
Abstract
Background:
Alzheimer’s disease has become increasingly prevalent among the older population, leading to significant social and economic burdens. Transcranial photobiomodulation (tPBM) has shown promise as a cognitive intervention for enhancing cognitive efficiency in healthy older adults, and individuals with mild cognitive impairment and Alzheimer’s disease. However, determining the optimal tPBM dosage is crucial for ensuring effective and efficient intervention.
Objective:
This study aimed to compare the effects of different dosages in a single tPBM session on cognitive efficiency in healthy older adults.
Methods:
In this randomized controlled trial, 88 healthy older participants were assigned to either a single dose (irradiance = 30 mW/cm2, fluence = 10.8 J/cm2; n = 44) or a double dose (irradiance = 30 mW/cm2, fluence = 21.6 J/cm2; n = 44) tPBM session. Cognitive efficiency was assessed using functional near-infrared spectroscopy during a visual working memory span task.
Results:
The single dose group exhibited significantly greater cognitive efficiency enhancement, indicated by a more pronounced reduction in oxygenated hemoglobin during a challenging task level (span level 9) (p = 0.021, d = 0.50), and better working memory task performance (p = 0.045, d = 0.31). Furthermore, participants with better visuospatial abilities demonstrated greater improvement after a single dose (r = –0.42, p = 0.004). In contrast, participants with varying cognitive function did not exhibit additional benefits from a double dose (r = –0.22–0.15, p = 0.16–0.95).
Conclusions:
These findings suggest that higher tPBM dosages may not necessarily result in superior cognitive improvement in older adults.
Keywords
INTRODUCTION
The prevalence of Alzheimer’s disease (AD) among older individuals has increased significantly in recent decades,1,2, 1,2 leading to substantial social and economic burdens.1,3, 1,3 Therefore, there is a critical need to identify strategies to maintain or improve brain function in aging populations. Given the significance of early intervention in delaying or even preventing the development of AD, research has been focused on intervening during preceding stages such as mild cognitive impairment or even at the preclinical stage of AD. Transcranial photobiomodulation (tPBM) has emerged as a promising non-pharmacological intervention, attracting attention for its potential to enhance cognitive function in healthy older adults and alleviate cognitive impairments in patients with neurodegenerative conditions. This technique involves applying low-power density red (600–670 nm) and near-infrared light (800–1100 nm) stimulation transcranially to the scalp, aiming to improve brain function.4,5, 4,5 Previous studies have proposed various brain mechanisms underlying the effects of tPBM, including increased cerebral blood flow, 6 enhanced tissue oxygenation,7,8, 7,8 and elevated production of adenosine triphosphate,8,9, 8,9 which supports neural activity and enhances brain function.8,9, 8,9
Several studies have reported positive outcomes following tPBM interventions in diverse populations, 10 including healthy older adults11,12, 11,12 and individuals with mild cognitive impairment,13,14, 13,14 dementia,15,16, 15,16 and Parkinson’s disease.17,18, 17,18 Participants who underwent tPBM for several weeks demonstrated improvements in cognitive functions such as memory, 19 attention, 20 executive function, 21 and language. 22 In addition, tPBM has been associated with positive effects on non-cognitive domains, including reductions in depressive and anxiety symptoms,23,24, 23,24 as well as improvements in mood 25 and sleep quality. 26 Previous studies utilizing functional near-infrared spectroscopy (fNIRS) have indicated that tPBM may enhance cognitive efficiency by reducing oxygenated hemoglobin (HbO), a sensitive indicator of cognitive effort, 27 required to complete tasks involving high memory loads. 28 Specifically, participants who received 350 s of active tPBM targeting the prefrontal cortex exhibited a significant reduction in working memory-related HbO levels in that area after the intervention while maintaining a similar performance level compared to their baseline. This finding suggests that participants achieved comparable task performance with reduced cognitive effort, as indicated by decreased working memory-related HbO levels. The observed effect has been reported in previous studies on single tPBM trials involving healthy younger adults, 29 healthy older adults, 28 and older adults with mild cognitive impairment. 14 It has also been observed following repeated tPBM sessions. 30
The effect of tPBM may vary depending on several factors, such as the variation in the placement of tPBM light.19,31,32, 19,31,32 The dosage of tPBM is also a critical factor that affects the tPBM effect. However, despite the promising findings on cognitive improvement from tPBM, determining the optimal dosage of tPBM remains a significant challenge. One of the main issues is the limited understanding of the extent to which near-infrared light is absorbed and penetrates the human brain. Existing studies have predominantly relied on animal33,34, 33,34 and cell-based models,35,36, 35,36 and extrapolating the dosage from these studies to human brain tissue may not be accurate. This concern is highlighted by the negative results observed in a previous large tPBM trial on acute stroke, 37 which is believed to be attributed to ineffective amounts of light reaching the brain. 38 Moreover, the biphasic dose response of near-infrared light stimulation presents another challenge. This phenomenon refers to the beneficial effects of near-infrared light increasing with dosage until a peak is reached, beyond which further increases can lead to diminishing effects and potentially even harmful consequences. 39 Despite several randomized control trials supporting the use of tPBM in enhancing cognitive function, there remains a lack of direct comparisons between different dosages within a single tPBM trial. Therefore, it is crucial to ascertain the optimal tPBM dosage to maximize intervention effects, prevent inefficacy such as diminished or null effects, and avoid potential overdose (i.e., adverse effects contrary to the intended intervention). By gaining a more comprehensive understanding of this matter, it will be possible to establish intervention protocols that effectively improve cognitive function, alleviate social burdens, and reduce healthcare costs.
Previous studies have aimed to determine the commonly used parameters of transcranial photobiomodulation (tPBM) that have shown effectiveness. For instance, a systematic review reported a range of irradiance from 1.7 mW/cm2 to 350 mW/cm2, and a range of fluence from 0.9 J/cm2 to 42 J/cm2. 40 However, due to the heterogeneous results, it remains inconclusive to determine the definitive effective parameters for humans, making it difficult to establish evidence-based guidelines for therapeutic applications of tPBM. 40 Another study found that in human studies, an irradiance of 20 to 25 mW/cm2 and fluence of 1 to 10 J/cm2 were commonly employed. 10 However, the optimal dose may vary depending on the population being treated. In studies involving individuals with psychological disorders, a scalp irradiance of 250 mW/cm2 and fluence of 60 J/cm2 were more frequently tested, and cognitive enhancement was observed. 41 This suggests that the optimal dose may differ among different populations. Besides, the commonly used parameters reported may not necessarily represent optimized doses for cognitive enhancement. Therefore, comparing the effects of different doses is necessary to determine the optimal dosage.
Despite the importance of dose optimization, there is limited research on dose response in single-session tPBM. A recent study compared the effects of high and low doses of tPBM in older adults, revealing that the high-dose group exhibited increased resting-state functional connectivity and improved visual search and processing speed. 42 However, methodological limitations warrant further investigation, including small sample size and lack of between-group statistical analyses. Additionally, it remains unclear whether different intervention schedules suit individuals with varying cognitive abilities within the older adult population.
The present study aimed to investigate the effects of different tPBM dosages within a single session on cognitive efficiency in healthy older adults. Cognitive efficiency was assessed by measuring changes in levels of HbO using fNIRS during a visuospatial working memory task. Participants received either a single dose or a double dose of tPBM, with the duration of near-infrared light exposure varied accordingly. Furthermore, the study also explored whether older adults with higher cognitive abilities exhibited greater improvement with one intervention dose, while those with lower cognitive abilities showed more improvement with the other dose.
MATERIALS AND METHODS
Participants
Previous studies have reported a medium to large effect size after tPBM.14,28,29, 14,28,29 Assuming a partial eta square of 0.1, a total of approximately 76 participants are needed to achieve a power of 0.8 at a 0.05 alpha level. Taking into account a 10% data loss due to motion artifacts or incomplete assessments, at least 84 participants were required for this study. Therefore, a total of 88 individuals, aged between 50 and 80 years, were recruited as participants for this study. The inclusion criteria required participants to understand the Chinese language and have a normal or corrected-to-normal vision. There were no restrictions on the use of herbal or pharmaceutical products to treat participants’ medical conditions such as high blood pressure or diabetes. However, potential participants with a reported history of head injury, neurological or psychiatric disorders, or physical disabilities that may impede task performance (e.g., color blindness or motor disabilities) were excluded from the study. This study was conducted in accordance with the Declaration of Helsinki of the World Medical Association Assembly and was approved by the Joint Chinese University of Hong Kong–New Territories East Cluster Clinical Research Ethics Committee. Informed consent was obtained from all participants before their participation.
Participants who met the criteria for possible mild cognitive impairment, as operationalized by Jak/Bondi’s criteria, 43 were excluded from the study. These criteria included having impaired scores (defined as more than one SD below the age- and education-corrected normative mean) on two of the six neuropsychological measures in the same cognitive domain (memory, language, or attention/executive function) or having impaired scores in each of the three cognitive domains measured. In addition, participants with a score below 21 on the Hong Kong version of the Montreal Cognitive Assessment were also excluded. None of the participants in either the single dose group or the double dose group met the aforementioned criteria, indicating that all participants in both groups were cognitively normal.
Procedures
All participants underwent a baseline neuropsychological assessment and an fNIRS session before the tPBM administration. During the fNIRS session, participants performed the visual working memory span task while their prefrontal hemodynamic activity was recorded. Participants were instructed to remain still and minimize head and body movements to prevent motion artifacts. In addition, demographic information such as age, gender, and educational level was collected from each participant. Following the baseline assessment, participants were divided into one of two groups randomly: the single dose group (n = 44) or the double dose group (n = 44). The single dose group received a single 6-min tPBM stimulation session, whereas the double dose group underwent a 12-min tPBM stimulation session. It should be noted that all participants were informed that the investigation aimed to assess the effects of tPBM, without disclosing the specific experimental design involving the comparison of tPBM effects across different durations. Consequently, the occurrence of a placebo effect was deemed less probable. Immediately after the tPBM session, both groups repeated the visual working memory span task while their prefrontal hemodynamic activity was recorded using fNIRS.
Neuropsychological assessment
All recruited participants first underwent a standardized neuropsychological assessment to ensure there were no differences in brain function between groups after group assignment. The assessment included various tests measuring memory, executive function, attention, and mental flexibility. These tests included the Hong Kong List Learning Test, 44 Rey-Osterrieth Complex Figure Test, 45 Digit Span Test, 46 Shape Trail Test, 47 Five-Point Test, 48 Boston Naming Test, 49 Category Fluency Test, 50 and the Hong Kong version of the Montreal Cognitive Assessment to assess global cognitive function. 51 All of these tests were selected because they are widely used for classifying MCI.47,52, 47,52 In addition, participants’ depressive and anxiety symptoms were assessed using the Chinese version of the Geriatric Depression Scale 53 and the 10-item Geriatric Anxiety Scale. 54
Visual working memory span task
Considering potential individual differences in education within this study, as well as cultural variations across different studies, a visual working memory task was employed over a verbal one. The visual working memory span task utilized in this study was adapted from a previously conducted fNIRS study that investigated the prefrontal hemodynamics of older adults with preserved visuospatial working memory function, which reported an increase in relative HbO levels with heightened cognitive task demand. 55 In this task, each trial started with a control task period lasting 10 s, during which participants were instructed to focus their attention on a fixation cross displayed on the center of the computer screen. Following the control task, nine blue square blocks were presented on the screen for a duration of one second. Subsequently, a sequence of blocks transitioned from blue to yellow, with each block changing color sequentially every second. Participants were instructed to memorize the sequence in which the blue blocks transformed into yellow. After the encoding period, a retrieval period followed. During this phase, a “start” cue appeared in the upper right corner of the screen, accompanied by a “finish” button positioned in the lower right corner. Participants needed to reproduce the sequence by selecting the square blocks on the screen in the same order as they were originally presented. After that, participants had to click the “finish” button to complete their responses (Fig. 1A). The task consisted of 18 trials, with each span sequence containing two trials. The span sequences ranged from two blocks to nine blocks in length (Fig. 1B). Before the main task began, participants underwent two practice trials to familiarize themselves with the task. The presentation of stimuli was performed using PsychoPy version 2022.2.4. 56 The visual working memory span score was calculated based on the longest sequence length that participants correctly reproduced in any one trial out of two trials for each span sequence. Notably, the task continued even after participants reached their longest correct span length.

A) Flow diagram of the visual working memory span task in trial with span level 2. B) The overall flow of the visual working memory span task. C) The locations of source and detector probes, channel arrangement, and projected cortical locations of the fNIRS system. The source probes are denoted by red dots, while the detector probes are indicated by blue dots. The yellow lines represent the 16 fNIRS measurement channels.
Hemodynamic measures
To measure prefrontal hemodynamic activity during the visual working memory span task, a 16-channel OEG-SpO2 system (Spectratech Inc., Tokyo, Japan) was employed. This system utilizes near-infrared light with wavelengths of 770 and 840 nm to estimate the relative concentration of HbO in participants’ prefrontal cortex, using the modified Beer-Lambert law. The OEG-SpO2 system consisted of six sources and six detectors arranged alternately in a 2×6 matrix configuration (Fig. 1C), with a separation distance of 3 cm between the sources and detectors. The center of the bottom probe was positioned approximately on FpZ, following the international 10/20 system for electrode placement. The sampling rate of the OEG-SpO2 was set at 12.21 Hz.
Transcranial photobiomodulation
The tPBM intervention was administered using a custom-built device with 81 light-emitting diodes (LEDs). Each LED emitted light of wavelength 810 nm in a continuous wave. These LEDs, measuring approximately 1 cm2 each, were positioned over the prefrontal, parietal, and temporal regions on both sides of the participants’ heads, approximately at FpZ, Fp1, Fp2, F7, F8, T7, T8, Fz, F3, F4, Cz, C3, C4, P3, and P4 based on the international 10/10 system. The selection of the targeted areas was based on previous studies that have reported a positive effect on cognitive function.11,14,57, 11,14,57 In the single dose group, the tPBM session lasted for 6 min, while in the double dose group, the procedure was repeated, resulting in a total session duration of 12 min. During the session, participants were instructed to close their eyes while the tPBM device operated. There were nine clusters of LEDs, each delivered 30 mW/cm2 and 1.8 J/cm2 of stimulation per min. The total energy delivered per cluster was 16 J per min. To avoid overheating, the tPBM intervention involved six one-min stimulation sessions, with one cluster or two clusters used each time. For the single dose group, the total energy delivery over the six-min session was 160 J (irradiance = 30 mW/cm2, fluence = 10.8 J/cm2). In the double dose group, the total energy delivered was 320 J (irradiance = 30 mW/cm2, fluence = 21.6 J/cm2). The dosage and duration for tPBM were determined based on a previous systematic review of tPBM studies aiming to enhance cognitive function. 10 Specifically, the reviewed studies demonstrated varying fluence ranging from 7 J/cm2 to 120 J/cm2, irradiance ranging from 12 mW/cm2 to 285 mW/cm2, and durations ranging from 2.5 min to 20 min. It is noted that none of the participants reported any discomfort or adverse effects during or after the tPBM intervention.
fNIRS data preprocessing
The fNIRS raw intensity data were converted into the HomER3 data format 58 for further preprocessing. First, the intensity signal was converted to optical density changes using the Intensity2OD function. Next, a low-pass filter with a cutoff frequency of 0.1 Hz was applied to remove high-frequency noise using the hmR_BandpassFilt function. The filtered optical density data was then converted to changes in relative HbO and HbR using the modified Beer-Lambert law implemented in the hmR_OD2Conc function, with a default differential pathlength factor of 6 for both wavelengths. A correlation-based signal improvement (CBSI) technique, a technique that improves the signal quality and reduces noise based on the negative correlation between HbO and HbR, 59 was applied using the hmrR_MotionCorrectCbsi function. The CBSI-corrected HbO and HbR data were then baseline corrected using the data recorded during the 10-s control task period before the start of the task. The baseline correction was performed using the hmrR_BlockAvg function. After baseline correction, the data were averaged across all time points within each trial and then across the two trials for each span length. Since the baseline corrected HbR signal mirrors the HbO signal after CBSI correction, only the HbO data was considered for further analysis.
Data analysis
Firstly, independent t-tests and chi-square tests were employed to compare the single dose group and the double dose group at baseline, evaluating demographic variables and performance on the baseline neuropsychological assessment. Next, a repeated measures ANOVA was conducted to assess changes in relative HbO in both groups. This analysis examined the interaction between time (before tPBM, after tPBM), span level (span level 2 to level 9), and channel (channel 1 to channel 16). In addition, a mixed ANOVA was performed to evaluate between-group differences in the changes in relative HbO. To further investigate any significant within-group and between-group differences, post-hoc paired t-tests and independent t-tests were employed, respectively. The Levene test was utilized to assess the homogeneity of variances for the independent t-tests. In cases where the sphericity assumption was violated for the repeated measures ANOVA and mixed ANOVA, the Greenhouse-Geisser correction was applied. Effect sizes were estimated using Cohen’s d and partial eta squared (
RESULTS
Demographics and baseline neuropsychological assessment performance
The age, gender, years of education and baseline neuropsychological assessment performance of both the single dose group and the double dose group are presented in Table 1. There were no significant differences between the two groups in terms of demographic variables (p = 0.13–0.65). Furthermore, both groups showed similar performance in the neuropsychological assessment (p = 0.18–0.89), and similar levels of depressive and anxiety symptoms (p = 0.32–0.74).
Demographic information and neuropsychological assessment performance of the single dose group and the double dose group
HK-MoCA, Hong Kong version of Montreal Cognitive Assessment. aChi-squared test was performed to evaluate group difference. bOne missing data. cFive missing data.
Changes in HbO during visual working memory span task after tPBM
The changes in relative HbO during the visual working memory span task were analyzed in both the single dose and double dose groups. Before tPBM, there were no significant between-group differences in relative HbO at any of the span levels across all channels (p = 0.11–0.997). The time×span×channel interaction was also not significant in both the single dose group (F[10.58, 444.37] = 1.14, p = 0.33,
In the single dose group, there was a significant time×span interaction (F[2.29, 98.35] = 13.93, p < 0.001,
Results of repeated measures ANOVA and mixed ANOVA in HbO
SS, sum of squares; dfNum, degrees of freedom numerator; dfDen, degrees of freedom denominator; MS, mean square;
Finally, comparing the changes in relative HbO between the single dose group and the double dose group, there was a significant group×span×time interaction (F[2.53, 217.57] = 3.84, p = 0.02,

A) Changes in HbO in the single dose group (n = 44) and double dose group (n = 44). The greater the decrease in HbO, the more improvement in cognitive efficiency. A significant group×span interaction was found (p = 0.015). The error bars represent±one standard error of the mean. Asterisks indicate the significance levels of independent t-tests for group differences in changes in HbO. †p < 0.06, *p < 0.05. B) Prefrontal activation maps depicting changes in HbO in the prefrontal cortex (in μM) during the visual working memory span task at span level 9. Individual channel data were utilized to create the activation maps. The color red represents less decrease in prefrontal activation after tPBM, while blue color represents more decrease in prefrontal activation after tPBM. In other words, the more intense the blue color, the greater the improvement in cognitive efficiency.
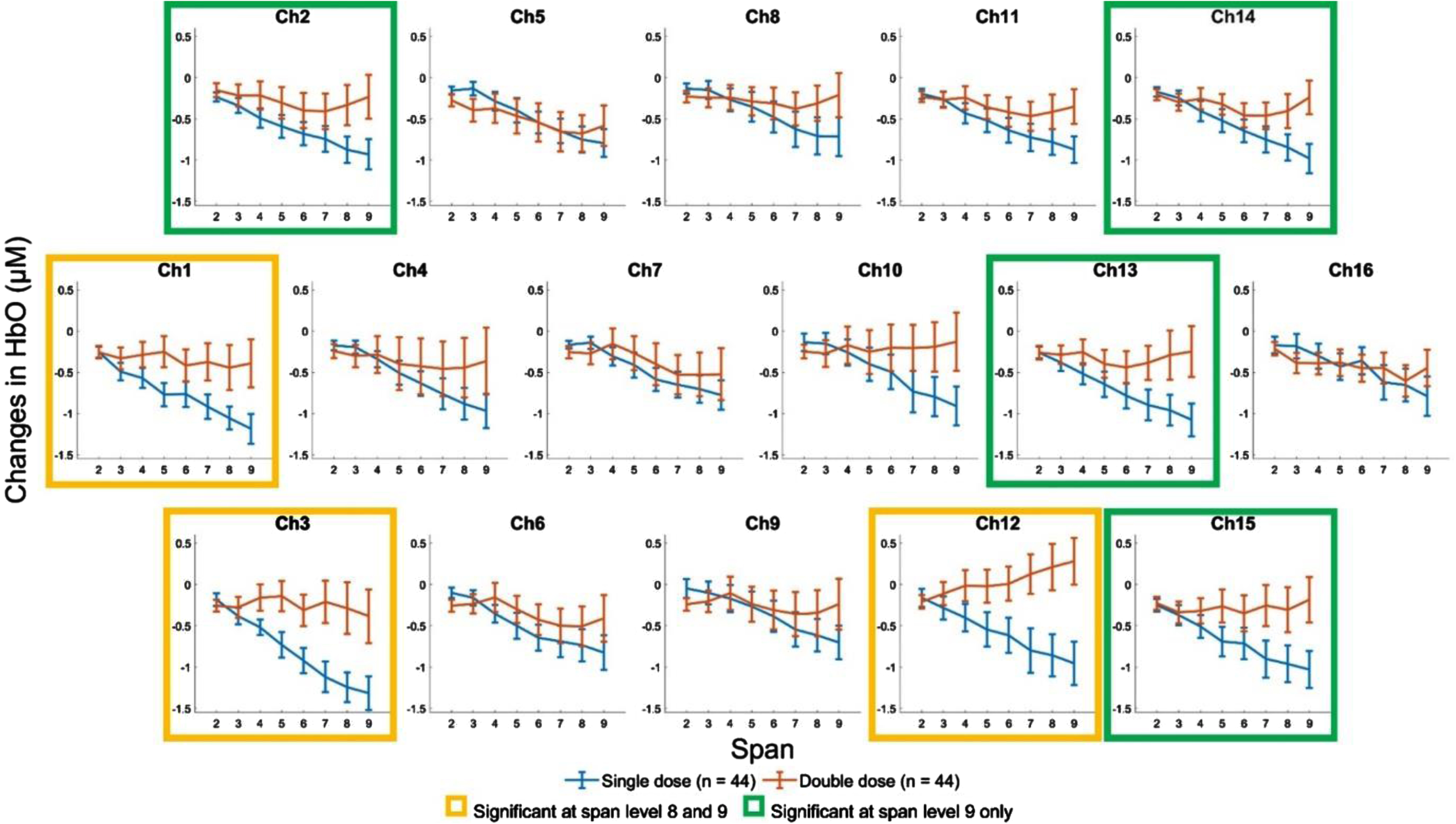
The changes in HbO in single dose group (n = 44) and double dose group (n = 44) across all fNIRS measurement channels at all span levels. The greater the decrease in HbO, the more improvement in cognitive efficiency. The error bars represent±one standard error of the mean. In terms of changes in HbO, there was a marginally significant group difference at span level 8 and a significant group difference at span level 9. The square borders highlight the channels that yielded significant group difference at these two levels, where yellow borders represent significant difference at both span levels 8 and 9, and green borders represent significant difference at span level 9 only.
Changes in performance on visual working memory span task after tPBM
Before receiving tPBM, the single dose group had an average visual working memory span score of 5.70 (SD = 1.37), while the double dose group had an average of 5.73 (SD = 1.15). The difference in span score between the two groups was not significantly different (t(86) = 0.084, p = 0.93). After receiving tPBM, the single dose group demonstrated a significant improvement in visual working memory span score from 5.70 (SD = 1.37) to 6.09 (SD = 1.49) (t(43) = 2.06, p = 0.045, d = 0.31). Similarly, the double dose group also showed an improvement from 5.73 (SD = 1.15) to 6.05 (SD = 1.18), but this increase did not reach statistical significance (t(43) = 1.46, p = 0.15, d = 0.22). Importantly, the group×time interaction was not significant (F[1.00, 86.00] = 0.056, p = 0.81,
Individual responsiveness to single and double dose tPBM
Based on the findings of the current sample, there was a large variation in cognitive efficiency changes. For instance, in the single tPBM group, the changes in HbO at span level 9 ranged from –3.57μM to +1.73μM. Similarly, in the double tPBM group, the range was from –3.42μM to +3.41μM. These results suggest that there may be individual differences in responsiveness to the tPBM effect. That is, individuals with higher cognitive abilities may show a greater effect from one tPBM dose, and individuals with lower cognitive abilities may show a greater effect from the other tPBM dose. To further explore this, correlation and regression analysis were conducted to examine the relationship between the neuropsychological assessment performance and the changes in HbO at span level 9.
The results of the correlation analysis for both groups are presented in Table 3. The analysis of the single tPBM group revealed significant correlations between the changes in HbO and the copy score (r = –0.42, p = 0.004), immediate recall (r = –0.36, p = 0.017), and delayed recall (r = –0.33, p = 0.030) of the Rey-Osterrieth Complex Figure Test, with better task performance associated with a greater decrease in HbO (Fig. 4). No significant correlations were found between the changes in HbO and other neuropsychological assessment performance scores (r = –0.25–0.18, p = 0.097–0.99). Stepwise linear regression analysis revealed that the changes in HbO could be predicted significantly by the copy score of the Rey-Osterrieth Complex Figure Test only (β=–0.13, R2 = 0.18, F[1.00, 42.00] = 9.22, p = 0.004). Therefore, the results suggest that individuals with better visuospatial ability seemed to benefit more from the single dose tPBM.
Pearson’s correlation coefficients between the changes in HbO at span level 9 and neuropsychological assessment performance
HK-MoCA, Hong Kong version of Montreal Cognitive Assessment. aOne missing data.

The relationship between the changes in HbO at span level 9 and the copy score of the Rey-Osterrieth Complex Figure Test. Significant correlations were found in the single dose group (r = –0.42, p = 0.004), but not in the double dose group (r = –0.036, p = 0.82). The greater the decrease in HbO, the more improvement in cognitive efficiency.
For the double tPBM group, there were no significant correlations between the changes in HbO and other scores in neuropsychological assessment (r = –0.22–0.15, p = 0.16–0.95). Furthermore, stepwise linear regression analysis showed that none of the variables was found to significantly contribute to the prediction model. Therefore, the results suggest that individuals with varying cognitive abilities tended to benefit more from a single dose of tPBM.
DISCUSSION
Despite tPBM demonstrating promising results in enhancing cognitive function among older individuals across the AD continuum, determining the optimal dosage of tPBM remains a major challenge in the field. The present study aimed to address this challenge by investigating changes in cognitive efficiency, measured using fNIRS, during a visual working memory span task after a tPBM session of single (i.e., fluence of 10.8 J/cm2 and irradiance = 30 mW/cm2) and double (i.e., fluence of 21.6 J/cm2 and irradiance = 30 mW/cm2) doses. The results showed that both the single dose and double dose groups exhibited a significant decrease in relative HbO levels after tPBM. Interestingly, the double dose group maintained their visual working memory span score, while the single dose group even showed improvement. These findings suggest enhancements in cognitive efficiency. Moreover, when comparing the improvement between the two groups, the single dose group exhibited a significantly greater decrease in relative HbO levels at more demanding span levels (i.e., span level 9) compared to the double dose group. Despite this, both groups showed comparable improvement in visual working memory span score, indicating that the single dose group demonstrated greater enhancement in cognitive efficiency. These results suggest that a lower dose may be more efficient and that a higher dose does not necessarily lead to better intervention effects.
The present findings are consistent with the biphasic dose response of near-infrared light stimulation, wherein a higher dose of tPBM may result in an attenuated intervention effect compared to a lower dose. 39 A previous study conducted on primary cortical neurons isolated from embryonic mice revealed a significant reduction in adenosine triphosphate and mitochondrial membrane potential when a fluence of 30 J/cm2 was applied, in comparison to a fluence of 10 J/cm2 delivered at a constant irradiance of 25 mW/cm2. 39 The present findings further support the biphasic dose response phenomenon in humans, which observed that a fluence of 10.8 J/cm2 resulted in greater improvement compared to 21.6 J/cm2, with a constant irradiance of 30 mW/cm2. These findings highlight the significance of conducting further investigations into the biphasic dose-response phenomenon in humans. Specifically, it is important to explore the effects of additional variations in tPBM parameters, including both increased and decreased dosages beyond the range of 10.8 J/cm2 and 21.6 J/cm2. This will help enhance our understanding of the dosage-response relationship. Besides, the results of the present study also highlight the importance of careful intervention protocol design to optimize outcomes. However, our results were inconsistent with a previous study on healthy older adults, which reported better outcomes after a high dose of tPBM. 42 In that study, only the high dose group (i.e., transcranial fluence of 52 J/cm2 and intranasal fluence of 18 J/cm2) showed a significant improvement in cognitive function, while the low dose group (i.e., transcranial fluence of 26 J/cm2 and intranasal fluence of 9 J/cm2) did not. This inconsistency suggests that there may be no universally optimal dosage for different intervention devices. In addition, the dose response may be influenced by various intervention parameters, such as the wavelength of light, which affects the depth of tissue penetration. 60 Therefore, further investigation into the interaction between different intervention parameters is necessary to fully understand the dose response. It is important to note that our findings do not invalidate the biphasic dose response, as the previous study may indicate the low dose group lacked sufficient energy for improvement, while the present study suggests that the single dose group already received enough energy for improvement, but further increase in dose resulted in an attenuated effect.
The observed improvement in cognitive efficiency after a single tPBM session aligns with previous studies that have shown enhanced cognitive efficiency in healthy older adults and older adults with mild cognitive impairment.14,28, 14,28 The present study further explored performance changes in response to single and double tPBM dosages. Unlike previous studies on healthy older adults, which did not find a significant increase in visual working memory span score; 28 the single dose group in the present study demonstrated a significant improvement in behavioral performance during the visual working memory span task. It is worth noting that both studies consistently showed a similar effect size of around 0.3, suggesting that the non-significance in the previous study may have been due to insufficient statistical power. Besides, the double dose group in the present study did not show a significant improvement in behavioral performance. Although there was a significant main effect of time, indicating decreases in relative HbO after tPBM, there was no significant interaction effect between time and span level. This finding is in line with previous studies that have suggested that tPBM can make a cognitively demanding task less arduous.14,28,29, 14,28,29 Therefore, it is consistent with the idea that the effect of tPBM attenuated, leading to less improvement in cognitive efficiency at higher levels of cognitive demand compared to the single dose group. As a result, there was no interaction between time and span levels observed in the double dose group.
Besides, it was found that the enhancement in cognitive efficiency is primarily observed in the bilateral sides of the prefrontal cortex. Previous neuroimaging studies have reported the activation of these regions when the participants performed a visual working memory task.61–63 Based on the present findings, it is postulated that tPBM could potentially be effective in enhancing cognitive efficiency within the brain regions specifically involved in completing the cognitive task. Consequently, a decrease in brain activation was observed in the bilateral sides, rather than the medial side, in the present study. Among the various experimental paradigms employed in fNIRS research, working memory has been extensively investigated.64–66 In the present study, a visual working memory task was chosen due to potential variations in participants’ educational backgrounds and the cultural differences. Since this study solely focused on visual working memory, future research could explore cognitive domains beyond visual working memory and investigate the cognitive enhancements achieved by stimulating different brain regions.
Furthermore, in addition to understanding the dose response, the present study investigated whether certain individuals benefit more from a single dose of tPBM, while others benefit more from a double dose. The results indicated that individuals with varying cognitive abilities did not show a significant relationship between cognitive function and the changes in HbO at span level 9 after a double dose of tPBM. This suggests that individuals with different cognitive functions tended to benefit more from a single dose of tPBM than a double dose. Moreover, it was found that individuals with better visuospatial abilities were more responsive to the effects of tPBM after a single dose intervention. The results suggest that tPBM intervention may be particularly beneficial for early prevention of cognitive decline when cognitive function is still not impaired at this stage. Due to the relatively small sample size, the statistical power to detect small effects may be limited. Therefore, no correction for multiple comparisons was performed in this study. Nevertheless, these findings offer valuable insights for conducting a larger-scale study in the future.
The finding of the present study indicate that a fluence of 10.8 J/cm2 and irradiance = 30 mW/cm2 yielded more improvement compared to a fluence of 21.6 J/cm2 with the same irradiance in cognitively normal older adults. These results suggest that targeting a fluence of 10.8 J/cm2 and an irradiance of 30 mW/cm2 may be appropriate for this specific population. However, it is important to note that these findings cannot be generalized to different populations, as the present study did not investigate the effects of these two doses in other populations. Future research could investigate the appropriate dose for diverse populations, including individuals of varying ages and both healthy and clinical populations. In addition, it is crucial to consider that higher doses may not necessarily yield better outcomes, as the present study demonstrated.
The present study focused on investigating the immediate effects of a single tPBM session. However, the effects of multiple tPBM sessions conducted over several days were not explored. Considering that typical tPBM interventions last several weeks or even months, 10 it is important to examine the underlying changes in hemodynamic responses and determine whether the effects accumulate over the course of the intervention. Doubling the dose in a single tPBM trial differs from doubling the fluence in an intervention lasting for an extended period. It is possible that cognitive efficiency may improve progressively with each stimulation session, suggesting a cumulative nature of effects. Therefore, further research could be conducted to explore the potential cumulative effects of tPBM interventions and their impact on cognitive improvement.
In conclusion, the present study suggests that different doses of tPBM have varying effects on cognitive efficiency in older adults. Specifically, a session of a single tPBM dose demonstrated greater enhancement in cognitive efficiency compared to a double dose tPBM. These findings suggest that a higher dose does not necessarily lead to better outcomes. These results also provide valuable insights for the development of intervention plans in the future. Further studies should be made to investigate the response to different intervention parameters to determine an optimal intervention plan. In addition, a follow-up assessment can also be considered in future studies to evaluate the cognitive improvement a few weeks after tPBM.
AUTHOR CONTRIBUTIONS
Tsz-lok Lee (Conceptualization; Formal analysis; Investigation; Methodology; Validation; Writing – original draft); Agnes S. Chan (Conceptualization; Methodology; Resources; Supervision; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank Quin Chan, Zihan Ding, Lizhi Guo, Tinsley Li, Sophia Sze, and Hilvin Yu for their assistance in the participant recruitment and data collection for this study.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author.