
Abstract
Post-stroke cognitive impairment and dementia (PSCID) is a complication that affects long-term functional outcomes after stroke. Studies on dementia after long-term follow-up in stroke have focused predominantly on ischemic stroke, which may be different from the development of dementia after spontaneous intracerebral hemorrhage (ICH). In this review, we summarize the existing data and hypotheses on the development of dementia after spontaneous ICH, review the management of post-ICH dementia, and suggest areas for future research. Dementia after spontaneous ICH has a cumulative incidence of up to 32.0–37.4% at 5 years post-ICH. Although the pathophysiology of post-ICH dementia has not been fully understood, two main theoretical frameworks can be considered: 1) the triggering role of ICH (both primary and secondary brain injury) in precipitating cognitive decline and dementia; and 2) the contributory role of pre-existing brain pathology (including small vessel disease and neurodegenerative pathology), reduced cognitive reserve, and genetic factors predisposing to cognitive dysfunction. These pathophysiological pathways may have synergistic effects that converge on dysfunction of the neurovascular unit and disruptions in functional connectivity leading to dementia post-ICH. Management of post-ICH dementia may include screening and monitoring, cognitive therapy, and pharmacotherapy. Non-invasive brain stimulation is an emerging therapeutic modality under investigation for safety and efficacy. Our review highlights that there remains a paucity of data and standardized reporting on incident dementia after spontaneous ICH. Further research is imperative for determining the incidence, risk factors, and pathophysiology of post-ICH dementia, in order to identify new therapies for the treatment of this debilitating condition.
Keywords
INTRODUCTION
Post-stroke cognitive impairment and dementia (PSCID) is increasingly recognized as a complication that influences long-term functional outcomes after stroke [1–8]. The pathophysiology of PSCID involves a complex interplay between pre-incident cognitive reserve, the characteristics of incident stroke, and accumulation of neurodegenerative and small vessel disease pathology in the brain [8]. Ongoing prospective cohorts have been established to further elucidate the pathophysiology and trajectories of cognitive decline [9, 10], as well as to predict and intervene early to prevent cognitive deterioration after stroke [11].
However, existing international literature focused predominantly on ischemic stroke, and even in studies that recruited both ischemic and hemorrhagic stroke patients, the number of patients with intracerebral hemorrhage (ICH) are small [12–14]. As the underlying pathology of acute ischemic stroke and spontaneous intracerebral hemorrhage are different, the pathophysiology and cognitive trajectories of PSCID are likely to be different as well. Although the pathophysiology of post-ICH dementia has not been fully understood, two main theoretical frameworks can be considered: 1) the triggering role of ICH in the genesis of cognitive decline and dementia [15–20], and 2) the contributory role of pre-existing brain pathology, reduced cognitive reserve, and genetic factors that predispose to cognitive dysfunction [4, 21–25]. These pathophysiological pathways may have synergistic effects that converge on dysfunction of the neurovascular unit and disruptions in functional connectivity leading to PSCID [8].
The concept of the neurovascular unit (NVU) was first introduced at the Stroke Progress Review Group meeting of the National Institute of Neurological Disorders and Stroke [26] in 2001, and expanded upon in Iadecola’s seminal paper in 2017 [27]. Composed of neurons, astrocytes, microglia, endothelial cells, smooth muscle cells and pericytes [27, 28], the NVU is responsible for maintenance of the blood-brain barrier (BBB) and cerebral homeostasis, as well as regulation of cerebral blood flow [29]. Dysfunction of the NVU and the neurovasculome is thought to underlie various pathogenic mechanisms of PSCID [8].
As the pathophysiology of PSCID after spontaneous ICH remains poorly understood, we aim to review the existing data and hypotheses, including the role of pre-existing brain pathology, cognitive reserve, and the spontaneous ICH event on dysfunction of the NVU and subsequent PSCID. In addition, we review the advances in the management of PSCID after spontaneous ICH and suggest areas for future research.
THE ROLE AND CHARACTERISTICS OF SPONTANEOUS ICH ON THE DEVELOPMENT OF DEMENTIA
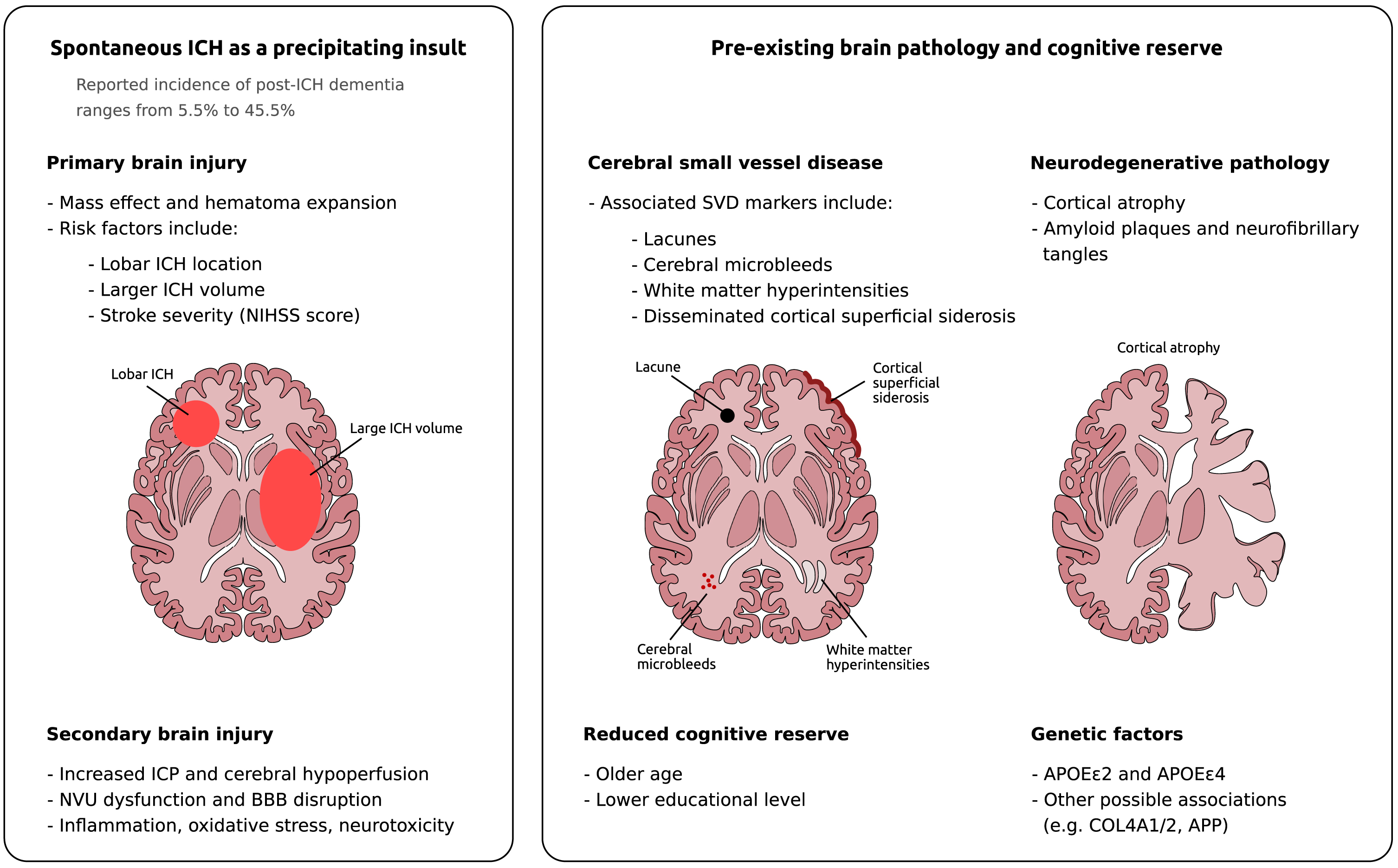
The most common etiology of spontaneous ICH is vascular risk factor-related arteriosclerotic microangiopathy, which results in lipohyalinosis and vessel wall weakening (most commonly occurring in the lenticulostriate arteries) [30], and cerebral amyloid angiopathy (CAA), which results in amyloid deposition weakening the cortical and leptomeningeal arteries [31, 32]. During spontaneous ICH, vessel wall rupture results in an expanding hematoma that causes the primary brain injury [20, 33]. Subsequently, an ensuing cascade of events leads to secondary brain injury, including 1) local increase in intracranial pressure (ICP) leading to cerebral hypoperfusion [15], 2) disruption of the NVU and BBB resulting in increased perilesional edema [16, 17], as well as 3) an inflammatory cascade resulting in increased oxidative stress and neuronal cell death [18, 19]. In this section, we review the existing data on the incidence of dementia and cognitive trajectories after spontaneous ICH, as well as the characteristics of the ICH that contribute to the pathophysiological cascade outlined above.
Incidence of dementia and cognitive trajectories after spontaneous ICH
Overall, the incidence of post-ICH dementia has been reported to range from 5.5% to 45.5% across all time points (Table 1) [4–6, 34–43]. The largest studies to date investigating post-stroke dementia after ICH include Biffi et al. (2016) [4], Moulin et al. (2016) [5], and Pasi et al. (2021) [22]. These and other prospective cohort studies [4, 44] demonstrated the incidence of early dementia (onset within 6 months after ICH) to be 19.0% [4], and the incidence of delayed dementia (onset≥6 months after ICH) to be 14.2% at 1 year [5], 19.8% at 2 years [5], 24.5% at 3 years [5], 28.3% to 35.0% at 4 years [5, 22], and 32.0% to 37.4% at 5 years post-ICH [21, 39] (Table 1). The rationale for assessing the development of post-ICH dementia after 6 months [4, 21] was to preclude confounding from factors related to acute neurological injury in the acute phase post-ICH [5].
Summary of selected articles reporting incidence of dementia after intracerebral hemorrhage
DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; NINDS-AIREN, National Institute of Neurological Disorders and Stroke and Association Internationale pour la Recherché et l’Enseignement en Neurosciences; VaD, vascular dementia; ICD-10, International Classification of Diseases, Tenth Revision; NINCDS-ADRDA, National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association; AD, Alzheimer’s disease; DSM-IV-TR, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision; ICD-9, International Classification of Diseases, Ninth Revision; TICS-m, Modified Telephone Interview for Cognitive Status; NIA-AA, National Institute on Aging and Alzheimer’s Association; VASCOG, The International Society for Vascular Behavioral and Cognitive Disorders; VCD, vascular cognitive disorder; MMSE, Mini-Mental State Examination. *Did not exclude pre-existing cognitive impairment or dementia. †Same study cohort but different date range.
However, there remains limited good quality long-term follow-up examining the trajectory of cognitive decline or the cognitive domains that are affected after ICH [9]. Recent reviews [12, 13] found that after spontaneous ICH, cognitive domains in information processing speed, executive function, memory, language, and visuospatial abilities were commonly affected [45–47]. However, such data was inconsistent across studies and had variable follow-up durations, which preclude a detailed analysis of domain-related cognitive deterioration after spontaneous ICH. This is an Important area for future research In PSCID after spontaneous ICH.
Pathophysiology and characteristics of spontaneous ICH that contribute to incident dementia
Characteristics of the hematoma that were shown to increase the risk of post-ICH dementia include lobar location of ICH [4, 5] and larger ICH volume [4] (Fig. 1). Lobar ICH likely disrupts cortical network connectivity leading to cognitive dysfunction after stroke [4, 5], while larger hematoma volume could cause greater mass effect and increased secondary injury after ICH [20, 48]. Clinically, the severity of stroke as measured by the National Institutes of Health Stroke Scale (NIHSS) score has been shown to increase risk of incident dementia after ICH [5, 6], with NIHSS score > 10 bringing forward dementia by around 25 years among stroke survivors (including both ischemic and hemorrhagic stroke) [6].
After spontaneous ICH, high ICP and cerebral hypoperfusion [49] leads to NVU dysfunction (via metabolic stress) [50] and cerebral ischemia, which has been shown to increase the risk of cognitive decline and dementia [15, 52]. Disruption of the BBB may reduce the clearance and increase the production of amyloid beta [53, 54], as well as allow neurotoxic plasma proteins (fibrinogen, plasminogen, thrombin etc.) to enter the brain, accelerating neuronal injury and neurodegeneration, even in the absence of amyloid-β [27, 55]. Lastly, the release of molecules such as hemoglobin, iron, and thrombin from the hematoma results in inflammation, oxidative stress, and neurotoxicity following ICH [18–20]. Sweeney et al showed that thrombin leads to the activation of protease-activated receptor-1 (PAR-1) on astrocytes, which decreased glutamatergic receptors and impaired long-term plasticity [56]. These pathophysiological pathways converge on disruptions in functional connectivity in the brain, which may then manifest phenotypically as cognitive impairment and dementia [8, 57–59].
THE ROLE OF PRE-EXISTING BRAIN PATHOLOGY AND COGNITIVE RESERVE ON THE DEVELOPMENT OF DEMENTIA AFTER SPONTANEOUS ICH
Pre-existing brain pathology associated with spontaneous ICH as well as poor cognitive reserve contribute to PSCID after ICH [9, 60]. These factors include small vessel disease and neurodegenerative pathology as well as genetic risk factors (Fig. 1). This section reviews the current evidence on these pre-existing factors and how they contribute to the development of dementia after spontaneous ICH.
Previous stroke or transient ischemic attack, as well as imaging biomarkers of cerebral small vessel disease, including lacunes, cerebral microbleeds, white matter hyperintensities (WMH), and disseminated cortical superficial siderosis (cSS), were significant risk factors for post-ICH dementia [4, 22] (Fig. 1). These cerebral small vessel disease markers have all been associated with dementia [61–64]. The mechanisms by which they affect cognition remain incompletely understood, but has been hypothesized to be due to network disruption and tissue damage [65–67], their association with vascular pathology predisposing to vascular and mixed dementia [66, 68], as well as contribution to amyloid deposition and Alzheimer’s disease pathology [55, 70]. Neurodegenerative pathology such as cortical atrophy, amyloid plaques and neurofibrillary tangles have also been implicated in the development of dementia after stroke [5, 23–25]. Rost et al. proposed that there may be synergistic effects between stroke, small vessel disease, and neurodegenerative lesions [8]. For instance, WMHs potentially play an additive role in Alzheimer’s disease pathogenesis by contributing to amyloid plaques and neurofibrillary tangles [55, 70], thereby lowering the threshold for the clinical expression of dementia [71, 72].
Demographic risk factors for post-ICH dementia include older age at index ICH [4–6] and lower educational level [4], which are reflective of reduced cognitive reserve [73] (Fig. 1). Individuals with reduced cognitive reserve are less able to withstand age-related and disease-related changes in the brain [74–76], including a spontaneous ICH event. Stern et al. [73] hypothesized that these individuals have brain networks with lower efficiency and capacity, and can tolerate less damage to existing networks before performance was affected (i.e., neural reserve); additionally, they are less able to recruit alternative networks to compensate (i.e., neural compensation). Mortimer [77] suggested that, given that Alzheimer’s disease pathology can be present in the brain without clinical symptoms [78, 79], having reduced cognitive reserve (e.g., lower educational attainment) may lower the threshold for the manifestation of clinical symptoms of dementia, after an insult to the brain such as ICH.
Genetic factors may also predispose to post-ICH dementia (Fig. 1). Biffi et al. found that apolipoprotein E (APOE) ɛ2 and ɛ4 genotypes were prognostic factors for early and late development of post-ICH dementia, respectively [4]. The APOE ɛ2 allele was associated with larger hematoma volume and hematoma expansion after primary ICH [39, 80], while both the APOE ɛ2 and APOE ɛ4 alleles were associated with increased risk of lobar ICH [81, 82]. These alleles were shown to increase cerebral vascular amyloid deposition, concentric vessel splitting and fibrinoid necrosis, predisposing to vessel rupture [83]. Apart from the APOE gene, mutations in the amyloid precursor protein (APP) gene were shown to increase vascular accumulation of amyloid beta, and represent the most common cause of hereditary CAA, which can manifest with spontaneous ICH [84, 85]. APP mutations can also cause early-onset Alzheimer’s disease as a result of amyloid beta neurotoxicity [86].
The two theoretical frameworks (spontaneous ICH as a precipitating insult, as well as pre-existing brain pathology and/or reduced cognitive reserve) are likely synergistic in contributing to post-ICH dementia pathophysiology [4, 28]. The development of dementia after spontaneous ICH is likely precipitated by cerebrovascular injury and inflammation from the hemorrhagic event [15–20], and predisposed by poor cognitive reserve and pre-existing pathological changes reflective of cerebral small vessel disease and/or neurodegeneration [4, 21–25]. Pathologic processes that cause NVU dysfunction are at play in both hypotheses [8], and could represent converging pathogenic pathways [27, 28]. Further research into the pathways that lead to PSCID after ICH are required and may potentially provide insight into prevention and treatment of PSCID in the future.
EVALUATION AND MANAGEMENT OF DEMENTIA AFTER SPONTANEOUS ICH
The 2022 American Heart Association/American Stroke Association (AHA/ASA) guidelines [87] recommended that in patients with spontaneous ICH, the administration of a cognitive screening tool in the post-acute period is useful to identify patients with cognitive impairment and dementia [88] (Fig. 2). The Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Rotterdam Cambridge Cognitive Examination (R-CAMCOG), and Addenbrooke’s Cognitive Examination –Revised (ACE-R) all demonstrated similar accuracy in detecting cognitive impairment and dementia in stroke patients [88]. The choice of screening tool may be determined based on feasibility, clinical setting, patient demographics, pre-test probability of cognitive impairment, and the patient’s clinical condition including the presence of other ICH-related impairments [87, 89]. Neuropsychological assessment (involving the evaluation of multiple cognitive domains, e.g., attention, verbal and visual episodic memory, language, visuospatial skills, executive function, etc.) may be useful in both identifying dementia as well as characterizing its severity and clinical features, which could inform therapeutic recommendations and care planning [90–92]. Additionally, a validated screening tool for depression should be used to exclude pseudodementia, and depression should be treated if present [87, 94].
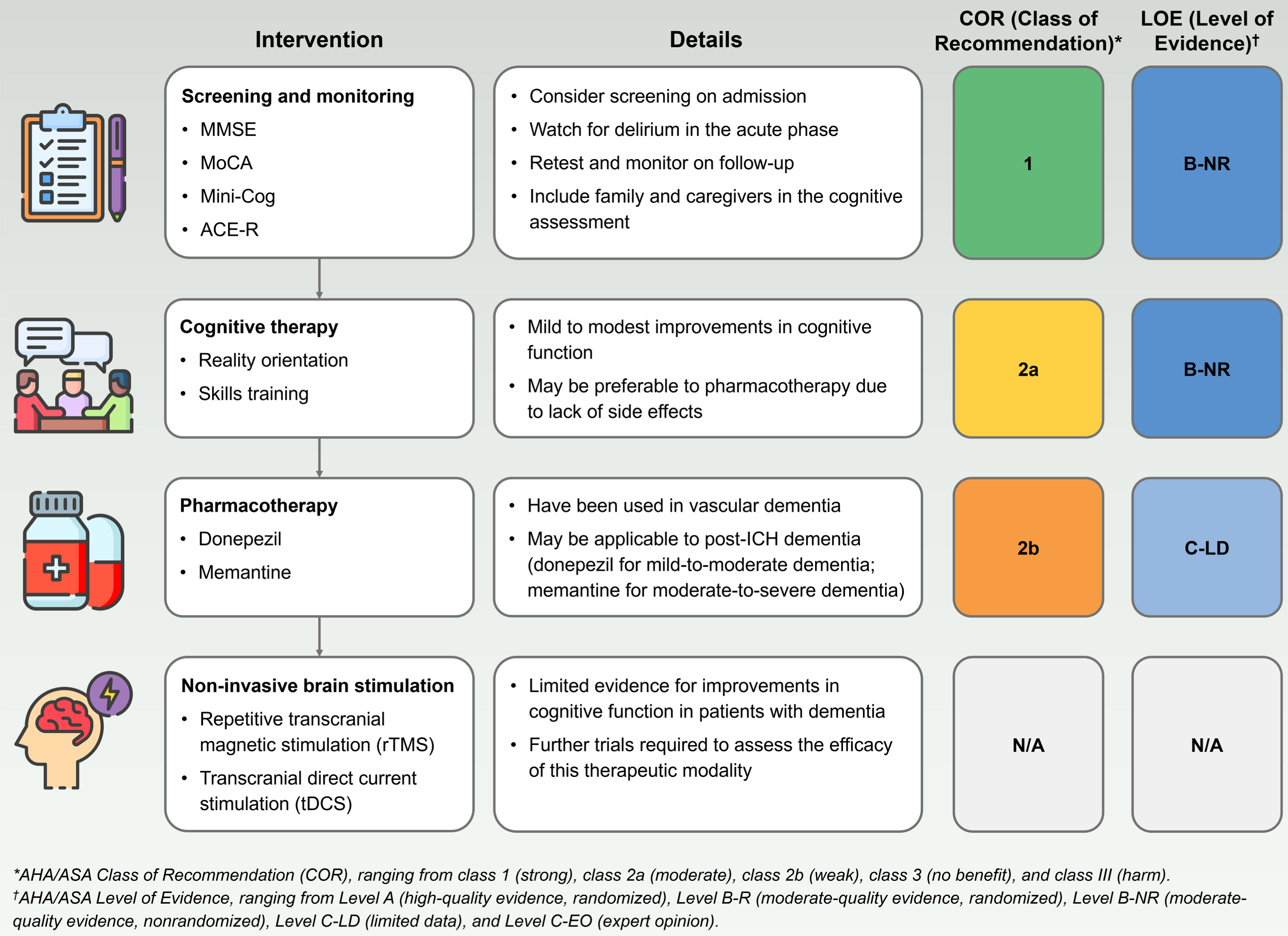
The patient’s family and caregivers should be included in the cognitive assessment [87]. This is because both overreporting (due to factors such as heightened psychological distress [95, 96]) and underreporting (due to factors such as anosognosia, where the patient is unaware of their cognitive deficits [97]) of cognitive impairment may occur after ICH. The effectiveness of different screening strategies in patients with ICH (including which patients to screen, as well as the timing and frequency of screening) has not been evaluated in prospective clinical trials. As there is evidence of delayed dementia after ICH [4, 21], retesting and monitoring cognitive function after ICH may be useful on long-term outpatient follow-up [87].
In terms of therapy, non-pharmacological, pharmacological, and interventional modalities have been used (Fig. 2). Cognitive therapy is largely theoretically driven and involves standardized exercises targeting specific cognitive functions in order to optimize cognition and daily functioning [98]. In patients with post-stroke dementia, several meta-analyses have shown benefits of cognitive therapy in the improvement of memory deficits [99], attention deficits [100], and executive dysfunction [101], with limited evidence in post-ICH dementia specifically. Given the potential benefits and lack of adverse effects, it is reasonable to refer patients with post-ICH dementia for cognitive therapy [87].
No pharmacotherapeutic trials have been conducted to investigate the treatment of post-ICH dementia specifically. Donepezil, a cholinesterase inhibitor, has been shown to improve cognitive function and activities of daily living (ADLs) in patients with vascular cognitive impairment [102, 103], while memantine, an NMDA receptor antagonist, has been found to enhance cognitive function, behavior, and mood in vascular dementia [104]. Given the clinical evidence supporting the use of these pharmacological therapies, it may be reasonable to consider using cholinesterase inhibitors for mild to moderate dementia and memantine for moderate to severe dementia after ICH [87].
Recently, non-invasive brain stimulation (NIBS), including repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS) have emerged as potential treatment modalities for patients with dementia [105]. Several meta-analyses have reported significantly improved memory and cognitive function in patients with dementia treated with rTMS [106, 107] and tDCS [108] compared to sham treatment. However, despite promising results, interim analysis of a large multi-center double-blind randomized controlled trial demonstrated no significant difference in cognitive function scores between patients receiving rTMS and sham treatment [109]. There is a need for future large-scale, controlled studies to assess the efficacy of NIBS for patients with dementia as well as post-ICH dementia specifically.
In addition, post-ICH dementia should be managed in the context of other related complications. Post-stroke cognitive impairment is associated with sleep disorders, depression, personality and behavioral changes, and other neuropsychological changes, all contributing to a lower quality of life [110]. Neuropsychiatric symptoms found in patients post-ICH include affective symptoms, vegetative symptoms, hyperactivity, apathy, and psychosis, with higher risk in the subgroup with post-ICH dementia [111]. In patients with dementia after ICH, it is imperative to also address these complications and aim to improve quality of life for optimal and holistic patient care. Lastly, in terms of prevention, controlling vascular risk factors is essential to prevent the progression to dementia in patients after spontaneous ICH [7, 112].
CONCLUSION
Incident dementia after spontaneous ICH is relatively common, with a cumulative incidence of up to 32.0–37.4% at 5 years post-ICH. The development of dementia after spontaneous ICH is likely precipitated by primary and secondary brain injury from the hemorrhagic event, and predisposed by pre-existing pathology including cerebral small vessel disease and/or neurodegeneration, as well as reduced cognitive reserve and potentially genetic factors. These pathways converge on NVU dysfunction and disruptions in functional connectivity leading to dementia post-ICH. Management of post-ICH dementia may include screening and monitoring, cognitive therapy, and pharmacotherapy. Non-invasive brain stimulation is an emerging therapeutic modality currently still under investigation for its safety and efficacy.
Our review highlights that there remains a paucity of data specifically on incident dementia after spontaneous ICH. Additionally, methodological heterogeneity of previous studies may limit the accurate determination of the incidence and risk factors of dementia after spontaneous ICH. Further research is imperative for determining the incidence, risk factors, and pathophysiology of dementia after spontaneous intracerebral hemorrhage, in order to identify new therapies for the treatment of this debilitating condition.
AUTHOR CONTRIBUTIONS
Zheting Zhang (Conceptualization; Data curation; Formal analysis; Methodology; Writing – original draft; Writing – review & editing); Mervyn Jun Rui Lim (Conceptualization; Data curation; Formal analysis; Methodology; Supervision; Writing – original draft; Writing – review & editing).