
Abstract
Background:
Dementia stigma has adverse effects on people with dementia and their carers. These effects can lead to poor quality of life among other negative impacts.
Objective:
The aim of this study is to develop and pilot a novel dementia stigma reduction intervention in rural Kenya, leveraging existing Community Health Workers (CHWs) for its delivery.
Methods:
The pre-post pilot study was conducted, utilizing a parallel mixed-methods design. Ten CHWs were trained to deliver a contextually developed dementia anti-stigma intervention. These CHWs delivered four workshops to 59 members of the general public in Makueni County, with each workshop lasting between 1.5 to 2 hours. Focus group discussions and pre/post surveys were used as measures.
Results:
The intervention was well received amongst the participants, particularly in terms of its format and accessibility. We observed the largest effects in reducing negative beliefs related to treatment (η2 = 0.34), living well with dementia (η2 = 0.98), and care (η2 = 0.56) for the general public post intervention. Improvements to attitudes were also observed in the CHWs, but the effect sizes were typically smaller.
Conclusions:
The intervention was accessible and feasible in rural Kenya, while also showing preliminary benefits to stigma related outcomes. The findings indicate that culturally sensitive interventions can be delivered in a pragmatic and context specific manner, thus filling an important knowledge gap in addressing stigma in low-resource settings. Future research is needed to ascertain the intervention’s long-term benefits and whether it tackles important behavioral outcomes and beliefs deeply ingrained within communities.
INTRODUCTION
Dementia stigma negatively affects the health and quality of life of those living with the condition and their carers [1]. It can also act as a barrier to seek information, care, and support [2, 3]. Dementia stigma can be conceptualized in several ways, based on who perpetrates it and the nature in which it occurs [2, 4]. For example, public stigma typically relates to the stereotypes, prejudice, and discrimination that members of the general public enact on people with the condition [5]. A consequence of public stigma can be social exclusion [4], in which people with dementia are denied public participation or distanced due to beliefs that people with dementia are incompetent or unpredictable [4, 6]. In addition to public stigma, people with dementia and their carers may also experience other types of stigma including stigma by association (e.g., stigma attached to those associated with the person with dementia such as a carer) and self-stigma (e.g., people with dementia internalizing public stigma) [7]. Models of stigma recognize the importance of cultural norms in shaping how stigma presents itself [8, 9].
Approximately 258,000 older adults in Kenya are potentially living with dementia [10]. Generally, the number is expected to rise to 361,000 by the year 2050, a 316% increase since 2019 [11]. Despite the growing numbers of people with dementia, not a lot is known about how dementia stigma manifests in Kenya. While we can infer common patterns from other countries, very little exists on dementia stigma in Africa in general [12]. In one of the studies in the region, it was found that dementia was often believed to result from being bewitched or cursed, and that through spirituality dementia outcomes can be improved [13]. Dementia was also commonly attributed to normal aging or ‘falling from grace’— in that, one who previously assumed a high social status has now lost it [13]. Depending on the belief held, people with dementia are either seen as having been punished or not in need of formal support. It is unsurprising that these beliefs can have a negative effect on health-seeking behavior [14], and amplify the challenges of livingwith dementia.
There are well established models of reducing stigma that typically encompass education and contact [15]. Despite the highlighted impacts of dementia stigma and pathways to change, there is a dearth of interventions primarily aimed at reducing stigma in low- and middle-income countries (LMICs) such as Kenya. As of 2019, there was not a single stigma reduction intervention related to dementia outside of the US, Canada, UK, and Australia [16]. Only recently has a protocol for dementia stigma reduction in Brazil been published [17], albeit aimed at healthcare staff. There is an apparent lag behind mental health stigma reduction interventions which appear to be growing in number and quality [18]. However, even within the mental health stigma field there is scope for improvement, with the majority of interventions not considering cultural values and context [5, 19]. Developing dementia stigma reduction interventions that are culturally specific and fit within the local context is essential to ensure they are relevant, acceptable and effective to the context and participants.
The aim of this study is to develop and pilot a novel dementia stigma reduction intervention in rural Kenya, leveraging existing Community Health Workers (CHWs) for its delivery. In this study we evaluate the acceptability and feasibility of the intervention on dementia stigma reduction.
METHODS
Context
The research occurred within Makueni County in rural Kenya with a population of about one million. It is one of the counties whose residents greatly attribute dementia and other mental illnesses to witchcraft resulting in limited access to timely diagnosis and care [13, 20].
The government of Kenya through the Ministry of Health has enabled the recruitment of CHWs who work within community health units and are attached to a health facility. Each CHW is attached to 20–100 households and is in charge of the delivery of basic health services including health promotion [21]. The CHWs report to Community Health Assistants who are answerable to the Community Public Officer or Nurse under the title ‘community health extension worker’ [22]. CHWs are often chosen to deliver public health interventions to the community since they are easily accessible to the community members and are well endowed with the knowledge of appropriate referral systems in the event that there is a condition that requires further medical examination or care [22]. They have been shown to be effective in delivering behavior change interventions especially in situations where there is paucity of healthcare workers [21].
Intervention
The development of the anti-stigma intervention followed the Medical Research Council (MRC) framework for development of complex interventions comprising four phases [23]. In each of the phases, key considerations were made such as relevant stakeholder engagement throughout the development process and dynamic iterative processes to intervention development [24]. Further details of the development process are in the Supplementary Material.
The final intervention took the form of a train-the-trainer program, in which individuals without formal education receive training on a given topic and instructions on how to train others on the approach [25]. Within the context of this study, we delivered training to ten CHWs to promote awareness and reduce dementia stigma. Content included promoting understanding of dementia, demystifying myths and misconceptions and promoting social inclusion through a case vignette and discussions (Fig. 1). Videos of people living with dementia and carers were used as the social contact element of the intervention— an empirical and important element of anti-stigma interventions [26]. The CHWs were also given guidance on how to deliver a similar session to members of the general public [27].
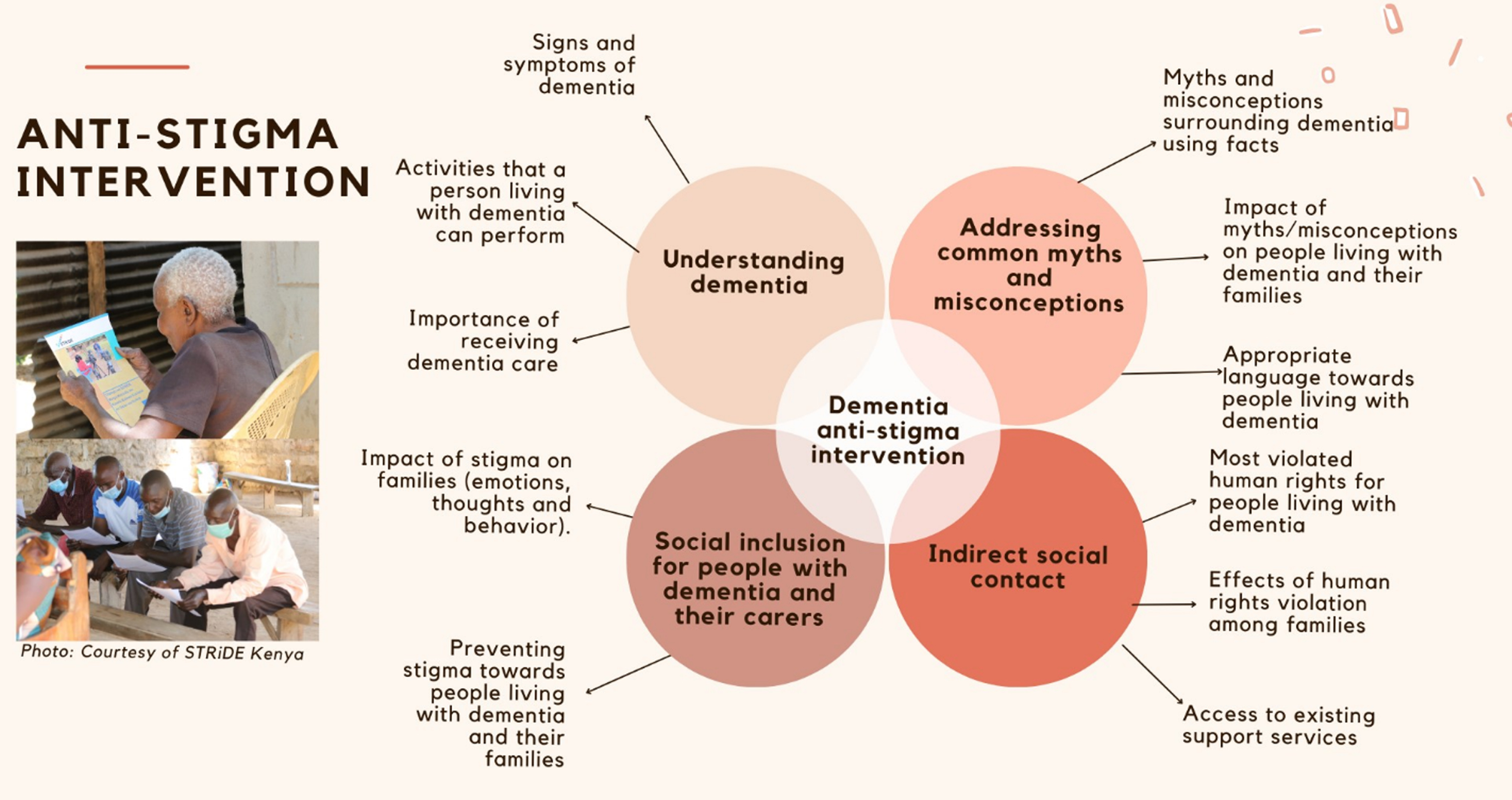
Dementia Anti-Stigma Intervention (DASI). Consent was obtained from all featured participants.
Pairs of CHWs were then asked to deliver and facilitate stigma reduction workshops with the general public. CHWs delivered four group workshops (composed of 10–12 adults, which included people of different ages and different experiences of dementia), over a two-week period. Each workshop lasted between 1.5 to 2 hours.
The intervention can be found here: https://stride-dementia.org/wp-content/uploads/2022/07/STRIDE_Intervention_Kenya.pdf
Design
The pre-post study was conducted, utilizing a parallel mixed-methods design.
Procedures
Participants included a pragmatic sample of ten CHWs (within the study site) and members of the general public involved in the intervention. The members of the general public were recruited by the CHWs through convenience sampling, inviting adults (18 years and older) in the community. The research team asked the CHWs to identify a broad sociodemographic representation (e.g., diverse age, gender, social status, and experience of dementia). Participants were required to be over the age of 18 years old and provide informed consent to participate in the research. Information was provided to the participants prior to the study, and they were provided with an opportunity to ask any questions before choosing to participate. CHWs and members of the general public were informed that they would be involved in the intervention.
For CHWs, questionnaires about knowledge and beliefs surrounding dementia were collected prior to their first training session and then within one month after delivering the stigma reduction workshops. For the general public, the same questionnaires were asked prior to their first stigma reduction workshop and then one month after the workshop. A subset of participants were invited to participate in focus group discussions (FGDs) to understand their experiences and opinions of the intervention. Six FGDs (two FGDs with CHWs and four FGDs with members of the general public who received the intervention) were conducted within one month of the intervention being delivered by the CHWs. The participants of the six focused groups were chosen based on the following categories: CHWs, carers of people with dementia, people with a relative with dementia, people who do not have a relative with dementia, and a mixed group of people with relatives and those without relatives living with dementia. The selection of participants for the FGDs was based on convenience (degree of participation during intervention delivery and availability). FGDs were led by a female Kenyan dementia researcher (CM), audio-taped and lasted between 60 and 90 minutes. All the training, intervention material and questionnaires were delivered in Kamba (one of the local languages in Kenya).
Measures
Socio-demographic questionnaire: This included information on age, gender, education, religion, and employment.
Alzheimer’s Disease International (ADI) global questionnaire on dementia stigma: This questionnaire was adapted from the World Alzheimer’s Report (WAR) through public engagement and input from the research team and covers knowledge, attitudes and behavioral intention, and has been tested among 70,000 people in 155 countries [2]. In the current study, there were some edits to the statements (e.g., clarifying that nursing home could also mean residential care homes, and removing questions that were overly scientific (e.g., presence of apolipoprotein E and high levels of norepinephrine). This is because participants generally had lower levels of education and some of these terms were new to participants during adaptation. The adapted version included 91-items that measured knowledge (i.e., causal attribution of dementia) alongside attitudes and beliefs related to: (i) treatment, institutional care, and safety, (ii) social distance, (iii) personal risk, (iv) secrecy, (v) help-seeking, (vi) health care worker stigma, (vii) anticipated stigma, (viii) resource allocation, and (ix) structural stigma. All item responses were provided on a Likert scale.
The interview guides, developed by the research team included open-ended questions covering challenges and motivations of participants to engage in the training, intervention appraisal, knowledge acquisition and its application following training.
Analysis
Descriptive statistics (mean and standard deviation; frequency and percentage) were reported for participant sociodemographic information. These were reported separately for the general public and CHWs.
Perceived etiology of dementia was reported descriptively at each time point (i.e., frequencies, percentages) for the general public and CHWs. For general public data, a Wilcoxon analysis was completed on items between time points. For the purpose of this between time point, we excluded “don’t know” responses. To facilitate interpretation of the 5-point Likert scales, we dichotomized outcomes into affirmative (Very likely and Likely) and non-affirmative responses (Not likely and Not at all likely), excluding “don’t know”.
Belief items were conceptually grouped into themes (Supplementary Table 1), namely, beliefs about risk (k = 3), treatment (k = 4), living with dementia (k = 9), care (k = 5), and secrecy (k = 8). Individual items were reverse coded so that all items could be interpreted consistently (e.g., 5 represents more negative beliefs). Items within each theme were summed, responses with missing data or “don’t know” were excluded. Repeated measure ANOVA was used to understand the difference between time points, with an effect size reported (partial eta squared). Partial eta squared was used as standardized means to compare change. As a guide, η2 = 0.01 indicates a small effect, η2 = 0.06 indicates a medium effect, and η2 = 0.14 indicates a large effect size. The analysis was replicated for the general public and CHWs separately.
To evaluate the nature of missing data within the beliefs data at baseline and follow-up, Little’s MCAR test was employed. A p-value less than 0.05 on the test indicates that the data were not missing at random. If data were missing at random, we repeated the main analysis following mean imputation in cases where there were less than 50% missing items within a belief theme. The belief data at baseline (General public, Little’s MCAR = 0.25; CHWs, Little’s MCAR = 1.00) and follow-up (General public, Little’s MCAR = 0.16; CHWs, Little’s MCAR = 1.00) were considered missing at random.
For FGDs, audio files were transcribed and translated to English for analysis. Inductive thematic analysis was adopted, to ensure that interpretation is data-driven and that we do not miss any unexpected themes by trying to fit it into a pre-existing coding frame [28]. Researchers (CM and LM) coded the transcripts. The scripts were initially reviewed independently, and a meeting followed to agree on a coding framework. The researchers then coded the scripts independently and met to review the different codes. These codes were subsequently grouped into subthemes and themes, based on commonality. While CM conducted the interviews and formed part of the analysis team, she remained cognizant of any personal views that may affect the analysis to ensure that themes emerged from the data. Specifically, we adopted a pragmatic standpoint as an epistemological perspective, to better allow us to seek practical insights into the stigma reduction intervention.
Quantitative analysis was performed on SPSS (version 25) while qualitative analysis was performed using NVivo 12 [29, 30].
RESULTS
Fifty-nine members of the general public and 10 CHWs participated in the anti-stigma intervention pilot evaluation. The general public were aged between 21 and 73 years old, and 57.6% were female (n = 34). Six participants (10.2%) had never heard of the terms “dementia” or “Alzheimer’s disease”. The CHWs were aged between 41 and 61 years, and predominantly female (n = 7, 70%). All CHWs had heard of “dementia” and/or “Alzheimer’s disease” (Table 1).
Baseline demographics reported for general public (n = 59) and CHWs (n = 10) that participated in the stigma reduction intervention
*Multiple response items
Four participants from the general public (6.7%) did not complete the follow-up questionnaire. Those who did not complete the follow-up questionnaire did not significantly differ from the rest of the sample based on age (MD = –8.82, p = 0.25), sex (χ2 = 1.87, p = 0.30), educational attainment (χ2 = 1.55, p = 0.82), or whether they had heard of dementia before (χ2 = 7.69, p = 0.05). There were no dropouts between timepoints for CHWs.
Attitudes
General public: One month post intervention, there was a statistically significant reduction in negative beliefs related to risk (p = 0.04), treatment (p < 0.001), living well with dementia (p < 0.001), care (p < 0.001), and secrecy (p = 0.03) (Table 2). Following mean imputation across themes (where there was less than 50% data missing), the same direction of effects was reported (Supplementary Table 2).
Attitudes towards dementia pre- and post- the stigma reduction intervention
Community health workers: Following the program, the CHWs had improved beliefs across all domains. However, only beliefs about treatment had a large enough effect to be statistically significant (ηp2 = 0.60, p = 0.01) (Table 2 and Supplementary Table 3).
Causal attribution
General public: At baseline, the most frequent affirmative response to the causal attribution of dementia was brain disease (n = 55; 93.2%), normal aging (n = 49; 83.1%), and brain injury (n = 44; 74.6%). Witchcraft received the fewest affirmative responses (n = 7; 11.9%). Following the intervention, the most frequent affirmative responses were brain disease (n = 51; 86.4%), unhealthy lifestyle (n = 43; 72.9%), and lack of family support (n = 43; 72.9%). Again, witchcraft was the least frequently reported etiology with an affirmative response (n = 9; 15.3%). Non-parametric paired analysis revealed that the general public’s knowledge surrounding the etiology of dementia did not significantly change between timepoints (p > 0.05); the one exception being that participants at follow-up were more likely to believe that dementia is due to a lack of family support (Z = –3.61, p < 0.001). See SupplementaryTables 4 and 5.
Community health workers: At baseline, the predominant causal attribution for dementia amongst CHWs was brain disease, with 90.0% of respondents (n = 9) affirming this belief. The next most common attribution was that it was caused by head or brain injury (n = 7; 70.0%) and lack of family support (n = 7; 70%). 60% (n = 6) also believed dementia was a normal part of aging. Although receiving one of the lowest affirmative responses, 20% (n = 2) of CHWs believed that dementia was due to witchcraft. At follow-up, 100% (n = 10) of participants attributed dementia to being a brain disease, though 90% of CHWs (n = 9) believed that dementia was due to normal aging. One CHW (10.0%) still responded affirmatively to the statement that dementia is due to witchcraft at follow-up, despite also believing that dementia was a brain disease. See Supplementary Tables 6 and 7.
Qualitative results
Thematic analysis identified four overarching themes: 1) positive aspects of delivery, 2) challenges to delivery, 3) motivators to participation, and 4) perceived efficacy.
The first theme was related to the perceived positive aspects of delivery. Within this theme, we grouped codes that related to positive feedback surrounding how the intervention was delivered and highlight four subthemes; group working, inclusivity, accessible, and positive relationships with the trainer.
Group working: Most participants described the group setting as the most conducive set up rather than individualized sessions since they would learn from each other through interactions and get different perspectives through the discussions (see Table 3, section A1).
A summary of themes and subthemes from thematic analysis of Focus Group Discussion transcripts
Inclusivity: Participants also preferred the diversity in the formation of the groups as it included representatives from different ages, providing a unique opportunity for broader reach and sharing experiences across various ages. CHWs were also able to identify that being inclusive could allow the general public to support one another. One example provided was how literate participants could support illiterate participants in contributing to some elements of the workshop (see Table 3, section A2).
Accessible: Participants praised the accessible nature of the workshops, most notably by using language that was understandable. This included using simple terminology and the local language rather than English during the workshops (see Table 3, section A3).
Positive relationships with trainer: Overall, the general public felt that the trainers were well trained, and there was broad positivity towards them. Some did acknowledge that the trainers (as CHWs) were already known to them, and thus the workshops built upon existing relationships (see Table 3, section A4). Within these subthemes, there was also the view that the trainers respected their time, which made them to feel valued (see Table 3, section A4).
The second theme was related to the motivators of participating in the intervention.
Acquisition of knowledge: This was a common subtheme mentioned as a motivating factor for attending the training. There appeared to be a general desire to learn about the condition, without other motivations (see lived experience subtheme). Typically, they acknowledged that they did not know much about dementia beforehand. CHWs also reported to have observed this desire to learn (see Table 3, section B1).
Community benefit: For CHWs, due to their job role in serving the community, they saw how attending the training would benefit the community as a whole (see Table 3, section B2).
Lived experiences: For some participants, they described past experiences of seeing neglect, isolation and mental health issues for people living with dementia and did not know how to offer any care and support. As such, participants felt that this was an opportunity to learn these skills to help similar people in the future (see Table 3, section B3).
Both the general public and the CHWs recognized the value of the intervention, and in particular commented on how they felt it improved their knowledge and skills.
Improved knowledge and skills: Participants were able to reflect on knowledge gained from the intervention and describe how their knowledge and behavior had changed compared to before the intervention. Subjectively, both the general public and the CHWs reported improvements (see Table 3, section C1).
Participants were also able to identify areas for improvement, or perceived challenges in the way that the intervention was delivered.
Access to materials: Participants expressed a desire to have their own training materials to aid them during the training process. They preferred to have them in order to follow the trainer through the session as well as a tool for educating others after the intervention was over. These materials would also serve as reminders during the recapitulation portion of the session as reported by some participants (see Table 3, section D1).
Broader reach: Some participants were aware of other people that wanted to attend the workshop but were unable due to logistical constraints. CHWs also recognized a desire for others to attend. However, the CHWs identified that due to the centralized nature of the workshops, it prevented people from attending due to lack of transport (see Table 3,section D2).
DISCUSSION
This is the first dementia stigma reduction intervention piloted in Kenya. Our findings indicate that our novel, CHW-led intervention, was well received amongst both the CHWs and the general public, thus building upon previous evidence highlighting how community health providers can have a role in engaging with communities in rural areas and LMICs [31–33]. Preliminary evidence also suggest that the intervention would potentially have an impact in reducing some domains of dementia stigma.
There were several perceived strengths of the intervention, including the adoption of group working, its inclusiveness, and the positive relationships with the trainers. Importantly, the findings indicate that participants saw the intervention as being accessible, praising the terminology used and the adoption of the local Kamba language for its delivery. Within Kenya, 38.5% of adults are illiterate [34], and while English and Swahili are official languages of Kenya, Kamba is typically the primary language of the Akamba community who make up 97% of Makueni County [35]. Although tailoring content to the target audience seems common sense, this is not always achieved. For example, within the UK, only 24.3% of evaluated patient leaflets met recommended reading criteria [36].
FGDs did identify that the interventions had scope for improvement, if additional reading material related to the content was provided. Such information would provide opportunities for the general public to engage with the topic before, during, and after the workshops. We can draw upon learning models, such as constructivism [37], where information booklets could help people better achieve self-directed learning. Creation of such a resource would have a cost, particularly if we wanted to ensure that the content was accessible.
Following the intervention, attitudes and beliefs surrounding treatment, care and living with dementia demonstrated the largest positive effects amongst the general public. These findings were robust following imputation and aligned with subjective reports about how the intervention improved knowledge. Improved beliefs surrounding risk factors were observed following the intervention, but the effects were more modest before (ηp2 = 0.14) and after imputation (ηp2 = 0.07). In line with these findings, the majority of knowledge surrounding causal attribution did not significantly change following the intervention. Interestingly, the only item to significantly change was more from the general public who stated that lack of family support was a cause of dementia. This shift may be attributable to the intervention’s emphasis on the importance of supporting people with dementia. Perhaps an approach to mitigate this in the future would be to further develop the section on family support in order to explain its place in the care of a person with dementia and ultimately demystify the perceived association between family support (as described in our intervention) and dementia etiology.
It should also be noted that content related to risk factors and etiology did not prominently feature within the intervention, outside key messages that dementia is a brain disease and not due to normal aging or witchcraft (two common views in Kenya) [13, 20]. The fact that there was still a minority of participants who believed that dementia was caused by witchcraft or just normal aging after the intervention, could indicate that these beliefs are deeply ingrained [38, 39]. In fact, considering dementia as part of normal aging, visiting traditional and faith healers and taking no action have been found to be the initial dementia care pathways following dementia suspicion in rural Kenya [2]. This finding is not unique to our setting as other studies in sub-Saharan Africa have established this pathway as a mechanism sought by people with dementia and their families to manage the condition [39]. Irrespective, there is a case for raising awareness about dementia etiology and risk factors through public health messages as a means to reduce risk of dementia [40] and reduce the existing knowledge gap on causal attribution.
Our findings indicate that despite CHWs receiving the dementia training to be able to deliver the stigma reduction intervention, there were no statistically significant improvement across beliefs and attitudes following imputation. While CHWs were not seen as the primary beneficiaries of the intervention, it is positive that attitudes did not worsen as a result of the intervention even though the majority of CHWs still believed dementia was a normal part of aging. We should reflect that the CHWs were more likely to have heard of both dementia and Alzheimer’s disease terms and had more experience of the condition, compared to the general public. In addition, the CHWs had more positive dementia beliefs compared to the general public across majority of outcomes at baseline and follow-up. However, healthcare staff are not immune from holding negative beliefs, particularly in LMICs [2]. Intrinsically, educating healthcare workers may also prove to be beneficial as a way of increasing awareness on dementia [41]. The inclusion of the fact that dementia tends to double after every five years beyond the age of 65 years [42] could have been mistaken as being normal during old age by the CHWs. This reflects an overarching principle defining etiology of dementia that is not specific to our setting as other studies within sub-Saharan Africa have established similar findings [38, 39]. As such, there is a need to better clarify the context around this information and distinguish between increased prevalence and the relationship between aging and dementia in future trainings. Considering this is a group that has better knowledge of Alzheimer’s disease and dementia, an additional measure would be beneficial to ascertain the change. We recommend using a knowledge, attitudes and practice questionnaire in addition to standardized measures to ascertain change.
Study limitations
There are several limitations of the study. First, given that this was not a study on the effectiveness of the intervention, we may not make conclusions about the impact of the intervention and therefore statistical significance of the change (or lack thereof) portrayed by our findings, particularly for CHWs and where effect sizes are small. Second, we are only able to comment on the short-term benefits of our stigma reduction intervention. This is a reoccurring issue amongst mental health stigma reduction interventions in LMICs, with the majority only following participants up at the end of the intervention only [18]. The improvements in dementia attitudes, even if short-term are promising, do not guarantee long-term improvements. For example, an anti-stigma intervention (education, contact and education+contact) demonstrated no significant intervention by time effect on dementia stigma immediately after follow-up [43]. The authors did note that dementia stigma did reduce across interventions, with greater effects being reported after 12 weeks and those with the highest baseline stigma. This perhaps highlights the need to tailor interventions for the target audience considering the preliminary findings drawn from the CHWs group. We also acknowledge that attitude outcomes (rather than causal attribution) improved for the general public and largely remain unchanged for CHWs. Due to the modest sample size, a larger cohort is needed to definitively report on efficacy. Any further development of the intervention will need to iron out potential messaging issues related to the causes of dementia.
Third, the measured outcome of our study primarily relates to knowledge, beliefs and attitudes. As such, our outcomes represent two out of three subtypes of public stigma: misinformation (i.e., knowledge) and prejudice (i.e., attitudes) [5]. This does mean that our findings do not capture discrimination (i.e., behavior), however, some items do relate to imagined behavior (e.g., “If I had dementia, I would encourage my family to keep it a secret”). Capturing behavior can be difficult, particularly when 27.1% of our sample had no experience of someone with dementia. However, as highlighted earlier, hypothetical behavior may not necessarily reflect actual behavior. Fourth, the changes observed here may not necessarily be representative of the wider population. Notably, we envisage that there will be a level of volunteer bias, where certain demographics (e.g., higher education) or people with certain interests (e.g., dementia) are more likely to participate. Although, specific criteria to recruit those with specific socio-demographic characteristics in the group was indicated prior to recruitment, we also acknowledge a potential bias to the sampling frame as the selection was made by the CHWs, which could mean that they selected participants only well known to them or those active within their community health units. Finally, we did not have a control group, and therefore it is hard to say with certainty that the effects reported can be directly attributed to the intervention.
Conclusion
In as much as our study was not fundamentally focused on assessing the gap in knowledge and attitudes towards dementia, it adds onto information relating to the subject matter in similar contexts. It highlights the significant gap pertaining to information on dementia within our communities [44]. This pilot study demonstrates that a CHW-led dementia stigma reduction intervention in rural Kenya is both acceptable and feasible. The findings indicate that culturally sensitive interventions can be delivered in a pragmatic and context specific manner, thus filling an important knowledge gap in LMICs [16] and potentially creating dementia-friendly communities [45]. Future research is needed to ascertain whether the intervention can be scaled up within Kenya, to a wider audience. It is essential for future research to understand whether the benefits are sustainable long-term, and whether it tackles important behavioral outcomes.
AUTHORS CONTRIBUTIONS
Christine Musyimi (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Visualization; Writing – original draft; Writing – review & editing); Levi A Muyela (Data curation; Investigation; Project administration; Writing – original draft; Writing – review & editing); David M Ndetei (Funding acquisition; Resources; Supervision; Writing – review & editing); Sara Evans-Lacko (Conceptualization; Formal analysis; Investigation; Supervision; Writing – original draft; Writing – review & editing); Nicolas Farina (Formal analysis; Investigation; Methodology; Supervision; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This work was supported by the UK Research and Innovation’s Global Challenges Research Fund (grant number ES/P010938/1). The funder has not influenced the design, outcome or interpretation of the study.
CONFLICT OF INTEREST
Christine Musyimi is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
All other authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.