
Abstract
Background:
The significant increase in Alzheimer’s disease and related dementia prevalence is a global health crisis, acutely impacting low- and lower-middle and upper-middle-income countries (LLMICs/UMICs).
Objective:
The objective of this study is to identify key barriers and gaps in dementia care and research in LLMICs and UMICs.
Methods:
We conducted an international, cross-sectional survey among clinicians and healthcare professionals (n = 249 in 34 countries) across LLMICs and UMICs, exploring patient demographics, use of clinical diagnosis, dementia evaluation, screening/evaluation tools, and care and treatment.
Results:
Significant disparities were found in diagnostic practices, access to assessments, and access to care. On average, clinicians in LLMICs saw more patients, had less time for evaluations, lower use of formal screening and tools, and less access to biomarkers. They were also under-resourced compared to UMICs.
Conclusions:
The findings provide insights for policymakers, healthcare organizations, and researchers to address the complex challenges associated with dementia care in diverse settings. Addressing these challenges requires a multipronged approach involving local, national, and international stakeholders.
INTRODUCTION
Alzheimer’s disease and related dementias (ADRD) will affect 152 million individuals by 2050, 1 primarily due to increasing life expectancy. Nearly two-thirds of ADRD cases will be in low- and middle-income countries (LMICs) in the next three decades. Most LMICs are largely unprepared for the projected dementia prevalence, where the multidimensional impact will increase disability and dependency for older adults, the financial and emotional burden for caregivers, and community tensions associated with ADRD stigma. 2 Socioeconomic vulnerabilities, including low educational attainment, limited healthcare infrastructure, and geopolitical factors, are several putative barriers that pose unique complexities in the assessment and treatment of dementia in an aging global population in LMICs. 3
Socioeconomic vulnerabilities are often rooted in historical and documented periods of colonialism, relationships with foreign institutions and industries, conflict, natural disasters, or structural adjustment programs.4,5, 4,5 LMICs with limited budgets and resources face a dilemma in prioritizing healthcare spending. With the growing demand for acute medical services and infrastructure development, chronic neurodegenerative conditions like dementia often receive lesser attention. Economic constraints affect not only the availability of resources for care but also the development of skilled healthcare professionals specialized in dementia. In a similar vein, the healthcare infrastructure in many LMICs will face larger challenges to be effectively prepared to handle the complexities of screening, assessment, treatment, and long-term care associated with ADRD than in high-income countries (HIC). 6 Chief among these challenges is a stark shortage of neurologists, neuropsychologists, geriatricians, gerontologists, and mental health professionals trained in diagnosing and managing dementia. 7 Conventional diagnostic tools such as neuroimaging and biomarkers (biofluids [cerebrospinal fluid, plasma] and neuroimaging) are scarce and expensive and, if available, are concentrated in large urban environments. 8 Additionally, geopolitical factors (e.g., conflict, climate change, social inequity, internal displacement) significantly influence healthcare priorities and funding in LMICs, where some countries have a web of international politics and economic dependencies that shape their healthcare agendas.5,9, 5,9 For instance, foreign aid and international health initiatives have primarily focused on communicable and infectious diseases like HIV/AIDS and tuberculosis, overshadowing non-communicable chronic disorders such as dementia.10 - 12 This results in a disproportionate allocation of resources, leaving dementia research, clinical trials, and care underfunded and under-researched.12 - 16
Given the heterogeneity, diversity, and intersectionality of the aforementioned factors, a multimodal approach is required for LMICs. 17 Models, assessments, and methodologies from HICs are not generalizable or easily adaptable for LMICs. 18 Diverse languages and dialects, distinct ethnic backgrounds, and varying literacy levels hinder efforts to raise awareness and educate communities about dementia. 19 Consequently, developing effective, culturally sensitive educational programs that resonate with diverse populations is a significant challenge. The cultural perception of dementia in LMICs adds another layer of complexity. In many of these societies, symptoms of dementia are often attributed to normal aging or even supernatural causes, leading to stigmatization and social isolation. 20 This perception impedes timely medical intervention and reduces the quality of life for patients and caregivers, often leading to underdiagnosis or misdiagnosis, delaying critical care and support.
LMICs face the daunting task of revamping their healthcare systems, addressing cultural stigmas, and reallocating resources to meet the growing needs for equitable dementia care. This requires not only local and national efforts but also international support and collaboration; however, the onus is often shouldered by providers. This study’s primary objective was to identify gaps and barriers in dementia care, support, research, and resources in LMICs to inform targeted strategies to address obstacles encountered across similar contexts. This study was led by the LMIC Workgroup, part of the Diversity and Disparities Professional Interest Area (PIA) of the Alzheimer’s Association International Society to Advance Alzheimer’s Research and Treatment (ISTAART).
METHODS
Study population and design
Participants were eligible to participate if they were clinicians, healthcare professionals, and/or clinical researchers working in LMICs who predominantly saw or provided treatment to adults with cognitive impairment or dementia, irrespective of any specific etiology. The LMIC Workgroup developed a survey that employed a cross-sectional design. To accommodate a culturally and linguistically diverse respondent pool, the original English questionnaire was forward-translated into French, Mandarin Chinese, Portuguese, and Spanish and then back-translated to ensure clarity and parallel interpretation. Data collection occurred between January to September 2023. The link to the survey was disseminated online to targeted countries through the LMIC Workgroup networks and the Alzheimer’s Association ISTAART PIAs. This study was approved by the Human Research Protection Office at Washington University (202204115); all participants consented to data use prior to participation.
Questionnaire
The survey consisted of 38 questions. The first set of 12 questions probed about participants’ demographic information, including age, nationality, location of work, type of institution, professional background, years of working activities, and training background. The remaining 24 questions focused on clinical practice, including the average number of patients seen every month, patients’ demographics, dementia etiologies encountered, utilization of clinical guidelines and tools (e.g., cognitive, functional, and behavioral screening tools), utilization of assessments and tests (e.g., neuropsychological, language and functional assessments, structural neuroimaging exams, imaging biomarker analysis, genetic testing for ADRD), pharmacological treatments, and available education or activities for caregivers. Finally, two open-ended questions inquired about the main challenges respondents face in clinical or research work, as well as identifying resources or support considered beneficial to clinical or research activities by the respondents. The link to the survey was disseminated online, via email and social media, to targeted countries through LMIC Workgroup networks and ISTAART. Data were collected using REDCap, a secure platform for creating and curating online databases and surveys.
Statistical analysis
Survey responder’s primary country of practice were categorized based on World Bank group classification. 21 There were 297 total respondents; 48 were excluded due to employment in HICs, resulting in the inclusion of 249 participants in the final dataset. We employ the classification group to derive three income categories: low-income countries (seven participants), lower-middle-income countries (96 participants), and upper-middle-income countries (146 participants). Initially, we compared the low-income countries group to the middle-income countries group. However, due to the small sample size in the low-income countries group, we elected to combine low-income with the low- and lower-middle-income countries group (LLMICs) to ensure a balanced sample size for comparing various factors. For questions that involved multiple-choice and checkbox responses, we combined all responses from different language versions with the English version as the reference based on the labels. Responses to questions with comments and the final two open-ended questions in non-English languages were translated into English. Based on the question about the use of dementia guidelines, we compiled a comprehensive list of guidelines mentioned by respondents. Then, we categorized them into four groups: established guidelines, laboratory or biomarker guidelines, screening, clinical evaluation, neuropsychological guidelines, and unspecified guidelines. Responses were initially coded based on keywords for the last two open-ended questions and grouped according to different thematic categories. Independent t-test was used to compare continuous variables and Chi-square test for categorical variables to identify statistically significant differences (p < 0.05) between the study groups. Statistical tests were two-sided, and data were analyzed using R version 4.2.3.
RESULTS
Participant characteristics
In the LLMICs group, there were 103 participants working in 14 countries, while the upper-middle-income countries (UMICs) included 146 participants working in 20 countries (Table 1; Supplementary Figure 1). Among respondents employed in LLMICs, the majority were male (64.1%), between 18 and 44 years of age (58.3%) and originated from Asia (49.5%). In contrast, among respondents who worked in UMICs, most were female (57.5%), between 18 and 44 years of age (50.7%) and originated from South America (68.5%). Notably, the two groups had similarities in professional backgrounds and working settings. In both LLMICs and UMICs, a higher proportion of participants worked in urban areas (81.6% and 93.2%, respectively, p = 0.007), were employed in public facilities (54.4% and 56.2%, respectively, p = 0.391), held professional positions in medicine (MD) (62.1% and 84.2%, respectively, p < 0.001), and conducted clinical and research work (63.1% and 76.0%, respectively, p < 0.001). Participants who worked in UMICs had more years of work experience and held PhD degrees compared to those in LLMICs (41.8% in UMICs compared to 13.6% in LLMICs). In terms of years of experience working, there were statistically significant differences noted between participants in 0–10 years (40.8% in LLMICs versus 29.5% in UMICs) and 21–40 years (19.4% in LLMICs versus 33.6% in UMICs) while there were no differences in 11–20 (35.0% versus 33.6%, respectively) or 40 + (1.0% versus 0.7%, respectively). In LLMICs, 13.6% of survey respondents held PhDs, compared to 41.8% in UMICs.
Participant characteristics
Patient characteristics
The mean number of patients seen by a respondent monthly in LLMICs was 240 compared to 105 in UMICs. In LLMICs, most of the patients were from suburban or peri-urban areas (48.5%), while in UMICs, the majority were from urban areas (69.9%) (Table 2).
Patients’ characteristics
Clinical diagnoses
The average monthly number of cases varied across subjective cognitive decline (SCD [14.3; 13.1]), mild cognitive impairment (MCI [14.3, 21.4]), general dementia (12.8, 25.7), dementia of the Alzheimer’s type (DAT [1.67; 1.77]) and unspecified dementia (2.53; 2.78) in LLMICs and UMICs, respectively. Notably, there were statistically significant differences in the number of dementia and MCI cases per month between the two groups (p < 0.001 and p = 0.02, respectively). However, no statistically significant difference was observed in the number of monthly SCD cases, DAT cases, and general dementia cases (p = 0.66, p = 0.72, p = 0.83, respectively). Respondents from both LLMICs and UMICs indicated that they had seen cases of SCD, MCI, dementia, and DAT within one month, with fewer reporting cases of unspecified dementia. Participants from both LLMICs (52.4%) and UMICs (82.2%) endorsed using a specific guideline or criteria for diagnosing dementia. However, in LLMICs, approximately 45% indicated using no particular guidance for ascertaining a diagnosis, which was significantly higher (p < 0.001) compared to 15% UMICs respondents. A larger number of respondents in UMICs (58.9%) reported use of established guidelines compared to those in LLMICs (42.7%) (p < 0.001) (Fig. 1). The top two guidelines used in LLMICs were DSM and ICD-10, while the DSM, NIA-AA, and unspecified tools or guidelines were used in UMICs. Significant differences were observed in the use of ICD-10, NIA-AA, and unspecified tools or guidelines (p < 0.001, p = 0.02, p = 0.03,respectively).

The number of reported uses of specified guidelines.
Dementia evaluation
Most participants in both LLMICs and UMICs affirmed using cognitive screening tools. Significant differences were observed in evaluation time and the use of cognitive screening tools between groups. The mean evaluation time in the LLMICs was 36.9 min, compared to 53.5 min in the UMICs group (p = 0.005). Compared to LLMICs, UMICs respondents endorsed greater use of screening tools such as MMSE or MoCA (79.6% versus 94.5%; p < 0.001). The MMSE, MoCA, and ACE-R or ACE-III were the most frequently used tools in both groups (Fig. 2), while tools such as MIS and GPCog were less commonly used. CERAD, RUDAS, and Brief Cognitive Screening Battery were frequently used in UMICs but were seldom used in LLMICs. Significant differences existed in the use of MMSE (p = 0.04), MoCA (p = 0.01), CERAD (p < .001), RUDAS (p = 0.04), and Brief Cognitive Screening Battery (p < 0.001) between the two groups.

The number of reported uses of screening tools.
A higher percentage of respondents in UMICs used informant-based or functional screening tools, compared to LLMICs used such tools (80.8% versus 40.8%; p < 0.001). Although CDR was the most frequently used functional screening tool in LLMICs, only 25.2% reported using it, compared to 58.9% in UMICs. Additionally, a higher percentage of participants in UMICs used the AD8, DAD, IQCODE, and Amsterdam IADL Questionnaire compared to the LLMICs group (Fig. 3). Differences were observed in the use of the CDR and IQCODE (p < 0.001, p = 0.01). Similar patterns were observed in the use of behavioral assessment tools. Most respondents in UMICs endorsed using at least one type of behavioral assessment tool, compared to those in LLMICs (71.2% versus 37.9%; p < 0.001). Behavioral assessment tools like the Geriatric Depression Scale (29.1% versus 56.2% [p < 0.001]) and Neuropsychiatric Inventory Questionnaire (28.2% versus 47.9% [p = 0.001]) were commonly used but were underutilized in LLMICs compared to UMICs. Additional tools like the Cornell Depression Scale were used but more infrequently across respondents in UMICs (15.1%) and LLMICs (6.8%) (Fig. 4).
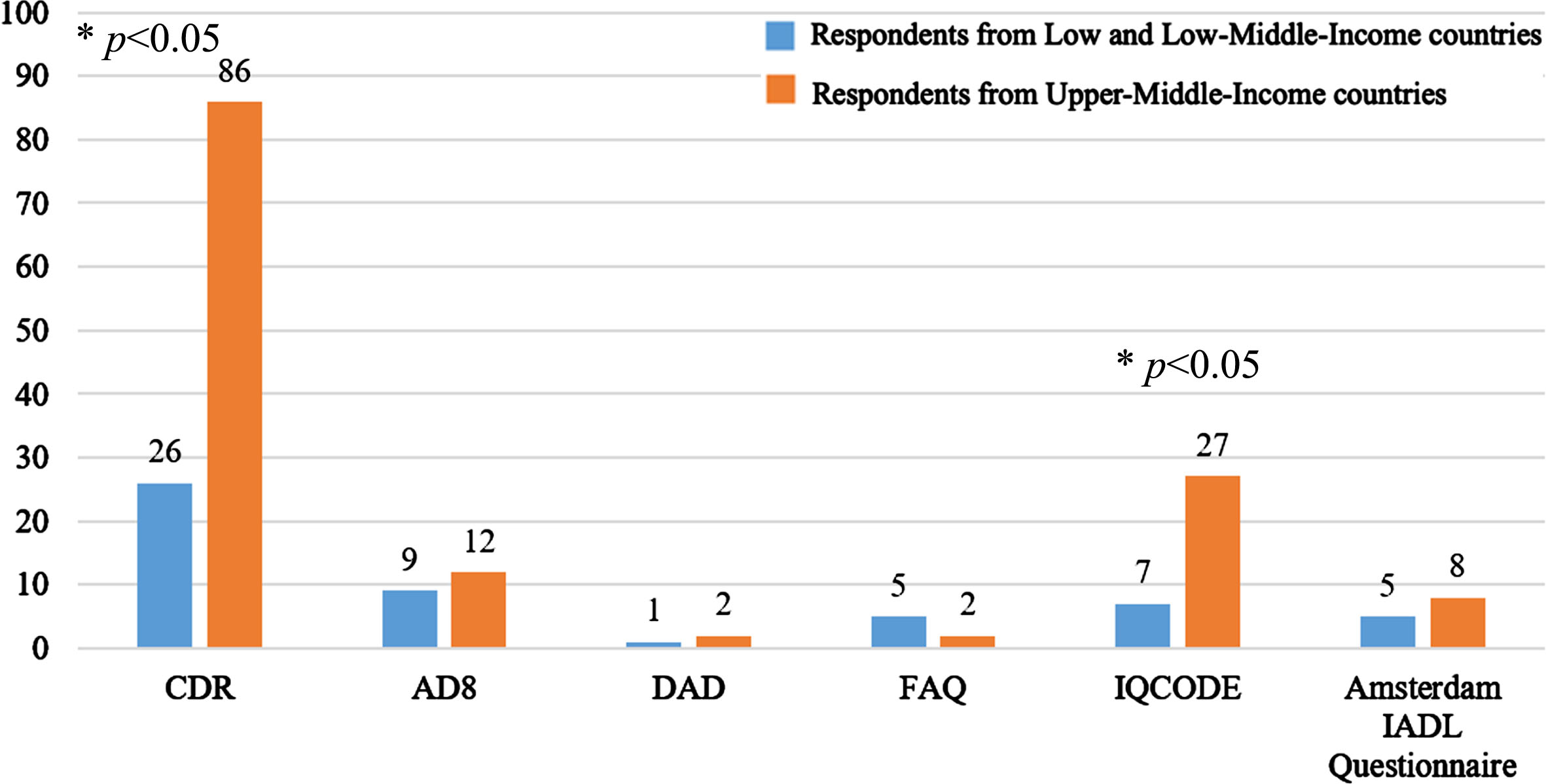
The number of reported uses of informant-based or functional screening tools.
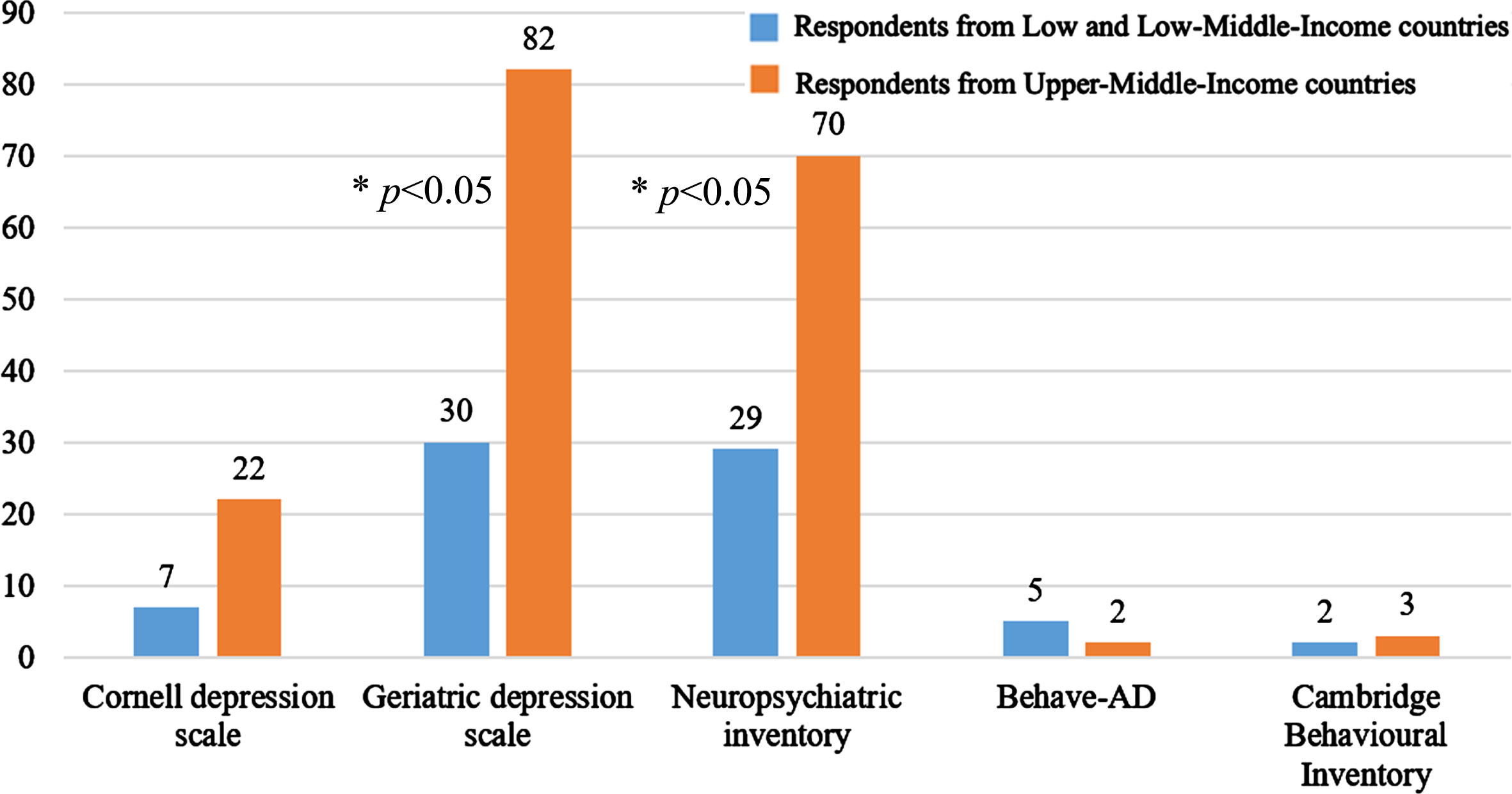
The number of reported uses of behavioral functional tools.
Reasons for not using screening tools
In cases where respondents did not use screening tools, specified reasons were investigated. The four main reasons selected by 20% to 30% of participants from LLMICs included no instrument available in the local language/dialect, lack of local norms or validation, lack of training, and lack of time (Supplementary Figure 2). In contrast, less than 10% of participants from UMICs agreed with the first three reasons, and only 11.6% of participants from UMICs selected a lack of time, compared to 29.1% of respondents from LLMICs. Statistically significant differences were observed across all chosen reasons between the two groups (p < 0.001).
Dementia assessment access and utilization
Participants in LLMICs and UMICs reported their access to various assessments including neuropsychological assessment (61.2% versus 78.8%), specialized language assessment (37.9% versus 50.7%), specialized functional assessment (31.1% versus 40.4%), structural neuroimaging exams (75.7% versus 87.0%), imaging biomarker analysis (17.5% versus 21.9%), cerebrospinal fluid analysis (25.2% versus 36.3%), and genetic testing (25.2% versus 32.9%) for ADRD (Supplementary Figure 3). The UMICs group reported higher access to all assessments, and there were statistically significant differences in the access to neuropsychological assessment (p = 0.001) and structural neuroimaging exams (p = 0.04). There was no statistically significant difference in the proportion of computed tomography (CT) or magnetic resonance imaging (MRI) scans used. However, a significant difference was observed in the average time to receive results between the two groups (p < 0.001), with 52.4% of respondents in LLMICs endorsed receiving results within four weeks, compared to 20.5% in UMICs. In imaging biomarker analysis, positron emission tomography with fluorodeoxyglucose (FDG-PET) was more accessible to participants in LLMICs (13.6%) compared to single-photon computed emission tomography (SPECT) (7.8%) and amyloid-PET (2.9%). SPECT (13.0%, FDG-PET (20.5%), and amyloid-PET (13.7%) were also more accessible in UMICs, while tau-PET was not accessible to either group. Although LLMICs had less access to imaging biomarker analysis, obtaining the results took a shorter time, with 13.6% endorsing having results within one month, compared to 2.1% in the UMICs group. Significant differences were observed in the use of amyloid-PET (p = 0.01) and the average time to receive results (p < 0.001) between groups.
For cerebrospinal fluid analysis, both groups had access to cell count only or general biochemistry and AD biomarkers. However, LLMICs had better access to cell count only or general biochemistry, while UMICs had better access to AD biomarkers. Approximately 17.5% of respondents in LLMICs endorsed getting results within a month, compared to 3.4% in the UMICs group. Significant differences were observed in the use of AD biomarkers and the average time to receive results between the two groups (p < 0.001).
Pharmacological/nonpharmacology treatments and caregiving
Respondents from both groups had access to pharmacological treatments, including cholinesterase inhibitors, memantine, antidepressants, antipsychotics, mood stabilizers, anti-seizure medications, and psychostimulants. The only significant difference was the availability of memantine, which was more accessible in UMICs compared to LLMICs (78.8% versus 58.3%; p < 0.001). Cognitive or neuropsychological rehabilitation, cognitive stimulation or training, occupational therapy, speech and language therapy, and physical therapy were available to patients in both groups. However, cognitive stimulation or training was less accessible in LLMICs compared to UMICs (33.0% versus 54.8%; p = 0.001). In both LLMICs and UMICs, more than half of the respondents indicated that centers provided training or activities for caregivers. General information, group training, and psychological support or psychotherapy were offered to caregivers without any statistically significant difference in access to caregivers between the two groups. However, there is a statistically significant difference in the availability of caregiver trials between the two groups (p < 0.001). Observational or interventional research trials were more available in UMICs (52.1%) than in LLMICs (29.1%).
Main challenges and helpful support
Respondents described daily challenges centered around a population-specific cultural perspective and from an institutional perspective. At the population-specific and cultural perspective level, macro-factors, such as a lack of awareness of dementia, dementia-related stigma, and inadequate health-related policies, as well as micro-factors, such as lack of money to cover medical expenses and caregiver burden, were common. At the institutional level, challenges were classified into business, clinical, or research. From the business platform, a lack of resources for the employee’s well-being, inadequate finances and decision-making for allocation, and a lack of support networks were prominent. The clinical level included inaccessibility and high cost of resources, such as tools and medications, and the lack of high-quality care. The research level included a lack of research opportunities, a lack of interest in research, a lack of research training, and difficulties in recruiting participants.
Respondents also mentioned some solutions to address critical areas in response to these challenges. Regarding population-specific cultural challenges, they noted that support, including financial support for families, meetings/conferences in the LMIC community to raise awareness of dementia, and training and relevant materials for caregivers in local language versions, would be helpful to solve those issues. Solutions to institutional challenges included support via long-term mentorship programs, international collaborative networks, training of clinicians and researchers, and the development and availability of language-appropriate, validated, standardized, and locally adapted tools and treatments that would be very helpful to address core issues (Table 3).
Key challenges that participants face in their clinical or research work and support they would like to receive from ISTAART
*“Training”, “Awareness”, “Funding” are three themes that mentioned in both “Population specific culture” and “Institution” domains. # “Lack of financial resources/workforce (human power)”, “Lack of equipment/facilities/space”, “Lack of support network” are three themes that mentioned in all domains under the “Institution” domain.
DISCUSSION
The increasing prevalence of ADRD, particularly in LMICs, poses a significant threat to global health and demands a comprehensive understanding of how risk factors vary across heterogeneous populations and how to improve access to earlier screening, diagnosis, and effective treatments. The need for more research has been explicitly centralized by the World Health Organization’s Blueprint for dementia research,22,23, 22,23 the Lancet Commission on dementia prevention, intervention, and care,12,24, 12,24 and annual reports 25 from Alzheimer’s Disease International. The results of this study add to the extant literature and provide valuable insights into the challenges and disparities faced by clinicians, healthcare professionals, and clinical researchers working in LMICs who care for patients with ADRD and cognitive impairment.
Our findings highlight the impact of economic vulnerabilities on healthcare systems where economic constraints not only limit the allocation of resources for dementia care but also impede the development of a skilled workforce specialized in managing ADRD. The shortage of healthcare professionals trained in dementia management poses a significant obstacle to providing timely screening, assessment, diagnosis, and care of ADRD patients. Moreover, the concentration of diagnostic tools in urban environments exacerbates disparities, leaving rural areas underserved. The stark contrast in the average number of patients seen in LLMICs compared to UMICs highlights the significant burden of dementia in resource-constrained settings. The geographical distribution of patients, with a higher percentage from suburban/peri-urban areas in LLMICs, reflects the challenges of delivering healthcare in diverse settings. The observed differences in the monthly patients diagnosed with MCI underscore structural disparities in early detection and intervention.
Many respondents in LLMICs reported not using specific guidelines, which raises concerns about standardized diagnostic practices and a lack of uniform assessment practices. The preference for established guidelines in HICs suggests a foundation for uniform diagnostic criteria in both LLMICs and UMICs. However, variations in the choice of guidelines, with DSM, and ICD-10, prominent in LLMICs, DSM, NIA-AA, and unspecified guidelines in UMICs, may indicate the need for consensus-building on diagnostic protocols. These differences could stem from cultural perceptions, resource availability, or familiarity with specific guidelines. The longer evaluation time in UMICs may reflect a more comprehensive evaluation process, but it raises concerns about the feasibility of their implementation in LLMICs. The variations in the utilization of different screening tools highlight the need for standardized training and guidelines to ensure consistent and accurate assessments across diverse settings. The identified reasons for not using screening tools, such as the absence of instruments in local languages, lack of local norms or validation, insufficient training, and limited time, underscore critical barriers in LLMICs. These challenges may contribute to delays in dementia diagnosis and hinder the implementation of early interventions. Tools like the RUDAS or Number Symbol Coding Task are brief and may serve to rapidly screen patients for impairments and further evaluations.26,27, 26,27 Discrepancies in access to various assessments, including neuropsychological evaluations and structural neuroimaging exams, highlight infrastructure challenges in LLMICs. While the availability of specific assessments may be lower, the shorter time to receive results in LLMICs suggests potential efficiency gains or regional differences in healthcare systems. However, the limited access to imaging biomarker analysis in LLMICs emphasizes the need for increased resource allocation and infrastructure development to ensure equitable diagnostic capabilities across different income settings.
The NIA-AA’s 2011 clinical guidelines 28 and 2018 research framework 29 will be accompanied by an upcoming Revised Criteria for Diagnosis and Staging of Alzheimer’s Disease: Alzheimer’s Association Workgroup. The 2024 revision will 1) add criteria for diagnosis and staging to inform research and clinical care since several targeted therapies have received regulatory approval, 2) incorporate plasma biomarkers for categorization, disease diagnosis, and staging, and 3) address nonequivalence between fluid and imaging biomarkers within a category. These essential changes reflect the rapid progress of therapeutics and biological staging, most of which occur in HICs. However, adopting these diagnoses and staging guidelines poses additional challenges for adoption and implementation in LMICs where a lack of screening and underdiagnosis are persistent gaps. Additionally, access to biomarkers is mostly limited to larger cities with resourced institutions in urban centers. Globally, ADRD research will need to measure the influence of structural and social determinants of health 30 on regulating the risk of dementia across different settings. Emerging research in LMICs is examining the direct effects of multidimensional poverty on dementia in fragile and conflict situations.31 - 33
Disparities in healthcare access and utilization were evident based on the consensus from the responses. LLMICs face challenges in obtaining timely results from diagnostic assessments. While some imaging biomarker analyses were more accessible, the overall availability of assessments, including neuropsychological evaluations, was lower compared to UMICs. These findings underscore the urgent need for infrastructure development and resource allocation to bridge these gaps in access. There were variations in the availability of pharmacological treatments and cognitive interventions between LLMICs and UMICs. Notably, the accessibility of memantine was significantly higher in UMICs. Additionally, caregiver support and trials were more prevalent in UMICs. These findings highlight the need for equitable treatment options and support services distribution, ensuring that caregivers in LMICs receive the necessary resources.
The identified challenges at both the population-specific cultural and institutional levels provide a comprehensive overview of the obstacles faced by clinicians and researchers in LMICs. The recognition of factors such as a lack of awareness, stigma, inadequate health policies, financial constraints, and caregiver burden highlights the multi-faceted and complex nature of ADRD across LMICs. This study’s findings have significant implications for developing targeted interventions and policies to improve dementia care in LMICs. Efforts to prioritize dementia assessment and care must consider the historical context, geopolitical factors, and economic infrastructure before shaping healthcare agendas in LMICs. The disparities identified in diagnostic practices, access to assessments, treatment options, and caregiver support call for a comprehensive and context-specific approach. Efforts should be directed towards establishing standardized diagnostic guidelines that are culturally relevant and ensuring the availability of assessment tools in local languages. Capacity-building initiatives, including free training programs for healthcare professionals, can address the identified barriers and enhance the quality of dementia care. Collaborative efforts between local, national, and international stakeholders are crucial for addressing institutional challenges and promoting resource allocation for dementia care.
While this study provides valuable insights, certain limitations should be acknowledged. The survey’s reliance on self-reported data introduces the potential for bias, cross-sectional design impacts change over time, and the sample size in low-income countries was small. Despite making the survey available via any web browser to ensure specific developer applications were not blocked, we were unable to recruit any respondents from China. Most patients are seen by family physicians and/or allied health professionals rather than neurologists. The preponderance of evidence was based on a large number of neurologists completing the questionaire. As a result, the results may reflect a specialist bias, which is more sensitive to dementia symptoms and approaches for assessment and management. Additionally, the study did not explore nuances of cultural beliefs around aging, stigma, and respect for older adults that could impact dementia care. The survey was distributed within the ISTAART network and by professionals in the LIMIC dementia working group, which may lead to a selection bias by including professionals with more awareness of existing resources and knowledge on dementia care. Despite these limitations, the findings contribute to the growing literature on dementia care in LMICs. We recruited diverse ages, sexes, professional backgrounds, and geographic locations to reflect the wide-ranging care providers in LMICs. Translation of the survey into multiple languages underscores the commitment to inclusivity, ensuring that language barriers do not hinder participation. The identified gaps and barriers emphasize the urgency of implementing targeted strategies, including international collaborations, policy reforms, and cultural and linguistic adaptation of screening, assessment, and diagnostic tools, to address the complex challenges associated with ADRD in LMICs.
This study sought to comprehensively examine the challenges and opportunities in dementia care in LMICs. The identified disparities in diagnostic practices, access to assessments, and treatment options underscore the urgency of addressing healthcare infrastructure and resource allocation. A concerted, multiprong approach is required to address economic challenges, ranging from policy reforms at individual institutions (e.g., clinics and hospitals) to international collaboration and support. The proposed solutions, informed by the experiences and perspectives of clinicians and researchers in LMICs, provide a roadmap for policymakers, healthcare organizations, and researchers to enhance dementia care in diverse and resource-constrained settings. The findings contribute to the global knowledge on dementia care and highlight the importance of context-specific strategies to bridge the gap in dementia care in LMICs.
AUTHOR CONTRIBUTIONS
Ganesh Babulal (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Supervision; Writing – original draft; Writing – review & editing); Wenqing Zha (Methodology; Software; Visualization); Jean-Francois Trani (Methodology; Writing – review & editing); Jorge Llibre Guerra (Methodology; Writing – review & editing); Boon Lead Tee (Methodology; Writing – review & editing); Yiqi Zhu (Methodology; Writing – review & editing); Yaohua Chen (Methodology; Writing – review & editing); Ling Chen (Methodology; Writing – review & editing); Michael Bubu (Methodology; Writing – review & editing); Sylvia Josephy-Hernandez (Methodology; Writing – review & editing); Stephen Wandera (Methodology; Writing – review & editing); Wambūi Karanja (Conceptualization; Formal analysis; Investigation; Methodology; Supervision; Writing – review & editing); Ratnavalli Ellajosyula (Conceptualization; Formal analysis; Investigation; Methodology; Supervision; Writing – review & editing); Paulo Caramelli (Conceptualization; Formal analysis; Investigation; Methodology; Project administration; Supervision; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
We would like to thank the respondents for lending their voices and lived experiences to this research and the staff and members of ISTAART who provided support in completing the data collection.
FUNDING
This work was partially supported by the National Institute of Health (NIH) and National Institute on Aging (NIH/NIA) grants R01AG068183 (GMB), R01AG074302 (GMB), and R01AG067428 (GMB).
CONFLICT OF INTEREST
Drs Ganesh Babulal and Paulo Caramelli are Editorial Board Members of this journal but were not involved in the peer-review process of this article nor had access to any information regarding its peer review.
DATA AVAILABILITY
The data supporting the findings of this study are available upon request from the contact author.