
Abstract
Background:
The widespread exposure to plastic products and the increasing number of individuals with cognitive impairments have imposed a heavy burden on society.
Objective:
This study aims to investigate the relationship between plastic product exposure in daily life and cognitive function in older Chinese individuals.
Methods:
Data were obtained from the 2023 Ningxia Older Psychological Health Cohort, comprising 4045 participants aged 60 and above. Cognitive function was assessed using the Mini-Mental State Examination scale. A population-based plastic exposure questionnaire was used to calculate plastic exposure scores (PES). Binary logistic regression was employed to analyze the relationship between PES and cognitive function, while restricted cubic splines were used to examine the dose-response relationship between PES and cognitive function. Latent profile analysis (LPA) was employed to explore the potential patterns of plastic exposure, and logistic regression was used to investigate the relationship between different exposure patterns and cognitive function. A linear regression model was utilized to investigate the relationship between PES and different dimensions of cognitive function.
Results:
Among the 4045 participants, 1915 individuals were assessed with mild cognitive impairment (MCI). After adjusting for all covariates, PES (OR = 1.04, 95% CI 1.02–1.06) was significantly associated with the risk of MCI and exhibited a dose-response relationship. LPA identified two potential categories of plastic exposure, with a higher risk of MCI observed in the group using plastic utensils.
Conclusions:
This study indicates a positive correlation between plastic exposure levels and MCI risk, particularly among individuals who frequently use plastic tableware.
INTRODUCTION
With the rapid growth of the aging population worldwide and the extension of life expectancy, the number of individuals suffering from cognitive impairments is rapidly increasing. According to a national survey in China in 2018, approximately 15.5% of individuals aged 60 and older have mild cognitive impairment (MCI), 6.0% have dementia, and 3.9% have Alzheimer’s disease. 1 Projections suggest that by 2060, the total number of cognitive impairment patients in China will reach 48.68 million. 2 Given the current lack of effective means to reverse dementia and Alzheimer’s disease, and the fact that cognitive impairment is often considered an intermediate state between normal aging and dementia, 3 it is crucial to identify modifiable risk factors associated with cognitive impairment in the early stages.
Previous studies have identified several factors that may impair cognitive function, such as advanced age, low educational level, and an unhealthy lifestyle. 4 Recent animal studies have suggested that exposure to plastic products may also have a negative impact on cognitive function.5–7 Plastic products are widely used in industrial production and daily life due to their lightweight and corrosion-resistant properties. 8 With the accelerated urbanization in China and the advancement of industrial levels, exposure to plastic products among the population is becoming increasingly common. For example, plastic bottles used for packaging beverages, soy milk, and milk; plastic bags used for shopping; and disposable plastic containers widely used in takeout services. 9 In previous studies, the main components of these plastic products were found to be additives such as phthalates, as well as plastic particles like polyethylene, polypropylene, and polyamide.10–12 These harmful substances are continuously released and enter the human body through the respiratory and digestive systems. In recent years, researchers have detected plastic particles in human blood, 13 lungs, 14 colon, 15 placenta, 16 feces, 17 and breast milk, 18 confirming that long-term exposure can affect heart function, 19 disrupt normal liver lipid metabolism 20 and induce cytotoxicity, 21 leading to comprehensive impacts on human health.22–25 Therefore, the harm of plastic products to human health should not beignored.
Recent animal studies have found that plastic exposure can impact cognitive function. For example, exposure to polystyrene microplastics exacerbates cognitive decline in aging mice, leading to potential neurotoxicity; 7 maternal exposure to polystyrene plastic particles can increase the risk of neurodevelopmental defects and cognitive impairments in offspring; 6 ecological research suggests that exposure to microplastics can negatively impact the cognitive function of bees. 5 Additionally, Hu et al. found that the oral ingestion of plastic leachate can lead to diminished cognitive functions and neuroinflammation in mammals, which may be related to changes the gut microbiota. 26 In a quasi-experimental study conducted by Zhang et al. involving human participants, changes in gut microbiota were observed in the plastic exposure group. 9 Combining the findings from animal and human experiments, we speculate that plastic exposure may have an impact on cognitive function in humans. Given the widespread prevalence and harmful effects of plastic exposure, as well as the scarce use of questionnaires in epidemiological surveys to assess plastic exposure in populations and study its relationship with cognitive function, there is an urgent need for an epidemiological survey in populations to investigate theirrelationship.
The main objective of this study is to assess plastic exposure in the population using a plastic exposure questionnaire and explore the relationship between plastic exposure and the cognitive decline of the older in China.
METHODS
Data sources and study population
The data for this cross-sectional study were obtained from the 2023 Ningxia Older Mental Health Cohort. This cohort was established between 2013 and 2015, with follow-up visits conducted every two to three years thereafter. Standardized questionnaires were used to collect data on sociodemographic and lifestyle factors, as well as health-related information, In addition, the plastic exposure questionnaire was added for the first time in the 2023 follow-up survey to assess the plastic exposure of the population. The primary purpose of the cohort is to monitor and evaluate the mental health status and dynamic trends of individuals aged 60 and above, along with assessing the implementation effects of various intervention measures and identifying influencing factors. The baseline of the project included a total of 4,458 eligible participants, and by 2023, five rounds of follow-up visits had been completed, resulting in a total of 13,680 older research subjects. 27
This dataset collected data on 4,350 participants in 2023, excluding participants under 60 years of age and incomplete data, and 4,045 participants were eventually included in the analysis.
Assessment of cognitive function
Cognitive function was assessed by the Mini-Mental State Examination (MMSE) scale, and the reliability and validity of the MMSE scale were well evaluated in different populations. 28 The MMSE scale assesses cognitive function in five dimensi-ons, 29 including orientation, registration, calculation, recall, and language ability, with a total score of 30 points. Studies have shown the feasibility of using educational levels to screen for cognitive impair-ment. 30 Therefore, we defined MCI as follows: MMSE score < 18 for subjects without formal education; MMSE score < 21 for those with primary school education; and MMSE score < 25 for those with more than middle school education. 31 Subjects with higher MMSE scores were considered to have normal cognition.
Assessment of plastic exposure
Plastic exposure was assessed by the population-based Plastic Exposure questionnaire (Supplementary Table 1). This questionnaire was designed by Hu et al and has high reliability (Cronbach’s α=0.86) and validity (SCVI/UA=0.81, S-CVI/Ave=0.979). 32 The questionnaire consists of 12 questions aimed at evaluating the frequency of individuals’ daily exposure to plastic products. We added up the scores of 12 questions to get the plastic exposure score (PES) and divided PES into high and low exposures using the median. Furthermore, the PES was split intoquartiles.
Covariables
Following the previous studies,33,34, 33,34 we consider potential confounders, including age, sex, ethnicity (Han versus others), residence (rural versus urban), main occupation before age 60 (nonmanual versus manual), marital status (married and others), education background (illiteracy, primary school, and junior high school), living type (living alone, living with a partner and others), income (<2000 CNY, 2000–5000 CNY, >5000 CNY), sleep quality, smoking, alcohol consumption, daily activity ability, depression, and 5 kinds of self-reported diseases (cancer, diabetes, hypertension, stroke, and cardiovascular disease).
Statistical analysis
Data were analyzed using various statistical methods. For normally distributed continuous variables, means and standard deviations (SDs) were reported. Categorical variables were described in terms of frequency and percentage. The t-tests and chi-square tests were utilized to compare differences in the baseline characteristics between the different groups, as appropriate.
Binary logistic regression analysis was used to investigate the association between plastic exposure and risk of MCI, with adjustment for potential confounders. Three models were constructed: Model 1 without confounding adjustment, Model 2 with demographic characteristics adjusted, and Model 3 which further adjusted health-related behaviors. Subgroup analysis was performed based on age (60–75 and > 75 years), sex, residence, occupation, marital status, smoking, alcohol consumption, and depression using Model 3. Restricted cubic spline (RCS) analysis was employed to identify any potential non-linear relationship between the PES and the risk of MCI. Latent profile analysis (LPA) was employed to explore the potential patterns of plastic exposure, and logistic regression was used to investigate the relationship between different exposure patterns and cognitive function. Adjust all covariates and use a linear regression model to explore the relationship between plastic exposure and five dimensions of cognitive function. For the robustness of the results, we have carried out several sensitivity analyses: (1) using propensity score inverse probability-weighted (IPTW) equilibrium covariates; (2) calculating E-value using methods by VanderWeele andDing.35,36, 35,36
R version 4.2.2 and Mplus version 8.3 were used for statistical analysis. All tests were two-tailed, and a p-value of less than 0.05 was considered statistically significant.
Ethics approval
This study was approved by the Ethics Committee of Ningxia Medical University (grant no. 2015151). Each subject signed written informed consent prior to the interview.
RESULTS
Baseline characteristics
Table 1 presents the baseline characteristics of participants with and without MCI. Of the 4,045 participants included in the analysis, 1,915 were assessed for MCI. The mean age of participants was 72.5±6.0, and 46% were male. Participants with MCI were older, more female, lived in rural areas, and had higher PES than those with normal cognitive function. In addition, statistically significant differences were observed in occupation, education, marital status, ethnicity, type of residence, income, quality of sleep, smoking and drinking, and depression (all p < 0.05). In the baseline characteristics across different levels of plastic exposure, participants in the high-exposure group were more likely to be younger, reside in rural areas, have lower income, and suffer from MCI. Detailed data can be found in Supplementary Table 2.
Baseline characteristics of participants
ADL, Activity of Daily Living Scale; PES, Plastic exposure score.
Logistic regression analysis of plastic exposure and MCI
Table 2 presents the results of a logistic regression analysis examining the relationship between plastic exposure and MCI. After adjusting for potential confounders (in Model 3), the findings indicate a substantial link between the PES (OR = 1.04, 95% CI 1.02–1.06) and the risk of MCI. When the PES was categorized into high and low levels of exposure, the risk of MCI was increased by 28% in the high-exposure group compared with the low-exposure group after adjusting for confounding factors (OR = 1.28, 95% CI 1.12 – 1.46). When dividing PES into quartiles and adjusting for all confounding factors (in Model 3), as compared to quartile 1, the adjusted ORs (95% CIs) for MCI were 0.98 (0.82–1.16) for Quartile 2, 1.23 (1.01–1.47) for Quartile 3, and 1.30 (1.07–1.58) for Quartile 4.
Logistic regression analysis of plastic exposure and MCI
Model 1 was unadjusted. Model 2 was adjusted by age, sex, residence, occupation, education, marital status, ethnicity. Model 3 was adjusted by age, sex, residence, occupation, education, marital status, ethnicity, living type, income, sleep quality, smoking, alcohol consumption, depression. OR, odds ratio; 95% CI, 95% confidence intervals.
Dose-response relationship
Figure 1 and Supplementary Figures 1 and 2 illustrate the results of the RCS regression analysis. A linear dose-response relationship was found between the PES and the risk of MCI among all participants (p for overall = 0.001, p for nonlinear = 0.283, Fig. 1). The risk of MCI demonstrated a considerable increase as PES increased. In addition, a statistically significant linear dose-response relationship was observed in male participants (p for overall < 0.001, p for nonlinear = 0.702, Supplementary Figure 1), but not in female participants (p for overall = 0.153, p for nonlinear = 0.094, Supplementary Figure 2).
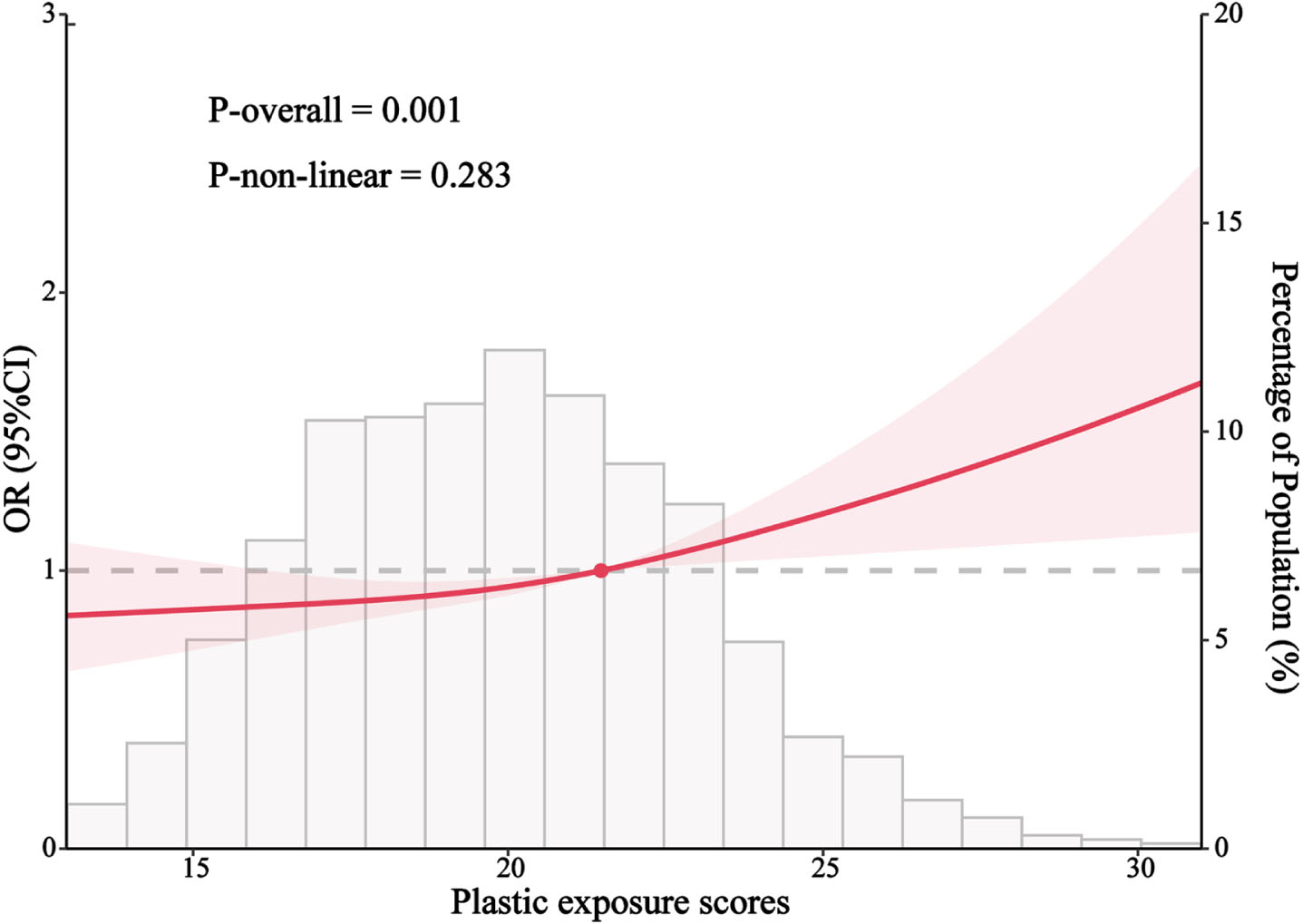
A dose-response relationship was observed between the plastic exposure scores and MCI through a restricted cubic spline regression model. The model was adjusted for age, sex, residence, occupation, education, marital status, ethnicity, living type, income, sleep quality, smoking, alcohol consumption, depression. Solid lines represent odds ratios (ORs) and the shaded areas represent 95% confidence intervals (CIs).
Subgroup and interaction analysis
Subgroup analysis was carried out to evaluate the correlation between the PES and the risk of MCI among specific subpopulations based on various demographic characteristics. Figure 2 demonstrates that, after controlling for all relevant factors as mentioned earlier, The association between PES and MCI was more significant in aged > 75 years (OR = 1.04, 95% CI 1.01–1.06), males (OR = 1.06, 95% CI 1.03–1.09), rural (OR = 1.04, 95% CI 1.02–1.07), nonmanual (OR = 1.04, 95% CI 1.02–1.06) and other marital status (OR = 1.04, 95% CI 1.02–1.06) groups. In addition, we found that gender can alter the association between PES and MCI (p for interaction = 0.031).

Association of PES with MCI stratified by participant characteristics. Each stratification controlled for all factors except the stratification factor itself. P-interaction was assessed by combining the variables’ cross-product term (PES×baseline characteristics) in the same model. OR, odds ratio; 95% CI, 95% confidence intervals.
Latent profile analysis
As shown in Table 3, to explore potential categories of plastic exposure, we added classes or groups at each step until the model fit did not improve further. Combining the indicators in Table 3 with the actual situation, two categories were identified as the optimal model. As can be observed in Fig. 3, the two categories differed greatly on the tenth question. The tenth question was about the frequency of plastic tableware use, so we named the two categories high plastic tableware exposure group and low plastic tableware exposure group respectively.
Fit indices of latent profile analysis

Feature distribution of potential classes.
Table 4 displays the association between two potential patterns of plastic exposure and MCI. After adjusting for all confounding factors, compared to the low plastic tableware exposure group, the high plastic tableware exposure group had a 22% increased risk of MCI (OR = 1.22, 95% CI 1.08–1.40).
Logistic regression analysis of plastic exposure pattern and cognitive impairment
Model 1 was unadjusted. Model 2 was adjusted by age, sex, residence, occupation, education, marital status, ethnicity. Model 3 was adjusted by age, sex, residence, occupation, education, marital status, ethnicity, living type, income, sleep quality, smoking, alcohol consumption, depression. OR, odds ratio; 95% CI, 95% confidence intervals.
Table 5 shows that there is a significant association between PES and MCI in the high plastic tableware exposure group after adjusting all confounding factors (OR = 1.04, 95% CI 1.01–1.07). Furthermore, within in the high plastic tableware exposure group, when PES was divided into high-exposure and low-exposure, participants with high-exposure had 24% (OR = 1.24, 95% CI 1.03–1.48) increased risk of MCI compared with low- exposure. No such association was found in the low plastic tableware exposure group.
Logical regression analysis of PES and MCI in different plastic exposure pattern groups
Group1: Low plastic tableware exposure group; Group2: High plastic tableware exposure group. Model 1 was unadjusted. Model 2 was adjusted by age, sex, residence, occupation, education, marital status, ethnicity. Model 3 was adjusted by age, sex, residence, occupation, education, marital status, ethnicity, living type, income, sleep quality, smoking, alcohol consumption, depression. OR, odds ratio; 95% CI, 95% confidence intervals.
Linear regression between plastic exposure and cognitive function in different dimensions
The results from Table 6 indicate a significant negative correlation between PES and two dimensions of cognitive functions (registration, attention, and calculation) after adjusting for all covariates. Following the categorization of PES into two groups, participants in the high-exposure group (Q2) exhibited a decrease of 0.051 points (95% CI: –0.097, –0.006) in registration scores and 0.168 points (95% CI: –0268, –0.068) in attention and calculation scores compared to those in the low-exposure group (Q1). After further stratifying PES into four categories, participants in the fourth quartile (Q4) of plastic exposure demonstrated a reduction of 0.065 points (95% CI: –0.131, –0.001) in registration scores and 0.229 points (95% CI: –0.373, –0.007) in attention and calculation scores relative to participants in the first quartile (Q1) of plastic exposure.
Linear regression between Plastic exposure and cognitive function in different dimensions
Numerical representation β coefficient (95% CI); *p < 0.05; **p < 0.01.
This linear regression model was adjusted by age, sex, residence, occupation, education, marital status, ethnicity, living type, income, sleep quality, smoking, alcohol consumption, depression.
Sensitivity analysis
After employing propensity score reweighting using the IPTW method to minimize discrepancies in participant characteristics, we achieved similar results, indicating that our main findings were not influenced by any biases stemming from the baseline characteristics of the participants (Supplementary Tables 3 and 4 and Fig. 3). Additionally, the outcomes of the E-value are presented in Supplementary Tables 5 and 6. For example, after dividing PES into two categories based on the median, the odds ratio of high-exposure to MCI compared to low-exposure was 1.281, resulting in an E-value of 1.881. Therefore, any unmeasured confounder must have an odds ratio with MCI of at least 1.881 to fully explain the observed odds ratio of 1.281 (Supplementary Table 5).
DISCUSSION
The results of this study indicate that in older individuals in China, higher PES are independently associated with the risk of MCI, showing a linear dose-response relationship. Furthermore, LPA identified potential categories of plastic exposure, revealing that individuals using plastic tableware have a higher risk of MCI compared to those who do notuse it.
Our research findings indicate that plastic exposure increases the risk of MCI. Previous studies have shown that harmful substances released from plastic exposure, such as phthalates, bisphenol A, polyethylene, and polyamide, are significant contributors to health damage, with broad-ranging impacts on health.22–25,37, 22–25,37 Some of these harmful substances have been demonstrated to affect cognitive function, for example, A birth cohort study in Taiwan suggests that maternal prenatal bisphenol A exposure is associated with cognitive developmental deficits in children. 38 Regarding the mechanisms through which plastic exposure impairs cognitive function, studies have shown that endocrine-disrupting chemicals such as bisphenol A induce neuroinflammation through various pathways including oxidative stress, activation of glial cells, alteration of gene expression, and damage to the blood-brain barrier. 39 Neuroinflammation is widely believed to be a significant pathway leading to cognitive decline. 40 Furthermore, research has also shown that microplastics and phthalates present in plastics can lead to alterations in the gut microbiota of mammalian species.41,42, 41,42 The gut microbiota, also known as the “second brain” in the abdomen, plays a crucial role in the development of age-related neurodegenerative diseases and interacts with the brain through the microbiota-gut-brain axis (MGBA). 43 Multiple research findings also indicate that the gut microbiota may influence cognitive function through pathways such as the MGBA.26,44, 26,44 In a recent quasi-experimental study by Zhang and colleagues in the population, alterations in the abundance of bacteria such as Lactobacillus, Bacteroides, and Clostridia in the gut microbiota of the plastic exposure group were observed. 9 This may be one of the reasons for the impact of plastic on human cognitive function. However, knowledge regarding the effects of plastic exposure on human cognitive function remains limited, necessitating further research to fully understand the relationship between plastic exposure and human cognitive function, as well as the underlying mechanisms involved.
Through LPA, we categorized plastic exposure into two groups and found that in the population using plastic tableware, the PES was independently associated with the risk of MCI. This relationship was not significant in the population not using plastic tableware. Tableware is an essential part of our dining experience as it comes into direct contact with food. When plastic tableware is used at home, endocrine disruptors and plastic particles are released into the food. 32 Moreover, many studies have shown that with increasing temperature, the release of plastic particles from disposable food-grade nylon bags, low-density polyethylene cups, bottles, and other plastic products also increases.45,46, 45,46 China has a rich tradition of consuming hot beverages and foods, 47 which implies that plastic tableware is frequently used in heated or high-temperature conditions. Therefore, individuals using plastic tableware may be exposed to higher levels of plastic particles, thereby increasing the risk of MCI.
This study observed a linear dose-response relationship between PES and the risk of MCI. After categorizing PES based on the median and quartiles, it was found that higher levels of plastic exposure were associated with an increased risk of MCI. Furthermore, consistent results were obtained through propensity score inverse probability weighting and several other sensitivity analyses, indicating that plastic exposure is an important risk factor for MCI. Therefore, the development of strategies and interventions aimed at reducing the risk of MCI in the older is imperative. These methods may include enhanced public awareness and education to increase people’s understanding of the health hazards posed by plastics.
There are several additional limitations to this study. Firstly, it is a cross-sectional study and cannot establish a causal relationship between plastic exposure and MCI. Secondly, using self-reported frequency of plastic product exposure instead of directly measuring exposure levels may not reflect the exact exposure dose, potentially affecting the analysis and leading to erroneous findings. Thirdly, the sample size of this study is small and the sample population is limited to one province, so the study results cannot be generalized to the national population. Therefore, further prospective studies with larger sample sizes are warranted. Despite these limitations, the study has several strengths. Firstly, we assessed the frequency of plastic exposure in the population using a questionnaire and explored the relationship between plastic exposure and cognitive function in the population, which is an area lacking in previous research. Secondly, we categorized plastic exposure in various ways and explored potential categories of plastic exposure, providing a comprehensive and detailed analysis of the relationship between plastic exposure and MCI. Thirdly, we controlled for various confounding factors and conducted several sensitivity analyses, enhancing the robustness of the study results.
Conclusions
The study shows that the higher the level of plastic exposure, the higher the risk of MCI, particularly among individuals who frequently use plastic tableware. Therefore, it is necessary to raise public awareness of the health hazards associated with plastic products and develop alternatives to reduce these risks. In addition, there is still a lack of knowledge about the adverse effects of plastics on human health, and further prospective studies and randomized controlled trials are needed to verify the relationship between plastic exposure and MCI.
AUTHOR CONTRIBUTIONS
Yongbin Zhu (Formal analysis; Methodology; Visualization; Writing – original draft); Yueping Wu (Formal analysis; Methodology); Liping Shi (Methodology); Yue Yang (Investigation); Yanrong Wang (Visualization); Degong Pan (Data curation); Shulan He (Conceptualization; Methodology); Liqun Wang (Data curation; Resources; Supervision); Jiangping Li (Conceptualization; Project administration; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors acknowledge all the participants.
FUNDING
This study was supported by Scientific Research Funding Project of Ningxia Medical University (Grant number: XT2022014) and National Natural Science Foundation of China (Grant number: 82260662).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
Data will be made available on request.