
Abstract
Background:
The association between COVID-19 infection and the onset of dementia among adults 65 years and older has the potential to increase the burden of dementia worldwide significantly. Our research, which focuses on understanding the likely increase in the burden of dementia due to COVID-19 infection in the USA, has crucial public policy implications. By providing these insights, we aim to empower policymakers, healthcare professionals, researchers, and public health officials to make informed decisions and plan for the future.
Objective:
Project the prevalence of dementia in the United States while accounting for the impact of COVID-19 infection on the onset of dementia.
Methods:
A dynamic multi-state population model was developed. The model was initialized with USA demographic data and estimates of age, gender, and race-specific transition rates from the Health and Retirement Study (HRS).
Results:
The projected increase in the burden of dementia among Americans 65 years and older is a staggering 14.838 million by 2050. However, due to the COVID-19 pandemic, we anticipate an additional 265,000 to 677,000 older adults 65 years and older will be affected by dementia. This will escalate the burden of dementia to a potential 15.103 million to 15.515 million by 2050, a significant human toll that we must be prepared for.
Conclusions:
The projected dementia numbers underscore the urgent need for policy and intervention in social care services and healthcare needs planning. This includes providing robust support systems for caregivers and ensuring the healthcare staff is adequately trained to meet the healthcare needs of dementia patients and their families.
INTRODUCTION
Dementia is a progressive deterioration of cognitive function, mainly caused by Alzheimer’s disease (AD). As the number of Americans 65 years and older is estimated to increase from 55 million in 2019 to 88 million by 2050, 1 the number of Americans living with dementia is also expected to grow significantly. Common risk factors for dementia include early life risk (i.e., education), midlife risk (i.e., hypertension, obesity, hearing loss, traumatic brain injury, and alcohol misuse), and later life risk (smoking, depression, physical inactivity, social isolation, diabetes, and air pollution). 2 The number of people with dementia is rising, and predictions about future trends in dementia prevalence vary depending on the underlying assumptions.
The impact of COVID-19 on cognitive function and its potential connection to neurodegenerative diseases like AD has garnered significant attention. Research after the COVID-19 pandemic showed that respiratory and gastrointestinal symptoms are accompanied by short- and long-term neuropsychiatric symptoms and long-term brain sequelae. 3 There is evidence of an increased risk of AD after a COVID-19 diagnosis due to the inflammatory effects of COVID-19 that play a role in AD. 4 Examining brain lysates from control and COVID-19 patients, researchers found evidence of increased activation of TGF-β signaling and increased tau phosphorylation, typically associated with AD, also seen in COVID-19 patients. 5 In another study of 41 autopsies of COVID-19 patients, hypoxic damage and microglial activation were found in the brain, along with elevated inflammatory markers, which are associated with cognitive defects. However, the low levels of detectable virus in the brain suggest that these effects arose from inflammation, not direct infection. 6 In a clinical study, the presence of known plasma biomarkers associated with AD, neurodegeneration, and neuroinflammation in older patients who were hospitalized with COVID-19 were examined. The results showed that t-tau, Nfl, GFAP, and UCH-L1 levels were higher in COVID-19 patients with neurological symptoms than those without. 7 A systematic review of the literature on COVID-19-associated cognitive impairment by Junior et al. found that it occurs not only in severe cases but also in those with an acute disease phase. 8 A prospective observational cohort study by Rass et al. looked at the neurological outcome three months after COVID-19 and found evidence of cognitive impairment in 23% of COVID-19 patients (29% in severe COVID-19 patients, 30% in moderate, and 3% in mild). 9 Vavougios et al. studied hospitalized patients with mild to moderate COVID-19 disease and found that 56.2% presented with cognitive decline according to the Montreal Cognitive Assessment test. 10 These various studies examining markers of ADs and inflammatory effects in patients post-COVID-19 infection suggest there may be some connection between COVID-19 and dementia. For this research, we hypothesize that older adults 65 years and older who had COVID-19, experienced mild to severe symptoms from the COVID-19 infection, and have mild cognitive impairment (diagnosed or undiagnosed) would have an increased risk of progression to dementia.
While the reported cases of COVID-19 in America was around 103 million, 11 a nationwide blood donor survey from the CDC that looked at the percentage of people with antibodies against COVID-19 estimates the infection-induced seroprevalence to be approximately 77.5% of Americans. 12 Given this staggering number of COVID-19 cases in America and its association with dementia, there is a need to quantify the likely future burden of dementia, prepare for the rise in dementia cases, and explore interventions to delay or reduce the onset of dementia. Evidence-based projection of dementia facilitates the understanding of the future burden of dementia and the resources required to provide health and social care for individuals with dementia effectively. As of 2019, it is estimated that the United States (US) had only half the number of geriatric professionals needed. 1 In 2019, the estimated economic burden of dementia was $290 billion in health care, long-term care, and hospice. 1 An aging population with increased dementia cases will lead to a significant increase in this already substantial health and social care cost. Understanding the future projection of the dementia burden can also incentivize more research into its prevention, treatment, and preparedness for health and social care needs. The FINGER research study in Finland investigated the effectiveness of multidomain lifestyle interventions in diet, exercise, cognitive training, and managing cardiovascular disease risk over two years, with control visits at five, seven, and eleven years post-intervention. The results showed that the intervention group had improved cognitive levels, regardless of genetic or baseline risk factors. 13 A similar clinical trial called the US Pointer trial is being conducted in the US to investigate if lifestyle interventions can protect cognitive function in individuals identified at increased risk for cognitive decline. 14 Further research into early intervention for dementia in the US population is of the utmost importance as the burden of dementia continues to rise substantially. In light of these previous studies, this paper aims to use age, gender, and race-specific transition rates and the recent data on the effect of COVID-19 on dementia onset to create an evidence-based projection of the number of older adults aged 65 and older in America with dementia.
METHODS
A dynamic multi-state population model 15,16 was developed to project the burden of dementia and the impact of the COVID-19 pandemic on dementia onset among older adults 65 years and older in the US. The model required standard demographic data and estimates of the transition to dementia. Demographic data were obtained from the National Vital Statistics report, and the transition rates were obtained from the Health and Retirement Study (HRS). 17
Dynamic multi-state population model
As shown in Fig. 1, the dynamic multi-state population model is a system dynamics model 18,19 with explicit health states. System dynamics models have been widely used to investigate the burden of chronic illnesses such as cardiovascular diseases, 20,21 dementia, 16 diabetes, 22 and chronic kidney diseases. 23,24 For the dementia model, the US population was disaggregated into three states: population under 65 years, population 65 years and older with no dementia, and population 65 years and older with dementia. Each state’s population was further disaggregated into four-dimensional vectors (subscripts): age, gender, race, and Covid status. Age was represented in the model as a single age cohort from newborn to age 0–64 for the population under 65 years and single age cohorts from age 65–100 and older for the population 65 years and older. Gender consists of male and female, while race includes non-Hispanic White, non-Hispanic Black, Hispanic, and Other races. COVID status was represented as “no-Covid” or “had-Covid”. No-Covid herein refers to individuals who have never been diagnosed with COVID-19, while had-Covid relates to individuals with at least one COVID-19 diagnosis. The Health and Retirement Study (HRS) assesses cognitive function in self-respondents with a range of tests adapted from the Telephone Interview for Cognitive Status (TICS). 25 We used the 27-point cognitive scale that included an immediate and delayed 10-noun free recall test, a series seven subtraction test, and a backward count from 20 test. Cut-points for no dementia and dementia were validated in the Aging, Demographics, and Memory Study, an HRS sub-study of AD and dementia that used a 3–4 hours in-home neuropsychological and clinical assessment as well as expert clinician adjudication to obtain a “gold-standard” diagnosis of dementia. A score of 0 to 6 was classified as dementia, and that of 7 to 27 as no dementia. 26,27

This diagram depicts stocks (rectangles) and flows (arrows) of the system dynamics dementia model for older adults in the US. Stocks and flows govern the states and changes in the health status of older adults over time. The flows capture the transition between stocks that shift individuals from one state to another over time. The diagram shows a population < 65 with and without COVID-19, a population >=65 with and without COVID-19, and a dementia population. To simplify the diagram, each stock has death as outflow, which is not explicitly depicted. Also, each stock is disaggregated by a single age cohort to ensure accurate chronological aging annually. It is important to emphasize that dementia onset applies to only a percentage of older adults 65 years and older, and dementia is not assumed to be a natural part of aging.
As shown in Fig. 1, births were calculated using the female reproductive age cohorts (fecund females aged 15–49) and their corresponding fertility rates. Deaths were calculated based on the mortality rates from each age cohort obtained from life tables. 28 Net migration was estimated via calibration. At the end of each year, the surviving population in each age cohort flows to the subsequent cohort, except the final age cohort (age 100 and older). The transition from the population under 65 years to the population 65 years and older is determined by becoming age 65 for individuals with or without COVID-19. The transition rates from the population 65 years and older (no-Covid) to those 65 years and older with dementia (no-Covid) have three-dimensional vectors: age, gender, and race, and were estimated using the Health and Retirement Study.
However, the transition rates from the population 65 years and older (had-Covid) to those 65 years and older with dementia (had-Covid) have two pathways. The first pathway is individuals 65 years and older (had-Covid) with no cognitive impairment will use the transition rates estimated from the Health and Retirement Study to progress to dementia. The second pathway is that individuals 65 years and older (had-Covid) who have mild cognitive impairment 29 and experience moderate to severe symptoms 30 will use transition rates estimated from the Health and Retirement Study adjusted by the findings from the literature as cited 4 of the hazard ratio of the onset of dementia given COVID-19 diagnoses. According to Wang and colleagues, 4 the hazard ratio of onset of dementia given a COVID-19 diagnosis is 1.59 for ages 65 to 74, 1.69 for ages 75 to 84, and 1.89 for aged 85 and older. The transition from the population 65 years and older with no dementia to dementia is determined by age, race, gender, and COVID status-specific transition rates. This ensures that when an individual transitions from one state to another at the end of each year, that individual also moves to the proper age, gender, race, and COVID status-specific state. The following are the critical assumptions made in the multi-state population model to project the impact of COVID-19 infection on dementia. First, the 2010–2018 race-specific fertility rates from the National Vital Statistics report were used in the model. Fertility rates in 2018 were assumed to remain constant over the projection period because a change in fertility will have no impact on the simulation by 2050, given that the study focuses on individuals 65 years and older. Second, age and race-specific mortality rates from the National Vital Statistics report were used. The following future mortality decline was assumed from 2023 to 2050 : 2.71% for ages 0 to 14, 1.05% for ages 15 to 49, 1.34% for ages 50 to 64, and 1.05% for age 65 and older. 31 Third, for the transition rates from the population 65 years and older with no dementia to the population with dementia, a 2.5% improvement was assumed, 32 and the same 2.5% improvement was considered for the proportion of the population 65 years and older with mild cognitive impairment. This assumption was informed by the findings by Robert and colleagues 32 that older people with dementia decline between 1% –2.5% annually. Lastly, the hazard ratio from Wang and colleagues 4 that indicates an increased risk of dementia from COVID-19 is applied to older adult individuals who had COVID-19 and developed mild to severe symptoms as a result of the COVID-19 infection and had mild cognitive impairment.
Data and estimation of transition rates
The 1998 to 2018 Health and Retirement Study (HRS) data was used to estimate the transition rates across the population states. The HRS is a longitudinal panel study that surveys a nationally representative sample of more than 26,000 Americans over the age of 50 every two years. The study explores changes in labor force participation and health transitions that individuals undergo toward the end of their work lives. The HRS has collected information about income, work, assets, pension plans, health insurance, disability, physical health and functioning, cognitive function, and healthcare expenditure. The input data to the transition rates estimate is in an extended format, and each observation occupies one data line. Each line of observation includes the individual’s age and values of covariates in the model. Everyone has multiple lines of observation. Since HRS is not an annual survey, we will fill in gaps with pseudo-data representing successive years to obtain annual transition rates. If an interval’s starting and ending states are the same, the filled-in data assumes those states. If the interval’s starting and ending states differ, the filled-in data assumes one transition at a random time. Multinomial logistic regressions are then fitted to estimate the probability of transitioning from the starting state to one of the ending states, including death. Multinomial regression models estimate age, gender, and race-specific transition rates. The equation below, with age, gender, and race as covariates, was used to calculate the transition rate. The equation was solved with multinomial logistic regression models using the “multinom” function in R.
Probabilistic sensitivity analysis
After computing point estimates for the transition rates from the multinomial logistic regression, the bootstrap method was used to estimate the likely distribution of transition rates to obtain the 95% confidence interval around these point estimates. First, we rescale sampling weights so that they sum up to 100%, and then we use the weights as probabilities to draw respondents (by identification, ID) with replacement using the “sample” function in R (v3.2.1). Each respondent (ID) may be drawn once, more than once, or not at all in the sampling. This process was repeated 1000 times to obtain 1000 datasets, which were then used to estimate the transition rates. Next, transition rates were calculated using the 1000 samples with the multinomial logistic regression model. Based on the 1000 sets of estimated transition rates, the distribution of age, gender, and race-specific transition rates and 95% (bootstrap) confidence intervals were obtained. Transition rates from the bootstrap analysis were used as input for the sensitivity analysis to determine the likely variation in the projected number of older adults with dementia.
Scenarios
Business as usual (BAU): The business as usual (BAU) scenario assumes no change to crucial model parameters that may be affected by policy, intervention, and a pandemic with neurological effects. Though this scenario is unlikely, given the constant introduction of interventions to improve dementia risk, we included this scenario as a reference point for evaluating the alternative scenarios.
Reported COVID-19 infection: The reported COVID-19 infection scenario accounts for the officially reported number of Americans by age, gender, and race that contracted COVID-19 at least once and its impact on the onset of dementia based on the evidence as reported in the literature cited. 33 As noted by Wang and colleagues, 4 older adults (age 65 years and older) who had COVID-19 have an increased risk of a new diagnosis of AD (dementia). The hazard ratio of older adults 65 to 74 years is (1.69 (1.37–1.85)), 75 to 84 years is (1.69 (1.54–1.85)), and 85 years and older is (1.89 (1.73–2.07)). The reported COVID-19 scenario was implemented by increasing the estimated age, gender, and race-specific transition rates from HRS by the hazard ratios.
Actual COVID-19 infection: The actual COVID-19 infection scenario accounts for the estimated true COVID-19 infection. A nationwide blood donor survey from the CDC examining the percentage of people with antibodies against COVID-19 estimates the infection-induced seroprevalence to be approximately 77.5% of Americans. 34 Hence, under this scenario, the number of people with COVID-19 was assumed to be three-fourths of the American population.
RESULTS
Figure 2 shows the age, gender, and race-specific transition rates estimated from the Health and Retirement Study. All the transition rates were found to increase with age. For the onset of dementia (no dementia to dementia), females had a higher rate of transitioning from no dementia to dementia compared to males across all races. Non-Hispanic Blacks and Hispanics, for both females and males, have a higher transition rate to dementia compared to non-Hispanic Whites and Other races. Also, at older age, non-Hispanic Blacks and Hispanics were found to have almost twice the risk of onset of dementia compared to non-Hispanic Whites and Other races. The onset of dementia for non-Hispanic Whites was estimated to increase from (0.0046) 0.46% at age 65 to (0.16) 16% by age 100 and older, while that for non-Hispanic Blacks increased from (0.022) 2.2% at 65 years to (0.256) 25.6% at age 100 and older. The onset of dementia for Hispanics increases from (0.214) 2.14% at age 65 to (0.242) 24.2% at age 100 and older. Meanwhile, for other races, it is (0.0148) 1.48% at age 65 to (0.117) 11.7% at age 100 and older. On the transition from no dementia to death, the mortality rate was found to increase with age; mortality rates from age 65 years to 85 years, for both genders, were similar, though non-Hispanic Blacks had consistently higher mortality rates compared to all races. But, from age 85 years and older, among the females, non-Hispanic Whites had the highest mortality rates, while non-Hispanic Blacks had the lowest mortality rate; however, for males, Hispanics had the lowest mortality rate at age 85 years and older, while non-Hispanic Whites remained the highest. The transition from dementia to death increases with age, and males have higher mortality rates compared to females. Among the females, non-Hispanic Whites had consistently higher mortality rates across all ages, while Hispanics had the lowest mortality rates. Among the males, non-Hispanic Whites and Other races had the highest mortality rates, while Hispanics had the lowest mortality rates.
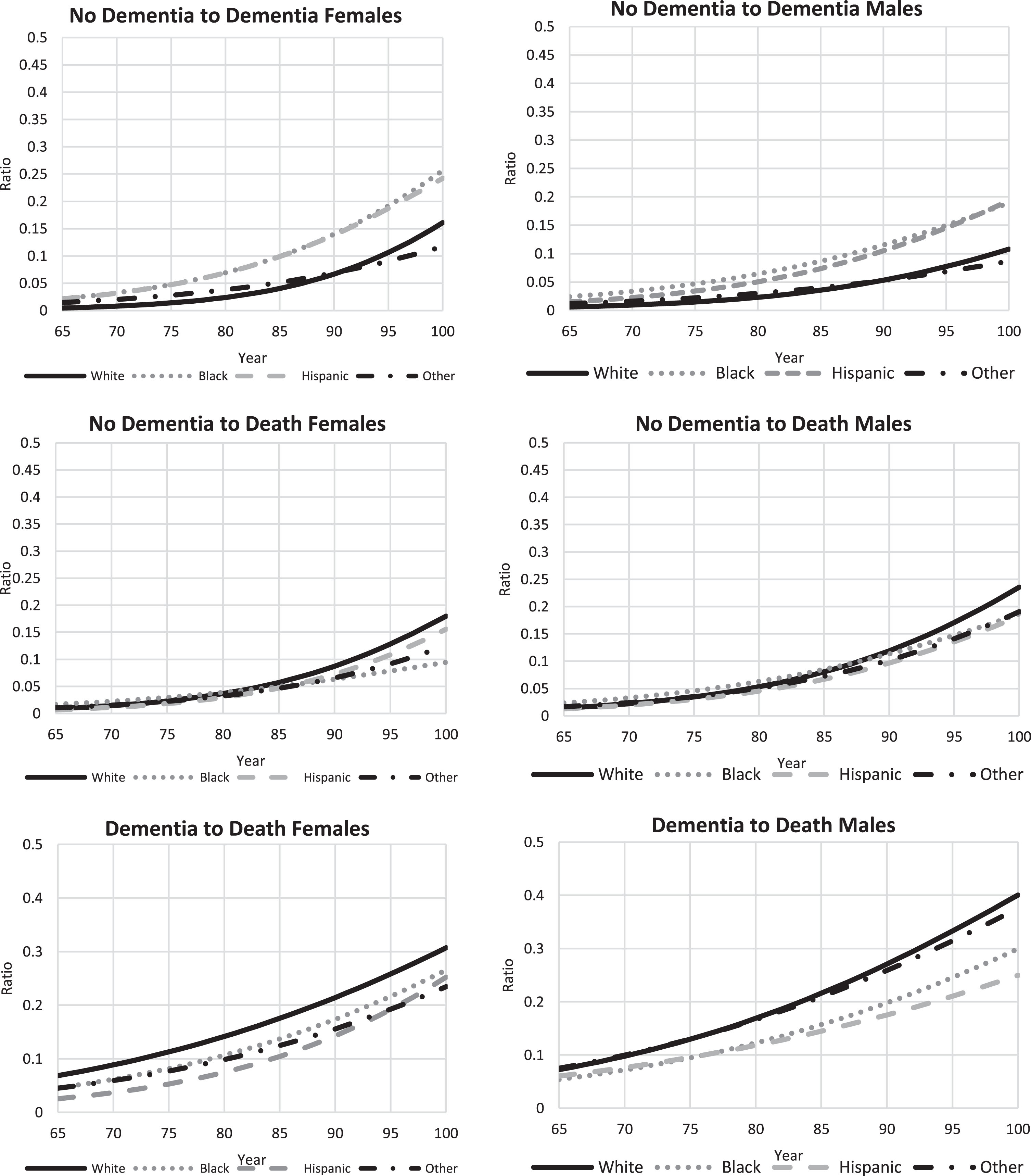
Transition rates across health states by gender for older adults 65 years and older: no dementia to dementia, no dementia to death, and dementia to deaths.
As shown in Fig. 3, the number of older adults 65 years and older with dementia under the business as usual (BAU) is projected to increase from 7.361 million (95% confidence interval of 7.352–7.369) in 2020 to 14.838 million (14.816–14.861) people by 2050. Of the older adults 65 years and older with dementia, 63% are female, and the proportion 85 years and older is projected to increase from 36% in 2020 to 54% by 2050. Due to the COVID-19 pandemic, under the reported COVID-19 infections scenario, it is projected that the number of older adults 65 years and older with dementia will increase from 7.361 million (7.352–7.369) in 2020 to 15.103 million (15.080–15.125) by 2050, representing an increase of 265,000 people by 2050 with dementia due to COVID-19, compared to the BAU. Likewise, under the actual COVID-19 infections scenario, dementia among older adults 65 years and older is projected to increase from 7.361 million (7.352–7.369) in 2020 to 15.515 million (15.491–15.538) by 2050, representing an increase of 677,000 people with dementia due to COVID-19, compared to the BAU.
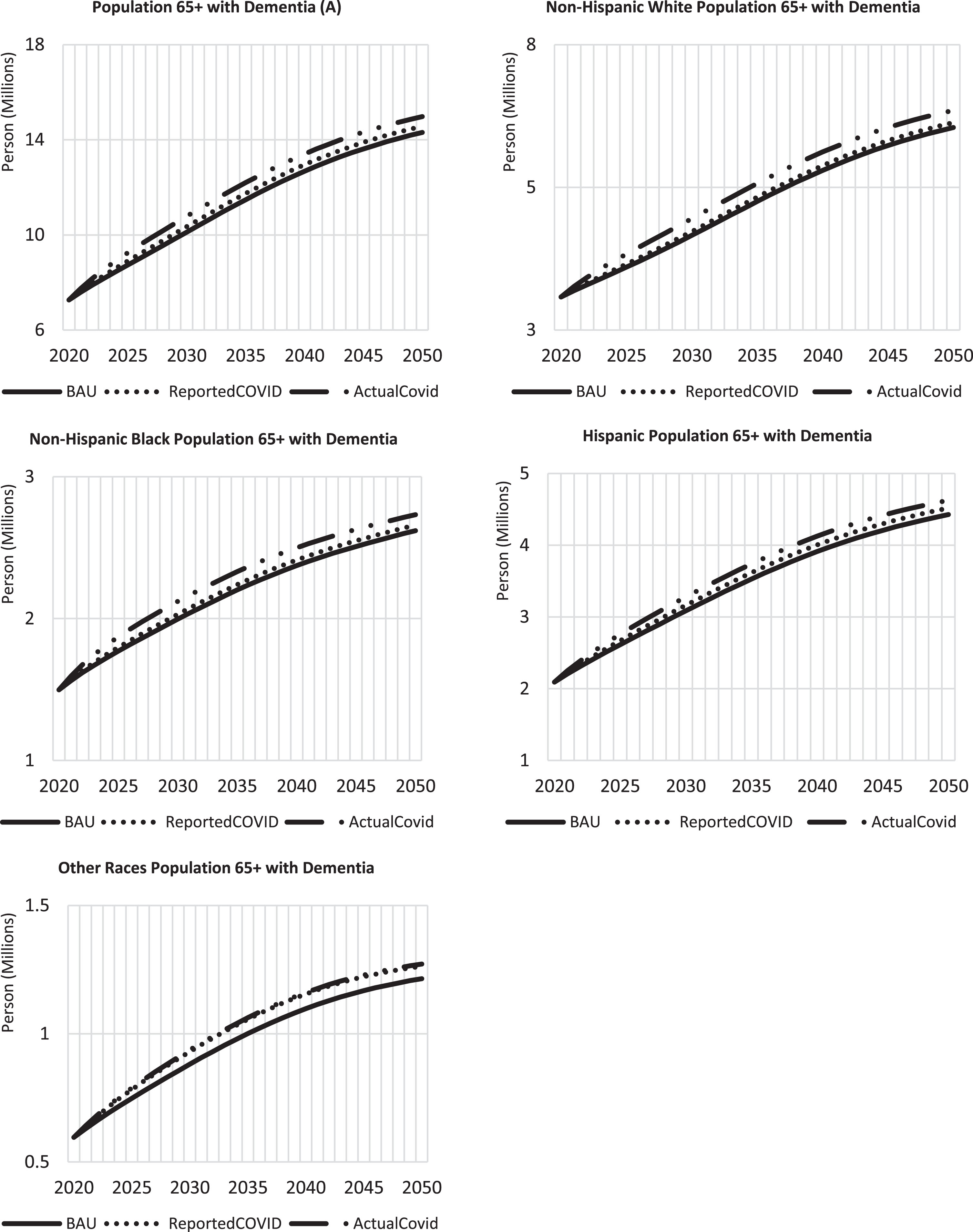
Projected number of adults aged 65 years and older with Dementia for all groups (A) and by race: non-Hispanic Whites (B), non-Hispanic Blacks (C), Hispanics (D), and Other Races (E).
For non-Hispanic Whites, under the BAU scenario, the number of older adults with dementia is projected to increase from 3.162 million (3.158–3.166) in 2020 to 6.429 million (6.420–6.438) people by 2050. Under the reported COVID-19 infections scenario, the number of older adults with dementia is projected to be 6.518 million (6.509–6.527) by 2050, representing an increase of 89,000 people compared to the BAU. Under the actual COVID-19 infections scenario, dementia among older adults is projected to be 6.742 million (6.733–6.751) by 2050, representing an increase of 313,000 people relative to the BAU. The number of older adults with dementia among the non-Hispanic Black population is projected to increase from 1.516 million (1.513–1.519) in 2020 to 2.704 million (2.697–2.711) by 2050. Under the reported and actual COVID-19 infection scenarios, dementia among older adults is projected to be 2.743 million (2.736–2.750) and 2.815 million (2.807–2.822), respectively, by 2050. This suggests an increase of 39,000 and 111,000 compared to the BAU. For the Hispanic population, the number of older adults with dementia is projected to increase from 2.089 million (2.083–2.096) in 2020 to 4.494 million (4.477–4.510) by 2050. Considering the reported COVID-19 infections scenario, dementia among older adults is projected to increase to 4.583 million (4.566–4.600) by 2050, indicating an increase of 89,000 people compared to the BAU. Likewise, under the actual COVID-19 infections scenario, the number of older adults with dementia is projected to increase to 4.690 million (4.672–4.707), representing an increase of 196,000 relative to the BAU. Lastly, for other races, dementia among older adults is projected to increase from 0.593 million (0.589–0.597) in 2020 to 1.212 million (1.202–1.221) by 2050. Under the reported COVID-19 infections scenario, the dementia population is projected to increase to 1.259 million (1.249–1.269) by 2050, representing an increase of 47,000 by 2050, compared to the BAU. Also, under the actual COVID-19 infections scenario, adults with dementia, among other races, are projected to increase to 1.268 million (1.258–1.278) by 2050, suggesting an increase of 56,000 by 2050. A detailed table of dementia projections in 2020, 2030, 2040, and 2050 is provided in Supplementary Table 1. The racial distribution of older adults with dementia indicates that under the BAU, by 2050, non-Hispanic Whites will constitute 43.45% of the older adults with dementia, while non-Hispanic blacks, Hispanics, and Other races are 18.15%, 30.2%, and 8.2% respectively. The distribution will remain similar under the reported and actual COVID-19 infection scenarios.
DISCUSSION
Due to the aging population, the number of older adults with dementia is projected to increase, and the proportion of older adults 85 years and older with dementia is expected to grow from 36% in 2020 to 54% by 2050 under the business-as-usual scenario. According to our projections, the number of older adults who will develop dementia by 2050 due to the COVID-19 pandemic will be between 265,000 and 677,000. Even though non-Hispanic Blacks and Hispanics constitute 12.6% and 19.1% of the US population in 2022, according to the US Census Bureau, they are projected to comprise 18.2% and 30.2% of older adults with dementia.
The projection from our research estimates that older adults 65 years and older with dementia under the business as usual (BAU) will be 14.838 million (14.816–14.861) by 2050. Our projection differs from the reported dementia burden in the literature. 35–37 A study in 2019 estimated the prevalence of AD and related dementias in the US up to 2060 using age, sex, and race as factors. Using Medicare claims data on the Medicare FFS (fee for service) beneficiaries aged≥65 years and the US Census Bureau’s annual population projections by sex, race, Hispanic origin, and 5-year age groups, they estimated the number of dementia patients to grow to 13.9 million by 2060, with the Hispanic population seeing the most significant increase. 35 Another study estimated the prevalence of preclinical and clinical AD by utilizing a multistate model from the biomarkers of preclinical AD. These results estimated the prevalence of dementia to grow to 9.30 million by 2060 and the number of persons with preclinical AD to increase to 75.68 million. 33 Studies on the projected prevalence of dementia in the US are limited, particularly those that use multi-state population models with evidence-based age, gender, and race-specific transition rates from nationally representative data. Our projection differs from that of Matthews and colleagues 35 and Brookmeyer and colleagues 36 because they obtained their projection by applying prevalence rates by age, sex, and race from non-representative population data to a projected US population. In contrast, our projection uses multi-state population models with evidence-based age, gender, and race-specific transition rates from nationally representative data. In addition, our model accounts for the expected reduction in mortality rates across all ages, thus increasing the years people live with dementia.
The finding that the number of older adults with dementia will increase has policy implications for social care services and healthcare needs. Caregiving is a significant part of the social care needs of individuals with dementia. Caregiving for dementia has two elements: informal and formal. Informal caregiving consists of unpaid care, typically provided by families and communities of the dementia patient. In 2022, caregivers of dementia patients provided approximately 18 billion hours of informal care, valued at $339.5 billion. 1 With the increased time and money spent caring for the patient, caregivers face a depleted income and finances. Moreover, this burden is not limited to monetary value. Caregivers of dementia patients are at risk of increased emotional stress and depression, a decrease in social networks, and concern over the maintenance of their health. 1 With the projected increase in dementia, the caregiver burden will respectively increase, pointing to the need for interventions to support dementia caregivers. Interventions can be educational programs to prepare families with the skills and knowledge to care for individuals with dementia. Other interventions include providing caregivers assistance with caregiving duties, increased social support, and access to support groups and counseling services. 1 Formal caregiving will also be impacted by this significant increase in dementia cases in America. The workforce of formal dementia caregivers includes primary care physicians, advanced practice clinicians, specialists, nurses, psychologists, therapists, social workers, home health aides, and personal care aides. 1 The direct care workforce consists of personal care aides and home health aides who assist with activities of daily living and instrumental activities of daily living, supporting the informal caregivers. 1 There is already a nationwide shortage of geriatricians and specialists and a high turnover rate for direct care workers. 1 To prepare for the increase in dementia patients, the healthcare workforce must be expanded and supported.
The projected increase in dementia will have cost implications. The total lifetime cost of care for a dementia patient was estimated at $392,874, with 70% of the cost taken on by family caregivers and the remaining by Medicare and Medicaid. 1 In 2021, the average cost for a private room in a nursing home was $108,405 per year, and $54,000 per year for assisted living residencies. 1 While Medicaid covers nursing homes and long-term care services, it is only covered for individuals with low income, leading to high costs that will only continue to increase as the number of Americans with dementia grows. This research further emphasizes the need for a greater focus on specific interventions to reduce the risk of transition to dementia. The WW-FINGERS study in Finland investigated the impact of early interventions in nutritional guidance, physical exercise, cognitive training, social activities, and managing vascular and metabolic risk factors on dementia progression. 13 Results showed improved cognition, including executive function, processing speed, and complex memory tasks. 13 The US version of the FINGER study, US-POINTER, is an ongoing study that explores the impact of lifestyle interventions on dementia progression in the US population. This research can be used to investigate further the effect of these lifestyle interventions on a population level.
The main limitation of this research is the potential for overestimation of the number of people with dementia. The number of people developing dementia due to COVID-19, as projected in this research, may not be mutually exclusive from those who would have otherwise developed dementia. To address this problem, we applied the hazard ratio to the estimated transition rate to dementia to the population 65 years and older with mild cognitive impairment (using the prevalence of mild cognitive impairment) who had COVID-19 and developed moderate to severe symptoms. The individuals 65 years and older who had COVID-19 but did not have mild cognitive impairment and or did not develop moderate to severe symptoms would have the same risk of progression to dementia as the general population 65 years and older. Another limitation is that the projection only accounts for age, sex, and race. Common risk factors for dementia, such as education, hypertension, obesity, hearing loss, traumatic brain injury, alcohol misuse, smoking, depression, physical inactivity, social isolation, diabetes, and air pollution, were not accounted for in the projections. It is important to note that a change in these risk factors may under or over-estimate the projected number of people with dementia. Lastly, another limitation of note is that this study used the hazard ratio of the impact of COVID-19 infection on dementia from only one study, which may not be representative of the US population. To address this limitation, the 1000 bootstrap probabilistic sensitivity analysis conducted on the estimated transition to dementia rates from the Health and Retirement Study, which is used in combination with the hazard ratio, ensures we account for the likely variations in the transition to dementia.
Conclusion
Our evidence-based multi-state population model incorporating transition rate estimates from the Health and Retirement Study and the impact of COVID-19 infection on dementia onset suggests that due to the COVID-19 pandemic, the number of older adults with dementia in the US is projected to increase between 265,000 and 677,000 by 2050. The expected increase in dementia is due to population aging. The corresponding increase in healthcare, social care service needs, and cost poses a significant challenge that requires urgent policy and intervention to address the intended and unintended consequences of dementia. The insights from this study suggest that there will be an increase in demand for intermediate and long-term care services for individuals with dementia. Whether this demand will be filled by the family, the private sector, the healthcare system, or the government is an issue that policymakers should consider in planning for US health and social care needs.
AUTHOR CONTRIBUTION
John P. Ansah (Conceptualization; Formal analysis; Methodology; Writing – original draft; Writing – review & editing); Hannah Zachara (Conceptualization; Writing – original draft; Writing – review & editing); Chi-Tsun Chiu (Data curation; Formal analysis; Methodology)
Footnotes
ACKNOWLEDGMENTS
Center for Community Health Integration is responsible for creating a conducive environment for this research.
FUNDING
The Center for Community Health Integration, School of Medicine, Case Western Reserve University, supported this research.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.