
Abstract
Background:
Antioxidant diets are considered to be protective factors for cognitive function. However, comprehensive measures of antioxidant diets are lacking.
Objective:
To examine the association between the Composite Dietary Antioxidant Index (CDAI) and cognitive function in the elderly.
Methods:
This cross-sectional study included a total of 2,456 participants (≥60 years old) from NHANES 2011–2014. Calculation of CDAI based on 6 minerals and vitamins (manganese, selenium, zinc, vitamins A, C, and E). Cognitive function was measured by the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) Word Learning sub-test, Animal Fluency Test (AFT), and Digit Symbol Substitution Test (DSST). We also created a composite cognitive z-score to represent global cognition. The statistical analyses we used included multiple linear regression analyses, subgroup analyses, curve-fitting analyses, and threshold effects analyses.
Results:
After controlling for demographic characteristics, lifestyle factors, and disease history, multivariate linear regression analyses showed that increased CDAI was positively associated with scores on global cognitive function and each cognitive domain (p < 0.05), with subgroup analyses suggesting that this association was more pronounced in stroke patients (p for interaction < 0.05). Curve-fitting analyses and threshold effect analyses showed saturation effects between CDAI and CREAD Test, AFT, and composite Z-score, and an inverted U-shaped relationship with DSST, with inflection points of –1.89, 0.79, 1.13, and 1.77, respectively.
Conclusions:
Our findings support that higher levels of CDAI are correlated with significantly elevated cognitive function. Maintaining CDAI in an appropriate range may contribute to cognitive health in elderly.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the most common cause of dementia in the aged population, having a significant negative impact on their quality of life and health. It is a degenerative illness of the brain with progressive dementia as its primary clinical manifestation [1]. According to the World Alzheimer Report 2022, the aging and growing global population will cause around 152 million people to suffer from dementia by the year 2050 [2]. Few clinically viable therapies for dementia have been developed in the last few decades, and early prevention has clearly been a key point in impeding the progression of the disease course. Scholars believe that cognitive dysfunction is an important predictor of dementia and that applying early interventions to slow the progression of mild cognitive dysfunction (i.e., preclinical dementia) to dementia is of great clinical value [3, 4]. Therefore, identifying modifiable risk factors for cognitive impairment and making timely lifestyle changes are important in preventing AD.
One major risk factor for the etiology and development of cognitive function impairment is oxidative stress (OS) [5]. The unique characteristics of the brain, including its high oxygen consumption (20% of the body), rich lipid content, and low antioxidant capacity, make it extremely vulnerable to OS [6]. OS is a state in which oxygen free radicals and other reactive oxides cause damage to biological molecules [7]. There is growing evidence of a strong relationship between excessive OS and cognitive impairment, as well as neurodegenerative diseases such as AD [8]. The role of diet is crucial in this context, as it provides exogenous antioxidants that effectively reduce the concentration of various biomarkers associated with OS in the body [9]. A recent review examining nutritional supplements and cognitive function during aging indicated that important antioxidants, including specific vitamins (i.e., vitamins A, C, and E), and minerals such as selenium and zinc, play potentially important roles in maintaining cognitive functions, such as attention, memory, and executive functioning during aging [10]. One population-based prospective cohort study concluded that a higher intake of antioxidant vitamins was associated with a lower risk of AD [11]. The underlying mechanisms may involve reactive oxygen species (ROS) scavenging and the inhibition of free radical-mediated lipid peroxidation to counteract OS and maintain cognitive processes [12–14]. In addition to antioxidant vitamins, mineral supplementation also plays a key role in supporting brain and cognitive health [15]. Several studies have shown that low intakes of manganese, selenium, and zinc are associated with poorer cognitive performance [16–18]. The underlying pathway may be that mineral deficiency leads to impaired synthesis and function of antioxidant enzymes such as glutathione peroxidase, superoxide dismutase and others [19, 20]. Therefore, we propose that dietary modification may be an effective way to mitigate cognitive impairment by reducing the level of OS in the body.
Considering the complex composition of the foods that people consume in their daily lives, people do not consume nutrients in isolation; rather, they consume food groups consisting of a wide variety of foods. Many dietary antioxidants with similar sources may have complex synergistic effects in vivo [21, 22]. The “single-nutrient” approach may not be sufficient to take into account the complex interactions between nutrients. Current trends in nutritional science have shifted from an emphasis on specific nutrients to an emphasis on overall diet quality [23].
In recent years, more and more scholars have focused on dietary patterns or diet quality to better understand the link between diet and cognitive decline or dementia. Xu et al. calculated an assessment of total antioxidant capacity in the diet based on eight antioxidant vitamins and also concluded that higher dietary antioxidant potential was associated with a reduced risk of cognitive dysfunction [24]. Similarly, Song et al. found a strong positive correlation between oxidative balance score and cognitive function among elderly Americans employing the oxidative balance score, a metric that integrates food and lifestyle [25]. Inconsistently, a US Nurses’ Health Study assessing dietary total antioxidant capacity based on a measure of iron-reduced antioxidant capacity associated with cognition in older women did not find a significant correlation between total dietary antioxidant capacity with cognitive performance [26]. We chose the Composite Dietary Antioxidant Index (CDAI) developed by Wright et al. as the exposure factor for our study [27]. In contrast to traditional dietary antioxidant indicators, the CDAI takes into account both the important antioxidant vitamins A, C, and E, as well as the micronutrients manganese, selenium, and zinc, which have indispensable antioxidant properties. By normalizing and summing their intakes, the CDAI provides a comprehensive assessment that gives a more complete picture of dietary antioxidant levels. In a prospective cohort study, Lu et al. observed a negative correlation between the CDAI and pro-inflammatory factors such as tumor necrosis factor-α and interleukin-1β, providing a basis for the accuracy of the index [28]. CDAI has demonstrated its application advantages and effectiveness in a number of epidemiological studies [29–32].
Therefore, the aim of this study was to examine the relationship between CDAI and cognitive function in older adults using the National Health and Nutrition Examination Survey (NHANES) dataset in a comprehensive cross-sectional analysis, aiming to add new evidence and insights to existing studies exploring the antioxidant capacity of the combined diet and cognitive function.
METHODS
Survey description
NHANES is a population-based, cross-sectional survey conducted by the U.S. Centers for Disease Control and Prevention (CDC) and the U.S. National Center for Health Statistics (NCHS) to collect accurate data related to health and nutrition. The NHANES was conducted regularly from 1971 to 1994, and in 1999, NHANES became continuous. Each year, approximately 5,000 people of all ages are interviewed in their homes and complete the home interview portion of the survey. Physical examinations and laboratory tests are carried out at mobile examination centers, which provide an ideal set-up for collecting high-quality data in a standardized environment. The dataset used in this study included information collected in 2011, 2012, 2013, and 2014. A total of 19,931 participants aged 20–80 years (mean age 31.5±24.5) participated in the study during the 2011–2014 cycle. A representative civilian, non-institutionalized US population was chosen for this study employing a complicated, multi-stage random sampling design [33]. NHANES was granted approval by the National Centre for Health Statistics Research Ethics Review Board. Each participant gave written informed consent before taking part in this study [34].
Study population
We retrieved published data on 19,931 participants aged 20–80 years from the 2011–2014 survey cycle of the NHANES and implemented strict inclusion exclusion criteria: Inclusion Criteria: Participants aged≥60 years. Enrollment: Included in the NHANES 2011–2014 survey. Exclusion Criteria: 1) Participants with incomplete data from the Assessment of Cognitive Functioning; 2) Participants with missing data on dietary intake, including manganese, selenium, zinc, vitamins A, C, and E; 3) Participants with missing covariate data. Specifically, 16,299 participants younger than 60 years of age, 698 participants without data on cognitive function assessment, 412 participants without data related to dietary intake, and 66 individuals with missing covariates were excluded from the final study, ultimately streamlining the sample size of 2,456 older Americans (Fig. 1).

The flow chart of participant selection.
Composite dietary antioxidant index
Trained technicians conducted two rounds of 24-hour dietary review interviews with respondents as part of NHANES data collection and assessment of their food consumption. Recalling information about the food and beverages they had consumed in the 24 hours before the interview was requested of the participants. The initial dietary recollection interview was done face-to-face at the mobile examination center, and the follow-up interview was conducted over the phone 3 to 10 days later. A modified version of the CDAI proposed by Wright et al. was utilized in this investigation, whose validity has been established in previous investigations to assess the combined exposure to dietary antioxidant consumption [27, 28]. This index selected six minerals and vitamins from dietary sources that deserve to be highlighted for dietary antioxidant exposure (manganese, selenium, zinc, vitamins A, C, and E). By deducting the universal mean and dividing it by the universal standard deviation, we were able to standardize each of the six dietary vitamins and minerals. The standardized dietary antioxidant intakes were then summed to calculate the CDAI. The formula is as follows.
In this mathematical formula, Xi reflects the antioxidant intake per day, μi signifies the arithmetic average Xi of the entire cohort for antioxidant i, and Si signifies the standard deviation (SD) of μi.
Assessment of cognitive function
We obtained cognitive function assessment data in the Cognitive Functioning section of the NHANES Data Questionnaire panel. Although cognitive assessment is not a substitute for the clinician’s thinking and judgment, the results are an important reference for diagnosis and help to examine and assess the association of cognitive function with many of the medical conditions and risk factors measured during the investigation.
We provide a generalized description of the range of assessments of cognitive function in NHANES: The Consortium to Establish a Registry for Alzheimer’s Disease-Word Learning (CERAD-WL) subtest evaluates both immediate and delayed learning of new linguistic information (memory subdomains) [35]. The examination comprised three separate learning trials CERAD-WL (1–3) and a delayed recall test CERAD-DR (which occurs after the other two cognitive examinations Animal Fluency Test (AFT) and Digit Symbol Substitution Test (DSST) are completed). To get the final CERAD Test score, we added the scores from the three learning tests and the delayed recall test. AFT is carried out to examine verbal fluency and provide a measure of the organism’s executive function [36]. The DSST is administered on a paper form and is a presentation part of the Wechsler Adult Intelligence Scale (WAIS-III), which depends on working memory, information processing speed, and duration of concentration [37]. It is worth noting that all three cognitive function assessment panels have been used extensively in mass screening and major epidemiological studies in ethnically and culturally diverse communities [38–40]. Because of the lack of criteria for reflecting overall information on cognitive functioning, we standardized the data for the CERAD Test, AFT, and DSST scores separately and the mean of the three standardized scores was recorded as the composite Z-score.
Covariates
The following covariates were included to identify as many potential confounders as possible. In this study, gender, age, race, marital status, and educational attainment were analyzed as demographic variables, body mass index (BMI) was considered as an indicator to assess the overall nutritional status, alcohol, and smoking habits were included, and patients’ history of hypertension, diabetes mellitus, and stroke were included as a history of prior illness. Age (≤70/>70 years) and BMI (≤24/>24 kg/m2) were used as stratification variables when assessing the effect of interactions. Regarding smoking history or drinking history, for the former, participants who answered “yes” indicated that they had smoked at least 100 cigarettes in their lifetime, and for the latter, participants who answered “yes” indicated that they had consumed at least 12 bottles of alcoholic beverages of any type in a year. In contrast, participants who answered “no” did not. With regard to disease history, this was obtained by means of a questionnaire on the question of whether the patient had ever been told by a doctor or health professional that he or she had a relevant disease. In addition, we included the Healthy Eating Index-2015 (HEI-2015) as a covariate to evaluate overall dietary quality. The HEI-2015 is an instrument developed by the United States Department of Agriculture (USDA) that consists of 13 components, each of which represents a different aspect of a healthy diet. These components include the intake of various types of foods, such as fruits, vegetables, and whole grains, and each component is scored according to specific criteria, as described in Supplementary Table 1 [41].
Statistical analysis
The research team made use of statistical computations tools R (version 4.1.3) and EmpowerStats (version 2.0). Mean and standard deviation (SD) are used to represent continuous variables, whereas frequencies and percentages are used to describe categorical data. The CDAI was divided into quartiles, with Q1 serving as the reference group. Data were analyzed for significance using chi-square tests and weighted t-tests. Multiple linear regression analyses were used to calculate beta values and 95% confidence intervals for the association between CDAI and cognitive function. Crude Model remained unadjusted, Model 1 was adjusted for gender, age, and ethnicity, and Model 2, our core model, was adjusted for marital status, educational attainment, BMI, history of smoking and alcohol use, history of hypertension, history of stroke, history of diabetes mellitus, and HEI-2015 diet score based on Model 1. The non-linear correlation between CDAI and cognitive function was further explored utilizing curve-fitting analysis and threshold effect analysis. Finally, we performed the same statistical procedures as stated above to explore potential variance within these specific populations by doing subgroup analyses and interaction tests for age, gender, BMI, hypertensive illness, diabetes mellitus, and stroke subgroups. The level of significance in this study was set at p < 0.05.
RESULTS
Basic characteristics
This study enrolled 2,456 eligible participants in total. With 48.0% being male and 52.0% being female, the average age of the participants was 69.4±6.8 years. For the assessment of cognitive function, the mean±standard deviation of the CERAD Test, AFT, DSST, and composite Z-score were 25.15±6.39, 16.87±5.44, 47.03±16.78, and 0.00±0.80, respectively. The CDAI was considered a continuous independent variable as well as a categorical variable (split into quartiles), with the lowest quartile as the benchmark. Across subgroups of the CDAI (quartiles, Q1–Q4), significant differences existed in sex, race, education, marital status, BMI, alcohol consumption, history of hypertension, history of diabetes mellitus, HEI-2015 diet score, CERAD Test, AFT, DSST, and the composite Z-score (Table 1).
Characteristics of 2456 participants aged 60 years or older in the 2011–2014 National Health and Nutrition Examination Survey (NHANES)
Mean±standard deviation (SD) is used to represent continuous variables, whereas frequencies (percentage) are used to describe categorical data. BMI, body mass index.
Association between CDAI and Cognitive function
The findings of the multivariate linear regression analysis between CDAI and cognitive function are displayed in Table 2. After a stepwise adjustment for potential confounders, a significant positive correlation between CDAI and the four cognitive function assessment scores was detected in the Crude model, Model 1, and Model 2 (all p < 0.05). The final adjusted model 2 showed that CDAI was significantly associated with higher scores on the CERAD Test [β (95% CI) = 0.13 (0.06, 0.20)], AFT [(β (95% CI) = 0.14 (0.08, 0.20)], DSST [(β (95% CI) = 0.27 (0.12, 0.43)], and composite Z-scores [(β (95% CI) = 0.02 (0.01, 0.03)]. After categorizing CDAI into quartiles, the above associations remained statistically significant (all p for trend < 0.05). When fully adjusted for potential confounders, significantly higher scores were found for Q4-stratified participants than for Q1-stratified participants in the CERAD Test, AFT, DSST, and composite Z-score groups. Specifically, the β values were [β(95% CI) = 1.24 (0.55, 1.93), p for trend = 0.002], [β(95% CI) = 1.43 (0.85, 2.01), p for trend < 0.001], [β(95% CI) = 3.53 (2.06, 5.00), p for trend trend = <0.001], [β(95% CI) = 0.22 (0.15, 0.30), p for trend < 0.001].
Association of CDAI with cognitive function
β [95%Cl] indicates the confidence interval of the regression coefficient (β). CDAI was converted from a continuous variable to a categorical variable (Quartiles1- Quartiles4). Crude model: No adjustments. Model 1: adjusted for age, gender, and race. Model 2: Model 1+ marital status, education level, BMI, drinking, smoking, stroke, hypertension, diabetes, and HEI-2015 diet score. CDAI, Composite Dietary Antioxidant Index; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; AFT, Animal Fluency Test; DSST, Digit Symbol Substitution Test.
Nonlinear association between the CDAI and cognitive function
The adjusted smoothed curves shown in Fig. 2 demonstrate the nonlinear relationship between CDAI and cognitive function. We discovered a saturation effect link between CDAI and Z-score using a two-piecewise linear regression model. As shown in Table 3, we calculated a turning point of 1.13 for the CDAI. When the CDAI was below 1.13, the Z-score increased parabolically with increasing CDAI but eventually stabilized when the CDAI reached the saturation point, indicating that the increase in CDAI did not further increase the Z-score. This phenomenon was also observed in CERAD Test and AFT with saturation points of –1.89 and 0.79, respectively. Besides, curve fitting showed an inverted U-shaped curve of CDAI versus DSST with an inflection point of 1.77 (Table 3).
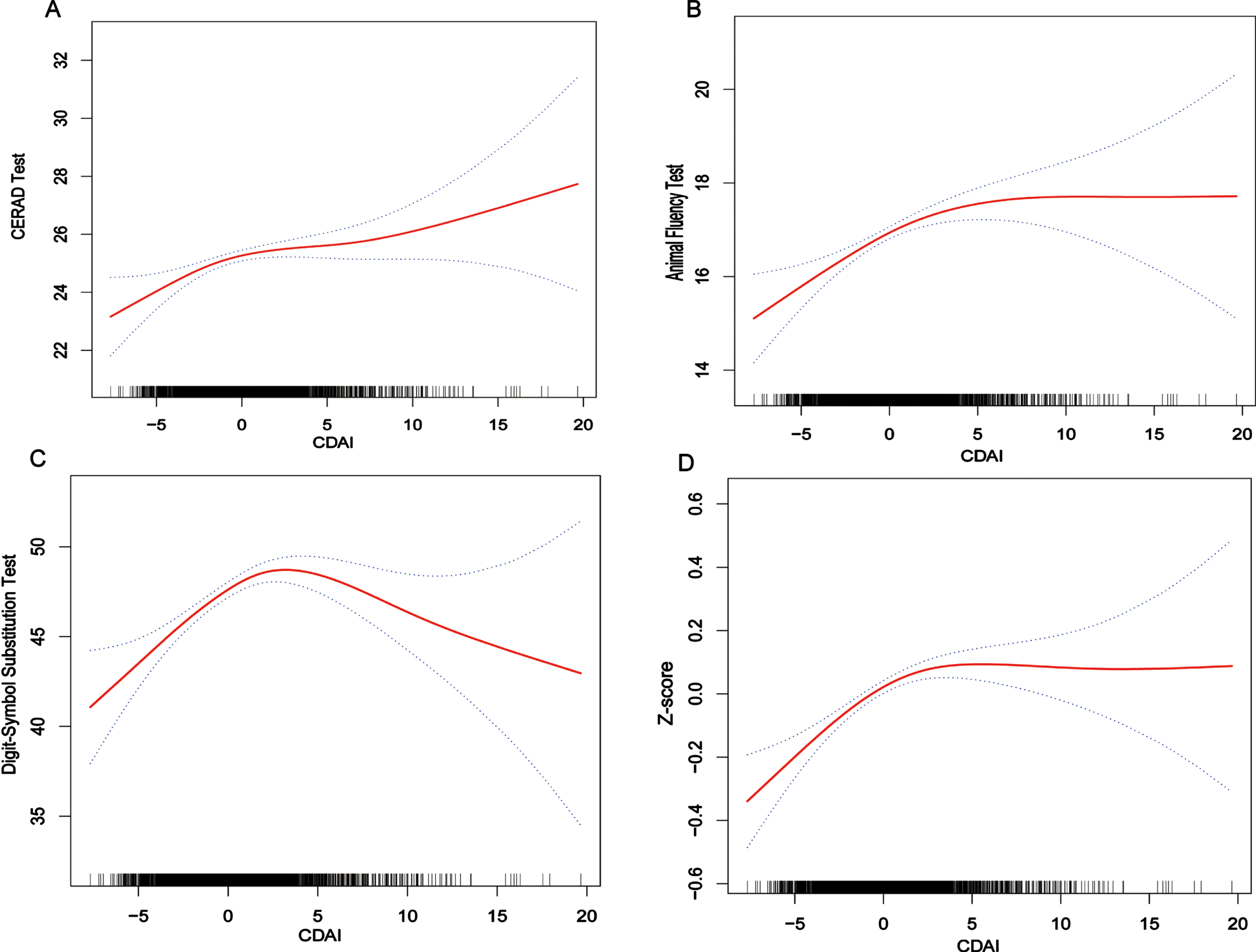
The non-linear associations between CDAI and cognitive function. The solid line represents the smooth curve fit between variables. Dotted lines represent the 95% confidence interval from the fit.
Threshold effect analysis of CDAI and cognitive function using the two- piecewise linear regression model
Adjusted β [95%Cl] indicates the confidence interval of the regression coefficient (β). Age, gender, race, marital status, education level, BMI, drinking, smoking, stroke, hypertension, diabetes, and HEI-2015 diet score were adjusted. CDAI, Composite Dietary Antioxidant Index; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; AFT, Animal Fluency Test; DSST, Digit Symbol Substitution Test; BMI, body mass index.
After analyses stratified by gender, among men, the saturation effect still lies in the relationship between CDAI and AFT, DSST, and Z-score, with saturation points of 3.85, 2.4, and –1.84, respectively. More interestingly, among women, we discovered an inverted U-shaped association between CDAI and Z-score as well as scores on all three cognitive function tests. The inflection points were 1.13, 0.52, 0.61, and 1.79, respectively (Fig. 3 and Table 3).

The non-linear associations between CDAI and cognitive function stratified by gender.
Subgroup analyses
Subgroup analyses were used to examine the relationship between CDAI and cognitive function to determine whether it was stable across subgroups, and the outcomes are shown in Fig. 4. Several subgroups were consistent in their associations, including gender (male/female), age (≤70/>70 years) and BMI (≤24/>24 kg/m2), history of hypertension (Yes/No), and history of diabetes mellitus (Yes/No) (all p for interaction > 0.05). However, there was a significant interaction between a history of stroke and CDAI. In this study, we found that the positive associations of CDAI with AFT, DSST, and Z-score were more significant in participants who had suffered a stroke [β(95% CI) = 0.37 (0.15, 0.58)], [β(95% CI) = 1.01 (0.44, 1.57)], [β(95% CI) = 0.05 (0.02, 0.08)] (all p for interaction < 0.05). As for the CREAD Test, the β value of CDAI on cognitive function was also stronger in the stroke patient group than in the non-stroke patient group, although there was no statistical interaction.

Subgroup analysis of the effect of CDAI on cognitive function. Subgroups analysis for the associations between the CDAI and CREAD Test (a), AFT(b), DSST(c), and z-score(d). Age, gender, race, marital status, education level, BMI, drinking, smoking, stroke, hypertension, diabetes, and HEI-2015 diet score were adjusted. β [95%Cl] indicates the confidence interval of the regression coefficient (β).
DISCUSSION
This cross-sectional study found that higher CDAI was significantly associated with better cognitive function in older adults, which includes several domains such as overall cognition and memory, executive functioning, processing speed, and attention. In addition, smoothed curve and threshold effect analyses revealed a saturation effect between CDAI and cognitive function, which means that cognitive function does not always improve significantly with increasing levels of CDAI in older adults, but eventually reaches a threshold and remains stable, a phenomenon that is present in older men. In contrast, for older women, there was an inverted U-shaped curve relationship between CDAI and cognitive function, suggesting that maintaining CDAI levels in the reasonable range is particularly important for the benefit of patients’ level of cognitive functioning, especially in older women. Our subgroup analyses and interaction tests suggest that the positive association between CDAI and cognitive function in older adults may be influenced by a history of stroke. Limited by the sample size of stroke patients, this result still needs further validation and extension. The outcomes mentioned above might offer some valuable theoretical pointers for preventing OS-related cognitive impairment in the elderly.
We explored a novel approach to assess the total antioxidant capacity of diets through the use of CDAI. An important advantage of this approach is the inclusion and standardization of both important antioxidant vitamins and important antioxidant minerals, and the use of a holistic approach to examine the overall impact of various antioxidants, which is able to capture possible interactions between antioxidant nutrients in foods. At the same time, we calculated a composite Z-score based on traditional cognitive scores to better assess participants’ overall cognitive functioning. Our findings are consistent with those of Peng et al. and Song et al. that there is a strong positive correlation between the antioxidant capacity of a complex diet and cognitive function [24, 25]. However, an American Nurses’ Health Study did not find a significant correlation between total dietary antioxidant capacity and cognitive performance [26]. One possible explanation for the discrepancies observed in the study results could be the potential for errors arising from variations in the algorithms used to calculate the different composite antioxidant indices. In addition, the diversity of dietary patterns between countries may be another contributing factor. Thirdly, variations in demographic variables (e.g., race) across studies may lead to inconsistent final findings. Overall, these factors need to be taken into account for a comprehensive assessment in future studies.
ROS are metabolic byproducts that are harmful when present in excessive amounts yet are required for physiological function [42]. The brain has a high demand for oxygen and is highly susceptible to peroxidative damage, and these oxidative stressors increase progressively over the life cycle, undermining the operation of mitochondria and causing harm to different bodily sections, particularly the central nervous system [8, 43]. Fukui et al. compared the cognitive performance of hyperoxia-treated aged and young rats, and they found that nerve endings in the former were more susceptible to OS. The experimental results showed that hyperoxia treatment increased thiobarbituric acid reactive substances in the hippocampus, cerebral cortex, and synaptic membranes of aged rats, and the release of acetylcholine from the nerve endings was significantly reduced, suggesting that cognitive functions of rats may be affected by OS and aging [44]. Furthermore, an overabundance of intracellular ROS can trigger the activation of the NF-κB pathway, initiate the expression of genes that promote inflammation, elevate inflammatory mediators, and result in systemic inflammation. This chronic condition could potentially be linked to cognitive impairment associated with aging [45]. In addition, a possible explanation for the results of our subgroup analysis is that the nervous system of stroke patients tends to be severely impaired due to the oxidative state and inflammatory response caused by excess free radicals [46–48]. However, the exact molecular mechanisms remain unclear, which needs to be verified by more basic experiments and prospective studies.
Because the efficiency of the endogenous antioxidant system in the body decreases as a person ages, exogenous antioxidants in the diet are essential in counteracting the effects of OS on brain health, which may explain the positive association of CDAI with cognitive scores in our study [49]. Numerous dietary antioxidants can exert antioxidant effects through their bioactive molecules acting as cell signaling regulators [50, 51]. Zinc, selenium, and manganese are essential antioxidants that shield the body from OS [52, 53]. Antioxidants that are not enzyme-based, such as vitamins A, C, and E, are crucial in mitigating oxidative alterations brought on by stress [54, 55]. These antioxidants tend to have similar dietary sources and they may act synergistically in interacting pathways that maintain cognition. For example, many antioxidants often need the support of other vitamins and phytochemicals from the same source to work [56]. In this way, CDAI can provide further information as it is able to identify and classify possible sources of antioxidants in complex diets. The combined effects of the CDAI evaluation of overall dietary antioxidant capacity on cognitive function can be more directly translated into dietary recommendations for public health education.
Our study has some limitations. Firstly, due to the cross-sectional study design, data collection for this study took place at a specific point in time and was unable to capture the dynamics of the variables. As a result, we were only able to observe an association between CDAI and cognitive functioning, rather than determining causality. Secondly, there can be measurement errors and inaccuracies in the dietary evaluation due to the lengthy duration of this study and the intricate design of the CDAI. Thirdly, the bioavailability and in vivo action of antioxidants upon intake were not taken into account in this investigation. Also, we are unable to completely exclude the possibility of further confounders, even after accounting for a number of significant ones. Limiting the study sample to the older population may also pose certain limitations. The findings may not be generalizable to other age groups. Therefore, caution should be exercised in interpreting our findings. The potential mechanisms behind the association between CDAI and cognitive function require more investigation. Future studies need to consider longitudinal designs or repeated measures to better understand the dynamics and causal relationships between variables.
Conclusions
In conclusion, this cross-sectional study indicates that older adults in the United States who have high levels of CDAI, a comprehensive indicator for assessing antioxidant diets, appear to have better cognitive performance. Moreover, we found a saturation effect between CDAI and CREAD Test, AFT, and composite Z-scores, and an inverted U-shaped association with DSST. This adds new evidence to existing studies exploring composite antioxidants and cognitive function. Further studies are necessary to explore the mechanisms underlying these associations.
AUTHOR CONTRIBUTIONS
Jiesheng Mao (Conceptualization; Data curation; Formal analysis; Funding acquisition; Methodology; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing); Haoxiang Hu (Funding acquisition; Investigation; Methodology; Project administration); Yunhan Zhao (Data curation; Methodology; Resources; Validation; Visualization); Mi Zhou (Data curation; Project administration; Resources; Software; Visualization); Xiaokai Yang (Funding acquisition; Investigation; Methodology; Project administration; Visualization; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors express their gratitude to the National Health and Nutrition Examination Survey for granting the data access for this study and all the participants in NHANES 2011–2014.
FUNDING
This research did not receive any specific funding from any funding body in the public, commercial, or not-for-profit sectors.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.