
Abstract
Background:
The mechanisms through which acculturation influences the onset of cognitive impairment and dementia are not well understood, especially among older Hispanics.
Objective:
To investigate whether inflammation and psycho-behavioral factors mediate the relationship between acculturation and incident dementia among older Mexican Americans.
Methods:
We analyzed the Sacramento Area Latino Study on Aging (1998–2007, SALSA), a longitudinal study (N = 1,194) with 10 years of follow-up, and used g-computation for mediation analysis with pooled logistic regression to evaluate whether acculturation (assessed by the Revised Acculturation Rating Scale for Mexican Americans [ARSMA-II]) affected dementia or cognitive impairment but not dementia (CIND) through inflammation (i.e., interleukin 6 [IL-6], tumor necrosis factor-α (TNF-α), high-sensitivity C-reactive protein [hs-CRP]), smoking, alcohol consumption, and depressive symptoms. The potential mediators were assessed at baseline.
Results:
The 10-year average adjusted risk ratio (aRR) for the effect of high U.S. acculturation and dementia/CIND was 0.66, 95% CI (0.36, 1.30). The indirect effects were: IL-6 (aRR = 0.98, 95% CI (0.88, 1.05)); TNF-α (aRR:0.99, 95% CI (0.93, 1.05)); hs-CRP: (aRR = 1.21, 95% CI (0.84, 1.95)); current smoking: aRR = 0.97, 95% CI (0.84, 1.16); daily/weekly alcohol consumption (aRR = 1.00, 95% CI (0.96, 1.05)); and depressive symptom score (aRR = 1.03, 95% CI (0.95, 1.26)). Hs-CRP yielded a proportion mediated of -26%, suggesting that hs-CRP could suppress the potential effect of high U.S. acculturation. The other factors explored resulted in little to no mediation.
Conclusions:
The effect of acculturation on time to incident dementia/CIND varied over time. Our study suggests that inflammation could suppress the effect between high U.S. acculturation and dementia risk.
Keywords
INTRODUCTION
Over 6 million Americans are currently living with Alzheimer’s disease and related dementias (ADRD) and the number of ADRD cases is expected to rise to 13.8 million by 2050. 1 Cognitive impairment and dementia are among the costliest diseases in the U.S. and have negative impacts on daily activities, independent living and overall quality of life, imposing a substantial burden on individuals, families, and society. 2 In 2023, the health and long-term costs for people with ADRD were projected to reach $345 billion and it is expected to increase exponentially in an aging U.S. population. 2
Stress and psycho-behavioral factors such as smoking, alcohol consumption and depression are potential contributors to cognitive impairment and dementia.3 –6 In particular, experiences such as migrating to a foreign country and resettlement could lead to increased stress.7,8, 7,8 Still, the effects of migration may depend on if and when individuals assimilate into the host country’s culture. This phenomenon known as “acculturation” can be defined as the process through which an immigrant adapts and adopts the new culture’s attitudes, values, and behaviors. 9 This is especially relevant for Hispanics in the U.S., as they represent one of the largest U.S. immigrant groups. 10 Less acculturated immigrants (e.g., first-generation) have been found to exhibit healthier dietary practices than more acculturated immigrants— referred to as initial immigrant health “advantage.”11,12, 11,12 However, a recent study found that Hispanics with greater assimilation to the Anglo culture had better cognitive performance but similar dementia risk as those with less acculturation. 13
The mechanisms through which acculturation influences dementia and cognitive impairment onset are not well understood, but prior research suggests some possibilities. For example, greater acculturation and subsequent loss of social ties with one’s country of origin have been shown to be associated with a higher risk of depression, 14 cigarette smoking, 9 and inflammation, 15 as well as dementia risk.16 –20 Thus, it may be that the relationship between greater acculturation and dementia onset could be partially mediated by the effects of acculturation on mental health, behaviors, and inflammatory processes.
As mentioned, it has been shown that Hispanics with greater assimilation to the Anglo culture had better cognitive performance but similar dementia risk as those with less acculturation. This leads one to question why there is little to no effect of greater assimilation to the U.S. Anglo culture on dementia risk. We hypothesize that certain factors such as inflammation markers or psycho-behavioral factors could mediate and more specifically promote or suppress the effect of high U.S. acculturation on dementia risk.
The purpose of this study was to investigate whether 1) markers of inflammation and 2) psycho-behavioral factors (depressive symptoms, smoking, alcohol consumption) mediate the relationship between acculturation and incident dementia among older Mexican Americans.
METHODS
Study population and data sources
We analyzed data from the Sacramento Area Latino Study on Aging (SALSA), a prospective cohort study of residents of Mexican descent residing in the Sacramento Valley of California. There were 1,789 Mexican Americans 60 years or older who were recruited at baseline and enrolled from 1998 to 2007. Home visits occurred every 12–15 months for a maximum of 6 follow-ups. Interviews were conducted in English or Spanish and elicited information on social and lifestyle factors. In addition, clinical exams and cognitive testing were conducted. More information on SALSA can be found elsewhere. 21
We excluded study participants who did not have information on acculturation (n = 11), had a diagnosis of dementia or cognitively impaired but not dementia (CIND) at baseline, that is, with prevalent dementia or CIND at baseline (n = 171), had two or fewer follow-ups (n = 177), or had missing information on potential mediators and confounders (n = 236), leaving an analytical sample of 1,194 (Fig. 1). All participants provided informed consent, and the UCLA Institutional Review Board approved this study (IRB#20-000996).

Study cohort flow diagram.
Variables and measures
Acculturation. We used the Revised Acculturation Rating Scale for Mexican Americans (ARSMA-II). 22 The 30-item ARSMA-II includes a 17-item Anglo Orientation Scale (AOS) and a 13-item Mexican Orientation Scale (MOS). The AOS includes questions such as “How often do you speak English?”, “Do you enjoy speaking English?”, “Do you associate with Anglos?” and the MOS includes questions such as “How often do you speak Spanish?”, “Do you enjoy speaking Spanish?” and “Do you associate with Latinos?”. Each question used a 5-point polytomous response scale ranging from 0 (not at all) to 4 (always). As elsewhere, 13 we calculated the acculturation score by subtracting the average MOS score from the average AOS score for each participant. Individuals with a zero or positive score were classified as being highly acculturated (i.e., score≥0, high assimilation with the Anglo culture or high U.S. acculturation) and those with a negative score as being less acculturated (score < 0, low assimilation with the Anglo culture or low US-acculturation). Acculturation was assessed at baseline.
Time to incident dementia or cognitively impaired but not dementia (CIND). To evaluate participants’ cognitive function, two cognitive screenings were used: the Modified Mini-Mental State Exam (3MSE), a commonly used screening test of global cognitive function, and the Spanish and English Verbal Learning Test (SEVLT), a delayed recall trial which captures recall among older Latinos of Mexican ancestry. 23 Furthermore, if participants (1) had scores below the 20th percentile at baseline on the 3MSE or SEVLT, or (2) had decreased≥8 points on the 3MSE or≥3 points on the SEVLT between baseline and follow-up, they were referred for further neuropsychological testing and a standard neuropsychological examination. These cases were reviewed by a team of neurologists and neuropsychologists and given a diagnosis of “cognitively normal,” “cognitively impaired but not dementia (CIND),” or “dementia” according to standard diagnostic criteria. 24 Additional information on the procedures for dementia and CIND screening and classification can be found elsewhere. 24 In this study, we used time to incident dementia or CIND as our outcome of interest to capture both cognitive decline prior to dementia and dementia incidence and to improve statistical power.
Potential mediators. We examined 6 potential mediators, including the following markers of inflammation: interleukin 6 (IL-6), tumor necrosis factor-α (TNF-α), and high-sensitivity C-reactive protein (hs-CRP). These markers were chosen because of their associations with dementia in older Mexican Americans. 20 The biospecimens were collected from each participant and processed and stored at the Medical Center Clinical Laboratory at the University of California, Davis. In particular, IL-6 and TNF-α were determined using the Quantiglo Chemiluminescent Immunoassay (R& D Systems, Minneapolis, Minnesota) and CRP levels were measured with the CRP Ultra Wide Range Reagent Kit latex-enhanced immunoassay (Equal Diagnostics, Exton, Pennsylvania). 20 In addition to markers of inflammation, we investigated potential psycho-behavioral mediators of the effect of acculturation on dementia: depressive symptoms in the past week assessed using the Center for Epidemiologic Studies Depression Scale, tobacco use (current smoker versus never/former smoker) and alcohol use (daily or weekly drinking versus monthly or yearly). These potential mediators were collected at baseline.
Potential confounders. We used a directed acyclic diagram (DAG) (Fig. 2) 25 to help present the assumptions about the relationships between the exposure (acculturation), the potential mediators, the outcome (dementia/CIND), and other covariates. The following baseline covariates were then identified and adjusted for: age (continuous), sex (male versus female), marital status (married versus not married), nativity (U.S.-born versus non-U.S. born), major lifetime occupation (manual versus non-manual versus other), education (≥12 years versus < 12 years) and gross monthly household income (< $1,000; $1,000-$1,499; $1,500-$1,999; $2,000-$2,499;≥$2,500).
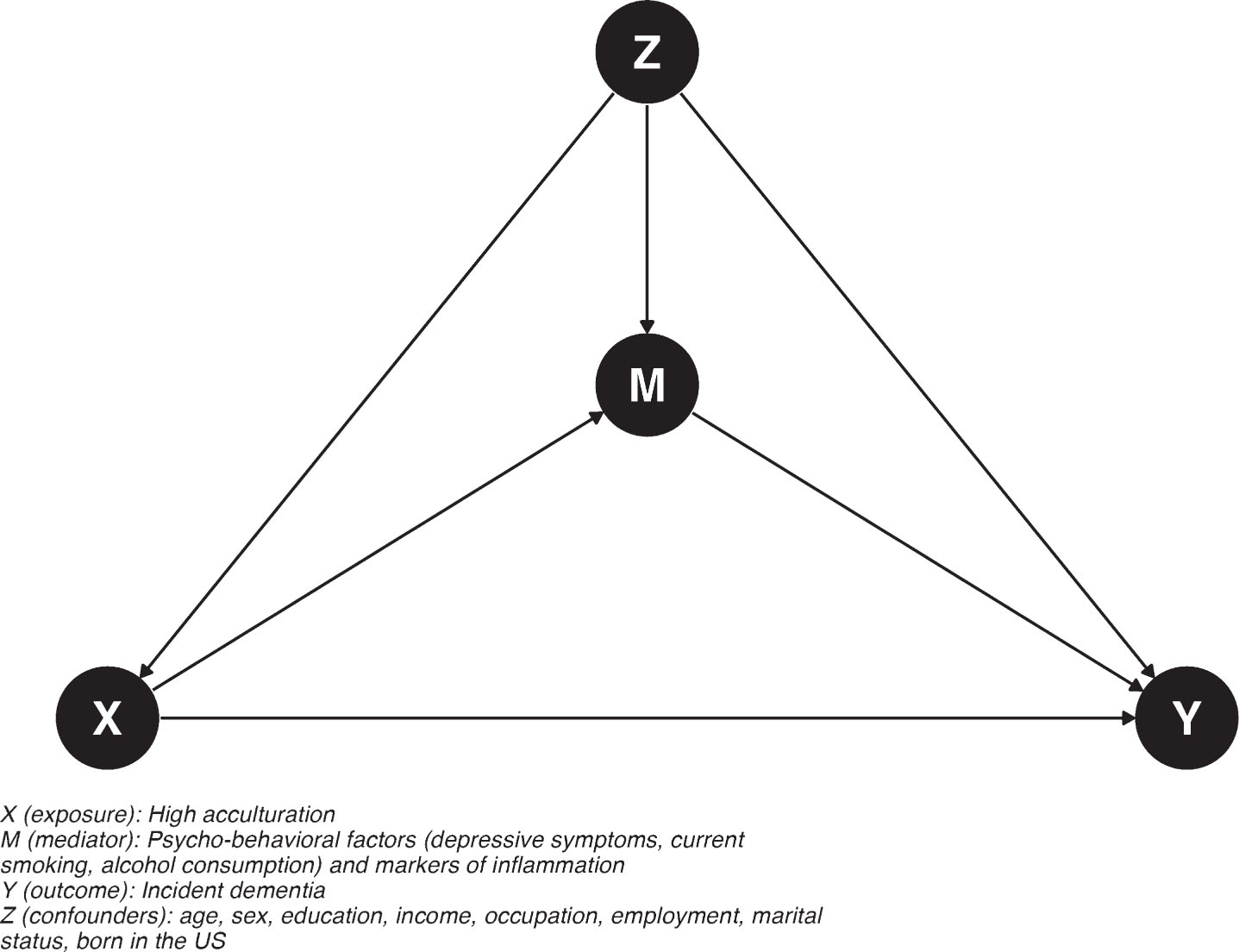
Hypothesized causal diagram of the assumed relationship between acculturation, potential mediators (e.g., markers of inflammation, psycho-behavioral factors) and dementia/cognitive impairment without dementia (CIND).
Statistical analysis
Causal mediation analysis. We conducted a causal mediation analysis26,27, 26,27 to estimate the natural indirect and direct effects28,29, 28,29 of acculturation on incident dementia/CIND via potential mediators (e.g., markers of inflammation, the indirect effect) and pathways not involving these mediators (i.e., the direct effect), respectively. More specifically, the (pure) natural direct effect (PDE) compares the potential outcomes of incident dementia under high versus low acculturation when setting the mediator to what it would attain under low acculturation. The (total) natural indirect effect (TIE) compares the potential outcomes of incident dementia under levels of the mediator attained in high versus low acculturation when setting the outcome to what it would attain under high acculturation. The total effect is the sum of both the PDE and TIE.
We used the g-computation algorithm, 30 a generalization of the standardization method for time-varying covariates, to decompose and estimate the natural effects of acculturation on incident dementia/CIND. We also calculated the proportion of the effect mediated by a given factor by dividing the indirect effect by the total effect for each exposure-mediator combination. For the relative scale, we divided the log of the indirect effect by the log of the total effect. The mediation analysis is described below and outlined in Wang and Arah. 26 Briefly, let us consider the exposure, acculturation (X), a potential mediator such as a marker of inflammation (M), the outcome, incident dementia/CIND (Y), and the potential covariates such as age and sex (Z). We undertook the following steps:
Step 1: Flexibly model the mediator variable on covariates, and outcome variable on covariates and mediator guided by the DAG (Fig. 2) to obtain relevant regression parameters needed for predicting the counterfactual quantities. This was done by:
Modeling the mediator (M) as a function of the exposure (X) and covariates (Z)
Modeling the outcome (Y) as a function of the exposure, the mediator and covariates including an interaction between the exposure and the mediator.
Step 2: Predict the potential mediator and outcome variables by:
Predicting the potential mediator M using the regression parameters (α) obtained above, the new simulated intervention variable doX (doX = 1, high acculturation, doX = 0, low acculturation), the potential mediator variable M
doX
(i.e., the potential outcome M, had doX been set to 1 or 0) and the baseline covariates Z.
Predicting the potential outcome
Step 3: Obtain the total effect (TE), total indirect effect (TIE) and pure direct effect (PDE) by:
Contrasting the potential outcome
Step 4: Obtain standard errors
Estimating standard errors and the 95% confidence interval by repeating the analysis (step 1–3) on 200 bootstrap samples.
To decompose effects using the g-computation algorithm, we made the following assumptions. We assumed no uncontrolled confounding of the expo-sure-mediator, mediator-outcome, and exposure-outcome relationships and no exposure-inducedmediator-outcome confounder. In addition, we assumed positivity 31 (common support), con-sistency 32 (treatment irrelevance), no interference 33 , no model form misspecification, and no selection bias, or measurement error.
Causal survival analysis. To model time to dementia/CIND, we implemented a causal survival analysis approach34,35, 34,35 whereby time is modeled explicitly. This method does not require the proportional hazard assumption.34,35, 34,35 To do so, we first fitted a pooled logistic regression of incident dementia/CIND on exposure and covariates and included an interaction term between the exposure, the mediator, and a quadratic function of time. Doing so allowed us to properly model time and estimate standardized risk ratio and risk difference for each time period.34,35, 34,35 Second, we predicted the survival probabilities (i.e., conditional probability of remaining free of dementia/CIND given acculturation, baseline covariates and time of follow-up) at each person-time observation under low and high acculturation (i.e., counterfactual predictions). Third, to estimate the average survival and risk at each discrete time, we used the Kaplan-Meier product formula. This allowed us to obtain adjusted survival probability curves and estimate the discrete-time standardized causal effect on the risk ratio and risk difference scales.34,35, 34,35 Fourth, standard errors and confidence interval were obtained via bootstrap.
All statistical analyses were performed in R, version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Baseline characteristics
Table 1 displays the baseline mean and proportion for each variable in the analytical dataset, overall and by acculturation level. The mean age of participants was 70 years and was similar in both groups. The median follow-up time for dementia/CIND was about 7 years. Ninety percent of those with a high U.S. acculturation score were born in the U.S. compared to 29% in the low-acculturation group. Highly acculturated individuals had more years of education, and a higher monthly household income compared to those with low-acculturation score. The means for the markers of inflammation, hs-CRP, Il-6 and TNF-α were similar in both groups. The proportion of those who consume alcohol daily or weekly (27% versus 16%), currently smoke (9% versus 11%) and the mean depressive symptoms (7 versus 11) differed by the level of U.S. acculturation(high versus low).
Baseline characteristics of study participants overall and according to acculturation status, Sacramento Area Latina study on Aging (SALSA), 1998–2007, N = 1,194
CIND, Cognitively Impaired but not Dementia; SD, Standard deviation.
Total effect between high acculturation and time-to-dementia/CIND
The plot of the standardized adjusted survival curves suggests that highly U.S. acculturated participants had lower risk of dementia/CIND compared to those who were less acculturated, however, confidence intervals of the survival curves overlapped (Fig. 3). The 10-year average cumulative incidence of dementia/CIND among individuals with High U.S. acculturation was 0.66 (adjusted risk ratio, aRR = 0.66 95% CI (0.36, 1.30) times that among those with low U.S. acculturation adjusting for potential confounders (Table 2). This effect is mostly compatible with a protective effect of acculturation; however, given the imprecision of the estimates, one cannot rule out a null or detrimental effect of high U.S. acculturation on dementia/CIND risk. In addition, the discrete-time risk ratio showed that the effect of high acculturation on time to incident dementia/CIND varied with time after the start of the study with highly U.S. acculturated participants having lower risk of dementia/CIND compared to those who were less acculturated between 40 (3.3 years) to 80 (6.7 years) months after the start of the study(Fig. 4).
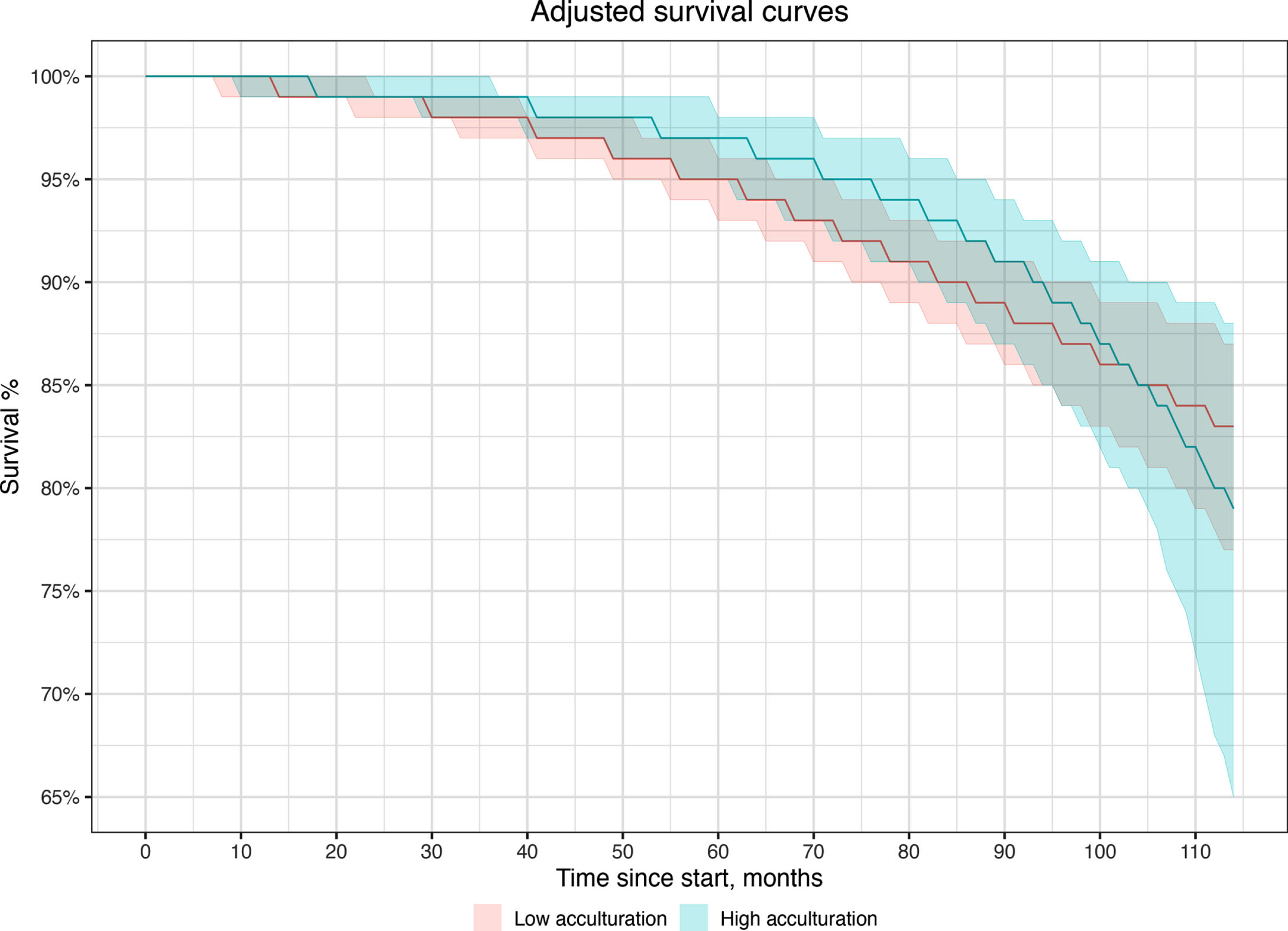
Adjusted survival curves (probability of being dementia/CIND-free) over the duration of the study among older Mexican Americans by acculturation status.
Total effect of acculturation on incident dementia/CIND in the Sacramento Area Latina study on Aging (SALSA, 1998–2007), N = 1,194
Model adjusted for age (in years), sex (male versus female), education (in years), income (< $1,000, $1,000–$1,499 $1,500–$1,999, $2,000–$2,499,≥$2,500), major lifetime occupation (nonmanual, manual, other), currently employed at a paying job (yes versus no), married (yes versus no), born in the U.S. (yes versus no).
Estimates of the direct and indirect Effects of Acculturation on Incident Dementia/CIND through potential mediators in the Sacramento Area Latina study on Aging (SALSA, 1998–2007), N = 1,194
Model adjusted for age (in years), sex (male versus female), education (in years), income (< $1,000, $1,000–$1,499 $1,500–$1,999, $2,000–$2,499, ≥$2,500), major lifetime occupation (nonmanual, manual, other), currently employed at a paying job (yes versus no), married (yes versus no), born in the U.S. (yes versus no). The proportion mediated was calculated as log(indirect effect)/log(total effect) where log(total effect) = log(direct effect) + log(indirect effect). Negative estimates are due to indirect and total effect be in opposite direction.
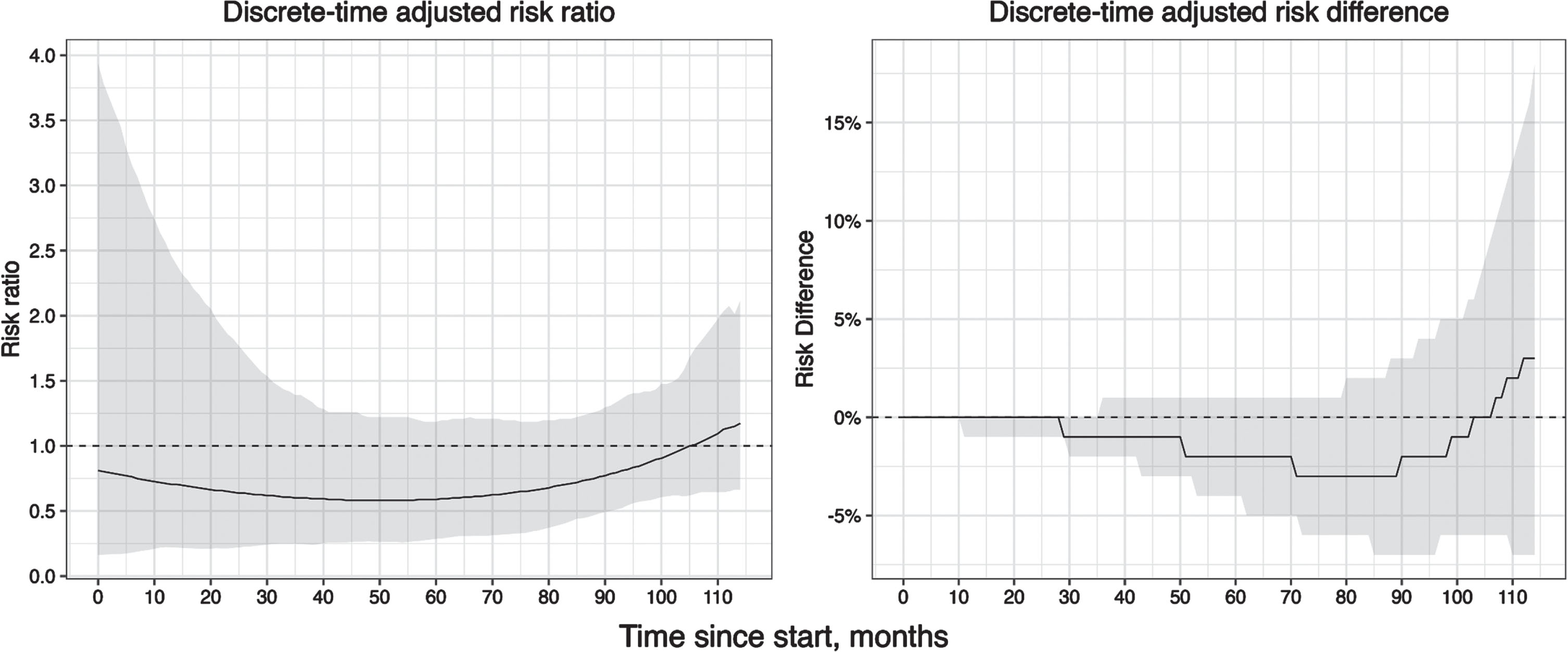
Adjusted risk ratio and risk difference for the effect of high U.S. acculturation on incident dementia/CIND.
Indirect effects via potential mediators and proportion mediated
The estimated indirect effects of makers of inflammation and psycho-behavioral factors in terms of adjusted risk ratio (aRR) were as follows: Interleukin 6 (aRR = 0.98, 95% CI (0.88, 1.05)); TNF-α: aRR: 0.99, 95% CI (0.93, 1.05)); high-sensitivity C-Reactive Protein (hs-CRP): aRR = 1.21, 95% CI (0.84, 1.95); current smoking: aRR = 0.97, 95% CI (0.84, 1.16); daily or weekly alcohol consumption: aRR = 1.00, 95% CI (0.96, 1.05); and presence of depressive symptoms: aRR = 1.03, 95% CI (0.95, 1.26).
In particular, the effect of high U.S. acculturation on dementia/CIND risk was mediated by hs-CRP: (aRR = 1.21, 95% CI (0.84, 1.95)), though estimates were imprecise. In other words, the risk of dementia/CIND if all participants had a high U.S. acculturation and their hs-CRP level were as they would be when participants have a high U.S. acculturation, would be aRR = 1.21, 95% CI (0.84, 1.95), times the risk of dementia/CIND if all participants had a high U.S. acculturation and their hs-CRP level were as they would be when participants have a low U.S. acculturation. This analysis allowed for the possibility of an interaction between high U.S. acculturation and hs-CRP on dementia/CIND risk (that is, the effect of high U.S. acculturation on dementia risk/CIND could vary by levels of hs-CRP) and assuming no bias and no model form misspecification. The corresponding proportion mediated was –26%, suggesting that the potential effect of high U.S. acculturation could be counteracted or suppressed by hs-CRP.
The other potential mediators explored in this study resulted in little to no mediation. In addition, while the effect of high U.S. acculturation on incident dementia not through the inflammatory marker hs-CRP (i.e., the direct effect) did not include the null (aRR = 0.40, 95% CI (0.11, 0.90)), the corresponding indirect effect through the inflammatory marker hs-CRP included the null (Table 2).
DISCUSSION
This study investigated the role of markers of inflammation and psycho-behavioral factors such as smoking, alcohol consumption and depressive symptoms as potential mediators in the relationship between acculturation and time to incident dementia/CIND among older Mexican Americans. More specifically, we tested whether certain factors such as inflammation markers or psycho-behavioral factors could mediate and more specifically promote or suppress the effect of high U.S. acculturation on dementia/CIND risk. We found that the effect of high U.S. acculturation on incident dementia/CIND varied with time and that there was some mediation through the inflammatory biomarker, high-sensitivity C-reactive Protein (although the estimates were imprecise) but not through other markers of inflammation and psycho-behavioral factors explored. In addition, our study suggests that hs-CRP could be acting as a suppressor of the total effect of high U.S. acculturation on dementia/CIND risk.
This study is important as it investigated whether markers of inflammation and psycho-behavioral factors mediated the association of high U.S. acculturation and time to incident dementia/CIND in older Mexican Americans. A study by Martinez-Miller et al first showed that high U.S. acculturation was positively associated with better cognitive performance but similar dementia/CIND risk as those with low-US acculturation among older Mexican Americans. 13 This suggested that there was potentially a moderate and slow effect of U.S. acculturation on cognition that was not strong enough to affect dementia/CIND risk. Alternatively, heterogeneity of effects in opposite direction could together result in null total effect, meriting further investigation.36 –38 Similarly, in a mediation context, null total effects could occur when the direct and indirect effect are in opposite direction as is the case for one of the markers of inflammation in our study, hs-CRP, reinforcing the importance of decomposition analysis to understand possible mechanisms even in the presence of a null total effect. Our study differs from Martinez-Miller 13 in that we investigated potential mechanisms through mediation analysis and applied a pooled logistic regression to avoid making the proportional hazard assumption. In addition, we estimated the dynamic and discrete-time effect of high U.S. acculturation on time to incident/CIND.
The current study showed that the effect of high U.S. acculturation varies with passage of time, with highly U.S. acculturated participants having lower risk of dementia/CIND compared to those who were less acculturated between 3 and 7 years after the start of the study, although there was some uncertainty in the estimates. The change in effect could be related to the acculturation process and subsequent behavior change. In particular, it has been shown that less acculturated immigrants tended to exhibit healthier dietary practices than more acculturated immigrants. 9 This could be because Hispanic immigrants with low acculturation (i.e. less assimilation to the Anglo culture) who are generally represented by first-generation immigrants may still benefit from the initial immigrant health “advantage”.11,12, 11,12 In contrast, high U.S. acculturation and loss of social ties over time with country of origin among immigrants have been found to be associated with a higher risk of depression, 14 cigarette smoking 9 and inflammation, 15 which have also been found to be associated with dementia risk.16 –20
Our study also showed that there was some mediation through the inflammatory biomarker, C-reactive Protein (although the estimates were imprecise) but not through other markers of inflammation and psycho-behavioral factors explored in the current study. First, it is important to note that even when the total effect nears the null as is the case in this study, it does not preclude the presence of an indirect effect. 39 This can occur, for instance, when the direct and indirect effect are close in magnitude but in opposite direction resulting in a null or near null effect by simple cancellation. In fact, in a recent paper (Nianogo RA. On Revisiting Null Effects in the Presence of Heterogeneity or Mediation: A Simulation-Based Illustration. Unpublished), we have shown that the total effect could near the null in the presence of heterogeneity or mediation even within a well-powered study where bias is absent, highlighting that the presence of a null total effect should not preclude the investigation of subgroup or path-specific (direct and indirect) effects. This phenomenon has been termed “inconsistent mediation” 40 and was first described by MacKinnon et al to highlight that the mediator can act as a suppressor factor. In fact, high-US acculturation may increase inflammation 15 (positive effect) which in turn may increase dementia risk 20 (positive effect) leading to an overall positive indirect effect while there was an overall total negative effect of high U.S. acculturation on cognitive performance 13 and to some extent dementia risk (although the estimates were imprecise).
Inflammation is implicated in the pathophysiology of several chronic diseases including dementia, 20 heart diseases and cancer. 41 Additionally, several stress-related experiences including social stress, and loss of social ties 15 could lead to increased inflammation. The finding that high-sensitivity C-reactive Protein, a marker of inflammation partially mediated the effect of high U.S. acculturation on dementia risk suggests that it may play a suppressing role of the protective effect of high U.S. acculturation. Regardless, other factors not explored in the current study could also mediate the relationship between high U.S. acculturation and dementia risk. Further studies should explore other mechanisms such as poor social support as potential mediators between high U.S. acculturation and dementia risk or cognitive performance.
In our study, we illustrated the implementation of causal mediation analysis within a causal survival analysis framework. As alluded earlier, the proportional hazard assumption is rarely met and as such allowing for the effect to vary over time is essential. This is what the causal survival analysis does by flexibly modeling time parametrically (and adding an interaction between time and the exposure of interest) and estimating the discrete-time risk ratio and risk differences— measures that are easier to understand and communicate compared to hazard ratios.35,42,43 , 35,42,43
Our study is not without limitations. First, our mediators (markers of inflammation and psycho-behavioral factors) were assessed at baseline and not at follow-up, assuming that the baseline and follow-up mediators would remain approximately constant. Future studies with longer follow-up data should confirm these findings. Second, we did not explore potential mediators such as stress3,4, 3,4 and social support 15 which are known to play an important role in dementia risk. Future longitudinal studies should explore other mechanisms in relation to dementia risk but also cognitive performance. Third, our study used a crude measure of acculturation (high U.S. acculturation [high assimilation] versus low U.S. acculturation [low assimilation]) as opposed to a more nuanced measure of acculturation. In fact, according to Berry’s model, 44 acculturation can be divided into four categories: assimilation (individuals adopt the host culture over their original culture), separation (individuals reject the host culture in favor of their original culture), integration (individuals adopt the host culture while maintaining their original culture), and marginalization (individuals reject both the host and their original cultures). Studies have shown that, in general, integration is associated with better mental health outcomes, while marginalization is associated with poorer mental outcomes. 45 These findings suggest that our two-level categorization could have obscured more nuanced effects of the various types of acculturation on dementia risk. Future studies should explore the relationship between these four types of acculturation and dementia risk. Fourth, while place of birth could be seen as a proxy for acculturation, we included it as an adjustment variable in analysis for the following reasons: (i), acculturation is a highly heterogeneous process, even in U.S.-born participants. As noted in the graph (Supplementary Figure 1) there is a gradient of acculturation even among U.S.-born individuals. One reason for this is that second-generation individuals (those born in the U.S. but with parents born in Mexico, for instance) represent a heterogenous group and may have various levels of acculturation depending on several factors, including social networks, socioeconomic status, etc., (ii) given the likely possibility that place of birth could affect both acculturation (the exposure) and dementia risk (the outcome), we considered place of birth as a potential confounder and adjusted for it, as done elsewhere 13 , (iii) since almost half of the sample was born in the U.S., excluding all of them will limit the sample size (size = 625) and further reducepower.
Fifth, the prevalence of the outcome in our study was relatively low, potentially playing a part in the imprecision of our estimates. Additionally, we focused this study on dementia risk to understand how certain risk factors could partially explain the acculturation difference in dementia risk, as dementia represents the later stages in the cognitive decline process. Further studies should investigate whether these findings would be replicated with alternative outcomes such as continuous cognition measures. Sixth, our findings may not generalize to all Hispanic Americans in the U.S. as our study participants were of Mexican descent, tended to be older, and living in low-income households. However, acculturation patterns and the Hispanic paradox 11 could reasonably be thought to occur similarly across Hispanic subgroups in the U.S.
Conclusion
Our study found that the effect of acculturation on incident dementia/CIND varies over time and that there was some mediation through the inflammatory biomarker, high-sensitivity C-reactive Protein but not through other markers of inflammation and psycho-behavioral factors such as smoking, high alcohol consumption and depressive symptoms. The study suggest that inflammation could play a suppressing role on the effect between high U.S. acculturation and dementia/CIND risk. Further research should explore other mechanisms such as poor social support and should be conducted in larger and longer-term studies.
AUTHOR CONTRIBUTIONS
Roch Nianogo (Conceptualization; Formal analysis; Funding acquisition; Methodology; Software; Writing – original draft; Writing – review & editing); Ron Hays (Conceptualization; Methodology; Supervision; Writing – review & editing); Yufan Gong (Data curation; Software; Writing – review & editing); Yu Yu (Data curation; Writing – review & editing); Beate Ritz (Conceptualization; Supervision; Writing – review & editing); O. Kenrik Duru (Conceptualization; Funding acquisition; Supervision; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
An oral presentation of an earlier version of this manuscript was presented at the RCMAR Annual meeting, March 29 – April 2, 2021.
FUNDING
This work was supported by the University of California, Los Angeles (UCLA), Resource Centers for Minority Aging Research Center for Health Improvement of Minority Elderly (RCMAR/CHIME) under NIH/NIA Grant P30-AG021684, and from the UCLA Clinical and Translational Science Institute (CTSI) under NIH/NCATS Grant Number UL1TR001881. RN is also currently partly supported by the National Institute on Minority Health and Health Disparities [1K01MD014163-01A1], National Institutes of Health, Bethesda, MD. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health (NIH). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The corresponding author had full access to all the data in the study and takes final responsibility for the paper.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.