
Abstract
This study surveyed 51 specialist clinicians for their views on existing cognitive screening tests for mild cognitive impairment and their opinions about a hypothetical remote screener driven by artificial intelligence (AI). Responses revealed significant concerns regarding the sensitivity, specificity, and time taken to administer current tests, along with a general willingness to consider adopting telephone-based screening driven by AI. Findings highlight the need to design screeners that address the challenges of recognizing the earliest stages of cognitive decline and that prioritize not only accuracy but also stakeholder input.
Keywords
INTRODUCTION
Correctly recognizing the earliest stages of cognitive decline associated with Alzheimer’s disease and related dementias (ADRD) is crucial to maximize life quality and treatment options and to reduce costs associated with disability and dependency [1, 2]. However, the identification of reliable signs of ADRD at the preclinical stage can be challenging, especially for clinicians lacking specialist training [3, 4], with the result that many older adults with memory concerns fail to receive an expert evaluation and diagnosis until the disease has progressed markedly [5, 6]. A comprehensive cognitive evaluation typically requires a lengthy in-person clinical examination by a psychologist or other trained professional, which can be onerous in terms of access, time, and cost. Numerous brief paper-and-pencil screening tests for dementia are available, and typically are used in healthcare settings to identify people who would benefit from a full diagnostic workup by a specialist clinician [7]. These tests are also employed to identify participants for inclusion in clinical trials [8, 9]. However, cognitive screening tests tend to vary in their sensitivity to the earliest stages of decline [10] and are not universally offered in primary care settings [11], where concerned older adults typically first present [5]. Hence, new methods for detecting early-stage cognitive decline are needed, and some of the most promising capitalize on the rapidly advancing field of artificial intelligence (AI).
The role of artificial intelligence in cognitive screening
The development and application of AI-driven technologies in healthcare has grown exponentially in recent years, and AI-driven tools to identify cognitive decline are being applied across various modalities, including neuroimaging, genetics, blood biomarkers, and speech and language [12–15], highlighting the potential for these methods to be used in clinical settings for the detection of early cognitive decline, also known as mild cognitive impairment (MCI). Many AI-based solutions offer clinical decision support to aid in diagnosis, and tout benefits such as improved efficiency, accuracy, error detection, and cost effectiveness. This, in turn, can lead to improved productivity and profit margins at the organizational level [16].
Our own work utilizing AI to analyze speech recorded over the telephone has demonstrated success in discriminating between cognitively healthy older adults, those with MCI, and those with mild Alzheimer’s disease, is rated as enjoyable and engaging by patients, and presents output to clinicians in a user-friendly dashboard interface [13, 18]. An additional benefit of this approach is that it can be administered remotely, with the only technical requirement being that the patient have access to a telephone. However, it is currently unknown whether AI-driven early detection tools will appreciably improve patient outcomes [19].
Several studies have reported on physicians’ attitudes towards AI in healthcare [20–23], with those in favor citing benefits such as improved patient access to screening, improved physician confidence in diagnosis, and reduced specialist time spent on tedious tasks [22]. Despite this optimism, uptake has so far generally been low [24–27], with perceived transparency and trustworthiness emerging as key concerns. This may be due to the “black box” nature of AI, where the process underlying the system’s operation and decision-making is unknown [28]. Given the expected growth of AI-based clinical decision support tools across almost all healthcare specialties, user feedback (including both clinicians and patients) regarding acceptability will be crucial to ensure the technology’s adoption and realization of potential benefits. In addition to overcoming clinician reluctance to adopt, any new AI-driven options for cognitive screening would presumably need to demonstrate clear advantages over currently available paper-and-pencil screeners. Two of the most widely-used cognitive screening tools are the Mini-Mental State Exam (MMSE) [29], and the Montreal Cognitive Assessment (MoCA) [30], both of which are brief and easy to administer. However, previous reports of both primary care and specialist clinician attitudes towards cognitive screeners cited several drawbacks, including concerns about cost and time to complete testing, and a lack of specificity in detecting MCI [6, 32]. Hence, any new AI-based screeners would need to be as, or more, accurate than current tools, cost effective, and brief.
With new AI-based screening approaches on the horizon, the opinions of specialist clinicians regarding current screening practices are an important consideration for potential uptake of these tools. The current study is novel in that it surveys a group of clinicians specializing in dementia assessment for their views on currently available cognitive screening tools, and their reactions to a hypothetical AI-driven screening service delivered via the telephone. Dementia specialists were selected under the assumption that they have the most detailed knowledge and experience of cognitive decline and would be in the best position to advise on how screening tests could be improved to increase early detection. Ultimately, specialist clinician-primary care provider collaboration will be needed to evaluate new and evolving technologies in screening and diagnosis to address the significant issue of underdiagnosis at the primary care level [33].
MATERIALS AND METHODS
A 19-question survey was created using Google Forms, with questions pertaining to the professional settings of respondents, their opinions on current cognitive screening tools, how they might be improved, and questions about uptake decisions for a hypothetical AI telephone-based screening service (see Supplementary Material). The survey questions were developed by the first author based on a literature review of provider opinions about cognitive screening. Two of the AI-specific questions were taken from a study examining primary care provider opinions on uptake of a telephone screening service for cognitive decline [34]. Responses to the AI-specific questions were measured on a 5-point Likert-type scale whereas the remaining questions required multiple choice or open-ended responses.
A convenience sample of U.S. clinicians specializing in dementia diagnosis were identified from two sources: the Alzheimer’s Association and the American Association of Retired Persons’ Community Resource Finder (https://www.communityresourcefinder.org/), and the Gerontological Society of America’s GSA Connect (https://connect.geron.org/home). The survey link was emailed to 229 clinicians over a 9-month period in 2023 and posted on GSA Connect in November 2023. (Email invitations had also been sent in 2020–2021 to 13 clinicians identified from the Community Resource Finder).
Fifty-two responses were recorded (response rate∼21.5%), although one was dropped from analyses because the respondent indicated that they did not work in a clinical capacity, resulting in a sample size of 51. Responses were anonymous, although respondents were eligible to receive a $10 Amazon gift card by providing their email address, which was later deleted. This study was approved by the Marymount University IRB #460. Data analysis, including descriptive statistics and chi-square analyses were conducted using SPSS version 27, with p < 0.05.
RESULTS
Characterizing the sample
As shown in Table 1, the majority of respondents had medical degrees and/or PhDs and specialized in gerontology, (neuro)psychology, or neurology. Most respondents worked in group settings of 20 or fewer colleagues, in university-affiliated medical centers. The majority of respondents evaluated more than 10 older adult patients a week, with nearly half spending more than 50% of their time conducting dementia evaluations.
Characteristics of the study sample (N=51)
Opinions on current cognitive screeners for MCI
The most notable concerns with current screening tools for MCI pertained to sensitivity and specificity of the instruments (52.8%) and the time-consuming nature of testing (32.2%) (see Fig. 1). The most commonly cited suggestions for how this could be improved were faster and/or shorter screening tests (24.2%) (see Fig. 2).
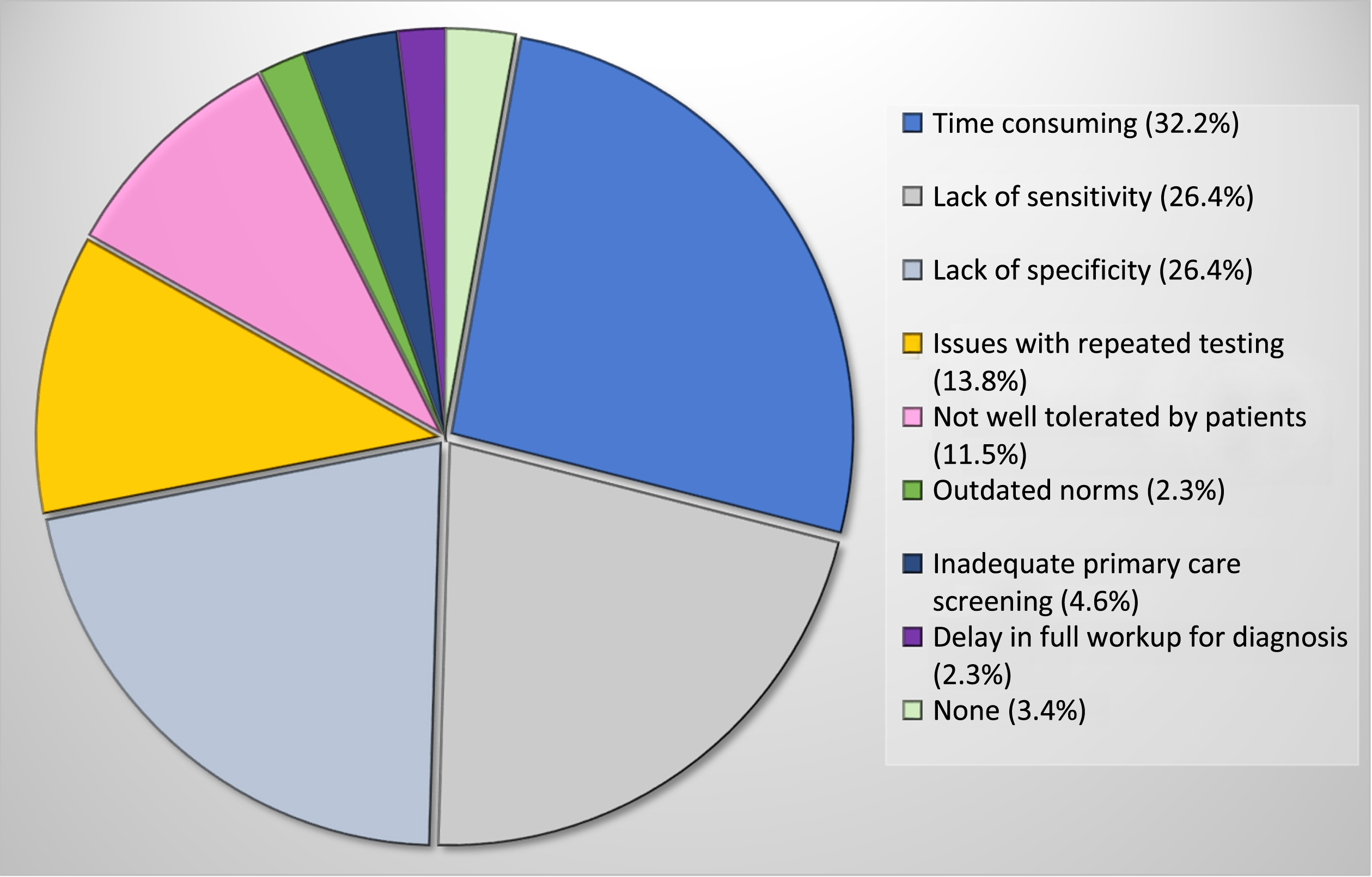
Percentage of total responses citing problems with current cognitive screeners for the identification of MCI. (Respondents could indicate more than one option).
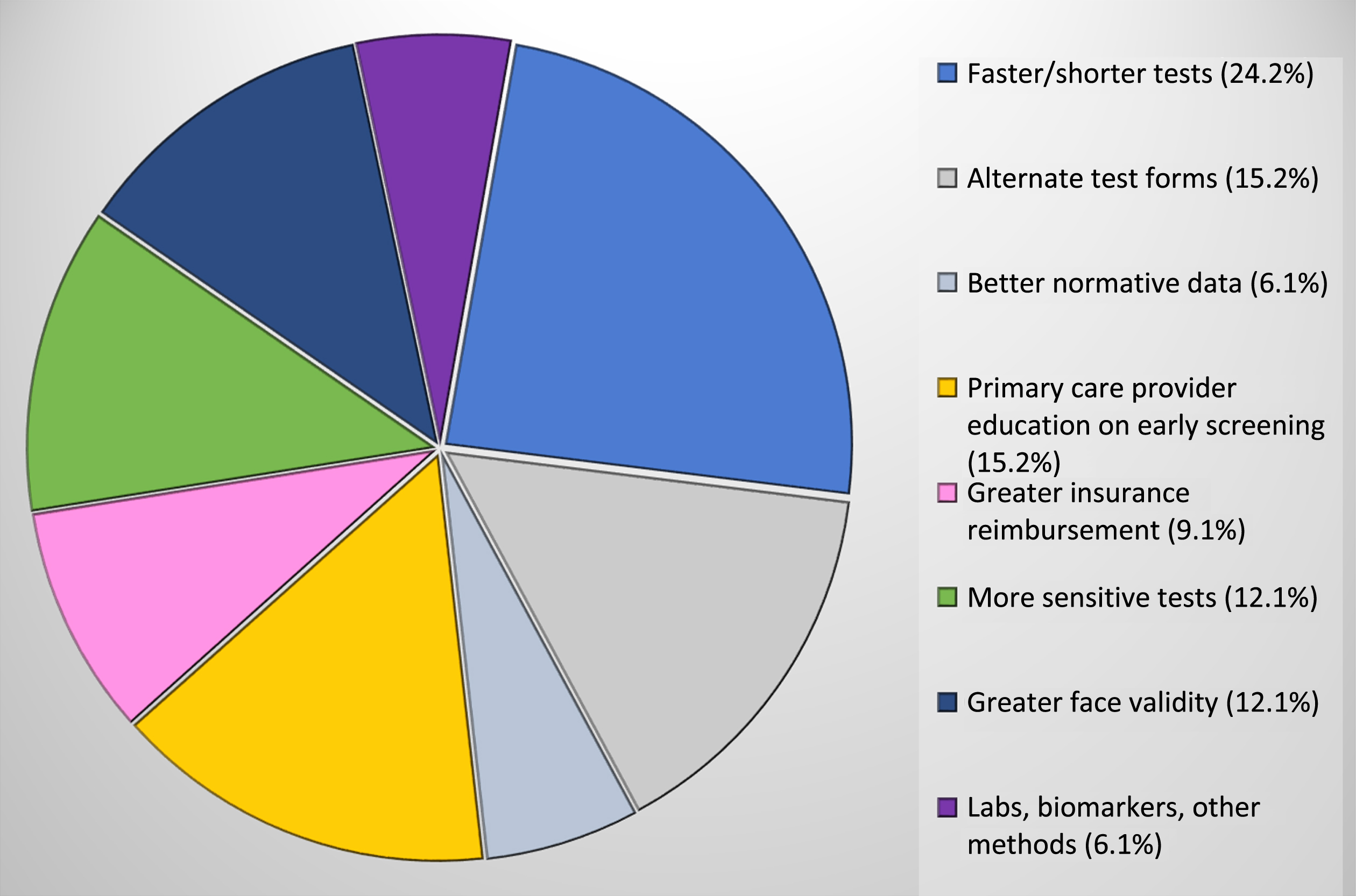
Percentage of total responses citing how current cognitive screeners for the identification of MCI could be improved. (Respondents could indicate more than one option).
Opinions on an (hypothetical) AI-driven telephone screening service
The majority of respondents (78.4%) either agreed or strongly agreed that they would make use of a telephone-based service that could identify MCI. A one-sample chi-square goodness of fit test confirmed that the distribution of all the three types of responses (agree, neutral, disagree) were significantly skewed towards positive opinions (χ2 = 46.71, 2 df, p < 0.001). Opinions on whether patients would make use of a telephone screener were less positively skewed (agree = 50.0%; neutral = 22%; disagree = 28%), but nonetheless still significant (χ2 = 6.52, 2 df, p = 0.038).
Cost was noted as a significant potential barrier to the implementation of a telephone service to identify MCI, with over half (52.9%) of respondents stating that this would influence their decision to adopt (χ2 = 10.71, 2 df, p = 0.005).
The most important characteristics of any proposed telephone service to screen for MCI were identified by respondents as patient tolerability (92.2%), reliability (90.2%), sensitivity (86.2%), and specificity (80.4%), with no significant differences in the proportions of agree/neutral/disagree responses by characteristic (χ2 = 0.47, 3 df, p = 0.925). Respondents provided a variety of preferred options when asked to name standard screeners that would be useful to present side-by-side with speech-based data for comparison purposes, citing the MoCA (38.6%) and MMSE (22.8%) most often. Other preferred screeners noted were the Mini-Cog [35] at 14.9% and ADAS-Cog [36] at 8.8%.
DISCUSSION
Recent evidence suggests that MCI is woefully underdiagnosed in primary care settings [33], arguing not only for improved education and training of primary care providers, but also for the deployment of accurate, rapid, and well tolerated screening tools. The current study surveyed clinicians specializing in the diagnosis of cognitive decline and dementia for their opinions on the current state of cognitive screening for MCI, and they cited several significant concerns. Consistent with previous reports, these concerns primarily revolved around the lack of sensitivity and specificity of the tools and the time it takes to administer, score, and interpret them [31, 32]. While commonly used tests like the MoCA and MMSE are relatively brief, the time taken to administer and score them is not inconsequential when medical appointments can be as short as 15 minutes [37]. Additionally, the MMSE’s lack of sensitivity to the earliest stages of decline is well documented [38, 39], rendering it a poor choice for MCI detection. Several other options are available, yet providers may be unsure of the “best” tests to use and when/how often to use them (e.g., to avoid practice effects with repeated administration).
Respondents’ most cited recommendation for the development of future cognitive screeners was to ensure they be brief, presumably due to the time constraints noted above [11, 40]. The advantage of AI-based screeners, such as those using spoken language, is that they can quantify cognitive decline using only short samples of speech (in the 1–2 minute range). The AI computations themselves can occur almost instantaneously, providing an output in real time. Our work, and that of others, has shown that this approach can accurately differentiate MCI from both healthy aging and Alzheimer’s disease [13, 42], is rapid, and well tolerated by patients [18]. Results of the current study suggest that clinicians are also receptive to adopting a hypothetical AI telephone-based screening service such as this, deeming sensitivity, specificity, reliability and tolerability as especially important characteristics of any new tool. Our research in developing a dashboard-type output to aid clinicians in the interpretation of an individual’s results suggests that both specialist clinicians and primary care providers alike could adopt the technology with little additional training required [17]. The current findings suggest that side-by-side comparisons with commonly used screeners such as the MoCA and MMSE would be a valuable addition to this dashboard.
Several limitations should be noted in this study, with the potential for response bias being the most important. A response rate of only 21.5% means that the majority of specialist clinicians who were emailed the survey link did not respond, notably limiting the study’s external validity. While low, a response rate such as this is not uncommon from healthcare providers [43, 44] and several studies have proposed methods to increase survey participation in this population [45, 46]. A second limitation is that the questions regarding the hypothetical AI-driven telephone screener were vaguely worded, such that respondents may each have envisaged quite different versions of said tool, and this in turn may have influenced results. For example, we never stated specifics such as whether the service would be fully automated versus having human interaction, which tasks would be used to elicit speech samples, and how the speech samples would be recorded, transmitted and analyzed. Whether and how any of these elements were considered by respondents is unknown. Hence, a more detailed and realistic depiction of an AI telephone screening tool will be an integral component of future work. Documented clinician concerns over data privacy [22], coupled with the sheer number of AI-driven tools already available, most with limited transparency, means that patient autonomy and privacy should be central ethical concerns for any clinician considering their use.
While respondents in the current study largely agreed that their older patients would use a telephone-based screening service, there was a notable minority (28%) who did not think that they would, for reasons we did not investigate. It is possible, at least in part, that individual interpretations of what this “service” would entail resulted in a variety of both positive and negative responses. The telephone is ubiquitous in most people’s homes and allows for the remote administration of screening tests, but may not be appropriate for patients with hearing, speech, or severe cognitive deficits. Tolerability of fully automated tools may also be an issue for some older adults who would prefer the opportunity to interact with a human [47].
Study limitations notwithstanding, these findings provide valuable insights on the current state of cognitive screening for MCI from experts using these tools on a daily basis. The proliferation of AI-driven healthcare technologies presents a great opportunity to address the shortcomings of common cognitive screeners through the intelligent design of accurate, brief, and well tolerated tools in future.
AUTHOR CONTRIBUTIONS
Catherine Diaz-Asper (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Visualization; Writing – original draft; Writing – review & editing); Chelsea Chandler, PhD (Conceptualization; Writing – review & editing); Brita Elvevåg (Conceptualization; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This work was supported by a research grant to CDA from Rotary USA’s Coins for Alzheimer’s Research Trust (CART) Fund.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to ethical restrictions.