
Abstract
Background:
Recent interest has surged in the locus coeruleus (LC) for its early involvement in Alzheimer’s disease (AD), notably concerning the apolipoprotein ɛ4 allele (APOE4).
Objective:
This study aimed to discern LC functional connectivity (FC) variations in preclinical AD subjects, dissecting the roles of APOE4 carrier status and amyloid-β (Aβ) deposition.
Methods:
A cohort of 112 cognitively intact individuals, all Aβ-positive, split into 70 APOE4 noncarriers and 42 carriers, underwent functional MRI scans, neuropsychological assessments, and APOE genotyping. The research utilized seed to voxel analysis for illustrating LC rsFC discrepancies between APOE4 statuses and employed a general linear model to examine the interactive influence of APOE4 carrier status and Aβ deposition on LC FC values.
Results:
The investigation revealed no significant differences in sex, age, or SUVR between APOE4 carriers and noncarriers. It found diminished LC FC with the occipital cortex in APOE4 carriers and identified a significant interaction between APOE4 carrier status and temporal lobe SUVR in LC FC with the occipital cortex. This interaction suggested a proportional increase in LC FC for APOE4 carriers. Additional notable interactions were observed affecting LC FC with various brain regions, indicating a proportional decrease in LC FC for APOE4 carriers.
Conclusions:
These findings confirm that APOE4 carrier status significantly influences LC FC in preclinical AD, showcasing an intricate relationship with regional Aβ deposition. This underscores the critical role of genetic and pathological factors in early AD pathophysiology, offering insights into potential biomarkers for early detection and intervention strategies.
INTRODUCTION
The apolipoprotein ɛ4 allele (APOE4) significantly influences the pathophysiology of Alzheimer’s disease (AD), with evidence of accelerated cognitive decline, expedited amyloid-β (Aβ) deposition, increased tau phosphorylation, and neuroinflammation in APOE4 carriers [1]. Specifically, APOE4’s impact on regional tau accumulation in preclinical AD patients has come into focus. One study reported that APOE4 affected regional tau accumulation in the entorhinal cortex, amygdala, inferior temporal cortex, inferior parietal cortex, and precuneus [2]. Furthermore, Aβ deposition mediated the relationship between APOE4 and tau accumulation in preclinical AD [2].
The locus coeruleus (LC), the “blue spot,” accumulates hyperphosphorylated tau as early as 30 years of age, marking it as the region with the earliest identifiable AD pathology. Consequently, the LC’s role at the onset of the AD spectrum has been highlighted. Indeed, evidence suggests that LC tau deposition correlates positively with AD progression [3], and disruption of LC integrity precedes cortical tau accumulation in preclinical AD [4]. Additionally, aggregated oligomeric Aβ in the axon terminals of the LC is hypothesized to be early seeding points that could spread and precipitate Aβ plaque formation in the distant brain cortex [5]. Therefore, delineating the intricate interplay between the LC and the cortex, and the impact of Aβ at the nascent stages of AD pathology is crucial for understanding the LC’s role in AD pathology.
Moreover, the association between APOE4 and the LC within the AD spectrum remains unclear. Research utilizing the UK Biobank indicated that APOE4 carriers were at an increased risk of AD, with a 13-fold increase in risk for APOE4 homozygotes [6]. Amyloid positivity in cognitively normal patients raised the risk of AD by 65–104%, and this risk soared to 348% in amyloid-positive APOE4 carriers [7]. APOE4 carriers also exhibited functional connectivity changes that occurred decades before the onset of clinical symptoms, with distinct default mode network connectivity reductions compared to noncarriers [8]. Given the LC’s proposed role in the preclinical phase of AD, considering the influence of APOE4 carrier status on the structural and functional correlates of the LC could enhance our comprehension of how APOE4 impacts AD pathology. Indeed, a recent study demonstrated that APOE4 exacerbated tau toxicity by inhibiting the vesicular monoamine transporter 2 in postmortem AD brains, contributing to norepinephrine toxicity and LC neurodegeneration [9]. These findings imply that APOE4 carrier status may differentially influence the structural and functional integrity of the LC.
Resting-state functional connectivity (RsFC) studies in preclinical AD are recognized for their diagnostic and clinical relevance, as they foreshadow the symptomatic emergence of AD [10] and precede structural changes along the AD trajectory [11]. With the LC being the site of earliest tau deposition, its RsFC with cortical areas in preclinical AD could reflect the incipient pathophysiological changes of AD.
To position the LC as a critical biomarker for tracking AD progression, its validation alongside classical biomarkers, such as APOE4, is essential. Our goal is to elucidate the differences in LC RsFC between APOE4 carriers and noncarriers in preclinical AD (amyloid-positive with normal cognition), accounting for regional Aβ deposition. We hypothesize that disparities exist in LC-cortex FC between APOE4 carriers and noncarriers. Additionally, we anticipate an interaction between APOE4 carrier status and regional Aβ in LC-cortex FC.
METHODS
Participants and clinical assessments
The Brain Health Center at Yeoui-do St. Mary’s Hospital, affiliated with The Catholic University of Korea, recruited 112 individuals with preclinical Alzheimer’s disease between November 2017 and August 2021. Participants were assessed using the Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD-K) [12], which includes cognitive tests such as verbal fluency, the 15-item Boston Naming Test, the Korean edition of the Mini-Mental State Examination [13], word list memory, recall and recognition, constructional praxis, and constructional recall. All participants demonstrated normal cognition, scoring 0 on the global clinical dementia rating (CDR) [14]. Each underwent an amyloid positron emission tomography scan, with methods detailed below, confirming amyloid beta presence. Study exclusion criteria were a history of cerebrovascular events, signs of such lesions, substance abuse, head trauma, mental health disorders, or usage of psychotropic medications. The study conformed to ethical standards from the Institutional Review Board of the Catholic University of Korea and the Declaration of Helsinki. Informed written consent was obtained from all participants.
APOE genotyping
DNA isolation was performed using the QIAmp Blood DNA Maxi Kit by Qiagen, located in Valencia, California. Genotyping for two APOE Single Nucleotide Polymorphisms (SNPs), rs429358 (E4) and rs7412 (E2), was conducted using TaqMan SNP genotyping assays from Applied Biosystems, Foster City, California.
Imaging data acquisition
PET-CT
[18F]-flutemetamol (FMM) production, acquisition, and analysis for FMM-PET adhered to established protocols [15]. This included coregistration and region of interest (ROI) specification, necessary for partial volume effect correction associated with cerebral atrophy. FMM PET data were evaluated using a standardized uptake value ratio (SUVR) at 90 min post-injection, with the pons ROI as a reference. Global Aβ was defined by average SUVR from six cortical ROIs: frontal, superior parietal, lateral temporal, striatum, anterior, and posterior cingulate cortex/precuneus [15]. An SUVR threshold of 0.62 distinguished “high” from “low” neocortical SUVR, with amyloid positivity determined by at least one cortical ROI with an SUVR of 0.62 or higher [15]. All participants were amyloid positive.
MRI
Imaging was conducted at Yeouido St. Mary’s Hospital’s Department of Radiology, The Catholic University of Korea, using a 3T Siemens Skyra with a 32-channel head coil. The T1-weighted magnetization-prepared rapid gradient echo scan sequences had the following parameters: Echo time (TE) = 2.6 ms, repetition time (TR) = 1940 ms, inversion time = 979 ms, field of view (FOV) = 230 mm, matrix = 256×256, and voxel size = 1.0×1.0×1.0 mm3. Resting-state functional images were captured with a multiband gradient-echo EPI technique: TE = 86.0 ms, TR = 3100 ms, slice acceleration factor = 3, slice thickness = 2 mm, FOV = 224 mm, matrix = 128×128×29, and voxel size = 1×1×2 mm3. During the 5 min recording of 150 volumes, patients were instructed to keep their eyes closed and think of nothing in particular, with pre- and post-scan confirmations to ensure wakefulness.
Resting state functional connectivity analysis
Functional imaging data were processed using CONN toolbox Version 20.b. [16]. The standard preprocessing pipeline included realignment, unwarping, slice-time correction, outlier detection, segmentation, normalization, and smoothing with a 4 mm Gaussian kernel. Slice timing information from the DICOM images corrected for slice-time discrepancies. Denoising regressed out physiological noise and movement residuals, with outliers identified by artifact detection tools (ART) included as confounders in the linear regression model. Motion correction, band-pass filtering (0.008–0.09 Hz), and linear detrending were applied.
Voxel-wise seed-based functional connectivity analysis
We used a metaMask for the locus coeruleus (LC) developed by Dahl et al. [17], a composite of six published LC masks. Figure 1 shows the LC overlaied on the Montreal Neurological Institute template. The registration of the template to the data adopted linear registration. LC connectivity maps were calculated for each participant and entered into group-level analysis. ROI-to-ROI analysis assessed correlations between the fourth ventricle and the LC. Whole-brain comparisons employed voxelwise statistics, with a cluster-level false discovery rate (FDR) correction threshold of p < 0.05 and an uncorrected voxel-level threshold of p < 0.001.

The locus coeruleus mask overlaid on the Montreal Neurological Institute template.
Demographic and clinical characteristics of the study participants(N = 112)
*p < 0.05. SD, standard deviation, CERAD-K, the Korean version of Consortium to Establish a Registry for Alzheimer’s Disease; VF, verbal fluency; BNT, 15-item Boston Naming Test; MMSE, Mini Mental Status Examination; WLM, word list memory; CP, constructional praxis; WLR, word list recall; WLRc, word list recognition; CR, constructional recall; SUVRPONS, standardized uptake value ratios of [18F] flutemetamol, with pons as a reference region.; ACC, anterior cingulate cortex; FL, frontal lobes; PL, parietal lobes; PCC, posterior cingulate cortex; TL, lateral temporal lobes.
Statistical analyses
R software (version 4.1.0) [18] conducted the statistical analyses. We compared demographic data, regional/global PET SUVR, and CERAD-K subscores between APOE4 noncarriers and carriers, adjusting for sex and age. Categorical variables underwent chi-square testing. The general linear model included FC as the dependent variable and APOE4 carrier status, global/regional SUVR, and their interactions as independent variables. A two-tailed α level of 0.05 determined statistical significance.
RESULTS
Demographic and clinical data
No significant differences were found in demographic or CERAD-K battery profiles (verbal fluency [VF], Boston Naming Test [BNT]; Mini-Mental State Examination [MMSE]; word list memory [WLM]; constructional praxis [CP]; word list recall [WLR]; word list recognition [WLRc], constructional recall [CR]) between APOE4 noncarriers and carriers. All subjects presented with a global standardized uptake value ratio referenced to the pons (SUVR_PONS) of 0.7±0.1 and were defined as amyloid positive. There was no significant difference in global SUVR_PONS or regional SUVR_PONS between the APOE4 noncarrier and carrier groups.
Difference in LC FC between APOE4 noncarriers and carriers
Table 2 and Fig. 2 illustrate the disparities in locus coeruleus functional connectivity (LC FC) between APOE4 noncarriers and carriers. In APOE4 carriers, there was a significantly reduced LC FC with the right intracalcarine cortex, right lingual gyrus, right occipital fusiform gyrus (+24, –68, –08), left occipital pole, left intracalcarine cortex, left lingual gyrus (–20, –88, –04), left superior division of the lateral occipital cortex, and left occipital pole (–28, –82, +20). The LC FC with the left superior division of the lateral occipital cortex, and left occipital pole (–28, –82, +20) had a negative correlation with anterior cingulate cortex SUVR in APOE4 noncarriers (Supplementary Table 1).
Results from seed-to-voxel analysis (Voxel threshold: p < 0.001, uncorrected, Cluster threshold: p < 0.05, cluster-size p-FDR corrected)
MNI, Montreal Neurological Institute, FDR, false discovery rate.
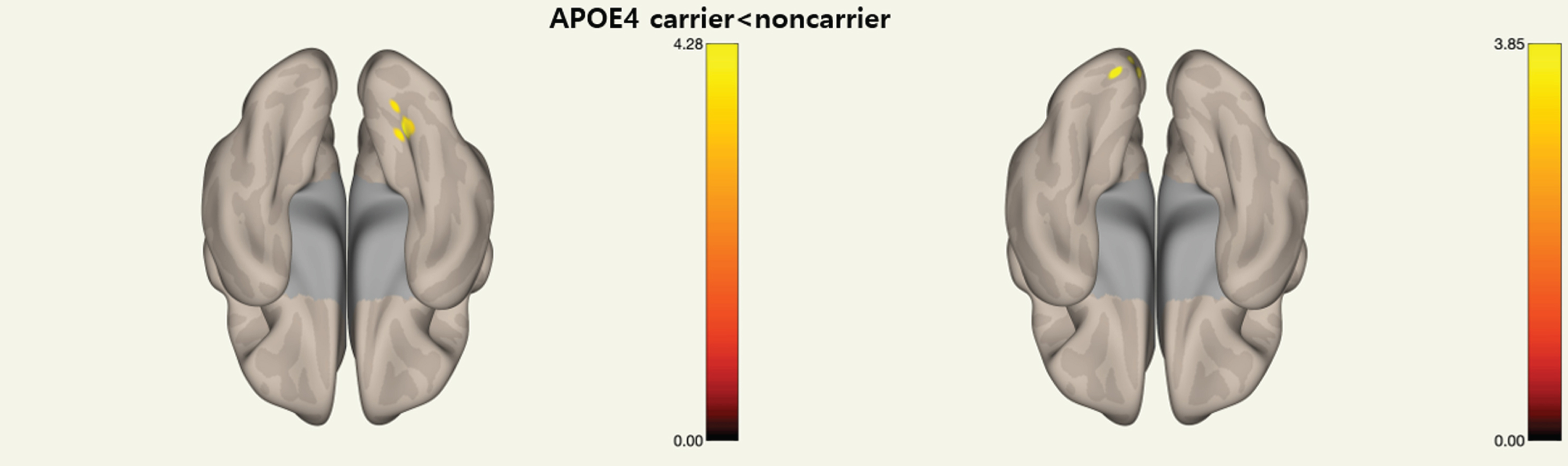
Regions with reduced locus coeruleus functional connectivity in preclinical Alzheimer’s disease with apolipoprotein ɛ4 allele carriers.
Significant APOE4 carrier status by regional and global SUVR interactions
Regions showing a significant APOE4 carrier status by regional SUVR interaction are summarized in Table 2 and Fig. 3. The correlations between LC FC with each regional SUVR and global SUVR in APOE4 noncarrier and carrier group are presented in Supplementary Table 2. A prominent interaction effect was observed between APOE4 carrier status and temporal lobe SUVR (TL SUVR) in the FC of the LC with the superior and inferior subdivisions of the left lateral occipital cortex (–36, –86, +12), with a standardized β coefficient of 1.0032, F = 14.13, adjusted R∧2 = 0.26, and p < 0.01 (Fig. 3a, b). Additionally, significant interactions were found between APOE4 carrier status and global SUVR in the FC of the LC with the left middle frontal gyrus and left frontal pole (–38, +34, +22), with a standardized β coefficient of –0.8817, F = 9.16, adjusted R∧2 = 0.18, and p < 0.01 (Fig. 3c, d), and with the left anterior division of the superior marginal gyrus and left postcentral gyrus (–66, –28, +34), with a standardized β coefficient of –0.7299, F = 7.08, adjusted R∧2 = 0.14, and p < 0.01 (Fig. 3e, f).
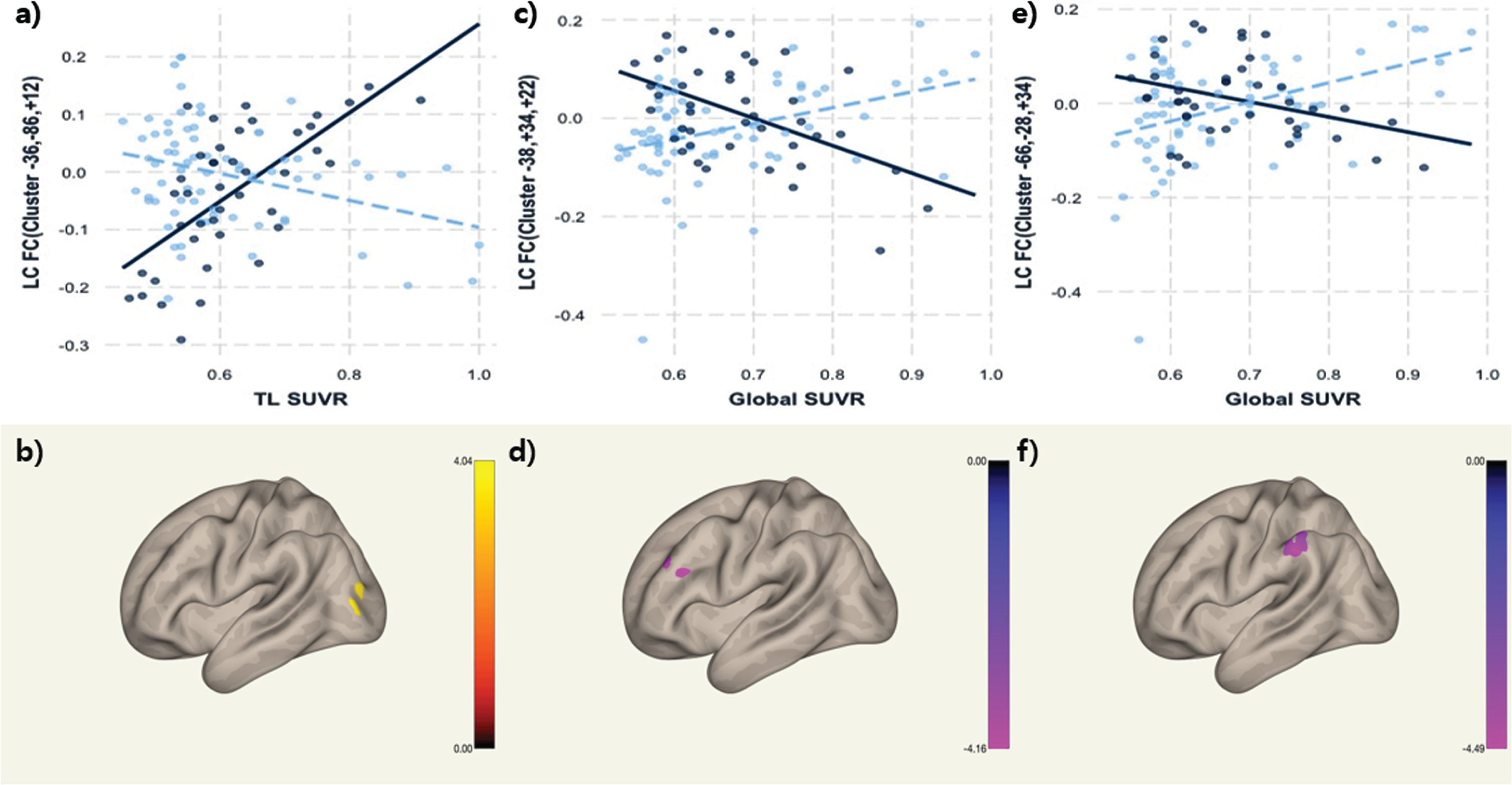
Association of LC FC with the interaction of APOE4 carrier status and regional Aβ deposition (Bold line: APOE4 carrier, Dashed line APOE4 noncarrier, Clusters presented in Montreal Neurological Institute coordinates).
DISCUSSION
To our knowledge, this is the inaugural study examining the impact of APOE4 carrier status on LC functional connectivity (FC) in preclinical AD, amyloid-positive patients with preserved cognition. We observed diminished LC FC with the occipital cortex in APOE4 carriers, alongside notable interactions between APOE4 carrier status and regional/global standardized uptake value ratios (SUVR) within the LC FC across occipital, frontal, and parietal cortices, underscoring significant clinical implications.
Firstly, compared to noncarriers, APOE4 carriers exhibited reduced LC FC with the occipital cortex, complemented by interactions with temporal lobe SUVR. This aligns with prior research illustrating the genotypic effect of APOE4 on resting-state FC in cognitively unimpaired individuals [19]. Our findings of early LC FC alterations with the occipital cortex, exhibiting patterns divergent by APOE4 carrier status, suggest potential early AD markers. A recent report indicated the vascular alpha1A adrenergic receptor of the occipital lobe is resilient to aging or cerebral amyloid angiopathy influences [20], in contrast to the vascular perturbations imparted by APOE4 in AD [21]. This may signify an independent effect of APOE4 on LC FC with the occipital cortex in our cohort. Further, enhanced LC FC with the occipital cortex in APOE4 carriers, in tandem with regional Aβ deposition, resonates with findings from older individuals displaying neuronal hyperactivation as a compensatory response to Aβ accumulation [22].
Secondly, we discerned interactions between APOE4 carrier status and global SUVR on the LC FC with the left middle frontal gyrus and left frontal pole. The LC, known for early tau accumulation, may act as an incipient AD marker, with its integrity presaging disease progression [23]. Postmortem investigations revealed a correlation between neuronal loss in the LC’s caudal segment and Aβ accumulation in the frontal cortex [24]. Normal aging is associated with a decline in LC-frontal FC, potentially linked to heightened distractibility [25]. Our findings suggest that APOE4 carriers may experience diminished frontal inhibitory control over the LC, influenced by global Aβ accumulation.
Thirdly, the interaction between APOE4 carrier status and global standardized uptake value ratios (SUVR) was observed in the LC FC with the left superior marginal and left posterior gyri, which form the somatosensory association cortex. Recent research has highlighted significant masking effects of attention and processing speed on somatosensory dysfunction within the AD progression [26], with this dysfunction manifesting early in the disease course [27]. The processing of somatosensory stimuli in AD is contingent upon the individual’s attentional variability [26]. As previously discussed, the LC is intimately linked with higher-order cognitive processes that necessitate focused attention on relevant stimuli [28]. In APOE4 carriers, an elevation in global SUVR corresponded with a decrease in LC FC with the left supramarginal and postcentral gyri, possibly indicating a disrupted interplay between the LC and the somatosensory network, associated with Aβ deposition. This pathophysiological process may exhibit variations between APOE4 carriers and noncarriers. Supporting this view, reduced FC predominantly in the motor and parietal regions was reported in cognitively normal, amyloid-negative individuals with neurodegeneration [29]. This pattern extended to preclinical AD subjects, with a predominance in the left hemisphere [29], congruent with our findings. Moreover, the postcentral and precentral gyri, essential components of the sensorimotor network, play a vital role in somatosensory integration in AD [30]. The FC between the LC and the somatosensory network could be influenced by APOE4 carrier status. A study involving cognitively intact individuals showed that APOE4 carriers displayed differential resting-state FC (rsFC) in the somatomotor network compared to APOE ɛ2 carriers, with decreased rsFC in the left precuneus and increased rsFC in the left precentral and supplementary motor areas [31]. To date, the supramarginal and postcentral gyri of the parietal cortex have not received as much focus as the posterior cingulate/precuneus network [32]. Future research incorporating the LC, the somatosensory network, and behavioral assessments [33] will be instrumental in deciphering early indicators of AD.
Fourthly, a negative functional connectivity with occipital in APOE4 carriers occurred at lower levels of TL amyloid, but a positive at higher levels of TL amyloid. Meanwhile, for global amyloid, APOE4 carriers exhibited a positive FC with the frontal areas at lower levels of amyloid. This opposite pattern may harbor several implications. For APOE4 carriers, positive FC at lower global amyloid levels might reflect a compensatory mechanism to maintain cognitive function. As amyloid deposition increases, overwhelmed compensatory mechanisms may lead to a breakdown of typical connectivity patterns and shift to negative FC. Moreover, the shift from positive to negative connectivity (or vice versa) with increasing amyloid burden suggest that AD pathology disrupts the normal functioning and coordination of neural networks, which may be more pronounced in APOE4 carriers due to the combined effects of genetic risk and amyloid pathology. Since the LC plays an integral role in arousal and alertness, and is one of the first brain regions to exhibit tau pathology, LC FC changes could reflect underlying neurodegenerative processes affecting neurotransmitter systems and brain network integrity. Moreover, these affected integrity maybe differentially apparent in APOE4 carriers.
This study has several limitations. First, it was a single-center study with a cross-sectional design. Nevertheless, given the challenges associated with recruiting large cohorts for AD trajectory research, our study’s stringent participant classification and substantial sample size bolster the validity of the results. Second, the study lacked an amyloid-negative control group. Third, the inclusion was limited to preclinical AD patients; incorporating individuals with confirmed mild cognitive impairment may have yielded more clinically significant outcomes. Fourth, the study did not provide detailed APOE genotype information or report on gene dose effects. Our investigation, while providing valuable insights into the complexities of Alzheimer’s disease pathology and its association with APOE4 carrier status, acknowledges the nuanced limitation of not incorporating the potential protective effects associated with APOE2 alleles and the gradational impact conferred by the gene dose effects of APOE4. This delineation opens avenues for future research to explore the intricate genetic landscape and its multifaceted influence on neurode pathways. Fifth, methodological limitations such as the use of a relatively large smoothing kernel and the absence of structured physiological noise removal methods (e.g., retrospective image correction, cardiac, or respiratory signal collection) may have impacted the findings. Additionally, the inherent limitations of resting-state functional connectivity (rsFC) studies—namely, their inability to depict structural brain connectivity or quantitatively measure individual mental activity—should not be disregarded. Lastly, we utilized a previously published LC template for localization purposes instead of an MRI sequence sensitive to neuromelanin.
Conclusions
This study is among the few to elucidate the distinct LC FC patterns between APOE4 carriers and noncarriers in the context of preclinical AD. Notably, significant interactions were observed between regional and global amyloid PET SUVR and APOE4 carrier status across various brain regions. These findings contribute to a deeper understanding of the relationship between the LC and APOE4 during AD progression. Future research incorporating multimodal approaches—including neuroimaging, neuropsychological testing, behavioral assessments, and blood biomarkers such as plasma tau and Aβ—will likely clarify the pivotal role of the LC and APOE4 in AD.
AUTHOR CONTRIBUTIONS
Yoo Hyun Um (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Visualization; Writing – original draft; Writing – review & editing); Sheng-Min Wang (Investigation; Writing – review & editing); Dong Woo Kang (Investigation; Writing – review & editing); Sunghwan Kim (Data curation; Formal analysis; Resources); Chang Uk Lee MD (Validation; Writing – review & editing); Donghyeon Kim (Validation; Writing – review & editing); Yeong Sim Choe (Validation; Writing – review & editing); Regina EY Kim (Validation; Writing – review & editing); Soyoung Lee (Conceptualization; Validation; Writing – review & editing); Min-Kyung Lee (Methodology; Validation; Writing – review & editing); Hyun Kook Lim, M.D., Ph.D. (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Supervision; Validation; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
FUNDING
This research was supported by Culture, Sports and Tourism R& D Program through the Korea Creative Content Agency (KOCCA) grant funded by the Ministry of Culture, Sports and Tourism (MCST) in 2022 (Project Name: Development of game-based digital therapeutics technology to treat mental disease, Project Number: R2022020030, Contribution Rate: 100%). This research was supported by Basic Medical Science Facilitation Program through the Catholic Medical Center of the Catholic University of Korea funded by the Catholic Education Foundation.
CONFLICT OF INTEREST
Hyun Kook Lim is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.