
Abstract
Background
Medicare claims data enables broad characterization of United States (US) patients with Alzheimer's disease and related dementias (ADRD). Resulting insights can be used as a reference to describe this population and as a benchmark for generalizability of patients with ADRD enrolled in clinical trials.
Objective
To characterize demographics, comorbidities, comedications, and healthcare resource utilization in US patients with newly diagnosed ADRD, focusing on differences across Medicare fee-for-service (FFS) and Medicare Advantage enrollees.
Methods
This observational cohort study used complete (100%) Medicare claims data inclusive of both FFS and Medicare Advantage insurance types. Study patients were ≥65-years-old with ≥12 months of continuous pre-index enrollment and Medicare Part D coverage. Two cohorts of patients were selected in calendar year 2019; those newly diagnosed with ADRD and those with a new acetylcholinesterase inhibitor (AChEI) claim.
Results
The newly diagnosed ADRD and new AChEI users cohorts included 861,727 and 395,319 patients, respectively. Demographics and comedications were generally similar across the two cohorts, supporting internal validity of the study results. Circulatory system-related comorbidities and mood disorders were common in both cohorts. Differences in race, inpatient claims and long-term care claims were observed between insurance types.
Conclusions
The study results provide a reference for describing the ADRD population in the US and emphasize the importance of evaluating new Alzheimer's disease drugs in broad patient populations with comorbidities and concomitant medication use.
Introduction
Randomized controlled trials (RCTs) are the gold standard for testing efficacy and safety of new medications. 1 However, RCT enrollment criteria may exclude real-world disease subgroups and/or lack appropriate generalizability to real-world populations. 2 Characterization of real-world disease populations using real-world data can inform the representativeness of clinical trial populations and give confidence in the generalizability of RCT results.
In the case of Alzheimer's disease and related dementias (ADRD), characterization of this real-world disease population can be accomplished using Medicare claims data,3–6 a data source that includes most patients living with ADRD in the United States (US). However, the identification of patients with ADRD in claims data is unlike ADRD identification in RCTs where methods such as positron emission tomography (PET) imaging for amyloid and tau can be utilized. 7 This is not currently possible in Medicare claims data for two reasons. First, PET imaging to support ADRD clinical diagnosis is not yet a common practice in the real world, 8 although the introduction of anti-amyloid therapies and Medicare coverage of PET imaging to support ADRD clinical diagnosis9,10 may change this in the future. Second, even if PET imaging to support ADRD clinical diagnosis becomes common in the real world, imaging results are not available in claims data. Therefore, claims research in ADRD relies on validated code-based claims algorithms to select study patients.
Previous real-world studies in the US Medicare population identified patients with Alzheimer's disease or ADRD using older claims algorithms.3–6 Recently, McCarthy et al. 11 validated the 1-year Bynum-Standard algorithm to identify patients with ADRD in Medicare claims data. This introduces the opportunity to better characterize the existing real-world population of patients with ADRD in the US using Medicare claims and this newly validated algorithm. 11
A cohort of new acetylcholinesterase inhibitors (AChEI) users was also compiled for analysis. Per DiFrancesco et al., 12 the positive predictive value (PPV) of using AChEIs to identify patients with ADRD is expected to be lower than the PPV reported for the 1-Year Bynum Standard Algorithm.11,12 However, previous research into treatment patterns has shown that patients newly diagnosed with ADRD often receive symptomatic anti-dementia medications prior to receiving an ADRD diagnosis. 13 Therefore, use of this additional medication use algorithm will facilitate (1) potential identification of patients slightly earlier in the disease process and (2) descriptive comparison with patients with ADRD selected using the 1-Year Bynum Standard Algorithm. Agreement of results across these two cohorts increases confidence in the internal validity and generalizability of the study findings.
Finally, a recent publication found an association between Medicare insurance type (Fee-for-Service [FFS] versus Advantage) and care quality. 14 Given this and the sparsity of results describing differences in ADRD Medicare populations based on insurance type, the current study also aimed to describe differences in demographics, comorbidities, comedications, and healthcare resource utilization (HCRU) among patients newly diagnosed with ADRD, stratified by insurance type.
Methods
Data source
Complete Medicare FFS Part A and Part B, Medicare Advantage (MA), and Medicare Part D administrative claims data were used for analysis in this study; this represents 100% of all Medicare claims. Medicare FFS and MA data were accessed through CareJourney's License with the Centers for Medicaid & Medicaid Services’ Virtual Research Data Center, which provides full access to Medicare Parts A, B, D, and MA claims. The beneficiary ID between MA and Medicare FFS is consistent across the data sets. Therefore, it is possible to identify the patients’ insurance plan type as FFS only, MA only, or both FFS and MA and to distinguish their coverage type for any care delivered. At the time of analysis, given a lag in access for MA claims, 2019 was the most recent year available for MA data. In 2019, Medicare covered 61.5 million lives 15 comprising 38.6 million Medicare FFS 16 and ∼22.9 million MA users. 17
Study design and patient population
This descriptive, observational cohort study included patients with a cohort-qualifying diagnosis or medication (i.e., qualifying index event) from January 1, 2019 through December 31, 2019 (index period). Patients were selected during 2019 to reduce biases associated with the 2020 COVID-19 pandemic and to allow for incorporation of available MA data, which had an access lag.
Patients were classified into newly diagnosed ADRD cohort or new AChEI users cohorts based on the inclusion and exclusion criteria given below. Since patients could qualify for both the newly diagnosed ADRD cohort and the new AChEI users cohort, the two cohorts were not mutually exclusive. These two cohorts include patients from both Medicare FFS and MA insurance types. Patients with both FFS and MA during the assessment period were called FFS/MA switchers. Common inclusion criteria across the cohorts were patients aged ≥65 years at the index date, ≥12 months of continuous pre-index medical enrollment (either Medicare FFS, Medicare MA, or a combination of both) and ≥12 months of pre-index Part D prescription enrollment, allowing for a 1-month enrollment gap in both medical and prescription enrollment. The 1-year pre-index period, including the index date, was considered as the “baseline period” for analyses.
Newly diagnosed ADRD cohort
The 1-year Bynum-Standard ADRD algorithm 11 was used to select patients for the newly diagnosed ADRD cohort. This algorithm utilizes a 1-year index period and requires at least one inpatient, skilled nursing facility, home health agency, or hospice ADRD claim; or two outpatient ADRD claims occurring at least 7 days apart in the Carrier (Provider) or hospital outpatient files from rural health clinics, federally qualified health centers, and critical access hospitals–payment option II. This algorithm has been validated in Medicare FFS claims and has a 70.3% PPV and 31.3% sensitivity for ADRD when compared with the Health and Retirement Study dementia status as the reference standard. 11 The index date used in this cohort was the date of the first ADRD diagnosis during the index period (January–December 2019). This cohort included patients with (1) ≥1 International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnosis code for ADRD in an inpatient setting with a claim end date in 2019 or (2) ≥2 ICD-10-CM diagnosis codes for ADRD recorded ≥7 days apart in an outpatient setting with claim end dates in 2019. To establish newly diagnosed ADRD, patients with an ADRD ICD-10-CM diagnosis code from 12 months pre-index to −1 day before the index date were excluded.
New AChEI users cohort
For descriptive comparison with the Bynum-Standard ADRD algorithm, a cohort of patients with new AChEI prescriptions was also compiled. This cohort included patients with ≥1 pharmacy claim for an AChEI during the index period. The date of the first AChEI claim for galantamine, rivastigmine, or donepezil during the index period (January–December 2019) was considered as the index date. To ensure new use of an AChEI, patients with an AChEI claim from 12 months pre-index to −1 day before the index date were excluded. Memantine was excluded because it is prescribed for treatment of moderate-to-severe disease, but not early disease.18,19 This algorithm is expected to have a lower PPV than the Bynum Standard ADRD algorithm per DiFrancesco et al. 12 However, given that patients may receive ADRD treatment before they receive ADRD diagnoses 13 this additional cohort provides unique insight into patients who are potentially earlier in the ADRD disease process.
Variables
Demographics assessed on the index day (i.e., first 2019 ADRD diagnosis for the newly diagnosed ADRD cohort or first 2019 AChEI medication for the new AChEI users cohort) included age, sex, census division, race, Medicaid-Medicare dual eligibility, and rurality. Medicare insurance type was assessed during the 1-year pre-index period including the index date. Patients could qualify for one of three mutually exclusive insurance type groups; FFS only, MA only, or both FFS and MA during baseline (classified as FFS/MA switchers).
The 1-year pre-index period, including the index date, was considered as the “baseline period” for analyses of comorbidities, comedications, and HCRU. Comorbidities were assessed using either validated or medically reviewed ICD-10-CM diagnosis code lists. The Charlson Comorbidity Index (CCI) 20 was also evaluated. Top dementia and non-dementia medications, obtained from Medicare Part D claims were reported. Comedication use was also assessed by drug class using the Anatomical Therapeutic Chemical classification system (Supplemental Table 1).
HCRU evaluation included the proportion of patients with claims for inpatient care, emergency room (ER) visits, and long-term care. Due to lack of claim-level specialty information in MA claims, specialist visits were analyzed in the subgroup of patients with FFS insurance coverage only. In the newly diagnosed ADRD cohort only, as a surrogate for ADRD-diagnosing physician specialty, specialist visits on the index day to a primary care physician (PCP), neurologist, immediate/ urgent care, or the ER, were assessed. Here, PCP was defined as a practitioner of internal medicine, general practice, family practice, or geriatric medicine.
Demographics, comorbidities, comedications, and HCRU analyses in both cohorts were stratified by insurance type (FFS only, MA only, or FFS/MA switchers) to describe differences observed across FFS and MA enrollees.
Statistical analysis
Data were summarized using descriptive statistics; cohorts were not adjusted to control for confounding/statistically compared as the primary objective of this study was to describe real-world populations with ADRD. To leverage inclusion of both FFS and MA data, the main analyses for both cohorts included all insurance types (FFS only, MA only, and FFS/MA switchers). In addition, all analyses in both cohorts were stratified by insurance type. Continuous variables were presented as means and standard deviations (SD) and categorical variables were presented as counts and frequencies.
Subgroup analyses in the newly diagnosed ADRD and new AChEI users cohorts and the insurance type stratifications were performed on the basis of patients’ age at the index date (65 to <75, 75 to <85, and ≥85 years); sex (male or female); rurality at the index date using rural-urban commuting area (RUCA) codes (rural [RUCA code 1–3], non-rural [RUCA code 4+], and other rural [no RUCA code available]); and long-term care status (yes or no).
Two sensitivity analyses were performed to assess the impact of study assumptions. Sensitivity Analysis #1 was applicable to both cohorts; here, the index period was expanded from 1 year to 3 years (January 1, 2017 through December 31, 2019) to determine if cohort selection over a single year impacted the results. This sensitivity analysis is equivalent to the 3-year Bynum-Standard ADRD algorithm for the newly diagnosed ADRD cohort. 11 Sensitivity Analysis #2 was applicable to the newly diagnosed ADRD cohort only; here, patients with an AChEI claim from 12 months pre-index to −1 day before the index date were excluded, as many patients in this cohort were treated with an AChEI during the pre-index period (i.e., before ADRD diagnosis) which could be indicative of established disease.
Results
After applying the relevant cohort selection criteria, 861,727 patients in the newly diagnosed ADRD cohort (Figure 1(a)), and 395,319 patients in the new AChEI users cohort (Figure 1(b)) were selected for analysis. In the newly diagnosed ADRD cohort, 437,989 (50.8%) were enrolled in FFS only, 382,799 (44.4%) were enrolled in MA only, and 40,939 (4.8%) were FFS/MA switchers (Table 1). In the new AChEI users cohort, 186,686 (47.2%) were enrolled in FFS only, 189,794 (48.0%) were enrolled in MA only, and 18,839 (4.8%) were FFS/MA switchers.
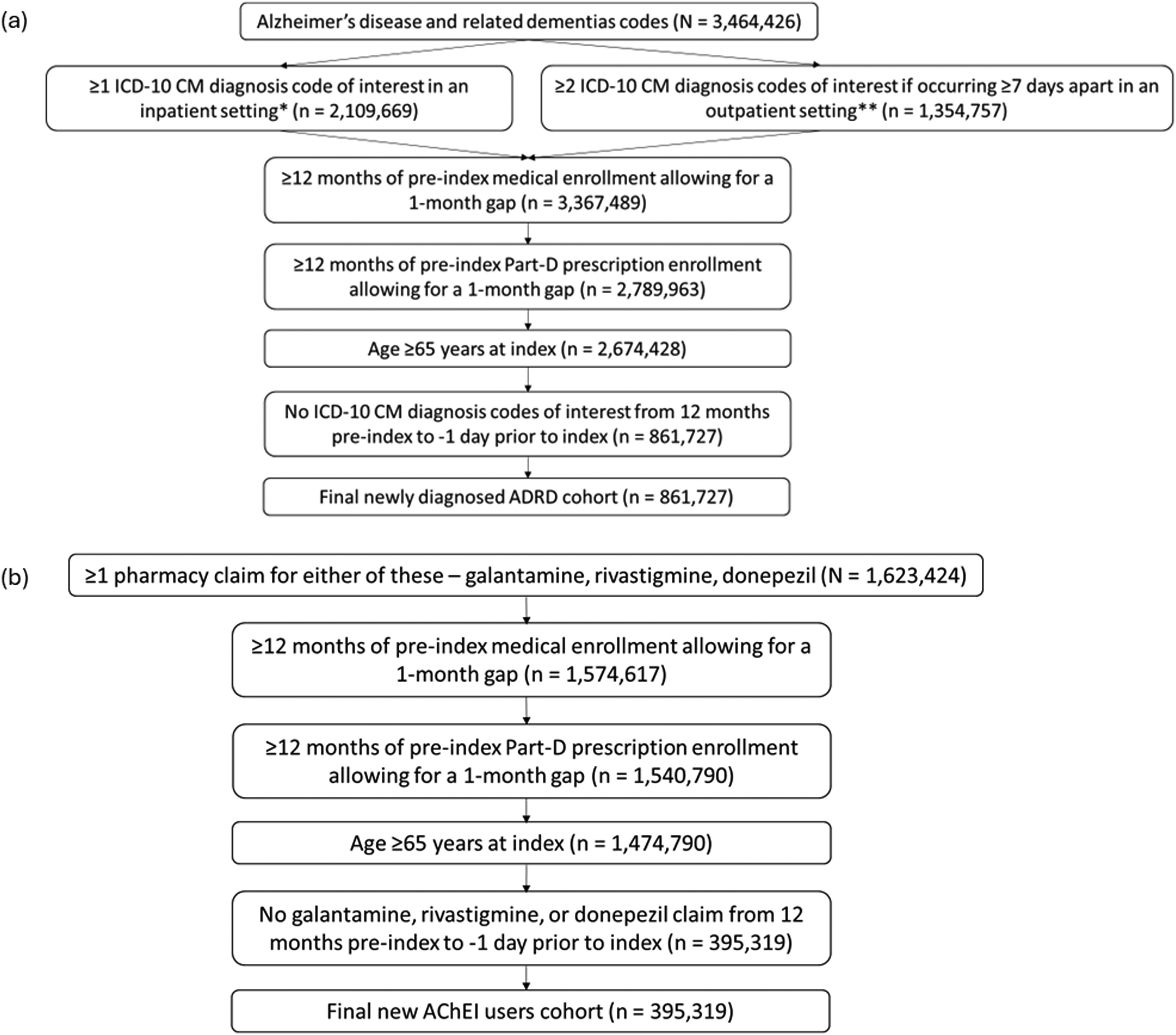
Selection of the study cohorts. (a) Newly diagnosed ADRD cohort (patients with an ADRD diagnosis) and (b) New AChEI users cohort (patients with new use of AChEIs). *Inpatient setting also includes skilled nursing facility, home health agency, and hospice. **Outpatient setting includes Carrier (Provider) or hospital outpatient files from rural health clinics, federally qualified health centers, and critical access hospitals–payment option II. AChEI, acetylcholinesterase inhibitors; ADRD, Alzheimer's disease and related dementias; ICD-10-CM, International Classification of Diseases, Tenth Revision, Clinical Modification.
Demographic characteristics across cohorts.
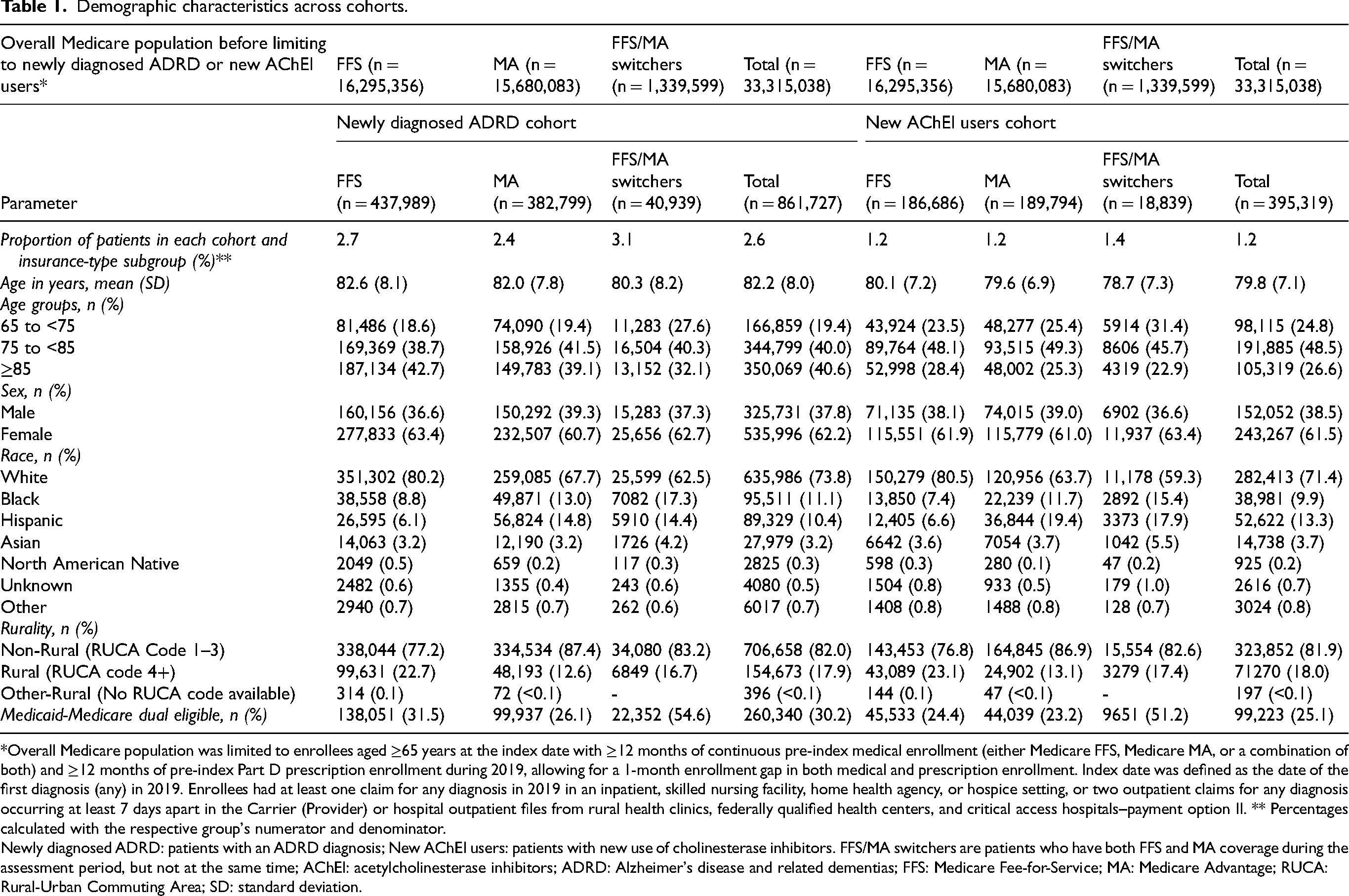
*Overall Medicare population was limited to enrollees aged ≥65 years at the index date with ≥12 months of continuous pre-index medical enrollment (either Medicare FFS, Medicare MA, or a combination of both) and ≥12 months of pre-index Part D prescription enrollment during 2019, allowing for a 1-month enrollment gap in both medical and prescription enrollment. Index date was defined as the date of the first diagnosis (any) in 2019. Enrollees had at least one claim for any diagnosis in 2019 in an inpatient, skilled nursing facility, home health agency, or hospice setting, or two outpatient claims for any diagnosis occurring at least 7 days apart in the Carrier (Provider) or hospital outpatient files from rural health clinics, federally qualified health centers, and critical access hospitals–payment option II. ** Percentages calculated with the respective group's numerator and denominator.
Newly diagnosed ADRD: patients with an ADRD diagnosis; New AChEI users: patients with new use of cholinesterase inhibitors. FFS/MA switchers are patients who have both FFS and MA coverage during the assessment period, but not at the same time; AChEI: acetylcholinesterase inhibitors; ADRD: Alzheimer's disease and related dementias; FFS: Medicare Fee-for-Service; MA: Medicare Advantage; RUCA: Rural-Urban Commuting Area; SD: standard deviation.
Demographic characteristics
Demographic characteristics were similar across both cohorts (Table 1). The mean (SD) age of patients was 82.2 (8.0) years in the newly diagnosed ADRD cohort and 79.8 (7.1) years in the new AChEI users cohort. Females (61.5%–62.2%) were more common than males (37.8%–38.5%). Black and Hispanic patients comprised 9.9% to 13.3% of the patients in these cohorts. The proportion of Medicaid-Medicare dual eligible patients was 30.2% in the newly diagnosed ADRD cohort and 25.1% in the new AChEI users cohort. Stratification by insurance type showed no differences in age and sex (Table 1). The proportions of Black patients differed across insurance types (FFS only, 7.4%–8.8%; MA only, 11.7%–13.0%; and FFS/MA switchers, 15.4%–17.3%). Similarly, the proportions of Hispanic patients differed across insurance types (FFS only, 6.1%– 6.6%; MA only, 14.8%–19.4%; and FFS/MA switchers, 14.4%–17.9%). FFS/MA switchers had the highest proportion of patients with Medicaid-Medicare dual eligibility (51.2%–54.6%), followed by FFS only (24.4%–31.5%), and MA only (23.2%–26.1%).
In the age-stratified subgroup analysis, the proportion of females increased with greater age across cohorts (Supplemental Table 2). The proportion of females in each age subgroup was similar across the newly diagnosed ADRD (56.0%–68.3%) and new AChEI users (58.6%–67.2%) cohorts. The proportion of Black and Hispanic patients reduced with increasing age. These patients were most common in the subgroup aged 65 to <75 years (newly diagnosed ADRD cohort: Black patients – 15.9% and Hispanic patients – 12.1% and new AChEI users cohort: Black patients – 11.8% and Hispanic patients – 15.7%).
In all additional subgroup analyses, few differences were observed across the subgroups of both the cohorts (Supplemental Tables 3–5). In the sex-stratified subgroup analysis, only the proportion of Medicaid-Medicare dual eligible patients slightly differed between males (20.3%–26.0%) and females (28.1%–32.8%) (Supplemental Table 3). In the long-term care-stratified subgroup analysis, use of long-term care was the highest in patients aged 75 to <85 years (38.2%–45.3%) and ≥85 years (35.2%–41.2%) (Supplemental Table 5).
Baseline comorbidities
Mean (SD) values for CCI, a predictive measure of mortality risk, were 4.8 (2.9) in the newly diagnosed ADRD cohort and 3.6 (2.6) in the new AChEI users cohort (Table 2). Hypertension was the most common baseline comorbidity (≥84.8%) across cohorts. The newly diagnosed ADRD cohort had a higher proportion of patients with circulatory system-related comorbidities, such as atrial fibrillation, acute myocardial infarction/ischemic heart disease, chronic kidney disease, heart failure, peripheral vascular disease, and stroke/transient ischemic attack. Mild cognitive impairment (MCI) was more common (21.7%) in the new AChEI users cohort, potentially indicative of an earlier stage of disease. The proportions of patients were similar for most comorbidities across cohorts. Stratification by insurance type showed a similar presence of comorbidities as observed in the main cohorts across FFS only, MA only, and FFS/MA switchers (Table 3).
Baseline comorbidities across cohorts.
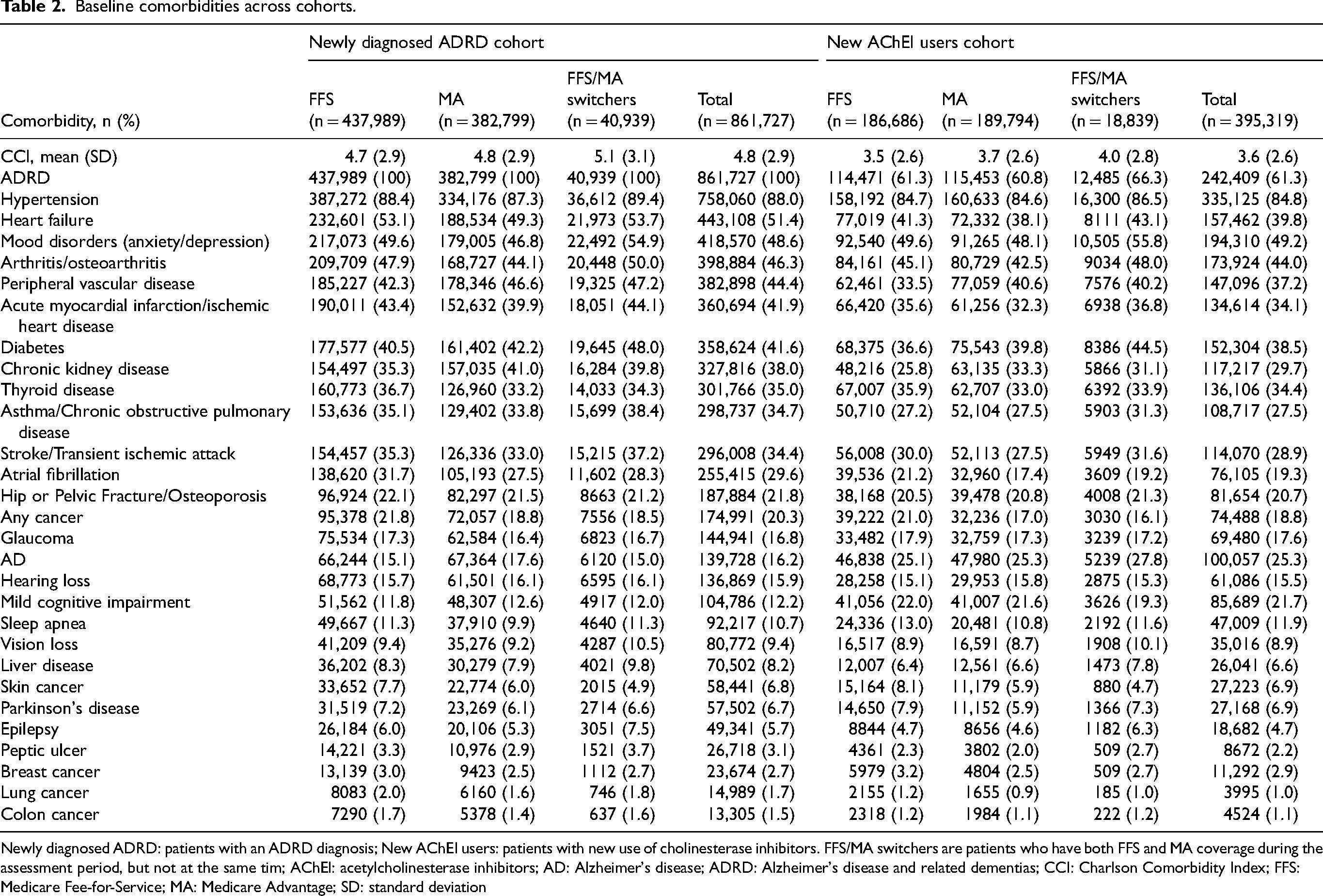
Newly diagnosed ADRD: patients with an ADRD diagnosis; New AChEI users: patients with new use of cholinesterase inhibitors. FFS/MA switchers are patients who have both FFS and MA coverage during the assessment period, but not at the same tim; AChEI: acetylcholinesterase inhibitors; AD: Alzheimer's disease; ADRD: Alzheimer's disease and related dementias; CCI: Charlson Comorbidity Index; FFS: Medicare Fee-for-Service; MA: Medicare Advantage; SD: standard deviation
Anti-dementia drug usage and top baseline comedications across cohorts by generic name.
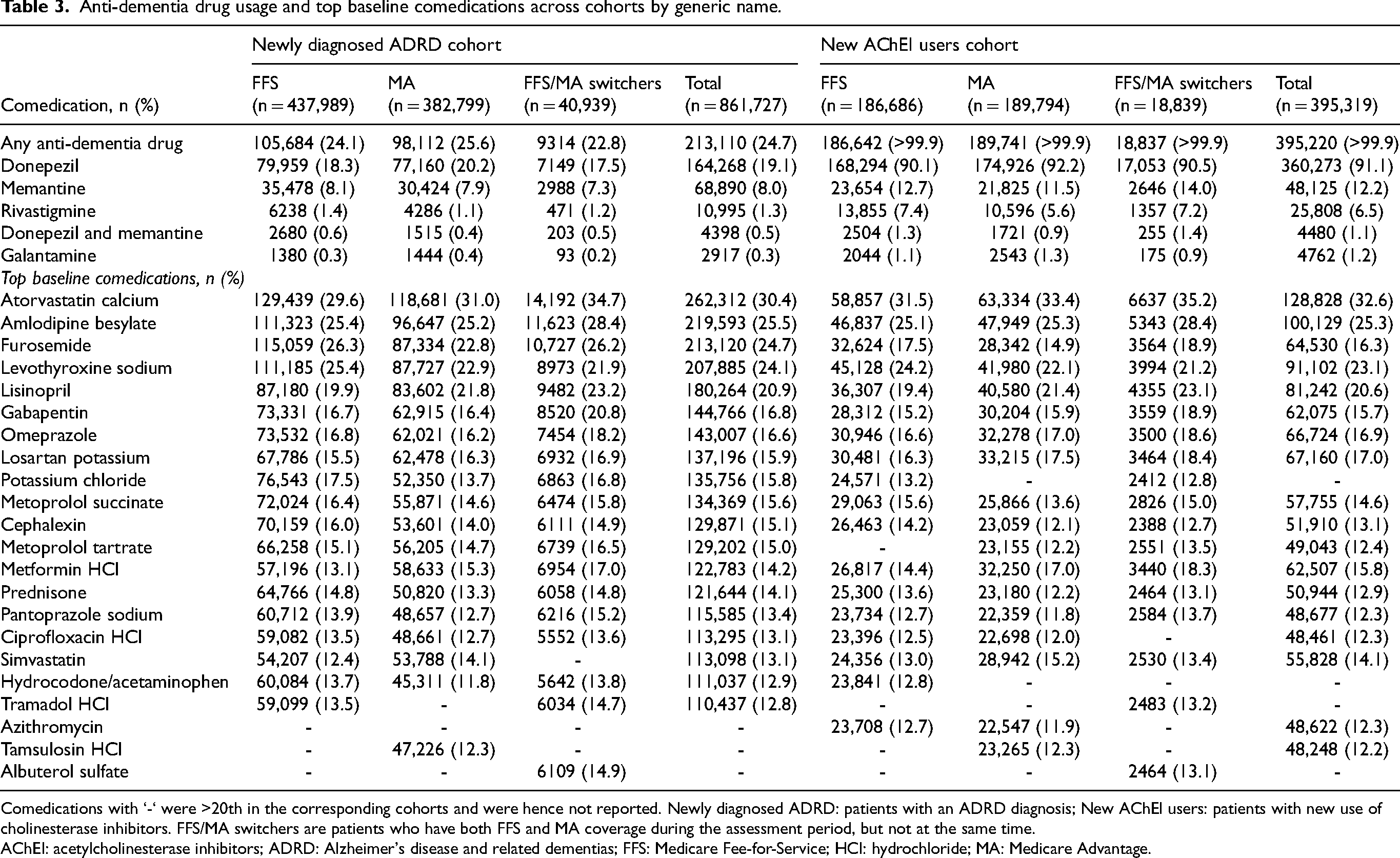
Comedications with ‘-‘ were >20th in the corresponding cohorts and were hence not reported. Newly diagnosed ADRD: patients with an ADRD diagnosis; New AChEI users: patients with new use of cholinesterase inhibitors. FFS/MA switchers are patients who have both FFS and MA coverage during the assessment period, but not at the same time.
AChEI: acetylcholinesterase inhibitors; ADRD: Alzheimer's disease and related dementias; FFS: Medicare Fee-for-Service; HCl: hydrochloride; MA: Medicare Advantage.
In the age-stratified subgroup analysis, CCI was similar across age groups (Supplemental Table 6). Patients aged ≥85 years had the highest proportion of circulatory system-related and bone-related comorbidities across cohorts. Patients aged 65 to <75 years had the highest proportion of diabetes (42.5%–50.1%), mood disorders (57.0%–61.7%), Parkinson's disease (8.4%–8.6%), and epilepsy (6.9%–10.8%); these comorbidities became less frequent with increased age.
In the sex-stratified subgroup analysis, males had a higher mean (SD) CCI than females in both the newly diagnosed ADRD (5.3 [3.0] versus 4.5 [2.8]) and new AChEI users cohorts (4.0 [2.7] versus 3.4 [2.5]) (Supplemental Table 7). Circulatory system-related comorbidities and diabetes were more common in males and bone-related comorbidities were more common in females across cohorts. Mood disorders were common and reported in ≥52.6% of females across cohorts.
No major differences were observed between the measure of rurality across cohorts (Supplemental Table 8). In the long-term care-stratified subgroup analysis, patients who required long-term care had a higher mean (SD) CCI than those who did not require long-term care in both the newly diagnosed ADRD (6.7 [3.0] versus 4.4 [2.7]) and new AChEI users cohorts (5.6 [2.8] versus 3.3 [2.4]) (Supplemental Table 9). Most comorbidities were also more common in patients who required long-term care than in those who did not require long-term care.
Baseline comedications
In the newly diagnosed ADRD cohort, 24.7% of patients utilized an anti-dementia drug during their baseline time period (i.e., before ADRD diagnosis); no differences in this proportion were observed when the cohorts were stratified by insurance group (Table 3). Most comedications had similar use across both cohorts. Atorvastatin calcium (≥30.4%) and amlodipine besylate (≥25.3%) were the most used non-anti-dementia comedications across cohorts (Table 3). Donepezil was the most used anti-dementia medication in the newly diagnosed ADRD (19.1%) and new AChEI users cohort (91.1%).
In the newly diagnosed ADRD cohort, baseline/pre-diagnosis anti-dementia drug use was highest in patients aged 75 to <85 years (28.9%) and lowest in patients aged ≥85 years (20.3%) (Supplemental Table 10). Use of non-dementia comedications was mostly similar across age groups in both newly diagnosed ADRD and new AChEI users cohorts. In the sex-stratified subgroup analysis, only levothyroxine sodium use was more common in females (28.4%–29.4%) than in males (14.5%–15.4%) (Supplemental Table 11). Use of other comedications were generally similar between the sexes.
The rurality-stratified subgroup analysis did not reveal major differences in any anti-dementia drug or comedication use in any cohort (Supplemental Table 12). Patients receiving long-term care in the newly diagnosed ADRD cohort had lower anti-dementia drug use than those not receiving long-term care (9.1% versus 28.3%) (Supplemental Table 13).
Healthcare resource utilization
The newly diagnosed ADRD cohort had a numerically higher proportion of patients with inpatient claims than the new AChEI users cohort (45.9% versus 28.1%) (Figure 2). However, the proportion of ER claims (42.3%–47.8%), and long-term care claims (13.6%–18.4%) was similar. Mean (SD) inpatient days and ER visits in the newly diagnosed ADRD cohort were 13.9 (20.7) and 2.1 (2.2), respectively. On stratification by insurance type, across cohorts, patients with MA insurance type alone had the lowest proportion of inpatient (24.5%–41.4%) and long-term care (10.2%–14.7%) claims, while the proportion of ER claims was similar across insurance types (Figure 2). Mean number of inpatient days and ER visits were also similar across insurance types.
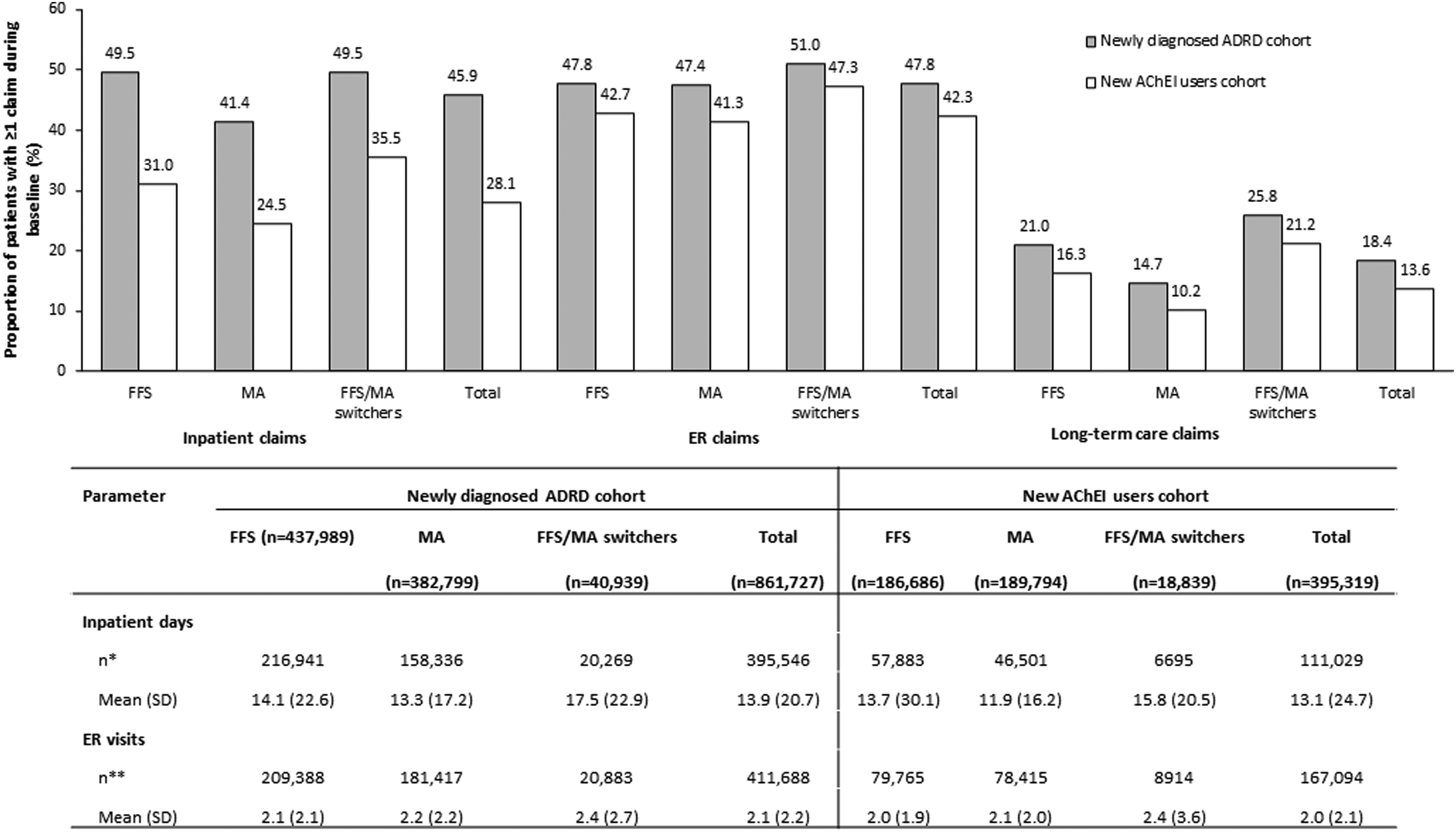
Healthcare resource utilization across cohorts. *Number of patients with an inpatient claim ending during the 12 months baseline (including index day). ** Number of patients with an ER visit ending during the 12 months baseline (including index day). Newly diagnosed ADRD: patients with an ADRD diagnosis; New AChEI users: patients with new use of cholinesterase inhibitors. FFS/MA switchers are patients who have both FFS and MA coverage during the assessment period, but not at the same time. AChEI: acetylcholinesterase inhibitors; ADRD: Alzheimer's disease and related dementias; ER: emergency room; FFS: Medicare Fee-for-Service; MA: Medicare Advantage.
HCRU was similar across the age-stratified and sex-stratified subgroups of the cohorts (Supplemental Figures 1 and 2). In the rurality-stratified subgroup analysis, a numerically higher proportion of patients residing in rural areas had ER claims (48.5%–57.5%) than those residing in non-rural or other rural areas (30.5%–45.7%) (Supplemental Figure 3). However, the mean number of inpatient days and ER visits were similar across the measure of rurality. In the long-term care-stratified subgroup analysis, across both cohorts, a higher proportion of patients receiving long-term care (91.3%–92.2%) had ≥1 inpatient claim and ER claim (65.3%–66.4%) than those not receiving long-term care (18.1%–35.4% and 38.5%–43.8%, respectively) (Supplemental Figure 4). Patients receiving long-term care also had more inpatient days than those not receiving long-term care.
Baseline specialist visits
This analysis was only executed in patients with FFS insurance due to lack of claim-level specialty information in MA claims. A numerically higher proportion of patients had cardiologist visits in the newly diagnosed ADRD cohort than in the new AChEI users cohort (58.1% versus 49.0%) (Table 4). On the other hand, the new AChEI users cohort had a higher proportion of neurologist visits than the newly diagnosed ADRD cohort (44.4% versus 30.3%). All other specialist visits were similar across cohorts.
Baseline specialist visits across cohorts and specialty of healthcare professionals providing the first ADRD diagnosis (FFS only).
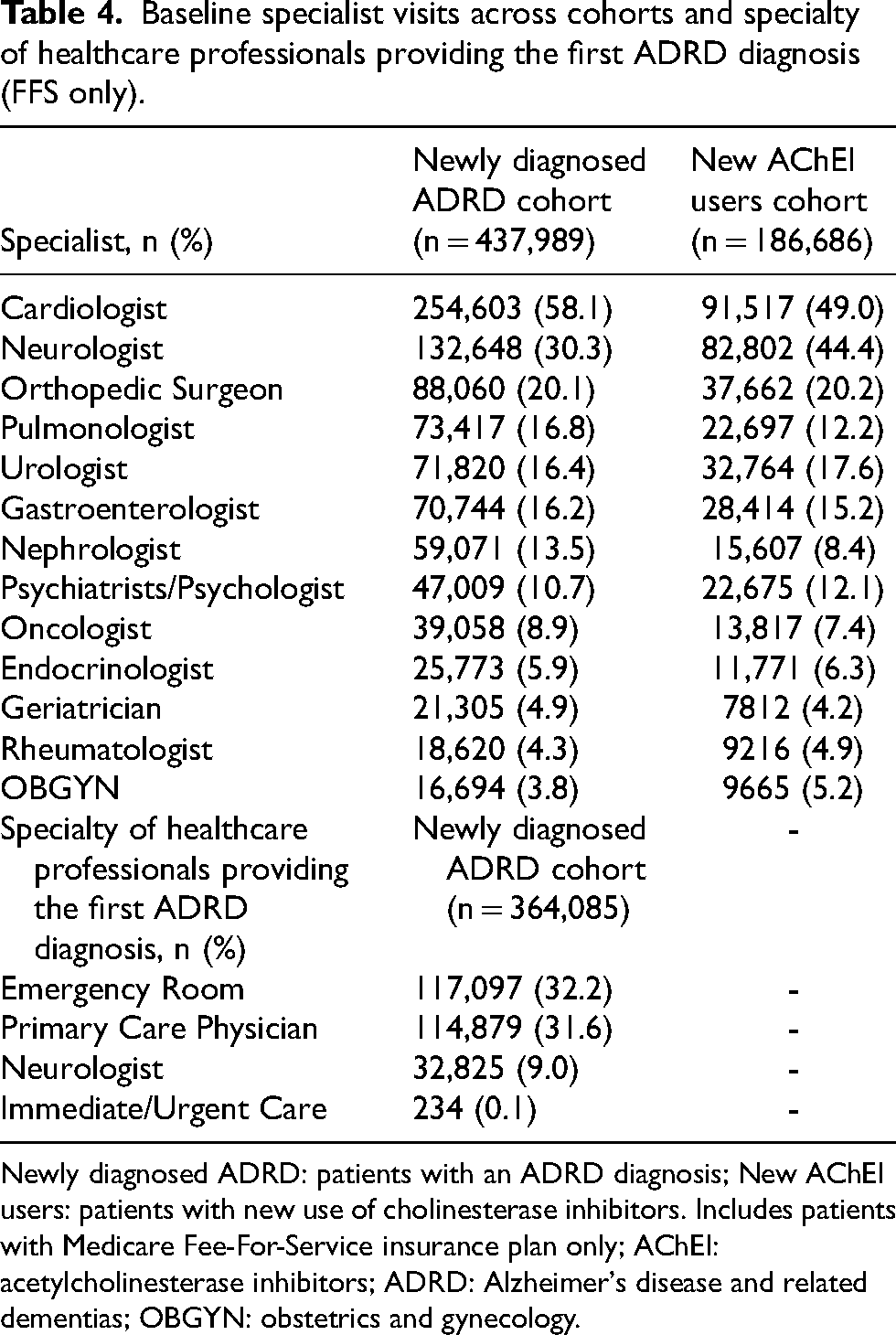
Newly diagnosed ADRD: patients with an ADRD diagnosis; New AChEI users: patients with new use of cholinesterase inhibitors. Includes patients with Medicare Fee-For-Service insurance plan only; AChEI: acetylcholinesterase inhibitors; ADRD: Alzheimer's disease and related dementias; OBGYN: obstetrics and gynecology.
In the age-stratified subgroup analysis, across cohorts, the 65 to <75 years subgroup had the highest proportion of patients with visits to the neurologist (42.8%–53.7%) and psychiatrist/psychologist (17.1%–21.0%) (Supplemental Table 14). The proportion of patients with these visits decreased with increasing age. Other specialist visits were similar across age subgroups.
In the sex-stratified subgroup analysis, across cohorts, males had a numerically higher proportion of visits to cardiologists (54.7%–63.5%), neurologists (35.5%–49.8%), and urologists (29.8%–32.1%) than females (45.5%–55.1%, 27.3%–41.0%, and 8.6%–8.7%, respectively) (Supplemental Table 15). Other specialist visits were similar across the sexes.
Across cohorts, patient visits to specialists were generally highest in non-rural areas (Supplemental Table 16) and among patients receiving long-term care (Supplemental Table 17).
Specialty of the healthcare professional providing the first ADRD diagnosis
As a surrogate for specialty of the diagnosing physician, specialty of the physician listed on the index ADRD claim was assessed. As above, this analysis was only executed in patients with FFS insurance due to lack of claim-level specialty information in MA claims. In addition, this analysis was executed only in the newly diagnosed ADRD cohort as prescription claims (which were the index event for the new AChEi users cohort) do not contain physician specialty information. Patients received the majority of their new ADRD diagnoses either in the ER (32.2%) or by a PCP (31.6%) (Table 4). These PCP diagnoses were most often performed by physicians with an internal medicine specialty (17.7%).
In the age-stratified subgroup analysis, only 5.2% of ≥85-year-old patients received their first ADRD diagnosis from a neurologist compared with 12.9% of 65 to <75-year-old patients (Supplemental Table 14). The sex-stratified (Supplemental Table 15) and rurality-stratified (Supplemental Table 16) subgroup analyses did not show any major differences from the main cohort analysis in the specialty of the HCP providing the first ADRD diagnosis.
In the long-term care-stratified subgroup analysis, patients not receiving long-term care had a numerically higher proportion of PCP-diagnosed or neurologist-diagnosed ADRD diagnoses than those receiving long-term care (33.3% versus 23.8% and 10.0% versus 4.7%, respectively) (Supplemental Table 17).
Sensitivity analyses
Two sensitivity analyses were employed to test the impact of study assumptions. In Sensitivity Analysis #1, the index period was expanded from 1 year to 3 years (January 1, 2017 to December 31, 2019). In Sensitivity Analysis #2, patients with an AChEI claim from 12 months pre-index to −1 day before the index date were excluded (note that Sensitivity Analysis #2 was performed only in the newly diagnosed ADRD cohort as this exclusion was already applied to the new AChEi users cohort). Supplemental Figure 5 and 6 show the selection of patients for Sensitivity Analyses #1 and #2, respectively. Results from the sensitivity analyses were similar to those from the main analysis in terms of demographic characteristics (Supplemental Tables 18 and 19), baseline comorbidities (Supplemental Tables 20 and 21), baseline comedications (Supplemental Tables 22 and 23), HCRU (Supplemental Figures 7 and 8), and baseline specialist visits and specialty of the HCP providing the first ADRD diagnosis (Supplemental Tables 24 and 25), supporting the internal validity of the study results.
Discussion
The current study used two cohorts compiled from Medicare claims data to describe the real-world US ADRD population and for use as a benchmark for generalizability of ADRD clinical trials. The first cohort was selected using the 1-year Bynum-Standard algorithm, a newly validated algorithm to identify patients newly diagnosed with ADRD in Medicare claims. 11 This study also selected an additional cohort of patients based on new AChEI use, a drug class commonly prescribed to patients with dementia symptoms. As patients with ADRD can be difficult to accurately identify in claims data, agreement of results across these two cohorts increases confidence in the internal validity and generalizability of the study findings. Demographic, comorbidity, comedication, and HCRU data have been provided for both cohorts.
The newly diagnosed ADRD and the new AChEi user cohorts were generally similar in all the evaluated parameters, although the AChEi users cohort was, on average, approximately two years younger than the newly diagnosed ADRD cohort. Of important note, 24.7% of patients in the newly diagnosed ADRD cohort had received an anti-dementia drug during the baseline period (i.e., before ADRD diagnosis). This, combined with the older age of patients in this cohort, may indicate that a proportion of patients in the newly diagnosed ADRD cohort had evidence of ADRD prior to receiving their first ADRD diagnosis claim. Furthermore, MCI—which was more prevalent in the new AChEI users cohort (21.7%), possibly due to their younger age—may have served as a precursor to ADRD that manifested as patients aged.
Consistent with previous real-world US studies,4,5,21 patients in the newly diagnosed ADRD and new AChEI users cohorts were more commonly female and the proportion of females increased with increasing age group. It is well known that the risk of AD increases with greater age as shown by Rajan et al. 22 who analyzed the 2020 US census data and reported an increase in the prevalence of clinical AD from 5.3% in 65–74-year-old individuals to 34.6% in ≥85-year-old individuals. In the same study, 1.4 million more females than males had clinical AD. Females generally live longer than males, 23 so the difference in survival may contribute to the greater prevalence of AD in females than in males. 24 Females are also more likely to avoid or delay medical treatment than males due to rising healthcare costs. 25 In the current study, this disparity between males and females was visible in the proportion of patients with visits to neurologists and other specialists. Thus, it is essential to ensure access to AD care, including by specialists, is equitably available to women.
In terms of racial differences, the incidence of AD has been reported to be greater among Black versus White individuals (hazard ratio 1.18; 95% confidence interval 1.16–1.19). 5 The proportion of Black patients with ADRD/dementia in the current study (≤11.1%) is numerically lower than the 18.6% reported in the Chicago Health and Aging Project, 22 suggesting that ADRD is underdiagnosed in Black individuals in the Medicare population. This is in line with an earlier report that 93% of non-Hispanic Black individuals with cognitive impairment consistent with dementia did not have a dementia-related diagnosis, 26 as well as with the Alzheimer's Association observation of AD underdiagnosis in Black individuals. 27 Interestingly, in the current study, the proportion of Black patients in the cohorts was higher in the youngest age subgroup (65 to <75 years: 11.8%–15.9%) than in patients aged 75 to <85 years (9.5%–11.3%) and ≥85 years (8.5%–8.8%). This contrasts previous observations of greater AD diagnosis among older Black patients. 28 The lack of appropriate diagnosis among Black individuals could be attributed to a distrust of medical care, lack of community outreach by physicians, and socioeconomic factors.29,30 Therefore, addressing the aforementioned concerns and then evaluating the racial differences of AD may lead to better insights regarding the etiology of AD or other causes of dementia in Black patients. In line with a recent analysis, 31 in the current study, more Black and Hispanic patients had MA only, or both FFS and MA insurance than FFS only, suggesting that future research on these populations should ensure inclusion of MA insurance type during data source selection. Furthermore, because racial/ethnic disparities exist in dementia treatment and access to appropriate healthcare,32,33 efforts should be made to ensure suitable healthcare access for racial/ethnic minorities.
A high proportion of patients in both cohorts had comorbidities such as hypertension and other cardiovascular disorders and mood disorders, possibly due to the elderly population included in this study. However, cardiovascular disease was more common in the newly diagnosed ADRD cohort than in the new AChEI users cohort, potentially due to the slightly older age of patients in the newly diagnosed ADRD cohort. As shown by the low uptake of AChEIs in the newly diagnosed ADRD cohort (≤19.1%), it is possible that patients with cardiovascular disease in this cohort did not receive AChEI due to their potential for cardiovascular complications. 34 Interestingly, the proportion of patients with diabetes decreased with increasing age. Since advanced age is a known predictor of diabetes mortality, 35 it is possible that ≥75-year-old patients with diabetes died before inclusion in this study. Sex-related differences in circulatory system-related comorbidities, 36 diabetes, 37 bone-related comorbidities, 38 and mood disorders39,40 were consistent with literature.
Interestingly, 32.2% of patients newly diagnosed with ADRD received their first ADRD diagnosis in the ER, with such diagnoses being more common in older patients. These patients may have been brought to the ER because of an event unrelated to ADRD but were diagnosed with ADRD during evaluation. It is possible that emergency care HCPs may not have adequate time to understand patient history in detail and lack appropriate training to diagnose neurodegenerative diseases in an acute care setting, thus making them more likely to incorrectly diagnose ADRD. That said, the 1-Year Bynum standard algorithm utilized to select patients with ADRD for this study required an additional/confirmatory ADRD diagnosis in the outpatient setting, occurring 7–365 days after their incident diagnosis. This suggests that these ER-diagnosed patients with ADRD do have ADRD but, for an unknown reason, were not initially diagnosed in primary care.
A major strength of the current study is the detailed description of the demographics, comorbidities, and medication history of patients with ADRD using the entirety of the Medicare system and including a stratification based on insurance type (FFS only, MA only, and FFS/MA switchers). In addition to understanding representation of relevant ADRD subgroups in clinical trials, this information could be used to understand gaps in diagnosis or treatment between different age, sex, or racial groups and treatment paradigms including where patients are diagnosed.
Limitations
Some limitations apply to this study. Administrative claims, such as Medicare claims, are used for billing purposes; therefore, clinical information insignificant for billing may not be captured. For the purpose of comedication assessment, this study was limited to patients with Part D enrollment, of which 74% of Medicare enrollees were enrolled in 2019. 15 Therefore, results reported in this study cannot be extrapolated to the approximately quarter of Medicare enrollees without Part D coverage. Complex diseases such as ADRD can be difficult to define in administrative claims databases. This reflected in the available algorithms for identifying ADRD. For example, the algorithm used to select the newly diagnosed ADRD cohort in this study 11 had a reported PPV of 70.3%, a sensitivity of 31.3%, and was validated only in FFS claims, not MA claims. Similarly, the algorithm used to select the new AChEI users cohort is expected to have an even lower positive predictive value in the range of 60% with a sensitivity of 30%. 12 However, agreement of results obtained from these two cohorts increases confidence in the study's internal validity. Additional limitations include specialty data availability in the FFS claims only; hence, specialty visit differences between FFS and MA enrollees cannot be ruled out. This study, as is common with claims research, had a limited baseline time period (i.e., 1 year pre-index) and assumed patients with chronic diseases or chronic medication use continue to receive claims for these conditions/medications. However, this may still be different from the “have you ever” questions employed during RCT inclusion/exclusion criteria, thus affecting generalizability to RCTs especially for conditions patients do not routinely seek care for. Moreover, although this study's results could be referred to while designing RCTs for new AD disease-modifying treatments, there are limits to its usefulness since ADRD severity cannot be assessed in claims data.
Conclusion
Extensive understanding of a drug's real-world target patient population can assist with clinical trial design, inform generalizability of clinical trial results, and highlight potential unaddressed risk. This information can be used to understand gaps in diagnosis or treatment between different age, sex, or racial groups and help uncover treatment paradigms including how/where patients are diagnosed with ADRD.
In this study, we used a newly validated claims algorithm to identify patients with newly diagnosed ADRD along with an additional cohort—new AChEI users—and described their characteristics. These results demonstrated that the newly diagnosed ADRD and new AChEI users cohorts were similar in terms of demographic characteristics, comorbidities, comedication use, and HCRU, with only slight differences—supporting the internal validity of our study results. Comparison across the cohorts describes a natural trajectory among patients with ADRD/dementia whereby they may receive an MCI diagnosis, followed by treatment with an AChEI, and ultimately an ADRD diagnosis. This potential delay in receipt of an ADRD diagnosis, as noted by baseline AChEI use and receipt of ADRD diagnoses in the ER, could impact administrative claims research of this population, especially those with early disease, and points to potential gaps in the US healthcare system. This healthcare system-level concern is exemplified by the lower-than-expected proportion of Black and Hispanic patients with ADRD identified in this study. As these minorities are unequally impacted by ADRD, underdiagnosis of ADRD in Black and Hispanic individuals in Medicare is concerning and warrants future research and intervention. Overall, these study results provide a reference for describing the ADRD population in the US and emphasize the importance of evaluating new AD drugs in broad patient populations with comorbidities and concomitant medication use.
Supplemental Material
sj-docx-1-alz-10.3233_JAD-231488 - Supplemental material for Demographics, comorbidities, and comedications in newly diagnosed patients with Alzheimer's disease and related dementias: Findings from United States Medicare claims data
Supplemental material, sj-docx-1-alz-10.3233_JAD-231488 for Demographics, comorbidities, and comedications in newly diagnosed patients with Alzheimer's disease and related dementias: Findings from United States Medicare claims data by Krista M Schroeder, Ana Sofia Afonso, Huabo Wang, Sarah Grace, Adam Phipps and John R Sims in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
Leo J. Philip Tharappel of Eli Lilly Services India Private Limited, Bengaluru, India provided medical writing and editorial support, which was funded by Eli Lilly and Company.
Author contributions
Krista Marie Schroeder (Conceptualization; Investigation; Methodology; Project administration; Resources; Supervision; Writing – original draft; Writing – review & editing); Ana Sofia Afonso (Conceptualization; Investigation; Methodology; Writing – review & editing); Huabo Wang (Data curation; Formal analysis; Writing – review & editing); Sarah Grace (Data curation; Formal analysis; Writing – review & editing); Adam Phipps (Conceptualization; Investigation; Methodology; Writing – review & editing); John R Sims (Conceptualization; Data curation; Investigation; Methodology; Writing – review & editing).
Funding
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This work was supported by Eli Lilly and Company.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Krista M. Schroeder, Ana Sofia Afonso, Adam Phipps, and John R. Sims are employees of Eli Lilly and Company and hold stock and/or stock options in Eli Lilly and Company. Huabo Wang and Sarah Grace are employees of CareJourney. CareJourney served as a paid vendor for Eli Lilly and Company for design and development of the data set for Alzheimer's disease studies.
Data availability
Supplemental material
Supplemental material for this article is available online.