
Abstract
Extracts made from plants are complex mixtures of substances with varying compositions depending on the plant material and method of manufacture. This complexity makes it difficult for scientists and clinicians to interpret findings from pharmacological and clinical research. We performed a narrative review summarizing information on ginkgo biloba leaf extract, its composition, pharmacological data and clinical evidence supporting its administration for the treatment of Alzheimer’s disease (AD). Medicinal products containing ginkgo biloba leaf extract which are manufactured in compliance with the requirements of the European Pharmacopoeia are approved as medicinal products for the treatment of dementia and related conditions by drug regulatory agencies in Europe, Asia and South America. As multicomponent mixtures, they may affect various targets in the pathogenesis of AD, the most common form of dementia. Pharmacodynamic studies demonstrate the effects of EGb 761 and individual constituents on various pathophysiological features of experimentally induced cognitive impairment and neurodegeneration that could contribute to its clinical efficacy. The safety and efficacy in the treatment of AD and cognitive decline has been studied in randomized, placebo-controlled clinical trials. Most of the studies that investigate the effects of ginkgo biloba extract (GbE) used the special extract EGb 761, which makes it the best-researched plant preparation worldwide. It is therefore the only herbal alternative to standard-of-care anti-dementia drugs. However, the mechanism of action has not been fully elucidated yet, and the clinical studies in AD show heterogeneity.
INTRODUCTION
Ginkgo biloba L. is a gymnosperm dioecious tree native to Asia, e.g., China, Japan, and Korea. Writings about Ginkgo biloba L. two-lobed leaves as a medicinal raw material were already documented in the 15th and 16th century. The first official mention was in the Chinese Pharmacopoeia in 1977 [1]. Nowadays, the pharmaceutical industry mainly collects ginkgo leaves from farms in China, France, and the USA; cultivated ginkgo trees are pruned into bush forms approximately 1.5 meters high for easy harvesting [1] (Fig. 1).
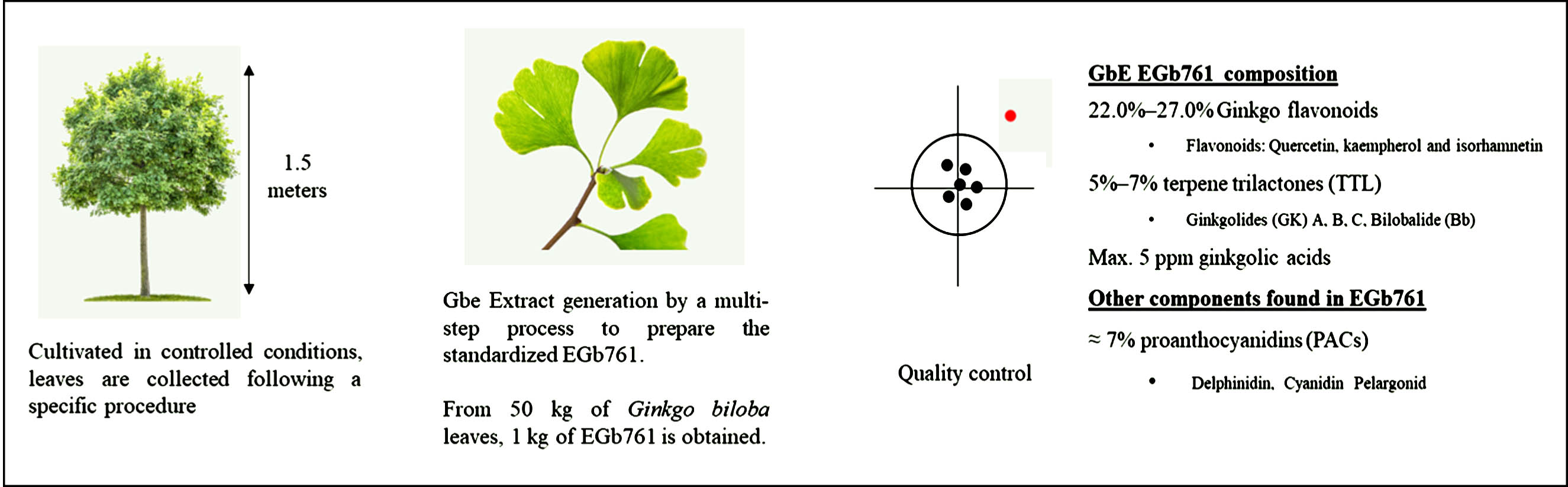
From the Ginkgo biloba L. tree to EGb 761.
The use of ginkgo biloba leaf extract (GbE) for the treatment of cardiovascular and cerebrovascular disorders is included in the Chinese Pharmacopeia, whereas in other parts of the world it is given for dementia and related conditions. Commercially, the proprietary extract EGb 761 was first introduced in 1965 by the pharmaceutical company Dr. Willmar Schwabe GmbH & Co. KG, Germany. Today medicinal products with EGb 761 as active substance have gained marketing authorizations by drug regulatory agencies in Europe, Asia, and South America [1]. In 2015 the Committee on Herbal Medicinal Products of the European Medicines Agency approved the well-established use of GbE for the treatment of age-related cognitive impairment. EGb 761 is administered orally, and standard dosages used in most studies and recommended by the manufacturer range from 120 mg/day to 240 mg/day [2]. The maximum recommended dose of 240 mg/daily is safe and well-tolerated. Even though EGb 761 has extensively been used for the treatment of cognitive decline, the underlying mechanisms of action have not yet been fully elucidated.
Alzheimer’s disease (AD) is an irreversible, progressive neurodegenerative disorder. Progressive changes in cognition (i.e., memory, language, or thinking) may be followed by behavioral and neuropsychiatric symptoms and, finally, the need for assistance in performing common daily life activities. AD and related dementia afflict 50 million people worldwide, and these numbers are projected to triple by 2050 [3]. Pathophysiologically, AD is defined by two main hallmarks: abnormal protein deposits of extracellular amyloid-β (Aβ) peptides, and neurofibrillary tangles (comprising different abnormal hyperphosphorylated tau species) [4]. However, AD is currently considered to be a multifactorial disorder which includes the presence of senile plaques, neurofibrillary tangles, neuroinflammation, malfunctioning of the cholinergic and other neurotransmitter systems, the presence of increased oxidative stress and dysfunctional gut microbiota [5].
Despite its limited and transient efficacy, the current standard of care for AD includes the use of acetylcholinesterase inhibitors (AChEI) such as donepezil, rivastigmine, and galantamine and the N-methyl-D-aspartic acid receptor antagonist memantine. AChEI and memantine are categorized as symptomatic treatments because they do not significantly change the progression of the disease [6]. Lecanemab and aducanumab are monoclonal antibodies against Aβ representing a new AD treatment category. They have been shown to reduce the amyloid burden and thereby target the fundamental pathogenetic mechanisms of the disease. Since they induce long-term changes in the clinical progression of AD they are categorized as disease-modifying treatments [7]. The special Ginkgo biloba extract has been shown to be effective in the treatment of AD in clinical trials [8] as well as in meta-analyses [9, 10].
The medicinal administration of herbal preparations is the subject of debate, since it ranges from medicinal products regulated by pharmaceutical legislation to unregulated dietary supplements. The latter have an insufficiently standardized chemical composition and usually lack a sound scientific basis for effectiveness and safety. Therefore, physicians may generally refrain from prescribing or recommending herbal products. The clinical use of GbEs which are manufactured according to pharmaceutical standards may not be well known to scientists and clinicians, although findings from numerous clinical trials, systematic reviews and meta-analyses, have been published in peer-reviewed journals, especially for the special ginkgo leaf extract EGb 761. The objective of this narrative review is to provide a comprehensive overview of the pharmacodynamic effects and the plant substances that shed light on its mechanism of action.
COMPOSITION
GbE as an active pharmaceutical ingredient of authorized medicinal products is manufactured according to the monograph of the European Pharmacopeia. The quantified plant extract contains 22.0%–27.0% ginkgo flavonoids such as quercetin, kaempferol, and isorhamnetin, 5%–7% terpene lactones consisting of 2.8%–3.4% ginkgolides A, B, C, and 2.6%–3.2% bilobalide (Fig. 1). Their chemical formulas and structures are shown in Fig. 2. The content of ginkgolic acids, which are potential allergens, is limited to max. 5 ppm [11]. Recently, proanthocyanidins (PACs) have gained more attention, since this class of compounds, i.e., oligomers containing delphinidin, cyanidin and pelargonidin, represent approximately 7% of EGb 761 [12] (Fig. 1). The composition in its entirety determines the pharmacokinetic and pharmacodynamic characteristics, which in turn determines clinical efficacy and safety.
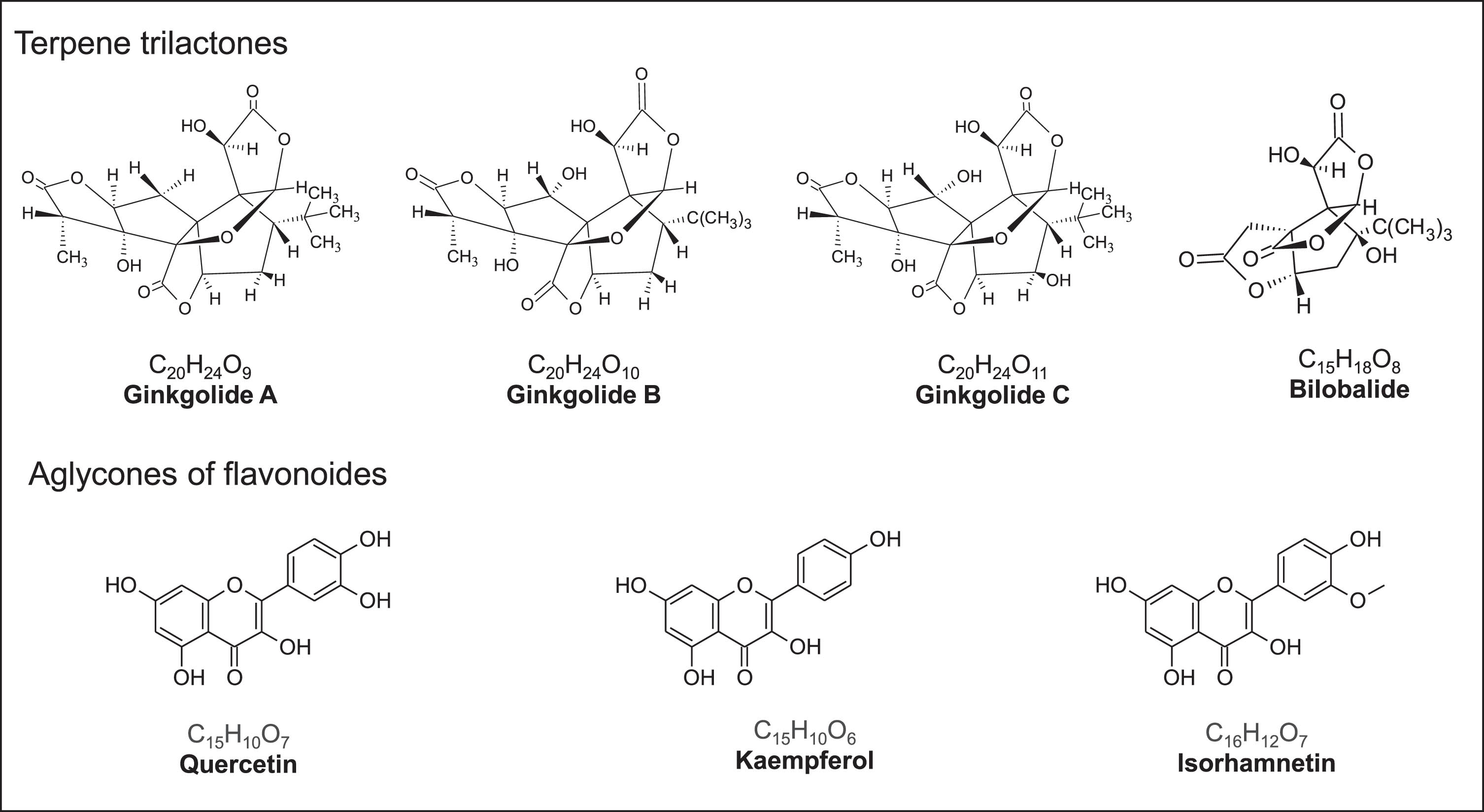
Chemical and structure formulas of ginkgolides and aglycones of flavonoids of Ginkgo biloba leaf extract.
PHARMACODYNAMIC EFFECTS OF EGB 761 AND PLANT CONSTITUENTS REGARDING AD TREATMENT
GbE is a multicomponent mixture of individual constituents and therefore does not have one sole target of pharmacodynamic activity. Most pharmacological studies were conducted with EGb 761. Flavone glycosides (kaempferol, quercetin, etc.) and terpene lactones (ginkgolide A, B, C, bilobalide) are major known active substances; PACs further could potentially contribute to its efficacy (Fig. 1). After oral administration of EGb 761 or ginkgolides these components are available in plasma of humans and animals and these substances penetrate the blood– brain barrier. Studies detected ginkgolide A and B and bilobalide as well as ginkgo flavonoids in the CNS of rats in concentrations sufficient to induce pharmacological effects [11, 13]. Table 1 provides an overview of the main pharmacodynamic effects of the whole extract or plant substances regarding AD pathology. Dosages of about 70 mg/kg daily in mice result in plasma levels equal to the ones in humans taking recommended dosages of 240 mg daily [14]; dosages of up to 100 mg/kg/daily in rats are also human equivalent.
Multifactorial pathology of AD versus the mechanisms of action of EGb 761
Increasing neuroplasticity
Stimulation of neuro- and synaptogenesis
Neurodegeneration in AD is accompanied by a slowing down of new cell formation in the hippocampus, decrease of the number of neurons and synapses as well as a decrease in the capability of long-term potentiation. This results in a decline in neuroplasticity in this part of the brain, which may be accelerated dramatically by protein deposits in the cells.
EGb 761 was given to mice overexpressing human amyloid precursor protein (AβPP) at a concentration of 0.6% in the diet, amounting to an average dosage of 69 mg/kg/daily. The plasma concentration of the plant substances was in the same range as in humans taking dosages of 240 mg EGb 761 daily. After 5 months, EGb 761 attenuated the loss of synaptic structural protein and significantly improved the cognitive function of the animals [15]. These findings were confirmed in a model for memory deficits in AD where scopolamine was administered to rats to induce cognitive impairment. EGb 761 at a dosage of 400 mg/kg/day for 14 days attenuated synaptic damage in hippocampal neurons and improved learning and memory deficits in the animals [16]. Given at a dosage of 50 mg/kg/day, EGb 761 enhanced the proliferation of neuronal stem cells in the brain of rats with vascular dementia and significantly improved learning and memory [17].
EGb 761 and its constituents enhance the plasticity as well as the sprouting, growth, and regeneration of axons; at the same time, they protect synapses from damage caused by Aβ and other harmful factors [18]. Bilobalide and quercetin enhanced neurogenesis and synaptogenesis through a common signaling pathway mediated by phosphorylation of cyclic-AMP response element binding protein (CREB) in another mouse model of AD [19]. EGb treatment (at 250 mg, 500 or 1000 mg/kg daily) before acquisition of object-recognition memory promoted the persistence of long-term memory by an upregulation of the brain-derived neurotrophic factor (BDNF) in the hippocampus of male rats [20].
Protein degradation and aggregation
Tau proteins are soluble substances which are abundant in the neurons of the central nervous system and maintain the stability of axons. AD pathology is associated with hyperphosphorylated tau proteins (p-tau) becoming insoluble and forming intracellular tangles. EGb 761 was given to human tau mutant-transgenic mice (P301S) overexpressing human AβPP at a concentration of 0.6% in the diet, which amounted to an average dosage of 69 mg/kg/daily, for 5 months to investigate its effect on cerebral p-tau levels [14]. EGb 761 inhibited the activity of p38-MAPK and GSK-3β as the two key enzymes generating p-tau. Treatment with ginkgolide A or bilobalide (as well as flavonoids to a lesser extent) significantly increased autophagy in cultured cells modelling human neurogenesis (SH-SY5Y cells) through an increased expression of autophagy-related molecules, such as ATG5 and beclin1. In the process, EGb 761 decreased the amount of p-tau, brain microglia shifted to an anti-inflammatory state, synapse loss was reduced, and cognitive function significantly improved [14]. The function of bilobalide (4 mg/kg daily, 8 mg/kg daily) given with food for 6 months was investigated in transgenic mice expressing human AβPP and PS1 mutant proteins. The compound promoted autophagy and improved learning and memorycapabilities [21].
Pathologically, AD is further characterized by extracellular amyloid protein aggregations containing insoluble Aβ in the neuritic plaques which impair synapses and affect neuronal activities. Aβ further triggers the release of neurotoxic mediators from microglia cells causing neuroinflammation. EGb 761 inhibited the formation of amyloid fibrils, attenuated amyloid neurotoxicity and inhibited caspase-3 activity, an enzyme which is involved in the formation of Aβ, in a neuroblastoma cell line (N2A) expressing two Aβ mutations [22]. It was further demonstrated in vitro that pre-treatment of cultured cortical neurons with ginkgolide A and B protected synapses from damage by Aβ toxicity [23]. In transgenic mice for AβPP, treatment with EGb 761 for 5 months reduced Aβ plaque formation, attenuated synapse loss and inhibited inflammatory microglia activation in the brain [15].
Increase of neurotransmission
EGb 761 as well as its flavonoids and ginkgolides were shown to affect the dopaminergic [24] and the cholinergic system as well as the neurotransmitters noradrenaline or serotonin [25]. The treatment of rats for 2 weeks with EGb 761 (100 mg/kg or 300 mg/kg daily p.o.) or ginkgo flavonoids for 14 days resulted in increased dopamine and acetylcholine levels in the prefrontal cortex [25].
A 14-day treatment of mice with 100 mg/kg/day EGb 761 inhibited the norepinephrine (NE) uptake in the synapses which mediates synaptic dopamine clearance of the prefrontal cortex. These findings may explain the enhancement of dopaminergic neurotransmission by EGb 761, resulting in improved cognition and attention [26].
Bilobalide has neuroprotective properties, and a potential mechanism of action could be the reduction in excitatory amino-acid neurotransmitter release such as glutamate (Glu) and aspartate (Asp) from neuronal tissue [27]. Bilobalide also increased γ-amino butyric acid (GABA) concentration and glutamic acid decarboxylase activity in mouse brains.
Rats with scopolamine-induced cognitive impairment were treated with EGb 761 (8.27 mg/kg thrice daily, equivalent to 80 mg/60 mg person three times a day) and donepezil. Cognitive function significantly improved, the animals presented increased brain levels of superoxide dismutase (SOD) and lower brain levels of ACh than compared with EGb761 or donepezil treatments alone [28].
Enhancement of mitochondrial function and radical scavenging
Improvement of mitochondrial function
A mitochondrial cascade hypothesis was developed for the pathogenesis of late-onset, sporadic AD where oxidative damage to mitochondria plays a central role [29]. First, the production of reactive oxygen species (ROS) causes accumulating mitochondrial damage. Oxidative mitochondrial biomolecules and protein damage again amplify ROS production. This triggers a cellular response by generating Aβ, apoptosis and tau phosphorylation, and tangle formation [29].
Together with oxidative stress, decreased mitochondrial function plays a major role in the development of AD. Overexpression of hyperphosphorylated and aggregated tau protein leads to mitochondrial dysfunction, which in turn causes tau pathology and neuronal damage [30]. Aβ generates free radicals which may cause oxidative damage to mitochondria [31]. EGb 761 improves the function and energy metabolism of the mitochondria, mainly driven by the ginkgolides. The extract showed antioxidant activity and protection of mitochondrial function against various toxicities [32]. Bilobalide increased the respiratory control ratio of mitochondria and consequently adenosine triphosphate (ATP)-levels. Furthermore, under ischemic conditions bilobalide allows mitochondria to maintain their respiratory activity, delaying the onset of ischemia-induced damage [33].
Antioxidative effects
Oxidative stress contributes to the development and progression of AD [34]. Oxidative damage to mitochondria leads to a decreased energy charge and redox state, loss of transmembrane potential (depolarization), and mitochondrial respiratory chain impairment which may constitute a part of the spectrum of chronic oxidative stress in AD. Accumulation of Aβ in the form of senile plaques is also thought to play a central role in the pathogenesis of AD mediated by oxidative stress. EGb 761 was able to protect mitochondria from the attack of hydrogen peroxide, antimycin and Aβ. Furthermore, EGb 761 reduced ROS levels and ROS-induced apoptosis in lymphocytes from aged mice treated orally with EGb 761 for 2 weeks [31]. Mainly flavonoids [35] as well as ginkgolides and PACs [36] are potent antioxidants which possess radical-scavenger activity leading to a reduction of ROS and an inhibition of membrane lipid oxidation. They further act as chelators of pro-oxidative heavy metal ions and increased expression of antioxidant proteins, such as superoxide dismutase or glutathione reductase.
Anti-inflammatory effects
Reduction of neuroinflammation
Together with the formation of Aβ and p-tau, failure in innate immune response and chronic neuroinflammation belong to the main mechanisms of AD pathology. Beside the function as radical scavengers, flavonoids mediate various mechanisms to reduce the inflammatory response including inflammatory cytokine production (i.e., IL-1β, TNF-α, lipooxygenases and prostaglandin E2) [37]. In a mouse model overexpressing human AβPP (TgCRND8), EGb 761 treatment decreased Aβ-induced microglial secretion of TNF-α and IL-1β and activation of caspase-1. The extract further reduced the concentration of the inflammatory NLRP3 protein in primary murine cells [15]. EGb761 administration for 6 months downregulated pro-inflammatory cytokines and inducible nitric oxide synthase (iNOS), and upregulated anti-inflammatory cytokines and Arginase-1 in the APP/PS1 mouse brain. This is supported by the finding that treatment of a murine microglial cell line with EGb761 inhibited the inflammatory reaction to Aβ [38]. In LPS-activated primary microglia cells, EGb 761 reduced neuroinflammation by targeting the COX/PGE2 pathway [39].
The effect of EGb761 was investigated on peripheral blood leukocytes from AD patients versus healthy controls. EGb 761 decreased the production of cytokines (i.e., TNF-α, IFN-γ, IL-10, IL-15, IL-1β) to a greater extent in the AD group than in the control group [40]. In an AD mouse model, the component bilobalide improved learning and memory, which was attributed to a suppressed inflammatory response [21]. PACs as another group of plant substances were also shown to inhibit the production of proinflammatory cytokines and inflammation mediators [41].
Beneficial changes in gut microbiome
Various studies have provided evidence for a microbiome– mediated gut– brain axis explaining how the gut microbiome influences brain health and modulating gut microbiome might be an interesting strategy to reduce the risk of AD [42]. A significant improvement of spatial memory by oral EGb 761 administration (100 mg/kg/day) for 2 months was demonstrated in an AD mouse model. In the study, the extract reshaped the disturbed gut microbiome and significantly reversed the dysfunction of the microbial metabolism [43]. Bacteria suspended in saline solution were seeded on agar plates to assay the inhibitory effect of ginkgo biloba leaf substances. Bilobalide, ginkgolides A and B and quercetin were suspended in methanol, applied to paper discs, and placed on the agar plates. After two days of incubation, the flavonoid kaempferol was shown to possess a potent inhibitory activity against Clostridium perfringens and Escherichia coli as well as quercetin against Clostridium perfringens while growth of beneficial bacteria such as {Bifidobacterium bifidum, {B. longum, {B. adolescentis, or Lactobacillus acidophilus was not altered [44].∥
Improvement of microcirculation
One of the most commonly described mechanisms of action of ginkgo biloba is the improvement in cerebral blood flow. EGb 761 has been shown to possess vaso-regulatory and blood flow-enhancing properties [45]. The herbal preparation normalizes the elasticity of human erythrocyte membranes and protects the red blood cells against sclerosis, increased viscosity and oxidative stress [46]. Visualization using radioactive 133Xe in humans showed that EGb 761 increases cerebral blood flow [47]. In another study, administering EGb 761 brought cerebral blood flow post ischemia back to normal levels in 19 patients [48]. A study was conducted in patients over age 62 with impaired cerebral perfusion due to arteriosclerosis; blood flow improved by 75% after treatment with EGb 761 [49].
CLINICAL EFFICACY OF EGB 761 IN INDIVIDUALS WITH COGNITIVE IMPAIRMENT
The first clinical studies on EGb 761 for the treatment of cognitive impairment were published in the 1980s [50], and a large number of trials have been conducted since then. To give an overview of the various types of studies in patients with dementia or mild cognitive impairment (MCI), we conducted an extensive PubMed search for GbE and EGb 761. We selected randomized controlled clinical trials (versus placebo, AChEI, combination of EGb 761 plus AChEI) [51–56], a pragmatic trial conducted in a primary care setting, [57], cohort studies [58–60], studies comparing EGb 761® and cholinesterase inhibitors [61–63], as well as prevention trials [58, 65] (Table 2).
Overview of clinical research on the efficacy of EGb 761 in MCI and dementia
AD, Alzheimer’s disease; ADAS-Cog, Alzheimer’s Disease Assessment Scale –cognitive subscale; CFT, Category Fluency Test; CGI, Clinical Global Impression; LFT, Letter Fluency Test; MMSE, Mini-Mental Status Examination; NPI, Neuropsychiatric Inventory; QOL-AD, Quality of Life in Alzheimer Disease; RAVLT, Rey Auditory Verbal Learning Test; RCT, randomized controlled trial; SKT, Syndrom-Kurztest (Short Cognitive Performance Test); STAI, State-Trait Anxiety Inventory; TMT, Trail-Making Test; WTS-ALS, Wiener Testsystem – Arbeitsleistungsserie (Vienna Test System – Work-Performance Series).
Placebo-controlled trials of EGb 761 in symptomatic treatment of neurocognitive disorders, including patients with AD
In two multi-center, double-blind, randomized, placebo-controlled, 24-week trials with the same design, 820 patients with mild to moderate dementia (AD, vascular dementia) associated with clinically significant neuropsychiatric symptoms (NPS) were treated with a once-daily formulation of 240 mg EGb 761. Efficacy and safety of this new dosing regimen of EGb 761 were demonstrated in each of these studies [51, 52]. Significant superiority over placebo was observed for both primary endpoints (Short Cognitive Performance Test) for cognition and Neuropsychiatric Inventory (NPI) for neuropsychiatric symptoms, p < 0.001) as well as for secondary outcomes (including activities of daily living (ADL) and Global Impression of Change (CGI)). A 22-week, randomized, placebo-controlled trial enrolled patients with mild to moderate dementia (AD, vascular dementia) who had clinically significant NPS. In this trial, EGb 761 (240 mg/day) was significantly superior to placebo in all cognitive outcomes (Syndrom Kurztest, Verbal Fluency Test, Clock-Drawing Test), ADL (Gottfries-Bråne-Steen Scale – ADL subscale), global rating of change (Gottfries-Bråne-Steen Scale – total score), and NPS (NPI) (all p-values<0.001). Results were essentially similar for the whole sample and patients with AD [66]. In these three trials, AD was diagnosed in accordance with the criteria of the National Institutes of Neurological and Communicative Disorders and Stroke/Alzheimer’s Disease and Related Disorders Association [67] and superiority over placebo was found for AD patients. A 6-month, randomized, multi-center trial to which 119 general practitioners recruited 176 patients with a clinical diagnosis of dementia, without the use of formal diagnostic criteria and without distinguishing between AD and other forms of dementia, found no difference between EGb 761 (120 mg/day) and placebo [57]. In this trial, one-third of the patients of both treatment groups were on AChEIs and more patients of the EGb 761 group than of the placebo group had taken GbE preparations before. Moreover, half of the patients of each group were randomized to intensive follow-up, and the other half was randomized to receive minimal follow-up, which further increased variances and decreased statistical power. One randomized, placebo-controlled trial conducted in the United States enrolled a sample of 513 highly selected patients with mild to moderate AD. Exclusion criteria related to cerebrovascular pathologies or neuropsychiatric symptoms were even stricter than commonly applied to patients of AChEI trials. This trial yielded inconclusive results for the total sample but found significant and borderline significant superiority of EGb 761 at a daily dose of 240 mg for the ADAS-cog and CGIC, respectively, in patients with at least minimal NPS [54]. A small, mono-centric, 3-month study in a specialized Alzheimer’s center and two larger multi-center trials, one in Germany with a 6-month treatment period [68, 69] and one in the United States with 12-month treatment [70], were conducted during the 1990s. While the mono-centric study included only patients with AD, patients with AD or multi-infarct dementia were enrolled in the two multi-canter trials. Due to prospective application of the diagnostic criteria for dementia of the Alzheimer type (Diagnostic and Statistical Manual of Mental Disorders, Version III, Revised), separate analyses could be run for the AD subgroups. Significant superiority over placebo could be demonstrated for cognitive outcomes (Syndrom Kurztest, Alzheimer’s Disease Assessment Scale – cognitive subscale) in all three trials. The clinical relevance of these findings was supported by significant superiority of EGb 761 in an ADL scale [71] or the CGI [68, 69]. In the single-center trial the CGI of change also showed a trend in favor of EGb 761, which, due to the small sample size, did not reach statistical significance [72].
The two latest randomized, placebo-controlled studies of EGb 761 in MCI will be discussed briefly since MCI is considered an early symptomatic stage of dementia disorders and, specifically, amnestic MCI is seen as a pre-dementia stage of AD [73]. In a double-blind, randomized, placebo-controlled, 24-week trial, 160 patients diagnosed with amnestic MCI associated with NPS were treated with EGb 761, 240 mg once daily [55]. Superiority of EGb 761 over placebo was reported for the cognitive tests (Trail-Making Test Forms A and B, p < 0.05), as well as for scales assessing NPS (NPI, p = 0.002), State-Trait Anxiety Inventory, and the informants’ CGI. Moreover, trends favoring EGb 761 were observed for the Geriatric Depression Scale and the patients’ global impression of change. In a multi-canter, double-blind, randomized, placebo-controlled, 12-week trial, 300 patients with very mild MCI were treated with EGb 761, 240 mg once daily. Significant improvement (p < 0.025) over placebo was found in a test of attention (Vienna Test System-Work Performance Series) and trends in favor of EGb 761 were seen in memory tests (Wechsler Memory Scale III) and a scale for perceived physical health (Short Form 36). Improvements in memory tests were more pronounced and also statistically significant for a pre-specified subgroup of patients with lower memory function at baseline [56].
Other trials of EGb 761 in symptomatic treatment of neurocognitive disorders, including patients with AD
In a comparison of EGb 761 to AChEIs in the treatment of AD, a small randomized 6-month trial found somewhat larger effects of rivastigmine than for EGb 761 (120 mg/day) in two cognitive tests [63], whereas a randomized, reference- and placebo-controlled trial found essentially similar treatment effects for EGb 761 (160 mg/day) and donepezil in two cognitive tests and the CGI after 6-month treatment [61]. A retrospective cohort of 133 patients with amnestic MCI found significant superiority of combined treatment with EGb 761 and AChEIs over AChEIs alone in a series of cognitive tests and on the NPI [62]. In a prospective observational cohort study involving 500 patients with amnestic MCI, a statistically significant 2-point median improvement in the Mini-Mental Status Examination (MMSE) was achieved during 24-month treatment with EGb 761 (120 mg/day), along with CGI of change improvement in more than 80% of patients, and a mean improvement by 2.4 points on the Hamilton Depression Scale [59]. Significant superiority of EGb 761 in combination with various AChEIs over AChEIs alone was seen in a cohort study involving 828 patients with AD [60].
Several meta-analyses have shown that EGb 761 provides beneficial effects in the symptomatic treatment of dementia [8, 75]. Importantly, EGb 761 did not only improve cognitive impairment, traditionally considered to be core symptomatology of dementia, ADL and global ratings [8, 74]; to a clinically significant extent, it also improved neuropsychiatric symptoms (also referred to as behavioral and psychological symptoms) which are present in the vast majority of patients with AD [8, 76] and are now considered core symptoms of dementia with diagnostic value [77]. The strongest effects were found for apathy, depression, anxiety, sleep, and nighttime behavior [76]. Moreover, for studies that enrolled patients with AD and those with vascular dementia, meta-analyses endorse the findings from individual studies that EGb 761 is effective in patients with AD [8, 10]. No excess numbers of adverse events or serious adverse events were found in studies and meta-analyses [8, 74].
Trials addressing prevention of AD
A few studies addressed the question as to whether EGb 761 might prevent cognitive decline and the development of dementia. The Ginkgo Evaluation of Memory (GEM) Study, initially designed as a 5-year, randomized double-blind, placebo-controlled trial of EGb 761 (120 mg twice per day), recruited 3069 non-demented elderly (cognitively normal or with MCI) from September 2000 to June 2002. Compared with placebo, the use of EGb 761 did not result in a decreased rate of progression to dementia or slower cognitive decline, despite reaching the required number of dementia events after the follow-up period had been extended (median 6.1 years) [64]. Above average education and a high proportion of subjects with very good or excellent perceived general health may have contributed to the extraordinarily slow cognitive decline and low incidence rate for AD.
The GuidAge Study was a randomized, parallel-group, double-blind, placebo-controlled clinical trial that enrolled 2854 participants in France between March 2002 and November 2004. Elderly subjects (70 years or above) who spontaneously reported memory complaints were allocated to receive EGb 761 (120 mg twice daily) or matched placebo and were followed-up for 5 years [78]. The use of EGb 761 did not reduce the risk of progression to AD compared with placebo [65]. However, in this study the incidence of dementia was much lower than expected: only 61 participants of the EGb 761-treated group and 73 patients of the placebo group developed probable AD over 5 years (hazard ratio 0.84). Hence, the statistical power to detect an effect was lower than estimated. Moreover, the risk of progressing to AD was not proportional over time but increased with the time of follow-up. For the subgroup of patients treated with EGb 761 for more than 4 years, a decrease in the risk for developing AD by 50% versus placebo was observed (p = 0.03). There was a significant treatment-by-time interaction (p = 0.043) and the proportional hazards assumption was not fulfilled. In post-hoc analyses, assuming non-proportional hazards and carrying out a corresponding statistical test, the hazard for progression to dementia was significantly different between EGb 761 and placebo groups (p = 0.0054), which points to a late effect of EGb 761. Since this was a post-hoc analysis, there is still no definitive answer to the question as to whether the treatment is effective in preventing dementia in patients with subjective memory impairment [79]. In a French cohort study that enrolled 3,612 elderly subjects (aged 65 and over), those who took EGb 761 (unspecified dose) experienced a significantly slower decline in cognitive abilities, as assessed by the MMSE, over a period of 20 years [58]. Thus, despite some encouraging results, the role of EGb 761 in the prevention of dementia remains an open question.
DISCUSSION
Extracts produced from ginkgo biloba leaves cover a very heterogenous spectrum ranging from highly standardized pharmaceutical substances to unregulated dietary supplements. Preparations derived from the same plant may differ considerably in their phytochemical composition, and thus their pharmacokinetic and pharmacodynamic properties: as a result, their clinical efficacy and safety may differ markedly. Extracts derived from Ginkgo biloba L collected at different times of the year or countries can differ significantly in their phytochemical composition, i.e., due to seasonal and geographical variability. Furthermore, proprietary multi-step manufacturing processes may also have an influence on the quality and the characteristics of the product. GbEs marketed as dietary supplements or pharmaceuticals do not follow the same strict quality control and regulatory procedures as medicinal products. Nutritional supplements may therefore contain several ingredients, some of which may not even be named on the label, and discrepancies between labelled and actual ingredients or the amounts of ingredients may occur [80]. In an analytical study of 63 different GbE preparations marketed in Germany, the results indicated a low reliability of the preparations that are sold as dietary supplements, whereas the reliability was high of preparations approved as drugs [81]. This applies to GbEs which are manufactured according to the requirements of the European Pharmacopeia. Our literature search revealed that the special extract EGb 761 was the best researched among GbEs.
Neuroinflammation plays a central role in the multifactorial pathophysiology of AD. Some studies have shown a reduction in serum inflammatory markers in patients treated with EGb 761 [82]. Other disease mechanisms of AD include neurodegeneration, mitochondrial damage, oxidative stress, or dysfunctional microbiota-gut brain axis. As a complex mixture of individual plant-derived chemical constituents which may act independently or synergistically, EGb 761 has been shown to exert a broad spectrum of pharmacological activities with potential relevance for AD pathophysiology. The reported activities include the stimulation of neuroplasticity, protection and restoration of mitochondrial function, reduction in the formation of p-tau and Aβ plaques, antioxidative effects, improvement of cerebral blood flow or restoration of dysfunctional microbiome, among others. A better understanding of the specific mechanism of action of EGb 761 in AD would be desirable so that patients can be selected who will benefit most from this therapeutical intervention. Currently, a randomized, open-label clinical trial of EGb 761 in patients with MCI is examining the blood markers of inflammation and oxidative stress [83]. It is probably this pleiotropic activity profile of EGb 761 with moderate pharmacological effects on various disease mechanisms that underlies the reported clinical efficacy in the treatment of AD.
Some clinical trials have yielded negative or inconclusive results, partly due to methodological problems such as highly selected and non-representative participants or potentially inappropriate settings; however, most clinical trials in patients with neurocognitive disorders showed superiority of EGb 761 over placebo, with improvements in cognition, NPS, ADL, and global ratings. A network meta-analysis was conducted to evaluate the therapeutic benefits and tolerability of EGb 761, three AChEIs (donepezil, galantamine, and rivastigmine), and memantine in mild-to-moderate AD patients. The selection of the three studies with EGb 761 remains unclear. The calculation in the publication reveals treatment effects for EGb 761 which are similar to rivastigmine. Nevertheless, the authors conclude that EGb761 and memantine showed no treatment benefits compared to placebo and AChEIs [84]. Other systematic reviews and meta-analyses support the efficacy of EGb 761 in the treatment of MCI and dementia, including AD [8, 74]. Consequently, some national and international guidelines and consensus documents have taken up EGb 761 as a symptomatic treatment option for MCI and/or dementia due to its favorable benefit/risk ratio (e.g., [85–88]). Overall, EGb 761 is well tolerated, even by elderly patients; no serious safety concerns have become evident during many years of widespread use.
CONCLUSIONS
Extensive pharmacological research has been carried out with EGb 761 in particular. Although a multitarget activity seems plausible, the mechanisms of action have not been elucidated. Moreover, it is not always clear if effects which were observed in vitro and in vivo are relevant for therapeutic use in humans in terms of concentration and bioavailability. While the effect of individual constituents on various pathophysiological features has been tested using different in vivo models, implementing this approach in clinical studies would be extremely difficult due to the complexity of EGb 761 composition. Clinical research is promising. However, studies reveal heterogeneity regarding methodology and outcomes. The synergistic effect of EGb 761 and AChEI and other topics deserve to be explored further in randomized clinical trials.
AUTHOR CONTRIBUTIONS
Xavier Morato (Conceptualization; Writing –original draft); Juan Pablo Tartari (Writing – review & editing); Vanesa Pytel (Writing – review & editing); Mercè Boada (Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
We are grateful to the experts at the ACE Alzheimer Center Barcelona for their continuous support. This work was funded by research funds of the Ace Alzheimer Center Barcelona.
FUNDING
This work was supported by funds from Fundació ACE, Institut Català de Neurociències Aplicades.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
Data sharing is not applicable to this article as no datasets were generated or analyzed during this study.