
Abstract
Background:
Alzheimer’s disease (AD) is the most common neurodegenerative disorder which primarily involves memory and cognitive functions. It is increasingly recognized that motor involvement is also a common and significant aspect of AD, contributing to functional decline and profoundly impacting quality of life. Motor impairment, either at early or later stages of cognitive disorders, can be considered as a proxy measure of cognitive impairment, and technological devices can provide objective measures for both diagnosis and prognosis purposes. However, compared to other neurodegenerative disorders, the use of technological tools in neurocognitive disorders, including AD, is still in its infancy.
Objective:
This report aims to evaluate the role of technological devices in assessing motor involvement across the AD spectrum and in other dementing conditions, providing an overview of the existing devices that show promise in this area and exploring their clinical applications.
Methods:
The evaluation involves a review of the existing literature in the PubMed, Web of Science, Scopus, and Cochrane databases on the effectiveness of these technologies. 21 studies were identified and categorized as: wearable inertial sensors/IMU, console/kinect, gait analysis, tapping device, tablet/mobile, and computer.
Results:
We found several parameters, such as speed and stride length, that appear promising for detecting abnormal motor function in MCI or dementia. In addition, some studies have found correlations between these motor aspects and cognitive state.
Conclusions:
Clinical application of technological tools to assess motor function in people with cognitive impairments of a neurodegenerative nature, such as AD, may improve early detection and stratification of patients.
Keywords
INTRODUCTION
Dementia is a progressive, irreversible syndrome characterized by cognitive decline in domains such as learning, memory, executive functions, language, attention, and perception together with functional impairment in daily activities. 1 According to the World Health Organization (WHO), more than 55 million people worldwide live with dementia, and 10 million new cases are reported each year. 2 Alzheimer’s disease (AD) is the more prevalent among the neurodegenerative disorder associated with dementia. To date the clinical course of AD is well characterized and its dementia phase is thought both to represent the final stage of a long-term condition and to be preceded by the well described mild cognitive impairment (MCI). Interestingly, motor signs have been increasingly described in subjects with MCI both as proxy markers of cognitive decline and as possible subtle signs of neurodegeneration (i.e., the mild motor impairment construct). Indeed, in recent years, researchers have pointed out the importance of individualized assessment and measurement tools that can capture both cognitive and motor aspects. 3 They also have outlined that in dementia and in preclinical or prodromal stages of neurocognitive disorders the motor aspects may also be involved early on in the disease course.4,5, 4,5
Motor changes (e.g., in balance, gait or hand movements) could thus be used as early, culture- and education-independent, and non-invasive markers of cognitive decline.6,7, 6,7 Indeed, to date there are several devices that can quantify motor parameters and detect impairments in an easy way both for patients and clinicians.8–10 Intensifying research in this area could help physicians to thoroughly investigate the clinical status of the patient in the early stages of the disease in order to treat the symptoms as early as possible. Nevertheless, to date the tools available to clinicians are limited and generally do not include integrated observation of cognitive and sensorimotor aspects.
Various machine learning approaches are increasingly being applied in the diagnosis and progression of dementia, mostly in conjunction with neuroimaging data, including amyloid positron emission tomography (PET) imaging, magnetic resonance (MR) imaging, and combined PET and MR imaging.11,12, 11,12 However, the detection of early motor changes could be relevant for in depth investigation of the motor cognitive functions of patients. Indeed, in the last decades we have seen technological advances, which allowed us to push the boundaries of healthcare further. 13
Herein, we review various approaches in which technology is currently used in the assessment of motor aspects and their relationship with cognitive state in patients with MCI or dementia, with a focus on the AD spectrum. Our aims are to explore the potential benefits of technology in clinical assessment and diagnostic process, alongside providing an overview of the existing literature on motor state changes in the specified populations.
MATERIALS AND METHODS
This review has been conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations.14–16 Based on the PICOS model, the “Participants” were patients with cognitive impairment of a neurodegenerative nature, such as AD; the “Intervention” was the use of technological tools among assessment methods, the “Comparator” was any conventional motor and cognitive evaluation method (e.g., paper and pencil neuropsychological tests); the “Outcome” was all measures related to cognitive state, gait and balance, physical functioning, disability, or Activities of Daily Living, and the “Study design” was controlled and open studies.
Selection criteria
Inclusion criteria were: 1) the presence of assessment through the use of technological tools as a typology of evaluation; 2) participants with cognitive impairment; 3) the application of conventional tests (e.g., paper and pencil neuropsychological tests); 4) all publication dates with no restrictions; 5) both controlled and open studies with case series were included.
Exclusion criteria were: 1) studies in which assessment does not concern motor aspects; 2) studies that monitored patients, rather than performing a single assessment, were excluded (e.g., tele monitoring, video monitoring, GPS etc.); 3) studies not written in English; 4) reviews, commentaries, abstracts, conference papers, studies on animal models or healthy subjects were excluded; 5) studies with pharmacologic goals; 6) patients with MCI/dementia caused by non-degenerative diseases, e.g., vascular diseases; 7) another cause with other neurodegenerative diseases such as Parkinson’s disease.
Study selection and data extraction
The outcomes of interest were related to motor function of upper and lower limbs, gait and balance, physical functioning, Activities of Daily Living with respect to cognitive function.
The PubMed, Web of Science, Scopus and Cochrane databases were searched on May 2023 for peer-reviewed with the following search string:
((Alzheimer’s* disease OR AD OR neurodegenerative disease OR Cognitive impairment OR Cognitive disorder OR Neurocognitive Disorders OR mild cognitive impairment OR MCI) AND ((motor function* OR Activities of Daily Living OR upper limb motor function OR posture OR balance OR lower limb motor function OR gait speed) AND (cognitive function OR cognitive impairment OR Cognitive disorder)) AND (wearable sensor* OR device OR sensor OR sensors OR inertial measurement OR Monitoring OR instrumentation* OR Wireless Technology* OR Wearable inertial sensors OR IMU OR accelerometer OR gyroscope OR magnetometer) AND (technology assessment OR sensors evaluation OR evaluation device)).
Search results were uploaded to Rayyan software, a web-based app to facilitate collaborations among reviewers during the selection of the studies. 17 Two authors (MH, SC) independently screened titles and abstracts. The reference lists of relevant papers were manually checked to identify additional studies potentially missed in the database search. Any disagreement was solved by consensus by a third reviewer (MP).
Authors independently extracted the following data from the included papers: study design, type of device, sample size, gender/age of patients, primary and secondary outcome measures, results.
Data collection and level of evidence
Variables of interest collected in this review included Author, Year, Type of study, Population, Device name, Intervention, Outcome Measures with device, Outcome Measures with the evaluation scale, Results, Level of evidence and grade of recommendation. The level of evidence of the studies was assigned according to the Oxford Centre for Evidence-Based Medicine framework (http://www.cebm.net/index.aspx?o=1025).
Quality assessment
The quality of evidence for each study was generally low as it was not possible to examine only prospective randomized controlled trials due to the heterogeneity of the devices and /or instruments under development, the small number of study participants, and the inadequate reporting of study details.
RESULTS
Selection of the studies
A total of 716 records were identified by means of literature search. After duplicates removal, 665 papers were screened through title and abstract and 128 papers were obtained for full-text screening that were independently reviewed and evaluated by two authors (MH, SC). Disagreement concerned 6 papers over the 128 selected for full-text examination (inter-rater agreement: 95.31% ) and was solved by consulting a third reviewer (MP). 21 articles fulfilled the inclusion criteria and were therefore included in the review (Fig. 1). The selected papers were grouped according to the investigated domain (i.e., gait and balance or upper limb performance) and type of evaluation device (i.e., wearable inertial sensors, tapping devices, tablet etc.).
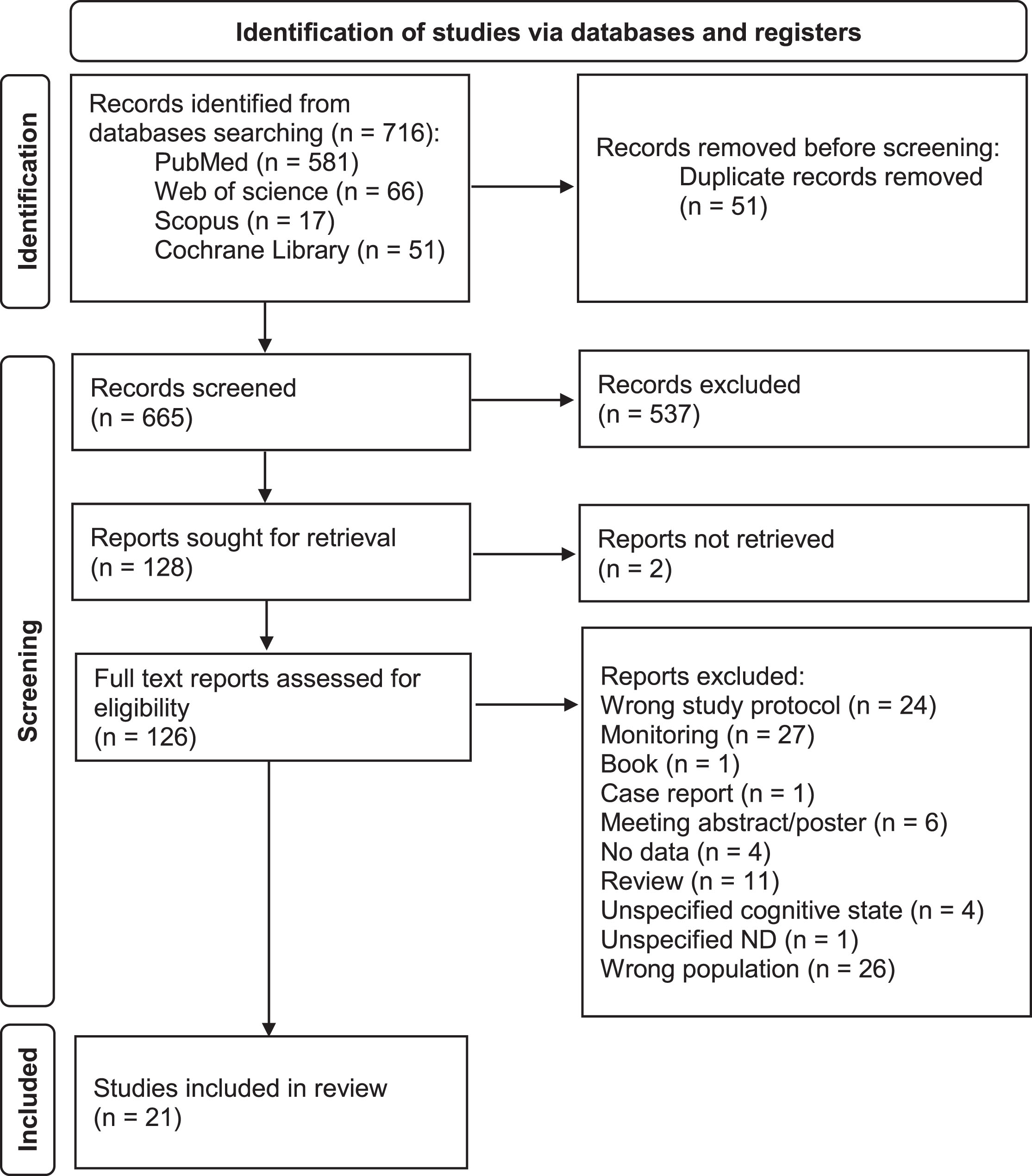
PRISMA diagram of the study (Page et al., 2021; www.prisma-statement.org).
Evaluation studies
Twenty one studies were aimed at the assessment of motor function in patients with cognitive deficits in different severity stages, with a focus on the AD spectrum (Table 1). If a paper also included other neurodegenerative diseases, it was included but we only considered participants who met the above-mentioned inclusion criteria for this review.
Description of the studies included in the review
ABC, Activity Balance Confidence Scale; ACE-III, Addenbrookes Cognitive Examination III; ACE-R, Addenbrookes Cognitive Examination Revised; AD, Alzheimer’s Disease; ADL, Activity of Daily Living; ADLQ, Activity of Daily Living Questionnaire; AD-MCI, MCI/Alzheimer’s disease; aMCI, amnestic Mild Cognitive Impairment; AVLT, Auditory Verbal Learning Test; BADLS, Bristol Activities of Daily Living Scale; BBS, Berg Balance Scale; BDI-II, Beck’s Depression Inventory II; BNT, Boston Naming Test; CASI, Cognitive Assessment Screening Instrument; CDR, Clinical Dementia Rating Scale; CDR-SB, Clinical Dementia Rating Scale – sum of boxes CDT, Clock Drawing Test; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; CES-D, Center for Epidemiologic Studies-Depression; CF, cognitive frailty group; CI, cognitively impaired; CIRS-G, Cumulative illness rating scale - Geriatrics; DLB, Dementia with Lewy bodies; DLQ, Daily Living Questionnaire; DRS, Dementia Rating Scale; DRS-II, Dementia Rating Scale 2; EQ-5D 5L, EuroQol – 5D 5 level; F, female; FAB, Frontal Assessment Battery; FCSRT, Free and Cued Selective Reminding Test; FES-I, Falls Efficacy Scale-International; FTBT, Follow-the-Ball Task; GDS, Geriatric Depression Scale; GDS-15, Geriatric Depression Scale 15-Item; HC, healthy control group; IADL, Instrumental Activity of Daily Living; IMU, inertial measurement unit; iTMT, instrumented trail-making task; M, male; MCI, Mild Cognitive Impairment; MMSE, Mini-Mental State Examination; MNA, Mini Nutritional Assessment; MND, Mild Neurocognitive Disorder; MoCA, Montreal Cognitive Assessment; N, number; N.S., not specified; NART, National Adult Reading Test; NCF, non-cognitive frailty group; ND, Neurodegenerative Disease; NPI, Neuropsychiatric Inventory; PC, Personal computer; POMA, Performance-Oriented Mobility Assessment; RCT, randomized clinical study; ROCF, Rey– Osterrieth Complex Figure; SD, standard deviation; SCWT, Stroop Color-Word Test; SDMT, Symbol Digit Modalities Test; SHERPA, Score Hospitalier d’évaluation du risque de perte d’autonomie; TAP, Test for Attentional Performance; TMT, Trail Making Test; TUG, Timed-Up and Go; VAS, Visual analogue scale; ZN-G, repeating numbers; ZVT-G, modified version of the Trail-Making-Test A.
Participants
The total number of participants is 3418 (controls = 1926) with a sample size ranging from 11 18 to 1249 19 and a median of 72 participants. The total of patients involved in the studies is 1492 (range = 11– 349) with a median of 38. Given the considerable heterogeneity in the approach to diagnostic labelling used in the reported papers, the target population was reported as MCI in 4 articles [250 patients (16.8% ), median = 14, range = 11–211], as well as AD [202 patients (13.5%), median = 34, range = 21–113], while MCI and AD were reported in 9 studies [807 patients (54.1%), median = 48, range = 18–349]. The remainder 4 reported on people with unspecified dementia [233 patients (15.6%), median = 56, range = 16–105]. The intervention was applied on 3063 subjects (median = 72, range = 11– 1249).
Outcome measures: Devices used in the studies
Wearable inertial sensors to evaluate gait and balance
Twelve studies evaluated MCI or dementia patients using wearable inertial sensors.19–30 These types of instruments utilize different inertial sensors, such as accelerometers and gyroscopes, to detect and quantify motion along the axes. In some cases, these sensors are worn by patients, for instance, at the waist or ankle level, while in other cases, they are integrated into larger devices, such as an unstable platform.
In a cross-sectional study, Bernhard et al. 20 tested the gait and balance with three sensor-units at both ankles and lower back. The study designed for unspecified dementia patients including walked, static balance with 4 positions of the feet (open, closed, semi-tandem and tandem stance), then performed on a foam pad, and found groups with gait speed and/or balance deficits showed impaired cognitive performance, supporting the association between motor performance and cognition. In another case-control study, Costa et al. 21 investigated an intervention using a combination of kinetic sensors and inertial units (trunk, legs and thighs) to assess the kinematics of postural control in seven tasks in patients with AD. After recognizing the interaction between postural stability and cognitive performance, they found that the analysis of postural kinematics has the potential to be used as a complementary biomarker in the diagnosis of AD. In a case-control study on individuals with unspecified dementia Mulas et al. 22 applied a wearable inertial sensor to the trunk of the participants during a natural 30 meters straight walk at a self-paced speed and Timed Up and Go (TUG) test. Gait parameters such as speed, stride length, cadence and duration of stance, swing and double support phase and walk ratio were obtained from the natural walk and 5 other parameters came from Timed Up and Go (duration, sit-to stand, intermediate 180° turn, final 180° turn, stand-to-sit). They found that aspects of mobility were significantly impaired in the presence of a cognitive deficit in comparison to healthy controls. Gait speed, stride length and Timed Up and Go duration are correlated with the extent of cognitive impairment. Buchman et al. 19 performed a longitudinal cohort study to explore the mobility of MCI and AD subjects with a wearable sensor positioned on the lower back with a neoprene belt. They extracted 26 parameters from 32 ft walk, Timed Up and Go and standing with eyes closed (one of which with 3 subtasks) and found that 10 out of 12 gait scores (specified in Table 1) were associated with incident mortality, ADL disability, motor disability, incident MCI or incident AD. The study findings suggest that modelling combinations of different mobility measurements are differentially associated with specific health outcomes. Hsu et al. 23 conducted a case-control study in patients with AD to investigate the use of foot-mounted sensors in a 40-meter walk test, which consisted of a single and dual task, and a balance test with waist-mounted sensors. The gait and balance measurement device consisted of a triaxial accelerometer, a uniaxial and biaxial gyroscope, a microcontroller and a micro-SD flash memory card. It considered 16 parameters from the gait test and 16 parameters from the balance test. The device is a convenient tool for automatically analyzing gait and balance information. In AD patients, the results showed a statistically significant difference with the healthy control group in gait parameters both in and between single-task and dual-task and a significantly higher average sway speed in the balance tests. In a case-control study, Gillain et al. 24 tested the efficacy of the tri-axial accelerometer to evaluate body movements in all three spatial planes (the gait performance with the pull test, the single-leg balance test, the Timed Up and Go test and a 30-meter stable gait test) in MCI, AD and Healthy Control. They showed the clinical motor tests were not able to significantly differentiate between groups, while the device demonstrated significantly lower gait speed and stride length regularity in AD patients. Furthermore, the MCI patients had a lower stride frequency in comparison to Healthy Control. Gait speed and stride frequency positively correlated with the patient’s global cognitive level. Zhou et al. 25 reported a case-control study that explored the effect of five wearable sensors attached to the lower back, left and right thighs and lower shins to quantify speed, stride length, cycle time and double support during gait task in patients with amnestic MCI and mild dementia and found gait parameters are potential digital biomarkers of cognitive impairment. Huang et al. 26 conducted a cross-sectional study in an amnestic MCI and mild AD sample to explore 30 s free walking test wearing inertial sensors to measure stride speed, cadence and heel strike angles. They found a significant association between memory deficit and increased fall risk and this latter aspect might represent an objective marker for the monitoring of memory and fall risk itself. Kuan et al. 27 assessed posturography, through the use of the stability system, and quantified gait performances wearing a device with inertial sensors on healthy controls, amnestic MCI and mild dementia due to AD patients. Indices of sensory integration were significantly worse in mild dementia than in MCI and Healthy Control. Clinical motor (Berg Balance Scale) and fall risk tests significantly differed between MCI and mild dementia in comparison to healthy controls. Moreover, results showed significantly lower different speed scores in MCI and lower stride length in mild dementia groups in comparison to healthy controls. Mishra et al. 28 evaluated the association of instrumented Trail-Making Task (iTMT), an interactive game-based software, to calculate instrumented Trail-Making Task time in patients with MCI. They found the device is able to distinguish individuals with MCI from Healthy Control older adults. Furthermore, they found correlations between instrumented Trail-Making Task, Montreal Cognitive Assessment (MoCA) score and gait speed. Wiloth and colleagues 29 validated a game-based assessment of balance-cognitive abilities, using a moveable plate connected to a computer and monitor, in people with unspecified mild-to-moderate dementia. They applied three tasks: Physiomat Trail Making Tasks (PTMT), an instrumental Trail Making Tasks; Follow The Ball Test (FTBT), in which participants had to follow a moving ball on the screen using balance; Physiomat Balance Tasks (PBT), in which participants had to remain as still as possible. The results of this cohort study showed a correlation between the time taken to complete Physiomat Trail Making Tasks and cognitive and motor tests. In a case-control study by Mc Ardle et al. 30 several aspects of gait were assessed using a sensor placed on the lower back of healthy participants and patients with AD performing a ten-meter walk at comfortable pace in the lab. AD patients were more variable for step, stance and swing time, spent longer in swing time and had greater swing time asymmetry in comparison to controls.
Considering these 12 studies on the use of wearable inertial sensors or Inertial Measurement Unit (IMU) for gait and balance, seven studies reported that slower gait speed was associated with poorer global cognition.20,22–27, 20,22–27 Six studies showed that another important parameter is stride, especially stride length, which is lower in patients compared to healthy controls.19,22–25,27, 19,22–25,27 Three studies found differences in the swing aspects of gait in patients compared to controls: Mulas reported a decrease in swing phase duration, Hsu showed a decrease in swing period percentage and McArdle highlighted an increase in swing time, swing time asymmetry and standard deviation.22,23,30, 22,23,30 Finally, two studies reported a decrease in cadence in patients compared to controls.19,22, 19,22
In four studies, dual task paradigm - motor and cognitive - enhanced differences between the groups.18,23–25, 18,23–25 Globally, gait and balance performances are reported as worse in patients in comparison to healthy controls and emerges an association between motor abilities and cognition.
Gaming consoles and kinect to evaluate gait and balance
Gaming consoles are already being used in physiotherapy rehabilitation and have spawned a whole new area— exergames— that allows people to carry out rehabilitation programs in a stimulating and interactive way. 31 In addition to this approach, this field also has the potential to measure movement for purposes other than rehabilitation. We report a cross-sectional study with people suffering from AD. Yang et al. 32 used the Kinect Depth Sensor System, which is part of the Microsoft Xbox console ecosystem, to measure a total of thirty angles formed by the limbs from fifteen different body joints with the centerline. This was done without the participants having to perform any task: they simply had to stand still and look straight ahead for forty seconds. In conclusion, authors found that changes in coordination function in limbs can reflect the clinical outcomes, cognition and global function.
Gait cycle formal analysis
Another aspect assessed through the use of technology is the patient’s gait cycle, which is composed of the stance phase and the swing phase, both of which are subdivided into several other phases. Of the twenty-one papers included in this review, one addressed this topic.
Montero-Odasso and colleagues 18 analyzed gait parameters in a cohort study of MCI patients walking on an engineered mat (GAITrite) during single and dual cognitive tasks. They found that the dual task, which involved counting backwards from 100, played a role in the patients’ gait performance, leading to an increase of step and stride time compared to the single task.
Finger tapping devices to assess upper limb function
Four studies used finger tapping to study motor performances of AD or MCI patients. These finger tapping sensors devices are typically placed on the fingers and are capable of detecting and measuring the intensity, frequency, duration, and pattern of taps produced by the individual. They can be used in research settings or clinical assessments to objectively measure hand performance, compare motor parameters and detect any subtle changes in motor function.
In a case-control study in MCI, AD and Healthy Control Suzumura et al. 33 applied a finger tapping device (UB-1) and found a decrease in patients’ performances in total travelling distance, dispersion of the contact duration and rhythm perturbation compared to Healthy Control. Moreover, they found a positive correlation between Mini-Mental State Examination (MMSE) and total travelling distance and a negative correlation between MMSE and dispersion of the contact duration, rhythm perturbation, balance between flexing movement and extending movement and dispersion of inter-hand gaps. Thus, finger dexterity is associated with decline in cognitive function evaluated with MMSE and its assessment can be used as an indicator of cognitive function. Suzumura and colleagues 34 requested to wear a device with magnetic sensors (UB-2) on their thumbs and index fingers of both hands and to perform finger tapping movements in four different scenarios. They collected 36 different parameters from the instrument, along with MMSE and Barthel Index scores. Results showed significant associations between the standard deviation (SD) of distance rate of velocity peak in extending movement and the SD of contact duration and cognitive function. In a case-control study, Suzumura et al. 35 used the same finger tapping device of the previous study 34 to measure 44 parameters, such as distance, velocity, acceleration, energy, number of freezing, contact duration, tapping interval, inter-tapping interval, similarity of hands, frequency and number of taps, in patients with MCI and Healthy Control. They reported a significant decrease in the number of taps and an increase in the average of tapping interval, inter-tapping interval and number of freezing in patients. Roalf et al. 4 applied a finger and foot tapping test in a case-control study on AD and MCI and found a decrease in the number of finger taps and an increase of inter tapping interval in AD and MCI in comparison to Healthy Control, with a unique pattern of dysfunction for each disorder, and these two parameters were associated with MMSE.
Globally, the most evaluated parameters are: inter tapping interval,4,35, 4,35 number of taps,4,35, 4,35 and contact duration.33,34, 33,34
Touchscreen-based tools to assess upper limb function
Given their widespread diffusion and the increasing ease of use facilitated by touchscreen, voice commands and artificial intelligence, tablets, smartphones and Personal Computers serve as valuable tools for assessing motor or cognitive performances in general. In this review, we found two papers using this type of device.
Holmes and colleagues 36 involved people with MCI, MCI/AD and AD in two tasks among two paradigms: copying an excerpt and describing a picture with the mechanical keyboard of a laptop; transcribing a different passage and answering three questions with the touch keyboard of a smartphone. Using machine learning models, they found a significant correlation between users’ patterns of typing on devices and their verbal memory, non-verbal memory, executive functions and language Furthermore, their method was able to produce quantitative measures of both global cognition and its relative subdomains directly from the analysis of the mentioned tasks.
Secondly, Yan et al. 37 conducted a case-control study in order to quantify, using technological devices, fine motor control of people with a diagnosis of MCI or probable AD. Specifically, participants were instructed to move between two dots as fast as possible using a stylus pen on a digitizer in two or four stroke conditions. The healthy controls group resulted to be faster, smoother and steadier than MCI group, which, in turn, performed better in each of these aspects than AD group.
As the instruments used in the two studies are very different, the results are not comparable. Nonetheless, speed is an important element in Yan et al. 37 , in line with other studies mentioned above dealing with different instruments, such as in the previous chapters “Wearable devices/IMU” and “Tapping device”. Furthermore, these two studies show that it is possible to distinguish cognitively impaired people and healthy controls by analyzing simple tasks performed with the hands, such as typing on a keyboard or using a pen on a tablet.
Wearable inertial sensors to assess upper limb function
Rovini et al. 38 performed an analysis of a case-control study in dysexecutive mild neurocognitive disorder (MND) patients to measure kinematic parameters with one ring-shaped sensor in the proximal phalanx of the dominant index finger. They found that cognitively impaired subjects exhibited slower movement, slower reaction and longer deceleration and had more difficulties in the modulation of the kinematics of their movements in comparison to Healthy Control. The device is small and might have the potential to be used for clinical application or for remote monitoring at home.
Outcome measures: Clinical scales used in the selected studies
We observed a significant heterogeneity in the scales used to assess the clinical correlates of the motor impairment observed in the selected studies. Table 2 facilitates a comparison of cognitive, psychological and functional abilities (Activities of Daily Living, or ADL) assessment tools used in the selected articles. As indicated in the Table 2, assessment tools may evaluate different stages of disease severity, domains or aspects of a particular domain. In some studies, multiple clinical tests were used and functional information from motor scales was included to provide a better understanding of the patient. Regarding the assessment of motor ability, studies generally used scales concerning stability and/or the fall risk. Some studies used scale to assess body composition or strength and physical impairment (Table 3).
Cognitive and psychological instruments applied in the studies included in the review
ACE-III, Addenbrookes Cognitive Examination III; ACE-R, Addenbrookes Cognitive Examination Revised; AVLT, Auditory Verbal Learning Test; BDI-II, Beck’s Depression Inventory II; BNT, Boston Naming Test; CASI, Cognitive Assessment Screening Instrument; CDR, Clinical Dementia Rating Scale; CDT, Clock Drawing Test; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; CES-D, Center for Epidemiologic Studies-Depression; CTP, Cookie Theft Picture; CVLT-SF, California Verbal Language Test-II Short Form; DRS, Dementia Rating Scale; DRS-2, Dementia Rating Scale 2; EQ-5D 5L, European Quality of Life 5 Dimensions 5 Level Version; FAB, Frontal Assessment Battery; FCSRT, Free and Cued Selective Reminding Test; GDS, Geriatric Depression Scale; IADL, Instrumental Activity of Daily Living; JLO, Judgment of Line Orientation; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; NART, National Adult Reading Test; NPI, Neuropsychiatric Inventory; PSQI, Pittsburgh Sleep Quality Index; ROCF, Rey– Osterrieth Complex Figure; SCWT, Stroop Color-Word Test; SDMT, Symbol Digit Modalities Test; SHERPA, Score Hospitalier d’évaluation du risque de perte d’autonomie; TAP, Test for Attentional Performance; TCF, Taylor Complex Figure; TMT, Trail Making Test; VAS, Visual Analogue Scale; ZN-G, repeating numbers resembling Digit span task; ZVT-G, modified version of the Trail-Making-Test A.
Motor and functional instruments applied in the studies included in the review
ABC, Activities-specific Balance Confidence; ADL, Activity of Daily Living; ADLQ, Activity of Daily Living Questionnaire; BADLS, Bristol Activities of Daily Living Scale; BBS, Berg Balance Scale; CIRS-G, Cumulative Illness Rating Scale; FES-I, Falls Efficacy Scale-International; POMA, Performance-Oriented Mobility Assessment; Tinetti; TUG, Timed Up and Go Test; VAS, Visual Analogue Scale.
DISCUSSION
We provide a review on motor function parameters evaluated with devices or sensors in dementia and/or MCI patients. We included 21 articles with heterogeneous devices, study outcomes and study design. Some studies focused on balance, gate and generally lower limbs (N = 14) and the others used the technologies in upper limbs (N = 7).
We found 13 studies on IMU sensors (12 lower limbs, 1 upper limb) and that have shown a potential efficacy in assessing motor involvement. They provide a continuous registration of motor parameters and can detect subtle changes in motor performance, including gait and balance, in a wide spectrum of settings. These devices are often lightweight and easy to use. Our finding of different protocols with a highly heterogeneous technology applied showed that challenges exist in validating and standardizing the data collected by these sensors across different populations. However, it seems that speed for lower and upper limb (N = 8) and stride for lower limb (N = 6) are two important parameters during the evaluation with wearable sensors. Further research is needed to establish the accuracy, reliability, and clinical utility of wearable sensors in assessing motor involvement in AD.
Two studies used motion systems to analyze movement patterns: in one case, authors used a sensorized mat, Gaitrite, and in the other one, they used a camera system, Kinect. The devices offer high-resolution assessment of motor function by capturing and analyzing movement patterns. While Gaitrite analysis focuses more on stride and gait velocity as the parameters to be mainly considered, like the studies with IMU sensors, Kinect focuses on movement coordination. However, motion systems are typically expensive and require specialized equipment and expertise for setup and analysis.
Six papers explored tapping sensors, tablet/smartphone or personal computer protocols, where they evaluated coordination and speed during the hand and fingers movement. The studies showed these tasks can be used for the evaluation of hand function and motor skills. Fine hand movements tests can be useful in assessing various motor aspects, such as finger dexterity, coordination, speed, and rhythm. They can provide quantitative data on the individual’s motor performance, allowing an objective evaluation. Three underlined speeds (expressed as number of taps in finger tapping paradigms) as a core parameter to take into consideration as a primary outcome.
Nonetheless, these apparently promising results should be cautiously considered, because of several potential confounders. First, target population, severity and devices differed across studies. As noted, motor symptoms in dementia patients can vary depending on the type and stage of cognitive decline. Therefore, it is important to evaluate changes in motor function in early stages, such as MCI, and possibly to stratify patients according to the different underlying neuropathology. Second, methodological differences, including type of movement, position of the sensors, registering parameters and outcome measures may hamper the findings replication. Third, the reported studies did not identify a “gold-standard” battery for a comprehensive assessment of motor function in subjects with AD and other dementing conditions. This is confirmed by the inhomogeneity of motor tests applied in the selection of studies reported in this review in Table 3. There is also a lack of agreement about a shared battery of cognitive tests to apply to explore the cognitive correlated of motor impairments even though the two major screening tests, MMSE and MoCA, are the most frequently used in the review, as reported in section “Outcome measure - Scale”. These tests cannot provide a comprehensive view of a patient’s cognition, although their main advantages are that they are universally recognized as global indicators of cognition and that they are quick and easy to administer. 39 However, regarding the rating scales, our findings are in keeping with previously published review on Outcome Measures in Dementia and MCI Trials, confirming the fact that evaluation scales in dementia/MCI trials remain inhomogeneous and diverse. 40
The evaluation of motor function with the device revealed that gait, balance,18–26,28–30,32, 18–26,28–30,32 and upper limbs movements4,27,33–37, 4,27,33–37 were associated with cognitive function, confirming a significant association between cognitive function and changes in motor abilities. Furthermore, traditional motor scales are usually not sensitive enough to detect small early changes in patients with cognitive impairment of a neurodegenerative nature, such as AD. We believe that the application of a blended assessment, consisting of traditional tests and modern evaluation methods with technological devices, might represent a better option for clinicians in order to differentiate between pathological and preserved motor function. Instruments should be valid, reliable and responsive to provide clinically important changes over time. Research efforts are necessary in order to validate existing devices and to identify the best performing ones, with the aim to identify the subtle motor disturbances that can advise the onset of the occurrence of a cognitive failure.
Limitation of the study
There was a limited possibility to perform a systematic review because of the different outcomes measured across studies and quality of the papers. Larger and more detailed device studies are needed to further explore their effectiveness given the reliable results of the limited current literature.
AUTHOR CONTRIBUTIONS
Mehrnaz Hamedani (Conceptualization; Data curation; Formal analysis; Methodology; Writing – original draft; Writing – review & editing); Stefano Caneva (Conceptualization; Data curation; Formal analysis; Methodology; Writing – original draft; Writing – review & editing); Gian Luigi Mancardi (Methodology; Writing – review & editing); Paolo Alessandro Alì (Writing – review & editing); Pietro Fiaschi (Methodology; Writing – review & editing); Federico Massa (Writing – review & editing); Angelo Schenone (Funding acquisition; Methodology; Writing – review & editing); Matteo Pardini (Conceptualization; Funding acquisition; Methodology; Supervision; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
AS gratefully acknowledges the support of the project “RAISE - Robotics and AI for Socioeconomic Empowerment” funded by the European Union - NextGenerationEU. MH and FM acknowledge the support of #NEXTGENERATIONEU (NGEU), funded by the Ministry of University and Research (MUR), National Recovery and Resilience Plan (NRRP), project MNESYS (PE0000006) – A Multiscale integrated approach to the study of the nervous system in health and disease (DN. 1553 11.10.2022). MP thanks the Italian Ministry of Health for funding the project “Dalla neurologia quantitativa alla tele-neurologia: quali strumenti per l’assessment computerizzato della disabilità motoria?”. 5×1000 2018-2019. We also thank the Department of Neurosciences, Rehabilitation, Ophthalmology, Genetic and Maternal Infantile Sciences (DINOGMI), for the valuable collaboration on this article.
The views and opinions expressed are those of the authors alone and do not necessarily reflect those of the European Union or the European Commission. Neither the European Union nor the European Commission can be held responsible for them.
FUNDING
This study was supported by grants from the Italian Ministry of Health, 5×1000 and European Union – NextGenerationEU.
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.
DATA AVAILABILITY
The data supporting the results of this study are openly available online.