
Abstract
Evidence in the literature indicates that aerobic physical activity may have a protective role in aging pathologies. However, it has not been clarified whether different types of aerobic exercise produce different effects. In particular, these potential differences have not been explored in patients with Alzheimer’s disease (AD). The present narrative review has the specific aim of evaluating whether land (walking/running) and water (swimming) aerobic activities exert different effects on cognitive functions and neural correlates in AD patients. In particular, the investigation is carried out by comparing the evidence provided from studies on AD animal models and on patients. On the whole, we ascertained that both human and animal studies documented beneficial effects of land and water aerobic exercise on cognition in AD. Also, the modulation of numerous biological processes is documented in association with structural modifications. Remarkably, we found that aerobic activity appears to improve cognition per se, independently from the specific kind of exercise performed. Aerobic exercise promotes brain functioning through the secretion of molecular factors from skeletal muscles and liver. These molecular factors stimulate neuroplasticity, reduce neuroinflammation, and inhibit neurodegenerative processes leading to amyloid-β accumulation. Additionally, aerobic exercise improves mitochondrial activity, reducing oxidative stress and enhancing ATP production. Aerobic activities protect against AD, but implementing exercise protocols for patients is challenging. We suggest that health policies and specialized institutions should direct increasing attention on aerobic activity as lifestyle modifiable factor for successful aging and age-related conditions.
Keywords
GENERAL OVERVIEW
The World Health Organization (WHO) recommends physical activity as a protective factor for physical and mental health [1]. According to the WHO, adults between the ages of 18 and 64 years should engage in at least 150 minutes of moderate-intensity aerobic physical activity or at least 75 minutes of vigorous-intensity aerobic physical activity per week. Additionally, muscle-strengthening activities involving major muscle groups are recommended at least twice a week. Physical activity is key in maintaining physical health, including reducing risk of cardiovascular diseases, Type 2 diabetes, some types of cancer, and improving bone and muscular health [2–6]. It also plays a crucial role in promoting mental health, including reducing symptoms of anxiety and depression, and improving cognitive function including memory, attention, and processing speed [7–9]. The benefits of physical activity are dose-dependent, meaning the more one engages in physical activity, the greater the health benefits [8, 10]. However, even small amounts of physical activity, such as short bouts of walking, have been found to improve one’s health [11]. It is important to note that physical activity is distinguished from physical exercise as such because it is to not just limited to going to the gym or performing structured exercise programs. The WHO defines physical activity as “any bodily movement produced by skeletal muscles that requires energy expenditure” [1]. It can include everyday activities such as walking, cycling, gardening, and household chores. The important thing is to find physical activities that one enjoys and can be sustained long-term [12, 13]. The WHO suggests that everyone can benefit from physical activity, regardless of age or fitnesslevel [1].
Physical activity can involve both aerobic and anaerobic exercises. According to WHO physical exercise can be defined as a “subcategory of physical activity that is planned, structured, repetitive, and purposeful in the sense that the improvement or maintenance of one or more components of physical fitness is the objective” [1]. Specifically, aerobic exercise is characterized by prolonged, moderate/high intensity activities that raise oxygen consumption and circulatory demands. Examples include walking, running, and swimming [14]. Non-aerobic exercise, on the other hand, involves brief, high intensity activities that primarily rely on the anaerobic metabolism for energy, which may include weightlifting and sprinting [15]. Although both types of exercise offer unique health benefits, aerobic exercise has been shown to have a greater impact on improving cardiovascular health, while non-aerobic exercise is more effective for building and maintaining musclemass [16, 17].
Recent studies have highlighted the positive effects of aerobic exercise on cognitive function, neural health, and brain plasticity [18–20]. Such evidence is in strong agreement with the concept of brain, cognitive, and neural reserves postulated by Stern [21–24]. According to Stern’s model, brain reserve refers to the total amount of neural tissue in the brain, in terms of number of neural cells and synapses, richness of neural complexity and circulatory substrate, powerful expression of molecular factors [14, 25–29]. Cognitive reserve is the ability to compensate for brain damage or loss of function through the use of more effective or alternative cognitive strategies and/or their adaptations [30–34]. Neural reserve is the ability of neurons to continue to function even if other neurons become damaged or die, by recruiting more efficient or alternative neural networks [35–38]. Finally, Stern adds also the concept of maintenance of cognitive function that involves the utilization of the reserve capacities to maintain optimal mental function, even in the face of injury or age-related decline. Stern’s model suggests that individuals with higher cognitive reserve are better able to cope with age-related changes and cognitive decline than those with lower reserve [39]. This model proposes that brain/cognitive/neural reserve is influenced by several environmental factors including education, occupation, and leisure activities, including physical exercise [22, 40–42].
In this framework, several studies have investigated the relationship between physical exercise and reserve mechanisms. Already several years ago, a study by Ahlskog et al. [43] examined the relationship between exercise and reserves and found that regular exercise was associated with increased brain volume and reduced risk of cognitive impairment in older adults.
A recent study by De Sà et al. [44] investigating the effects of physical exercise on cognitive function in individuals with mild cognitive impairment (MCI) found that exercise improved their cognitive function, suggesting that physical exercise may be a valuable tool in preventing or delaying the onset of dementia. Thus, the evidence indicates that physical exercise is a key promoter of brain/cognitive/neural reserve, neural health and brain plasticity and highlight the importance of incorporating regular physical activity into daily life to maintain optimal cognitive and neural health across the lifespan. Also, a recent systematic review highlighted that physical activities positively impacted on behavior of patients with dementia living in residential aged care facilities and reduced behavioral and psychologicalsigns [45].
In this framework, we recently reviewed human and animal studies on healthy individuals to deepen the mechanisms leading to brain/cognitive/neural reserve development in the presence of different aerobic exercise types [14]. We considered land (walking or running) and water (swimming) activities. The findings confirmed that both the types of activities positively affect cognitive/behavioral performance and the underlying brain neurobiology. Memory and executive functions resulted to be the cognitive domains more improved by the exposure to aerobic exercises. Structural and functional modifications were found mainly in the fronto-hippocampal axis (for more details see [14]). Reserve mechanisms reported in healthy populations are valuably involved in cope with age-related neuropathological processes underlying cognitive decline, as typically observed in Alzheimer’s disease (AD). AD is characterized at brain level by the extracellular accumulation of amyloid-β (Aβ) plaques and intracellular accumulation of hyperphosphorylated tau protein [46]. These pathological changes are accompanied by progressive atrophy of the hippocampus and other brain regions involved in memory and cognitive functions. Since the early stages of the disease, functional magnetic resonance imaging (fMRI) studies have also shown disruption of resting-state connectivity networks [47], such as default mode network (DMN), executive networks, and fronto-parietal network, with decreased activity in regions associated with memory, attention, and executive functions [48]. Additionally, there is evidence of altered brain glucose metabolism and blood flow [49].
On this basis, we review here the available evidence on brain/cognitive/neural reserve development mechanisms specifically induced by aerobic exercise, by deepening the specific effects of land and water activities in both human and animal individuals in the presence of cognitive decline and concomitant neurodegeneration. In the following, after a general synthesis of aerobic exercise effects on cognition in AD, specific analyses of the land and water activity effects will be reported. The results of our literature search are updated to April 2023.
AEROBIC EXERCISE EFFECTS ON COGNITIVE FUNCTIONS AND NEURAL SUBSTRATES IN ALZHEIMER’S DISEASE
Humans
Several studies promoted the physical exercise as a modifiable lifestyle factor associated with a decreased risk to develop dementia [50, 51]. Geda et al. [50], by using a self-report questionnaire, investigated the association between physical exercise of different intensity (low, moderate, and vigorous) and frequency (ranging from 1 time a month to daily) and risk to develop MCI in a large cohort of elderly people. They found that any frequency of moderate exercise performed in midlife was related with a reduced risk of having MCI. A recent study showed a significant improvement in executive functions after aerobic exercise in a group of MCI patients [52]. On the contrary, AD patients did not show a beneficial effect on cognition after aerobic training [52]. In a longitudinal case-study [53], two healthy elderly subjects positive for AD-biomarkers performed regularly a vigorous aerobic training (tennis and treadmill, respectively) during their midlife. They were regularly followed-up for 16 and 8 years receiving the diagnose of mild AD and MCI at the last visit. During the follow-up period both patients showed a very slow progression of cognitive dysfunctions. The Authors argued that practice a regular vigorous aerobic exercise exerted a protective effect on cognitive functions [53]. A group study reported that AD patients who were APOE ɛ4 allele carriers after 16-weeks of aerobic exercises (the training was performed 3 times a week and it included treadmill, stationary bike, and cross-trainer) showed improved cognitive functions, ameliorated physical performances, and less behavioral disturbances [54]. A recent systematic review reported that regular aerobic activity is associated with a reduction of pro-inflammatory cytokines in individuals with MCI [55].
However, a recent study found that aerobic exercise did not impact on neurodegenerative process as measured by neurofilament light in patients with AD [56].
Animal models
The effects of physical activity on cognitive functions have been largely investigated in preclinical studies. Evidence is available in both healthy and pathological animal models [14, 57–59]. The advantage of using animal models is provided by the possibility to rely on more effective management and high-level control due to basic genetical and physiological homogeneity, shorter gestational period and lifespan, numerous progenies, large chance of variable manipulation, and wide opportunity of deeply investigating nervous structure and biology [60]. Specifically, human aerobic and anaerobic exercises can be mimicked in rodents by utilizing ad hoc apparatuses. Anaerobic activity is performed by the animals in resistance training aimed to reach higher muscular strength and power (to give some examples, progressive training to climb a ladder with a load or to lift weight) [61]. Aerobic activity is studied in animals mainly by focusing on walking, running, and swimming activities. Walking and running activities can be structured in models of voluntary or forced exercises, by using specific running wheels, motorized or not, or walking/running treadmills, with controlled determination of speed and inclination [62, 63]. Moreover, swimming activity may be studied by placing the animals in a water pool, taking advantage of the rodents’ innate ability to swim [62].
On the whole, a larger bulk of studies has been devoted to the investigation of the effects on cognitive processes and neural correlates elicited by aerobic activity, compared to the anaerobic one [14, 64]. Aerobic exercise has been largely demonstrated to beneficially affect cognitive functions in rodent models of pathological aging, mild cognitive impairment, and AD [65]. In particular, learning and memory abilities appear improved in various components, such as spatial, contextual, and recognition memories [66]. Such beneficial effects are supported by numerous neuroplastic alterations. Specifically, a key role has been evoked for the neurotrophin brain-derived neurotrophic factor (BDNF) whose expression is affected by aerobic activity in aging and AD models [65, 67]. Moreover, studies on pathological aging models demonstrated also that aerobic exercise improves hippocampal function by augmenting neurogenesis [65, 66]. In addition, aerobic exercise strongly mitigates pro-inflammatory cytokines’ expression in the aging brain, as shown in rodents’ pathological models [55].
LAND ACTIVITIES AND COGNITION IN ALZHEIMER’S DISEASE PATIENTS AND ANIMAL MODELS
Human studies
A recent study [68] investigated the association between Nordic Walking and cognitive functioning in a group of patients with AD. The Nordic Walking is a particular aerobic activity in which walking is combined with the involvement of the entire upper body and arms by using poles. This activity requires an increased oxygen consumption than simple walking, improve the endurance and muscle strength. Authors reported an improvement in executive functions after training in a group of AD patients who underwent Nordic Walking compared to a group of AD patients who underwent Reality Orientation Therapy and Music therapy.
Chirles and colleagues [69] investigated the association between walking and brain functional connectivity changes in MCI patients. Patients with MCI and a group of healthy controls underwent 12-week walking training. After training the MCI group showed an increase of functional connectivity within the posterior nodes of DMN. The authors argued that these functional connectivity changes represented an enhancement of neural recruitment that may have a role in the cognitive compensatory mechanisms [69]. A recent study [70] showed increased connectivity in several brain networks including DMN, frontoparietal and salience networks, after walking training in patients with MCI and healthy elderly individuals. In addition, individuals who underwent training showed also improvement in memory functions [70]. ten Brinke et al. [71] compared the effect on hippocampal volumes of walking against resistance training or balance and tone training in female patients with MCI. Patients who underwent walking showed a bilateral increase of hippocampal volume respect to the other groups [71]. Recently, the effects of the walking activity on cognition and brain activation has been compared to dancing in older adults at risk of dementia [72]. The authors showed that walking and dancing improved executive functions and brain activation during a functional MRI task. However, no differences between the two typologies of physical exercise were detected [72]. Details of the above-mentioned studies are reported in Table 1.
Land activity effects on cognitive functions and neural substrates of Alzheimer’s disease patients
Animal models
A great bulk of studies investigated the effects of aerobic land activities in animal models of AD. Even just by analyzing the most recent studies, it is found that this type of activity is able to alleviate the cognitive alterations resulting from the pathology. These effects are supported by the modulation of several biological processes and by structural changes in the brain. Furthermore, it is possible to note that beneficial effects follow both voluntary (free access to wheels) and involuntary (motorized treadmill) as well as short-term and long-term aerobic activity protocols. Finally, it is important to underline that beneficial effects are found when the exposure to aerobic activity begins in an early phase of the pathology, but also in a more advanced phase.
More specifically, the effects of voluntary aerobic activity have been studied both in AD lesional models and in AD transgenic models. Bernardo et al. [73] studied the effects of a long-term protocol of free access to running wheels in a rat streptozotocin-induced AD model. However, an amelioration of memory deficits was found only when such a protocol was combined with an involuntary exercise protocol. Beneficial effects were present even when the exposure occurred only after the lesion. A number of studies on transgenic AD models demonstrated that long-term voluntary aerobic exercise provokes beneficial effects in different domains of cognition when the exposure occurs in an early phase of the pathology [74–77]. Moreover, Zhang et al. [78] demonstrated that a 3-month exposure of 10-month-old APP/PS1 mice to running wheel free access was able to ameliorate spatial learning and memory deficits and object recognition.
An even larger number of recent studies have investigated the effects of exposure to involuntary aerobic activity in AD lesional and transgenic models. In Amyloid-β (Aβ)-induced AD models, long-term involuntary aerobic activity is able to rescue cognitive alterations when the exposure occurs both before and after the lesion [79, 80]. This is true also when the exposure is shorter, lasting only four weeks [81, 82]. A large number of recent studies have demonstrated the beneficial effects of exposure to long-term involuntary aerobic activity in rescuing cognitive alterations of transgenic models of AD. Moreover, such effects are present also when the exposure occurs in an advanced phase of the pathology [83, 93–95].
As for the neurobiological and structural rearrangements that support the described beneficial effects of land aerobic exercise in AD rodent models, a great number of processes appear to be involved, and the great abundance of positive results suggests that numerous others will be described. In particular, exercise-induced modifications at structural and molecular levels are described both in consequence of the exposure to voluntary [73–77, 96] and involuntary [79–82, 82–95] aerobic activity. The exposure to land aerobic activity induces a potentiation of neuronal morphology and networking, which is accompanied by the modulation of the expression of molecular factors that support brain adaptive plasticity in coping with neuroinflammation and neurodegeneration.
Details of the above-mentioned studies are reported in Table 2.
WATER ACTIVITIES AND COGNITION IN ALZHEIMER’S DISEASE PATIENTS AND ANIMAL MODELS
Human studies
Studies on a swimming-pool training in patients with dementia [97–99] explored the effect of aquatic exercises on cognition and behavior in patients with dementia. Participants received 12-weeks of aquatic training including exercises for strength, agility, flexibility, balance, and relaxation. After the training a significant reduction of behavioral disturbances was observed [97–99]. Details of the above-mentioned studies are reported in Table 3.
Studies on water activity effects on cognitive functions and neural substrates of Alzheimer’s disease patients
Animal studies
The little evidence available in rodent models of AD supports the beneficial effects of swimming aerobic activity, in line with what is described for land activities.
In the rat streptozotocin-induced AD model it has been demonstrated that the exposure to swimming protocols is able to rescue learning and memory disfunctions, when the exposure occurs both before and after damage [100, 101]. Also in this case, a number of brain plastic changes are found in association with the improvement in cognition [100, 101]. Interestingly, transgenerational beneficial effects of swimming have been demonstrated. Maternal swimming during pregnancy prevents cognitive impairment induced by Aβ in adult offspring rats [102]. In addition, evidence is available that in the rat D-(+)-galactose-induced AD model a swimming protocol implying involuntary exercise induces attenuation of cognitive alterations at a comparable level with voluntary exercise based on free access to running wheels [103]. Details of the above-mentioned studies are reported in Table 4.
Studies on water activity effects on cognitive functions and neural substrates of Alzheimer’s disease animal models
CONCLUSION
The aim of the present literature analysis was to gain a deeper insight on the potentially beneficial role of land and water aerobic activities on AD pathology, clarifying the specific effects on cognition and behavior, as well as on related neurobiological and structural processes. We analyzed both human and animal research. Such an analysis is intended as a continuation of our previous literature investigation on the effects of land and water activities in healthy adults and successfully aged, both human and animal subjects [14]. Human and animal findings supported the beneficial effect of aerobic exercise on memory and executive functions, and on structure and functional efficiency mainly of fronto-hippocampal circuitries, clarifying the molecular and supramolecular mechanisms.
Interestingly, even in the presence of AD pathology land and water aerobic exercises exert beneficial effects on cognition as documented in both human and animal studies. Remarkably, we found that aerobic activity per se improves cognition, independently from the specific kind of exercise performed. In particular, human studies emphasize the improvement of mnesic and executive functions after aerobic training protocols in patients with AD. These beneficial effects are supported by an increase of hippocampal volume and changes in functional connectivity in the networks related to cognition such as DMN. As for animal evidence, land and water aerobic activities alleviate the AD-related cognitive impairments, particularly in learning and memory domains. In human studies, the beneficial effect of aerobic exercise is observable both in the individual and group practices. However, no mention of long-lasting effects is reported in the considered studies, and this issue partially limits the impact of the observed findings. In addition, in the reported human studies a larger number of females than males was recruited without any control exerted on sex differences. Therefore, we hypothesize that the presence of a potential bias due to sex on efficacy of land and water activities can exist. On the other hand, in animal studies beneficial effects of aerobic exercise are separately reported in male and female samples. However, it is worth noting that ordinarily male animals are more frequently used in experiments, given the easer handling (since no estrus influence control is required). The analyzed animal studies do not directly compare male and female samples to investigate the possible presence of interaction between sex and aerobic exercise in the effects. Further studies are needed to address this important issue.
Also, the modulation of numerous biological processes and structural modifications are documented as summarizes in Fig. 1. The beneficial action of the aerobic exercise is demonstrated in the very large number of studies in animal models that contrasts with the limited number of studies on the effects of aerobic exercise in AD patients. As shown in our previous study [14], animal studies allow the deepening of specific aspects of aerobic exercise beneficial action. Indeed, beneficial effects are reported after the applying of both voluntary and involuntary, short-term and long-term aerobic activity protocols. Furthermore, beneficial effects are found in early and advanced phases of the pathology and even if the exposure starts in the older age (as particularly documented in animal models [83, 95]). Therefore, the key-role that aerobic activity per se has in ameliorating brain functioning can be maintained also in the presence of AD. But which is the mechanism linking aerobic exercise and brain functioning?
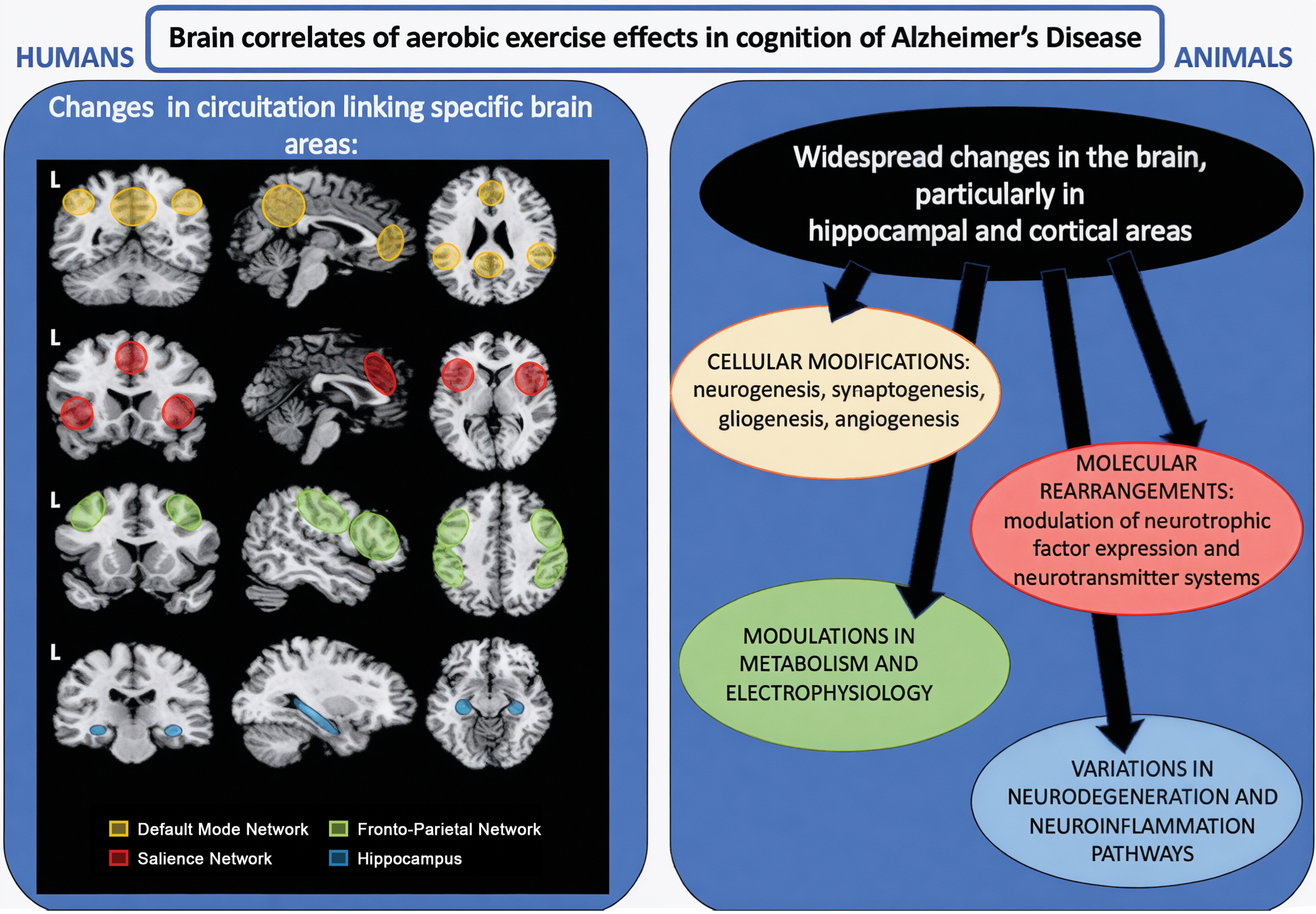
The figure summarizes the main brain correlates of effects of aerobic exercise in cognition of Alzheimer’s disease reported both by human (on the left) and animal (on the right) analyzed studies. For the only illustrative purpose the visualization of the human brain networks was achieved by using a manual drawing on the nodes on the template Ch2bet, available in MRIcron (https://www.nitrc.org/projects/mricron). L, Left. See text for further details.
Practicing aerobic exercise induces the secretion of molecular factors from body periphery, including the primary organs involved in physical activity, such as skeletal muscles and liver [104]. Briefly, skeletal muscle through its contraction activity involved in aerobic exercise induces the secretion of several “exercise-induced” molecular factors such as irisin, cathepsin B, CLU, and glycosylphosphatidylinositol-specific phospholipase D1 (GPLD1), which intrude in blood flow and reach the brain, by crossing the blood-brain barrier [105]. Such factors, when entered the brain, stimulate the expression of molecules (such as neurotrophic factors and, in particular, BDNF) that promote and support neuroplasticity, reduce neuroinflammation [106], and inhibit neurodegenerative processes (such as Aβ accumulation and neurofibrillary tangles formation) [104]. On the other hand, exercise stimulates the liver to secrete GPLD1 into the blood system. When entered the brain, such a specific phospholipase can inhibit Aβ accumulation [105]. In addition, it has been shown that aerobic exercise acts on the different phases of mitochondrial activity (also at brain level) by promoting development and maintaining the balancing of mitochondria, reduces oxidative stress derived by mitochondrial damage, and finally improves ATP production [105]. Moreover, it has been suggested that during exercise the muscles release the metabolite lactate that by crossing the blood-brain barrier is able to potentiate hippocampal BDNF expression with a potential beneficial effect on learning and memory [107]. Finally, the neuroprotective effects of physical activities have been also documented in other neurodegenerative conditions, such as Parkinson’s or Huntington’s diseases, via upregulation of synaptic signaling pathways, and in the frontotemporal dementia, by restoring the mitochondrial functions [108].
Through the above-described mechanisms, the aerobic exercise exerts beneficial actions that are largely demonstrated in animal studies. While on the one hand the presence of an astonish bulk of studies in animal models impresses, on the other hand the limited number of studies on the effects of aerobic exercise in AD patients is surprising. However, the scarceness of studies on land and water activities in AD population may be due to multifarious issues. Firstly, walking, running, and swimming activities cannot be considered only as motor performance, since they are highly cognitive-demanding and involve a complex ensemble of abilities. Indeed, they imply planning and execution of complex gestures, capacities of orientation, coordination, and rhythmizing of elaborate movements, balance, and anticipation functions, visuo-spatial monitoring of the environment, motor memory and imagery. It is noteworthy that in the case of fronto-parietal and cerebellar atrophy AD patients may show apraxia [109], namely impairment to execute complex motor sequences. Consequently, practicing land and water activities could be too challenging for AD patients [110]. In addition, AD patients have an augmented risk to fall, for the before cited reasons and also for the increased bone fragility, which is strictly related with Aβ deposition [111]. Finally, it is known that AD patients need a continuous supervision by the caregivers [112] and consequently can hardly autonomously attend land and water exercise activities.
In conclusion, it is ascertained that aerobic activities exert a protective effect on AD pathology (and also on other neurodegenerative disorders), as stated in the reserve framework [22, 39], but concretely the managing of AD patients to applying exercise protocols is difficult to carry out. Thus, it is fundamental that health policies specifically and amply focus on the importance of aerobic activity not only in successful aging, but also in age-related pathological conditions. On the other hand, specialized institutions should devote efforts and investments on the development of tailored training protocols to permit to the AD patients to safely benefit of aerobic exercise effects.
AUTHOR CONTRIBUTIONS
Francesca Gelfo (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Supervision; Writing – original draft; Writing – review & editing); Laura Petrosini (Supervision; Writing – review & editing); Laura Mandolesi (Supervision; Writing – review & editing); Eugenia Landolfo (Data curation); Giulia Caruso (Data curation); Francesca Balsamo (Data curation); Sabrina Bonarota (Data curation); Marco Bozzali (Supervision; Writing – review & editing); Carlo Caltagirone (Resources; Supervision; Writing – review & editing); Laura Serra (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Supervision; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
The Laboratories of the IRCCS Fondazione Santa Lucia are partially supported by Ministero della Salute (Italian Ministry of Health) (Fondo 5x1000 2022 cod: 5x2022MINSAL).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
LS and MB are Editorial Board Members of this journal but were not involved in the peer-review process of this article nor had access to any information regarding its peer-review.