NPSs.
Results:
Among mild cognitive impairment (MCI) participants, frailty was cross-sectionally associated with an increased risk of apathy, and longitudinally associated with increased risk of depression and apathy. Among AD participants, frailty was cross-sectionally associated with increased risk of depression and anxiety, and longitudinally associated with an increased risk of apathy. Among participants with cognitive progression, frailty was associated with increased risk of depression and apathy. In MCI participants, the influence of frailty on NPSs was partially mediated by hippocampus volume, whole brain volume, and monocytes, with mediating proportions ranging from 8.40% to 9.29%.
Conclusions:
Frailty was associated with NPSs such as depression, anxiety, and apathy among MCI, AD, and cognitive progression participants. Atrophy of the hippocampus and whole brain, as well as peripheral immunity may be involved in the potential mechanisms underlying the above associations.
Keywords
INTRODUCTION
Dementia is an acquired loss of cognition in multiple cognitive domains, accompanied by various behavioral and psychological symptoms, collectively known as neuropsychiatric symptoms (NPSs) [1]. The most common type of dementia is Alzheimer’s disease (AD). The AD continuum, ranging from subjective cognitive decline (SCD) or preclinical AD to mild cognitive impairment (MCI) and fully developed AD, has been described [2]. Most individuals with AD present with NPSs during the disease continuum [3] and some NPSs even appear earlier than cognitive impairment [4]. Accumulating evidence suggests that the onset time of different NPSs is associated with AD progression. For example, most NPSs including affective symptoms, sleep disturbances, and abnormal motor behavior occur in the MCI stage, while disinhibition, hallucinations, and euphoria occur in the moderate AD stage [5–7]. Previous prospective cohort studies showed that participants with NPSs were more likely to develop severe dementia and have a reduced life expectancy in non-demented population [8–10]. NPSs also impose great burden on their patients and caregivers [11–13]. Currently, there are very few medications that are useful for NPSs [14]. Thus, early identification and intervention of NPSs at different stages of AD are critical to reducing the burden imposed by NPSs.
Frailty is a vulnerability state due to poor resolution of homeostasis following a stress, which increases the risk of many adverse outcomes [15]. The unidimensional physical frailty phenotype model based on biologically interconnected symptoms and signs [16], and the multidimensional frailty index (FI) model based on age-related deficit accumulation [17] are two common instruments to assess frailty. In addition, emerging concepts of frailty phenotypes, including depressive frailty phenotype, social frailty, and biopsychosocial frailty, have been widely defined and validated [18–20]. It is crucial to select an appropriate model to assess frailty. Previous population-based cohort studies found deficit accumulation represented an important risk factor for cognitive dysfunction and a potential prognostic marker [21, 22]. Participants with a higher FI were more likely to have more AD pathology and for it to be expressed as dementia [23]. Emerging cross-sectional studies showed that physical frailty was associated with the occurrence of depression [24]. Inconsistent with these two studies, other cross-sectional studies found no significant associations [25, 26]. And longitudinal evidence in the deficit accumulation model is limited on this association. The frequencies of various NPSs were different across different AD stages, and the influence of frailty on NPSs at different stages of AD warrants investigation. The occurrence and development of NPSs in AD are influenced by brain structures. And there is evidence that inflammation is involved in the pathophysiology of frailty [27–29]. However, whether brain structures and inflammatory factors mediate the associations between frailty and the occurrence of NPSs remains largely unknown.
Therefore, we aimed to identify the cross-sectional and longitudinal associations of frailty with the occurrence of NPSs at different stages of AD within a prospective Alzheimer’s Disease Neuroimaging Initiative (ADNI) cohort. We also explored whether the brain structures and inflammatory factors mediated the associations between frailty and the occurrence of NPSs.
METHODS
Design and sample
The ADNI database is an ongoing longitudinal study launched in 2003. The primary goal of ADNI has been to test whether serial neuroimaging and other biological, clinical, and neuropsychological markers can be combined to measure clinical progression along the AD spectrum [30]. The details of study design have been published previously, which can be found at http://www.adni-info.org. Data for the current study were collected from the ADNI-1, ADNI-GO, ADNI-2, and ADNI-3 phases [31, 32]. We included 2,155 subjects with available basic clinical characteristics, medical history, imaging data, and cognitive assessment data from the ADNI database. As mentioned earlier [33], clinical classification was performed by the ADNI centers, dividing participants into cognitively normal (CN, Mini-Mental State Examination [MMSE] > 24, CDR = 0, non-depressed), mild cognitive impairment (MCI; MMSE > 24, CDR = 0.5, objective memory-loss on the education adjusted Wechsler Memory) and AD (ADD; 19 < MMSE < 24, CDR = 0.5–1.0, NINCDS/ADRDA criteria for probable AD are fulfilled) groups. Individuals with subjective memory complaints at baseline were included within the CN group. Cognitive progression was defined as conversion from CN to MCI/AD, or conversion from MCI to AD during the follow-up.
Modified frailty index
The main exposure of interest in this cohort study was frailty, which was measured by the modified frailty index (mFI) based on the deficit accumulation model. The FI has been validated to be a more precise method to evaluate the risk of adverse outcomes [34]. A simple 11-point FI was applicable in clinical practice [35] and adapted to the available data in the ADNI database. This 11-point scoring system includes 11 possible comorbidities and deficits: 1) non-independent functional status; 2) diabetes mellitus; 3) congestive cardiac failure; 4) hypertension; 5) myocardial infarction; 6) heart diseases; 7) peripheral vascular disease; 8) transient ischemic attack or cerebrovascular accident without accident; 9) acutely impaired sensorium; 10) lung diseases; and 11) cerebrovascular accident with deficits (see Supplementary Table 1 for details). As a comorbidity-dominant scoring system, it requires binary non-subjective responses. The score can also be calculated without phenotypic measures of the patients, such as exhaustion, slowness, and reduced physical activity. Each component is assigned one point with a total point range of 0–11. Based on modification and validation of the CSHA-FI, we categorized frailty status as frailty (score≥3 points), pre-frailty (1–2 points), and robust (0 point) [17, 37].
Neuropsychiatric assessment
In this study, the NPSs were assessed by Neuropsychiatric Inventory (NPI) and Neuropsychiatric Inventory Questionnaire (NPI-Q). The NPI-Q was administered by a study coordinator as a structured interview to an informant. The NPI-Q assessed the presence or absence of 12 emotional behaviors (i.e., depression, anxiety, apathy, agitation, delusion, hallucination, euphoria, disinhibition, irritability, aberrant motor behavior, sleep problems, and eating/appetite). Neuropsychiatric manifestations within a domain are collectively rated by the caregiver in terms of both frequency (1 to 4) and severity (1 to 3), yielding a composite symptom domain score (frequency×severity) [38]. A participant is considered as having a particular symptom when the NPI item score≥1. The presence of NPSs is defined as the presence of at least one of the symptoms on the NPI in the past month. We classified NPS into four sub-syndromes as previously suggested [39, 40]: 1) affective symptoms (depression, anxiety, and apathy); 2) hyperactivity (agitation, disinhibition, and irritability); 3) psychosis (delusions, hallucinations, sleep problems, and aberrant motor behaviors); and 4) others (euphoria and appetite/eating change).
Statistical analysis
Our statistical analysis plan was determined during the pre-analysis research process (Fig. 1). Comparisons of baseline characteristics (including the frequency of each NPSs) were conducted using the Kruskal-Wallis test for continuous variables and Chi-square test for categorical variables.
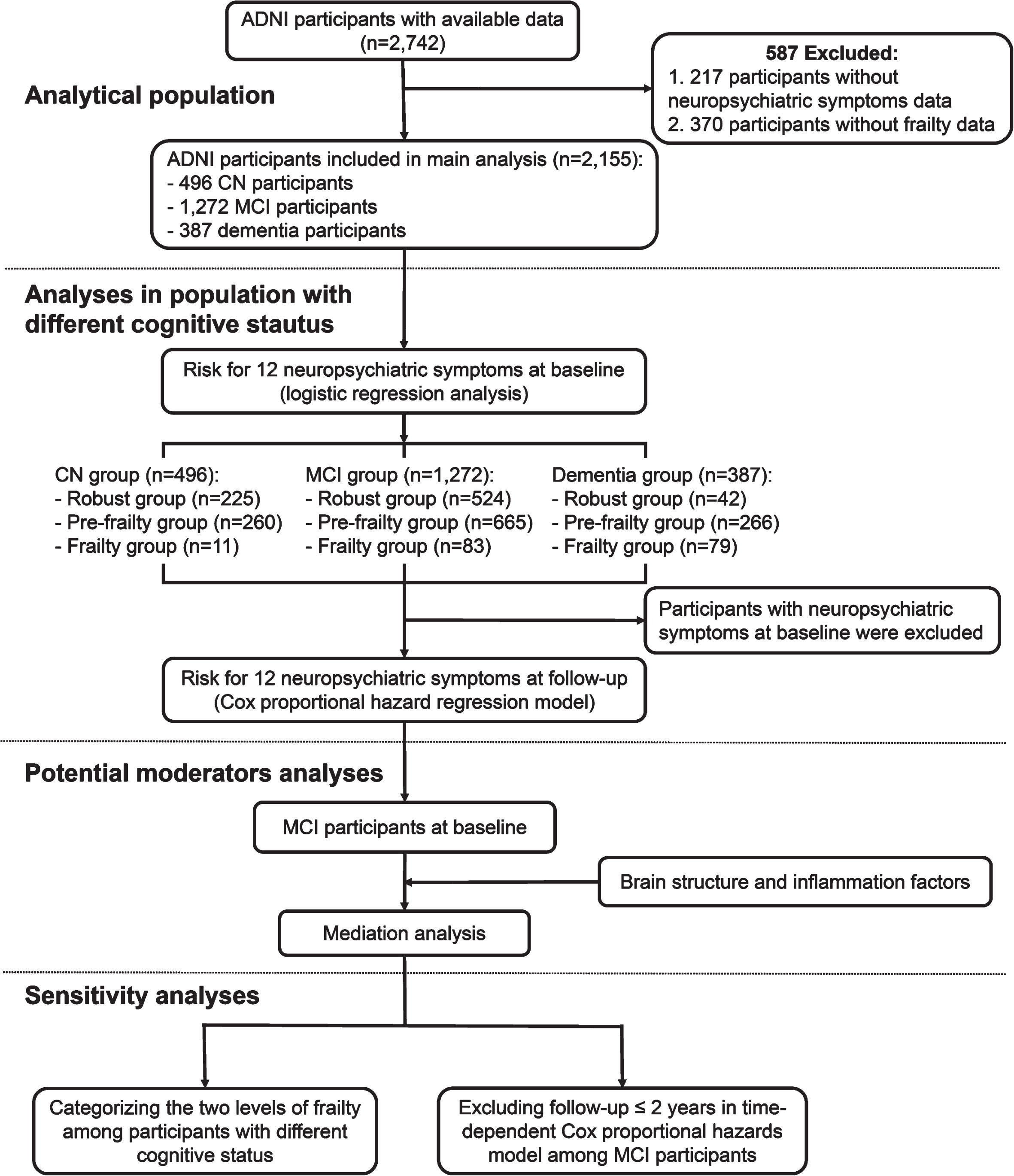
Flowchart of study design. The research overview summarizes the selection and analysis process of the analysis population. ADNI, Alzheimer’s Disease Neuroimaging Initiative; CN, cognitively normal; MCI, mild cognitive impairment.
The multinomial logistic regression model was used to separately examine the association of frailty with incident NPSs among CN, MCI, and AD participants. Next, we used the time-dependent Cox proportional hazards model that allowed simultaneous estimation of the probability of different NPSs among CN, MCI, AD, and cognition progressive groups. Separate odds ratios (OR), hazard ratio (HR), and 95% confidence interval (CI) were calculated for the pre-frailty and frailty groups, comparing each with the reference group (robust). All models were adjusted for age (continuous), gender (female = 0, male = 1), education (continuous) and APOE ɛ4 status (“44” or “43” or “42” = 1, other genotypes = 0).
Next, to examine whether the associations between frailty and the occurrence of NPSs were mediated by brain structures and inflammatory factors, linear regression model and logistic regression model were fitted based on the methods proposed by Baron and Kenny [41]. The first equation regressed the mediator (brain structures and inflammatory factors on the independent variable (frailty). The second equation regressed the dependent variable (NPSs) on the independent variable. The third equation regressed the dependent variable on both the independent variable and the mediator variable. Mediation effects were established if the following criteria were simultaneously reached: 1) frailty was significantly related to brain structures and inflammatory markers; 2) frailty was significantly related to the occurrence of NPSs; 3) brain structures and inflammatory markers were significantly related to the occurrence of NPSs; and 4) the associations between frailty and the occurrence of NPSs were attenuated when brain structures and inflammatory markers (the mediators) were added in the regression model. Furthermore, the attenuation or indirect effect was estimated, with the significance determined using 10,000 bootstrapped iterations, where each path of the model was controlled for age, gender, education, and APOE ɛ4 status.
Moreover, to investigate whether the associations between frailty and the occurrence of NPSs were influenced by demographic characteristics, we performed subgroup analyses stratified by age, sex, years of education, and body mass index (BMI) using multinomial logistic regression model.
Finally, to test the robustness of the results, we conducted sensitivity analyses by categorizing participants into two frailty statuses: robustness (mFI = 0) and frailty (mFI≥1), and excluding those with a follow-up≤2 years in time-dependent Cox proportional hazards model among MCI participants.
All statistical analyses were performed using R version 4.2.1 (The R Project). A two-tailed P-value <0.05 was considered statistically significant.
RESULTS
Characteristics of participants
The basic characteristics of the participants were listed in Table 1. As for ADNI, a total of 2,155 individuals (791 robustness, 1,191 pre-frailty, and 173 frailty) were included. Of the total participants, 387 were diagnosed with AD; 1,272 were diagnosed with MCI; and 496 were cognitive normals. Overall, the mean age±SD of all the 2,155 participants were 73.34±7.22 years, and the female proportion was 46.6%. As expected, compared with those in the robust group, participants in the pre-frailty and frailty groups had fewer years of education, higher BMI and more NPSs, and the two groups had older mean ages and smaller female proportions than the robust group (all p < 0.001). Notably, the frequencies of all NPSs except euphoria in participants with frailty and pre-frailty were significantly higher than those in the robust group (all p < 0.05).
Characteristics of study participants in the ADNI cohorts
Data are presented as n (%) and mean (SD). The p-values are derived using Student’s t test, Kruskal-Wallis test, or χ2 test among no frailty and frailty groups. ADNI, Alzheimer’s Disease Neuroimaging Initiative; APOE4, apolipoprotein E ɛ4; BMI, body mass index; CN, cognitively normal; DX, diagnosis; MCI, mild cognitive impairment; SD, standard deviation. *Statistically significant.
The effects of frailty on the risk of NPSs at different stages of AD at baseline.
In the multinomial logistic regression model, pre-frailty and frailty showed no significant associations with any NPS in CN participants (Fig. 2A). However, pre-frailty (OR = 1.52, 95% CI = 1.20–1.92) and frailty (OR = 1.95, 95% CI = 1.21–3.20) were associated with a higher risk of developing NPSs in MCI participants. To be specific, among the MCI participants, frailty was significantly associated with a higher risk of anxiety (OR = 1.50, 95% CI = 1.05–2.15) and apathy (OR = 3.35, 95% CI = 1.74–6.30), but not depression; and frailty increased the risks of irritability (OR = 2.42, 95% CI = 1.42–4.07) and aberrant appetite (OR = 2.94, 95% CI = 1.43–5.81) (Fig. 2B). Among demented participants, pre-frailty (OR = 3.34, 95% CI = 1.64–6.73) and frailty (OR = 4.16, 95% CI = 1.68–10.79) had associations with a higher risk of developing NPSs. To be specific, in those with dementia frailty was significantly associated with a higher risk of depression (OR = 2.33, 95% CI = 1.03–5.50) and anxiety (OR = 2.85, 95% CI = 1.10–8.44) rather than apathy; frailty increased the risk of partial psychosis including sleep problems (OR = 2.82, 95% CI = 1.02–9.12) and aberrant motor behavior (OR = 14.45, 95% CI = 2.72–267.91); and frailty was significantly associated with a higher risk of agitation (OR = 2.52, 95% CI = 1.04–6.62) and aberrant appetite (OR = 3.62, 95% CI = 1.24–13.26) (Fig. 2C).

The effects of frailty on the risk of NPSs at different stages of AD at baseline. In the multinomial logistic regression model, pre-frailty and frailty have no significant effect on all NPSs in CN participants (A). Pre-frailty and frailty have a higher risk of developing NPSs in MCI participants. Frailty was significantly associated with a higher risk of affective symptoms including anxiety and apathy, but not depression. Frailty increases the risk of irritability and aberrant appetite (B). In dementia participants, pre-frailty and frailty have a higher risk of developing NPSs. Frailty was significantly associated with a higher risk of affective symptoms including depression and anxiety. Frailty increases the risk of partial psychosis including sleep problems and aberrant motor behavior. Moreover, frailty was significantly associated with a higher risk of agitation and aberrant appetite (C). The OR or 95% CI between frailty and some NPSs could not be calculated due to the insufficient of participants. All model was adjusted for age, gender, education, and APOE ɛ4 status. *p < 0.05, **p < 0.01, and ***p < 0.001, respectively. AD, Alzheimer’s Disease; OR, odds ratio; CI, confidence interval; NPSs, neuropsychiatric symptoms; CN, cognitively normal; MCI, mild cognitive impairment.
The effects of frailty on the risk of NPSs at different stages of AD during the follow-up.
In the time-dependent Cox proportional hazards model, pre-frailty and frailty showed no significant effects on all the NPSs in CN participants after a mean follow-up of 6.13 years (Fig. 3A). In MCI participants, after a mean follow-up of 4.48 years, pre-frailty (HR = 1.41, 95% CI = 1.15–1.73) rather than frailty was associated with a higher risk of developing NPSs. Higher mFI was significantly associated with a higher risk of affective symptoms including depression and apathy. Of note, pre-frailty rather than frailty was a risk factor for anxiety (HR = 1.34, 95% CI = 1.08–1.66) and aberrant appetite (HR = 1.27, 95% CI = 1.02–1.59). In addition, frailty increases the risk of delusion (HR = 2.12, 95% CI = 1.09–4.10). Higher mFI was significantly associated with a higher risk of aberrant motor behavior and euphoria (Fig. 3B). In AD participants, after a mean follow-up of 1.75 years, frailty was significantly associated with a higher risk of apathy (HR = 2.99, 95% CI = 1.30–6.84) and delusion (HR = 6.23, 95% CI = 1.41–27.55) (Fig. 3C).

The effects of frailty on the risk of NPSs at different stages of AD during follow-up. In the time-dependent Cox proportional hazards model, pre-frailty and frailty have no significant effect on all NPSs in CN participants after a mean follow-up of 6.13 years (A). After a mean follow-up of 4.48 years, in MCI participants, pre-frailty rather than frailty has a higher risk of developing NPSs. Higher mFI was significantly associated with a higher risk of affective symptoms including depression and apathy. Pre-frailty rather than frailty was a risk factor for anxiety and aberrant appetite. In addition, frailty increases the risk of delusion. Higher mFI was significantly associated with a higher risk of aberrant motor behavior and euphoria (B). Finally, after a mean follow-up of 1.75 years, in AD participants, frailty was significantly associated with a higher risk of apathy and delusion (C). The HR or 95% CI between frailty and some NPSs could not be calculated due to the insufficient of participants. All model was adjusted for age, gender, education, and APOE ɛ4 status. *p < 0.05, **p < 0.01, and ***p < 0.001, respectively. AD, Alzheimer’s Disease; HR, hazard ratio; CI, confidence interval; NPSs, neuropsychiatric symptoms; CN, cognitively normal; MCI, mild cognitive impairment.
During the follow-up, 500 participants showed cognitive progression. The time-dependent Cox proportional hazards model showed that among the participants with cognitive progression after a mean follow-up of 5.51 years, frailty was significantly associated with a higher risk of depression (HR = 2.05, 95% CI = 1.22–3.44) and apathy (HR = 1.78, 95% CI = 1.06–2.98); frailty increased the risk of delusion (HR = 2.78, 95% CI = 1.29–5.96) and sleep problems (HR = 1.84, 95% CI = 1.06–3.21); and pre-frailty increased the risk of irritability (HR = 1.36, 95% CI = 1.03–1.80) and euphoria (HR = 1.97, 95% CI = 1.07–3.64) (Supplementary Table 2).
Causal mediation analyses
We next investigated whether frailty contributed to NPSs via modulating brain structures and inflammatory markers. We selected MCI patients as the target population, in which frailty was significantly associated with more NPSs (Supplementary Table 3). We found that the relationships between frailty and NPSs were mediated by the hippocampus volume, whole brain volume, and monocytes. These mediation effects were considered partial mediation with the mediating proportions of 9.24% (hippocampus volume), 9.29% (whole brain volume) and 8.40% (monocytes) (Fig. 4).

Mediation analyses with NPSs as the outcome in mild cognitive impairment participants. The relationship between frailty and NPSs was mediated by the hippocampus, whole brain volume, and monocytes among mild cognitive impairment participants. NPSs, neuropsychiatric symptoms; IE, indirect effect; Path a, regression model of mediators on frailty; Path b, regression model of the neuropsychiatric symptoms on mediators; Path c, regression model of neuropsychiatric symptoms on frailty; Path c’, regression model of neuropsychiatric symptoms on both frailty and mediators.
Subgroup analyses according to demographic characteristics at baseline among MCI participants
Subgroup analyses were conducted to explore the interaction between individual demographic characteristics and frailty in MCI participants, as shown in Supplementary Table 4. In females, frailty was associated with more NPSs, especially affective symptoms, compared to males. However, frailty was associated with the occurrence of NPSs in participants with advanced age.
Sensitivity analyses
Firstly, we categorized participants into two frailty statuses and examined the effect of frailty on NPSs. Consistent with our primary results, the sensitivity analyses showed that frailty had no significant association with any NPS in CN participants at baseline and during follow-up. Among MCI participants, frailty was still significantly associated with a higher risk of NPSs, especially affective symptoms including depression, anxiety, and apathy, at baseline and during follow-up (Supplementary Table 5). Moreover, among the MCI participants, after excluding the participants with a follow-up≤2 years, the time-dependent Cox proportional hazards model showed similar results: pre-frailty was associated with a higher risk of developing affective symptoms including depression (HR = 1.35, 95% CI = 1.06–1.73), anxiety (HR = 1.29, 95% CI = 1.00–1.66), and apathy (HR = 1.36, 95% CI = 1.05–1.76); frailty showed no significant associations with affective symptoms, hyperactivity, or psychosis; and frailty was associated with a higher risk of euphoria (HR = 4.05, 95% CI = 1.70–9.67) (Supplementary Table 6).
DISCUSSION
With 2,155 adults included, our study found the associations between frailty and the risk of NPSs at different stages of AD. Our cross-sectional analysis showed significant associations between frailty and the incidence NPSs especially affective symptoms in MCI and AD participants. Furthermore, Cox proportion regression models showed that pre-frailty and frailty were longitudinally associated with some affective symptoms and psychosis among MCI participants and those with cognitive progression. Sensitivity analyses demonstrated that frailty remained a risk factor for affective symptoms among MCI participants. Moreover, the mediation effects of hippocampus volume, whole brain volume, and monocytes were revealed on the associations between frailty and the occurrence of NPSs, with their mediating proportions of 9.24% (hippocampus volume), 9.29% (whole brain volume), and 8.40% (monocytes).
To our knowledge, this is the first prospective study investigating the longitudinal associations between frailty and the incidence of NPSs at different stages of AD and exploring the mediators of such associations. Depression and apathy are the most frequently observed in people with MCI and early AD, which are more susceptible to frailty than other NPSs [42]. Previous studies found that frailty was significantly cross-sectionally associated with depression, regardless of cognitive status [43–45]. We also demonstrated that frailty was significantly cross-sectionally associated with depression in AD participants but not MCI participants. In addition, we found that frailty did confer a higher risk of depression in participants with MCI and cognitive progression during the follow-up. Two previous studies found apathy was a risk factor for frailty in both cross-sectional and longitudinal analyses [46, 47]. We also observed that frailty was significantly cross-sectionally associated with incident apathy in MCI and AD participants, and it increased the risk of incident apathy in MCI, AD, and cognitive progression participants during the follow-up. A strong link has been demonstrated between frailty and anxiety in both younger and older adults by a prospective population-based cohort study [48]. Our study showed that pre-frailty was significantly associated with incident anxiety in MCI and AD participants cross-sectionally, and pre-frailty increased the risk of incident anxiety in MCI participants during the follow-up. The above associations between frailty and these three affective symptoms remained robust in sensitivity analyses. Frailty had significant associations with some psychotic disorders such as aberrant motor behavior and sleep problems in AD people at baseline, and frailty also increased the risk of these psychotic disorders in participants with MCI and cognitive progression during the follow-up. In addition, previous studies found gender differences in depressogenic vulnerability and patterns of neuro-immune dysregulation [49]. Similarly, we found that frailty in females was cross-sectionally associated with more NPSs among MCI participants, especially affective symptoms. We also observed age differences in the associations between frailty and NPSs. To be specific, the associations between frailty and NPSs were significant among younger participants, but non-significant in those with advanced age [48]. Our findings suggest that frailty might be a valuable tool for screening NPSs among MCI and AD populations. When patients present with pre-frailty or frailty, strategies to change patients’ lifestyles should be tailored to prevent or delay the development of NPSs. Assessment and screening for frailty may have clinical implications for NPS prevention.
Though the underlying mechanisms were not completely clear, we found that frailty may affect NPSs by brain tissue such as the hippocampus volume and whole brain volume. NPSs are associated with abnormalities in specific brain regions such as the hippocampus, anterior cingulate cortex, ventromedial prefrontal cortex, and medial orbitofrontal cortex [3, 12]. Existing studies have found that frailty often accompanies the accumulation of senescent cells, the loss of tissue regenerative potential [50, 51], inflammatory activity, and oxidative stress [52–54], all of which may trigger neuronal loss and ultimately lead to the occurrence of NPSs. Furthermore, a previous study revealed that frailty was associated with higher levels of inflammatory markers, such as C-reactive protein and interleukin-6 [28]. Evidence showed that increased peripheral monocytes could lead to acute sickness behaviors by producing pro-inflammatory cytokines [55]. Our results of the mediation effect suggested that monocytes also played a partial role in the effects of frailty on NPSs, which indicated that peripheral immunity may be a promising direction for NPS prevention and treatment. In addition, there is evidence that dopamine and serotonin (5-HT) systems play a predominant role in the field of effort-based decision-making for rewards [56, 57], which are related to depression and apathy [52]. Endocrine system dysfunction is one of the most common characteristics in patients with frailty [58, 59]. There are differences in developmental subtypes and sex hormones between females and males, making females more vulnerable to chronic stress than males, which might lead to either chronic excessive inflammation or a state of immunosuppression [60, 61]. This could partially explain the greater susceptibility of females to stress-related psychiatric disorders including major depression and anxiety. Of note, the reason why the associations between frailty and the majority of NPSs were not significant among participants with advanced age may be that physiological systems affecting mental health such as hormonal alterations or inflammation become less active in later life [62, 63].
The current study has several strengths. Given that the longitudinal studies on the association between frailty and incident NPSs were scarce, we provide first-hand prospective evidence in this regard. Furthermore, we divided the participants according to different cognitive statuses to better reflect the impact of frailty on NPSs across the AD continuum. Finally, we used informant-observed NPI-Q to assess NPSs, and used FI to evaluate frailty. The FI has better predictive power for adverse health outcomes [64]. And it has been validated as a proxy for accelerated aging [65].
However, several limitations of our study should be taken into consideration. First, we excluded many participants due to the missing data on frailty assessments and NPSs, which might introduce potential bias. Second, some NPSs were based on a shorter period, for example, depressive episodes require only 2 weeks [66]. Such episodes of NPSs may therefore have just been missed, which might have underestimated the effects of frailty. Third, data on the components of the FI were collected through self-reported medical history, and reporting bias might exist. However, a study found that the characteristics of frailty are similar, regardless of using self-reported or test-based measures to construct an index of frailty [67]. Fourth, our study mainly included white participants, and the associations we observed between frailty and NPSs are warranted to be replicated in other ethnicities. Fifth, the associations based on observational longitudinal research were not necessarily causal relationships. A Mendelian randomization study is required to examine the potential roles of frailty in the future prevention of neuropsychiatric disorders.
Conclusion
In conclusion, the present study uncovered close relationships of frailty with NPSs at different stages of AD, especially depression, anxiety, and apathy. We further showed the associations could be partly mediated by the hippocampus, whole brain, and monocytes. Prevention and management of frailty at different stages of AD might facilitate the prevention of specific NPSs. Integrating frailty assessment into the primary prevention of NPSs may favour the identification of high-risk individuals. Though the underlying mechanisms were not completely clear, these results still offer new evidence for the effects of frailty on NPSs. More studies are needed to strengthen the evidence base and validate these findings.
AUTHOR CONTRIBUTIONS
Hao-Chen Chi (Formal analysis; Methodology; Software; Visualization; Writing – original draft; Writing – review & editing); Ling-Zhi Ma (Formal analysis; Methodology; Software; Visualization; Writing – original draft; Writing – review & editing); Zhi-Bo Wang (Formal analysis; Methodology; Software; Visualization; Writing – original draft); Ze-Hu Sheng (Formal analysis; Methodology; Software; Visualization); Jia-Yao Liu (Methodology; Software; Visualization); Yin-Chu Mi (Data curation; Formal analysis; Methodology); Yan Fu (Methodology; Software; Visualization); Shuang-Ling Han (Formal analysis; Methodology; Visualization); Yi-Ming Huang (Formal analysis; Methodology; Writing – original draft).
Pei-Yang Gao (Methodology; Software; Visualization); Lan Tan (Conceptualization; Funding acquisition; Supervision; Writing – original draft; Writing – review & editing); Jin-Tai Yu, Ph.D., M.D. (Conceptualization; Formal analysis; Funding acquisition; Methodology; Software; Supervision; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors thank all the Alzheimer’s Disease Neuroimaging Initiative (ADNI) staff and participants. Data collection and sharing for this project was funded by ADNI (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.;Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd. and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
). The grantee organization is the Northern California Institute for Research and education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
FUNDING
This study was supported by grants from the National Natural Science Foundation of China (82071201, 81971032), Shanghai Municipal Science and Technology Major Project (No.2018SHZDZX01), Research Start-up Fund of Huashan Hospital (2022QD002), Excellence 2025 Talent Cultivation Program at Fudan University (3030277001), and ZHANGJIANG LAB, Tianqiao and Chrissy Chen Institute, and the State Key Laboratory of Neurobiology and Frontiers Center for Brain Science of Ministry of Education, Fudan University.
CONFLICT OF INTEREST
Jin-Tai Yu and Lan Tan are Editorial Board Members of this journal but were not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
All other authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author.