
Abstract
Alzheimer’s disease (AD) is a progressive neurodegenerative disorder responsible for over half of dementia cases, with two-thirds being women. Growing evidence from preclinical and clinical studies underscores the significance of sex-specific biological mechanisms in shaping AD risk. While older age is the greatest risk factor for AD, other distinct biological mechanisms increase the risk and progression of AD in women including sex hormones, brain structural differences, genetic background, immunomodulation and vascular disorders. Research indicates a correlation between declining estrogen levels during menopause and an increased risk of developing AD, highlighting a possible link with AD pathogenesis. The neuroprotective effects of estrogen vary with the age of treatment initiation, menopause stage, and type. This review assesses clinical and observational studies conducted in women, examining the influence of estrogen on cognitive function or addressing the ongoing question regarding the potential use of hormone replacement therapy (HRT) as a preventive or therapeutic option for AD. This review covers recent literature and discusses the working hypothesis, current use, controversies and challenges regarding HRT in preventing and treating age-related cognitive decline and AD. The available evidence indicates that estrogen plays a significant role in influencing dementia risk, with studies demonstrating both beneficial and detrimental effects of HRT. Recommendations regarding HRT usage should carefully consider the age when the hormonal supplementation is initiated, baseline characteristics such as genotype and cardiovascular health, and treatment duration until this approach can be more thoroughly investigated or progress in the development of alternative treatments can be made.
Keywords
INTRODUCTION
Aging is an inevitable biological process which contributes as the greatest risk factor for late-onset Alzheimer’s disease (AD). The prevalence of AD increases significantly with age as aging contributes to the accumulation of cellular damage and dysfunction. With the global population and average life expectancy continuing to rise, the burden of age-related diseases such as AD on the public health systems is rapidly becoming overwhelming. Consequently, the demand for treatment is increasing, however therapeutic options remain limited [1].
Women account for two-thirds of global dementia cases, reflecting the 2-3 times increased risk of developing AD compared to men, in which symptoms of cognitive decline manifest as more severe in women and progress more rapidly into the advanced stages of the disease [2]. Prioritizing the identification of factors responsible for the overrepresentation of women in AD and devising approaches to mitigate this elevated risk could have profound implications for the imminent increase in global AD incidence.
A significant sex difference between men and women is the sex-specific precisely controlled fluctuation in adult hormone levels. Estrogens are the primary female sex hormones, primarily produced in the ovary upon stimulation of primary follicle development, with one of its key physiological roles being the regulation of ovulation. In contrast to male sex hormones, which maintain relatively constant levels throughout adulthood, menopause leads to the natural depletion of the primordial female follicle pool which results in the cessation of estrogen production and the rapid decline in endogenous hormone levels. Both androgens and estrogens are neuroactive and are recognized to have significant neuroprotective effects [3, 4]. However, the loss of female neuroprotective factors during menopause has been hypothesized to contribute to the profound alteration in the estrogenic environment and as a result may have contributed to an increased vulnerability in women to develop AD [5–7].
The critical window hypothesis proposes the timing of hormone replacement therapy (HRT) plays a crucial role in the effectiveness and potential benefits for menopausal women. According to this hypothesis, there is an optimal period referred to as the ‘window of opportunity’ during which estrogen therapy can provide the most effective neuroprotective benefits. It has been proposed that HRT effectivity is highly contingent on a specific period shortly after the menopausal transition when administration is most beneficial. Estrogen therapy is particularly effective at delaying cognitive aging when initiated shortly after menopause, but not when it is initiated decades after the menopause. However, some but not all, previous findings support this hypothesis [8]. An alternative to the critical window hypothesis is the healthy cell bias hypothesis, which emphasizes the timing of HRT initiation. According to this hypothesis, the likelihood of HRT having a beneficial effect is higher if it is started closer to the age of menopause. A key distinction between the critical window hypothesis and the healthy cell bias hypothesis is that the latter uniquely considers baseline characteristics, such as neurological status, as crucial factors in predicting the effectiveness of HRT.
HRT traditionally had been prescribed for peri- and postmenopausal women to supplement declining endogenous estrogen levels and alleviate various undesirable vasomotor and menopausal symptoms, such as depression, irritability, hot flashes, perspiration, and urinary incontinence [9]. The effect of menopausal hormone therapy on the risk of dementia is uncertain [10]. Early meta-analyses of collated results from studies discovered a protective effect of menopausal HRT against the onset of AD, providing strong evidence to substantiate the beneficial claims of HRT on cognition [11, 12], while newer studies suggest moderate effectiveness in reducing AD risk [13]. Observational data suggested that HRT was linked to a reduced risk of dementia, but some experimental evidence shows that HRT can increase the risk of dementia. In a cohort study in Taiwan, the HRT cohort had a 35% increased risk of dementia when compared with the comparison cohort [14]. In a meta-analysis conducted, estrogen therapy (ET) use in midlife was linked to a 32% reduction in dementia risk, while estrogen-progestogen therapy (EPT) showed a non-significant 23% risk reduction compared to non-use. In contrast, late-life use of both formulations was associated with an increased risk of dementia, with the risk being higher for EPT than ET, though neither increase was statistically significant [15].
HRT in the prevention of cognitive decline has also shown conflicting results. Studies that included Apolipoprotein E (APOE) as an independent variable have produced mixed results, reporting positive, null, and negative outcomes associated with hormone therapy [16]. Women who carried the Apolipoprotein E4 (APOE4) gene and had undergone HRT therapy had shown larger brain volumes and improved cognition in comparison to APOE4-non-HRT users [17]. APOE4 HRT users had an increased volume in the entorhinal and amygdala volumes which both play an important role in cognition therefore this could indicate HRT as a neuroprotective factor against AD in a specific subcohort of individuals [17]. In contrast, a notable trend was observed in another study where women with APOE4 who received HRT experienced more cognitive decline compared to those with APOE4 who did not undergo estrogen therapy [18]. Kunzler and colleagues found that the efficacy of HRT with APOE4 is dependent on the relative contribution of extracellular and soluble amyloid-β (Aβ) to neurodegeneration during AD progression [19]. In contrast, compared with APOE4 women who never used HRT, past or current HT users experienced modest yet statistically significant worse rates of decline in cognition [20].
The rising interest in HRT as a neuroprotective treatment accumulated increased attention, promoting laboratory research to explore the underlying mechanisms of estrogens and instigation of clinical trials to further address this hypothesis. The Women’s Health Initiative Memory Study (WHIMS) [21] recruited a subset of patients from the Women’s Health Initiative Study (WHI) is the largest-scale randomized controlled trial to date that evaluated the impact of HRT on dementia and cognitive impairments that enrolled participants who were dementia-free and aged over 65 years. A total of 4,532 participants were randomized and received either continuous combined HRT, or placebo [22], while an additional 2974 hysterectomized women received continuous unopposed HRT, or placebo [21]. After 4 years, the data collected revealed that exposure to HRT led to a twofold increase in the risk of dementia diagnosis, resulting in exacerbated cognitive decline compared to the control group. The findings of WHIMS at the time were particularly controversial, as they directly contraindicated evidence suggesting the beneficial effects of estrogen on cognitive health [22, 23]. Today, these results have left a profound uncertainty regarding the clinical recommendations for postmenopausal women, which has persisted in both literature and public opinion two decades later.
This review focuses on assessing critical differences in clinical and observational studies that have explored the impact of estrogens on cognition or attempted to address the predominant queries regarding the utilization of HRT as a potential therapeutic intervention for AD.
METHODOLOGY
We retrieved articles through a systematic review of the databases SCOPUS, and PubMed (keywords “Alzheimer’s disease”, “hormone replacement therapy”, “hormone therapy”, “dementia”, “estrogen”, “estradiol”, “cognition”, and “memory” and by searching reference sections from identified studies and review articles). The papers returned from the search were then manually screened for relevance. The results of the systematic review were published earlier covering the published literature until 2021 [24] and the main findings are summarized here. In addition, the screened literature published after 2021 has also been included (Fig. 1). Each abstract was screened independently by two authors to identify the articles that met our inclusion criteria of clinical studies with an HRT focus. All authors discussed any conflicts to determine whether to include or exclude articles from this review. The articles referred to in Fig. 1 are summarized in Table 1 and are discussed in the relevant sections of the review.
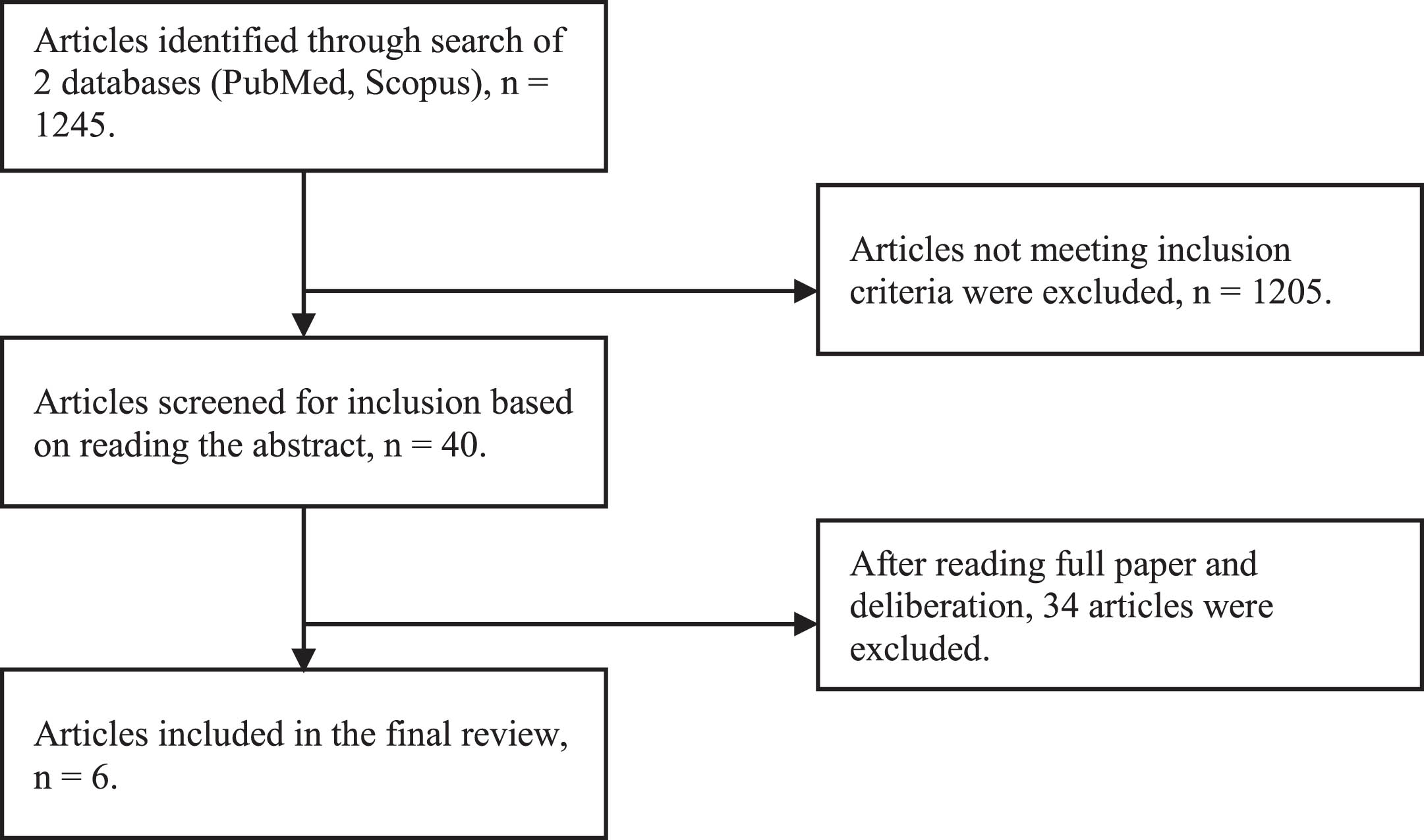
PRISMA 2020 Flow Diagram detailing the article selection process.
Summary of human observational and clinical studies, and studies with retrospective analysis published since 2021
AD, Alzheimer’s disease; CEPM, combined estrogen plus progestin by the manufacturer; CEPP, combined estrogen plus progestin by the physician; EMTs, estrogen-modulating therapies; HRT, hormone replacement therapy; MCI, mild cognitive impairment; MHT, menopausal hormone therapy; MCI, mild cognitive impairment; NDDs, neurological degenerative diseases.
The primary objective of this review is to compile the relevant, including the most recent, literature available on the subject and discuss the mechanisms, effects, and hypotheses that underlie the contradictory findings regarding HRT in the prevention and treatment of age-related cognitive deficits and AD. This review aims to examine the potential therapeutic efficacy of HRT in AD management, while also critically evaluating the methodological differences that could explain the contradictory findings found in the literature.
SEX DIFFERENCES IN ALZHEIMER’S DISEASE
AD is characterized by its widespread cortical hypertrophy and the hallmarks include accumulation of extracellular Aβ core and intracellular hyperphosphorylated tau protein. AD exhibits gender bias, in which one gender has shown to have a greater prevalence or severity of the disease than the other. Sex differences influence the development and progression of AD and women have a greater lifetime risk of developing AD. It is estimated that the lifetime risk for AD by the age of 45 is approximately one in five (20%) for women and one in 10 (10%) for men with the risk for both sexes being slightly higher at age 65 [25]. An important factor to take into consideration is that aging is one of the most critical risk factors for sporadic AD and thus a higher frequency of AD diagnosis in women can be attributed to women living longer than men [26]. The percentage of people with AD increases dramatically with age with 5% of people aged 65–74, 13.1% of people aged 75–84, and 33.3% of people aged 85 or older having AD [27]. After the age of 65, the remaining lifetime risk of developing AD for women is almost twice that of men. However, the incidence of AD cannot simply be attributed to the higher longevity of women compared to men [28]. It has also been shown that neurodegeneration and clinical symptoms of the disease occur more rapidly for females compared to men [26]. Other influencing factors may include differences in cognitive ability, brain anatomy, genetic background and sex steroid hormones. The prevalence and effects of cerebrovascular, metabolic and socio-economic risk factors also differ between men and women for AD [29]. The impact of dementia not only varies by sex differences but also geographically [29]. Many studies in North and South America cohorts have found no significant sex difference in the incidence of AD [30, 31]. In comparison, several studies performed in Europe [32] and Asia [33] suggested a higher incidence in women, in particular for women over the age of 80.
Brain atrophy is a characteristic feature of AD with the rate and patterns of AD atrophy differing between the sexes with brain atrophy being faster in women than in men [34]. The sex differences in brain structures have been observed by magnetic resonance imaging in human studies. Men have demonstrated larger amygdala and thalamus volumes compared to women; this is worth noticing as there is a relatively higher number of androgen receptors in the amygdala. Women have shown larger hippocampus size with a relatively higher number of estrogen receptors in the hippocampus [35]. Men on average have a larger overall absolute brain volume (i.e., not corrected for body size) ranging from 8% to 13% larger volume in males than females [36] and thus would suffer less or slower structural loss and have shown less atrophy in numerous brain regions along with a slower decline in certain cognitive tasks in comparison to women. However, throughout a woman’s lifespan, it has been shown that there is a greater cortical thickness compared to men which would have a protective effect [37]. Furthermore, regarding the ventricular system, men have greater cerebrospinal fluid (CSF) volumes, lateral ventricles, and sulcal volumes in comparison to women. In addition, a higher percentage of white matter is observed in men in contrast to women having a higher percentage of grey matter and higher cerebral blood flow both at rest and during cognitive activity [38]. The sex differences in brain structure and function have implications for the differences in biofluid results. In women, a more pronounced increase was reported in neurofibrillary tangles in the hippocampus with age in comparison to men suggesting a sex-specific neuroanatomic susceptibility [39].
Several studies have examined sex differences in AD-related biofluid-based biomarkers as a method to examine the development of AD. Regarding Aβ, low levels of Aβ42 or the Aβ42/Aβ40 ratio indicate an elevated brain amyloid pathology. No sex differences were observed in the concentrations of CSF Aβ42, Aβ40, or Aβ42/Aβ40 ratio and total tau concentration [40]. However, women showed a greater decline in hippocampal atrophy and memory performance and increased CSF phosphorylated-tau concentrations for a given CSF Aβ42 concentration [41]. One study using the immunomagnetic reduction assay found higher plasma total tau concentrations in men after adjusting for age and APOE genotype [42]. Higher CSF neurofilament light (NfL) concentrations were observed among men across the AD clinical spectrum [43], though plasma and serum NfL concentrations showed no sex difference [44]. Neurogranin (Ng) concentrations were higher in cognitively normal women compared to men in one study [45], but another study showed higher CSF Ng concentrations in women that did not reach significance [46]. Currently, there is minimal literature on markers of AD and related sex differences [47].
Sex differences have been observed in cognitive function in both adulthood and aging. Studies have shown that men perform better on spatial memory while women are more proficient at verbal and object location tasks. Gender-dependent cognitive activity is heavily dependent on sex hormones as these hormones significantly influence cognitive function from neuronal development until the end of the lifespan. Cognitive impairment especially memory problems is a frequent complaint of patients impacted by AD. Mild cognitive impairment (MCI) is associated with the preclinical stage of AD. Studies have shown early onset MCI patients tend to have more visuospatial memory problems, while late-onset MCI patients have shown more verbal memory issues [35]. As women have the advantage in verbal memory, there is a sustained cognitive performance in the early stages of AD despite moderate levels of brain pathology. This may be functionally beneficial; however, the downside has shown that there is a delay in amnestic MCI diagnosis resulting in a more severe burden of disease at the time of diagnosis and a rapid decline afterwards. As a result, this limits the opportunity for early intervention [25]. However, it is important to note the complexity of factors to take into consideration such as existing health and education. Overall, women generally performed better in verbal learning with both men and women experiencing a decline in performance with age. However, in impoverished older cohorts with poorer health, and among slightly better-educated men, a trend emerged showing a male advantage starting from age 70. Conversely, in cohorts where women had better education, they demonstrated less decline with age [48].
The main risk factor which has been identified in AD contributing to the sex difference in disease prevalence is the decline in sex-steroid hormones in postmenopausal women. This decline has an implication in metabolic dysregulation and bioenergetic deficits in the etiology of the disease. A significant sex difference that has a prognostic impact on AD in women is the menopause transition (MT). This transitional state in females manifests further than reproductive senescence. It exhibits several neurological symptoms, including disruption of estrogen-regulated systems which accounts for impairment in multiple cognitive domains. Preclinical studies have demonstrated that the uncoupling of estrogen-mediated brain energy metabolism has resulted in the marking of the onset of MT and induces a hypometabolic state which can be accompanied by shifts in neurological function which are regulated by estrogen that seem to be unrelated to reproduction [49]. Typically, symptoms of late-onset AD arise in the early to mid-70 s, yet the pathology of AD appears during the prodromal phase which occurs in proximity to MT [49].
Estrogens are the primary female sex hormones and are important in the early development of both primary and secondary sexual characteristics along with embryonal and fetal development of the neuronal networks [50]. The three major forms of physiological estrogens are estrone (E1), estradiol (E2, or 17β-estradiol), and estriol (E3). Estrogens are mainly produced by the ovaries; however, a significant amount of synthesis occurs within the brain, primarily the E2 form. Whereas E1 plays a larger vital role after menopause and E3 is the least potent estrogen, E2 is the major product resulting from the whole biosynthesis process and is described as the most potent estrogen during the premenopausal period. Evidence highlights the importance of E2 in regulating synaptic plasticity, promoting neural survival, and mediating sex-specific behaviors [51]. Menopause has been shown to result in decreased estrogen concentration due to the loss of ovarian follicular function [52]. In addition, at an advanced age, there is an impairment of the cognitive enhancing effect of estrogen that may be associated with age-linked alterations in signaling and the expression of estrogen receptors (ERs) in the hippocampus [53].
There is a strong assumption about the link between estrogen deficiency in women with menopause and AD [54]. The neuroprotective function of estrogen results in decreasing Aβ and glutamate toxicities [55]. Further neuroprotective effects include improving synaptic plasticity, diminishing the brain’s inflammation [56] and reducing tau protein hyperphosphorylation [57]. Earlier age at menopause was associated with a faster decline in global cognition along with an increase in AD neuropathology, in particular, neuritic plaques [58]. Alongside the association between estrogen deficiency in women and a higher risk of AD, reduced testosterone levels may also play a role in an increased risk of AD in men. Lower androgen levels were associated with an increase in Aβ suggesting that subclinical androgen deficiency enhances the expression of AD-related peptides in vivo. Significant inverse relationships between brain testosterone levels and brain soluble Aβ were discovered in men experiencing memory loss [59] as well as in patients with prostate cancer treated with androgen deprivation therapy [37] leading to a consequential increase risk of AD.
ApoE is crucial for transporting phospholipids and cholesterol through receptor-mediated interactions at cell surfaces [60]. There are three variants: APOE2, APOE3, and APOE4 [18] with APOE4 being the strongest genetic risk factor for AD [61] whereas APOE2 can be neuroprotective [62]. APOE4 increases Aβ-aggregation and impairs clearance of the amyloid relative to other APOE isoforms [60] with one animal study demonstrating APOE4 exacerbating tau-mediated neurodegeneration [63]. Carrying one copy of APOE4 increases the risk of AD by 3-4 fold while carrying two copies has a 10–15 fold increase [64, 65]. The results of a study have shown that men and women possessing the APOE E3/E4 genotype exhibit the same odds of developing AD between the ages of 55 and 85 years, but women have an increased risk at younger ages. Women with the APOE E3/E4 genotype have an increased risk of MCI between ages 55–70 and AD between ages 65–75 [66]. The APOE4 allele is also linked to significant cognitive decline in women aged 70–80 [67], and higher risk for neurofibrillary and amyloid plaque neuropathology, potentially due to waning estrogen levels [68]. ApoE expression is regulated by estrogen, progesterone, and testosterone, indicating sex-specific roles in late-onset AD pathogenesis [69]. Estrogen upregulates the synthesis and expression of ApoE in the brain [70]. Estrogen replacement therapy (ERT) shows that APOE4 women experience more cognitive decline with ERT than APOE4 females without ERT, while APOE2 and APOE3 women show cognitive improvement [18, 71]. An explanation for this is the stimulation of estrogen receptors alpha and beta (ERα and ERβ), in which ERα upregulates ApoE protein expression while ERβ downregulates APOE gene expression and protein levels [72]. Therefore, it is possible for APOE4 carriers receiving ERT to be subjected to overexpression of APOE4 from ERα stimulation by estrogen while in contrast APOE2 and APOE3 carriers receiving the same treatment may benefit from the neuroprotective APOE2/3 overexpression [72, 159].
Neuroinflammation represents a significant risk factor for the development of AD, defined by gliosis, the proliferation and activation of microglia and astrocytes and the subsequent production of inflammatory factors [73]. Genome-wide association studies (GWAS) identified polymorphisms of genes involved in immune responses, and the expression of these was enriched in microglia and macrophages [74, 75]. Microglia, primary immune cells in the central nervous system, play an important role in immune surveillance responsible for the clearing of protein aggregates such as Aβ. Age-dependent and senescence-driven impairments of microglia functions and responses have a pivotal role in the onset and progression of AD [76]. In AD, activated microglia in proximity to Aβ-plaques generated higher levels of pro-inflammatory cytokines and accelerated Aβ accumulation [77]. Sex differences exist in the neuroimmune system in the number and activation states of microglia, in the activation of astrocytes, and cytokine release and function [78].
Adaptive and innate immune responses also differ qualitatively between sexes with different patterns of antibodies and cytokines produced between the genders [79]. Sex hormones contribute to sex differences in immune activation in which circulating estrogens act to increase immune function in both female and male mice [80, 81]. In contrast, testosterone suppresses immune function in both sexes [82]. In one study, it was discovered that females were more efficient in the mechanisms that regulate leukocyte function as rapid detection and elimination of pathogens had increased the threshold for pathogen-induced tissue injury in females [83]. Another study carried out a subchronic, systemic immune challenge to demonstrate sex-specific patterns of memory deficits. The results showed that both males and females were susceptible to impairments in memory after the immune challenge, but females are more vulnerable to early-onset memory deficits, on the other hand, males tend to be more prone to later development of impairments across multiple memory systems. However, these memory deficits persist and are not associated with markers of neuroimmune activation [84].
The dysregulation of microglia and astrocyte-mediated neuro-immune response has been strongly implicated in AD [85]. In conclusion, the maintenance of homeostatic microglial function may be important in early AD and research has highlighted the importance of identifying sex-specific cellular and signaling mechanisms in neuroimmune activation.
The vascular system plays a vital role in the progression of AD and the system significantly differs between men and women. Cerebrovascular alterations are a major cause of dementia [86] and strong evidence links midlife hypertension and diabetes to both vascular dementia and AD. Alterations in neurovascular function play a key role in both the pathobiology of vascular cognitive impairment and AD and the neurovascular unit is a major target of vascular risk factors promoting vascular cognitive impairment, AD and Aβ [87–89]. Vascular abnormalities are detected in at least 50% of AD cases and are becoming more prevalent with increasing age of diagnosis [90]. The vascular hypothesis emerged as an alternative to the amyloid hypothesis as an explanation for the pathophysiology of AD where the model hypothesizes that vascular damage, such as blood-brain barrier (BBB) disruption impairs Aβ clearance and is followed by accumulation of Aβ in the brain to vasculotoxic and neurotoxic levels [88, 91]. Besides impairment of the BBB, other factors such as decreased cerebral blood flow, and the establishment of inflammation would be responsible for subsequent neuronal damage as these factors promote aggregation of Aβ in the brain [92, 93]. The BBB breakdown is an early biomarker of human cognitive dysfunction [94] and the APOE4 gene has been shown to accelerate BBB breakdown and degeneration of brain capillary pericytes [95].
There are emerging sex differences in vascular risk factors for AD. There is a higher prevalence of coronary artery disease (CAD) in males than in females for all ages [96] however women with CAD have worse outcomes than their male counterparts [97]. The lower incidence of CAD in women may be due to the protective effects of estrogen through vasodilation and the protective effects against inflammation, atherosclerotic plaques and oxidative stress [98]. There is a strong association between CAD and cognitive decline [99] and hippocampal damage [100].
Proposed explanations to explain the sex differences in dementia incidence have often emphasized the influence of sex hormones, with little consideration paid to date to the potential impact of hormonal contraception on brain health. Worldwide, over 60% of women of reproductive age use contraceptives, with the majority opting for hormonal methods [101]. In a study of UK biobank participants, the study observed the use of oral contraceptives (OCs) was linked to a reduced risk of dementia, with no evidence of any association between the age at which OCs were first used and the risk of dementia [102]. A study conducted among women from the Singaporean Chinese population found that in contrast to individuals who have never used OCs, women with short-term use (≤5 years) were found to have a diminished risk of dementia compared to those who have never used OCs. However, this association was not observed in those with more than 5 years of use [103]. A study utilizing data from the South Korean National Health Insurance System database revealed that the use of OC was significantly associated with approximately 10% lower risk of dementia compared to individuals who had never used OCs, with no differences observed between those who had used OCs for less than or more than a year [104]. Other studies found no significant link between history of OC use and risk of AD diagnosis [105]. Similarly, in another study, there was no significant association between OC usage and subjective memory complaint cases [106]. This indicates that the evidence regarding the relationship between OC use and AD diagnosis is inconsistent. Patel et al. (2022) [107] performed a study on 251 female undergraduates separated into groups of high endogenous estradiol levels, low endogenous estradiol levels, and exogenous synthetic estradiol in the form of OCs. The authors concluded that low endogenous estradiol levels negatively impacted spatial reference memory (in Virtual Morris Water Task) compared to high endogenous estradiol levels and exogenous synthetic estradiol levels [107]. However, estradiol did not affect the spatial tasks of Virtual Radial Arm Maze and Mental Rotation Task. Therefore, this suggests that estradiol plays a role in more complex spatial memory tasks [107]. The women in the exogenous estradiol group performed similarly to the women with high endogenous estradiol levels in most cases and had no significant behavioral impairments [107]. In summary, some studies have found a positive association between OCs and brain health, indicating modest yet expanding evidence supporting potential benefits for women’s health [108] but other studies did not find any effect on cognitive performance [107]. Importantly, these studies assess different outcomes such as dementia risk or cognitive performance tested by different tools and examining different aspects of memory andcognition.
Parity and childbirth uniquely impact women and are associated with changes in hormone levels, health conditions, and lifestyle that influence the risk of dementia. In a study examining cohorts from 11 countries over 3 continents, it was observed that across all cohorts, grand multiparous (5 or more childbirths) women had a 47% greater risk of dementia in comparison to primiparous (1 childbirth) women. Furthermore, nulliparous (no children) women and women with 2 to 4 childbirths showed a comparable dementia risk to primiparous women. The study concluded that parity was associated with women’s risk of dementia [109]. Another study revealed that grand multiparous women who have had≥5 completed pregnancies demonstrated roughly a 1.7-fold higher risk of AD compared to those with 1 to 4 completed pregnancies. Conversely, those with incomplete pregnancies have approximately half the level of AD risk compared to those who have never experienced an incomplete pregnancy. Similarly, the study concluded that grand multiparity had an association with a higher risk of AD, while incomplete pregnancies were associated with a low risk of AD in late-life [110]. The biological processes of pregnancy may contribute to an increased risk of AD in women who have their first child at very young (<20 years) or relatively old (≥40 years) ages [111]. Zhang and colleagues carried out a study to determine the differences between genders in the associations between parity and cognitive function. Data were taken from the UK Biobank and comprised of 502,505 people aged between 37 and 74 between 2006 and 2010 [112]. Only participants of European ancestry were used, to control for genetic differences. Without adjustments, a positive association between parity and cognitive performance was found in men, however, parity had a negative effect on cognition in women [112]. When the data was adjusted for education, the association between parity and cognition strengthened in men, and depending on the domain, strengthened or reduced it in women [112]. Additionally, there is an increased risk of dementia in women < 25 years of age at first delivery [102]. However, the findings suggest that risk variation in women might not solely be associated with factors related to childbirth because a similar U-shaped pattern in dementia risk was also observed among men concerning the number of children they fathered. The similar association noticed between the number of children and dementia risk between men and women might suggest that the risk is not related to hormonal differences [102]. The association between parity and a woman’s risk of dementia may also vary depending on geographical differences. In comparison to women with 1 to 4 childbirths, grand multiparous (5 or more childbirths) women exhibited a higher risk of dementia in both European and Latin American cohorts, whereas nulliparous women were found to have a higher risk of dementia in Asian cohorts [109].
Socio-economic risk factors can account for AD prevalence. Around a third of AD cases worldwide may be attributed to modifiable risk factors and AD incidence may be reduced through improved access to education, reducing the prevalence of vascular risk factors and also linked to depression [113]. The risk of dementia may vary based on socioeconomic status, indicated by differences in factors such as education, income, wealth, or occupational status. Women were more likely than men to develop incident dementia, be older, have a lower socioeconomic status in adulthood, and more often experience medical conditions such as hypercholesterolemia, obesity, high alcohol consumption, physical inactivity, and depression. Additionally, women tend to have lower levels of education, social contact, and cognitive activity. In contrast, men were more likely to have hypertension, diabetes, hearing impairment, and an unhealthy diet compared to women [114]. Education has a protective effect against the risk of developing clinical AD in both men and women with the male gender being protective which may be due to a higher educational attainment [115]. In cohort studies carried out in the UK, findings suggested a reduction in educational disparities between the sexes, due to secular increases in educational opportunities, which could help diminish the differences in dementia risk and cognitive decline in the future [116]. Maitreyee et al. (2023) [117] performed a cross-sectional study to examine the relationships between age, cognition, reproductive factors and word-finding abilities. 53 healthy postmenopausal women aged between 48 and 79 were given a questionnaire on their demographics and reproductive history [117]. They then completed a battery of cognitive tasks, related to verbal fluency, continuous series naming accuracy and latency. The study found that women who spent more time in education performed better in category and letter fluency, continuous series switch rates, picture and auditory naming accuracy, and faster picture naming latencies [117]. Later menarche was associated with lower word generation on category fluency and shorter picture and auditory naming latencies. A longer reproductive period was also associated with better category fluency, picture and auditory naming accuracy, and shorter picture latency [117]. The study concluded that age plays a significant role in working memory, and less so in verbal fluency. The number of years spent in education is associated with word-finding, while reproductive factors have only a subtle effect on naming ability [117].
Depression, which is twice as likely to be diagnosed in women, is another significant risk factor [118]. A recurring theme from clinical observations is that the period between puberty and menopause is marked by higher rates of depression and certain anxiety disorders in women. An important observation is that puberty, the menstrual cycle, pregnancy, and menopause can trigger the onset, recurrence, and worsening of affective mood and anxiety disorders. However, the brain systems, biological mechanisms, and physiological factors that mediate the psychiatric effects of these reproductive events are not well understood [119]. Studies on sex differences in the link between depression and AD are inconsistent with some studies showing men with depression are at greater risk [120], while others show higher risk for women [121]. As depression is more prevalent in women, a diagnosis of depression may have a greater overall impact on the risk of AD dementia among women.
Both previous and active smoking is associated with a significantly increased risk for AD [122]. There is little evidence about the impact of smoking on both the efficacy and side effects of HRT. However, smoking can reduce or completely cancel the efficacy of orally administered estrogens [123] with smokers requiring higher dosages of HRT to achieve comparable clinical effects to that observed in non-smokers. Women who smoke heavily are recommended to cease smoking to be effectively treated with the lowest dose of HRT [124]. Compared to women who never smoked, current smokers and former smokers showed an increased risk of early menopause. This elevated risk was particularly notable among women who reported smoking for 11–15 pack-years, 16–20 pack-years, and more than 20 pack-years. However, women who smoked 10 or fewer cigarettes per day but quit by age 25 had a risk comparable to that of those who never smoked [125]. Infrequent or moderate alcohol usage may be protective, while high levels elevate dementia risk, with alcohol use disorder linked to early-onset dementia [126]. Alcohol consumption was positively associated with endogenous estrogen levels [127] suggesting that low alcohol intake may be protective [128]. These studies suggest that smoking and alcohol consumption need to be considered when examining the efficacy and side effects of HRT.
Research on sex and gender differences in the field of AD is still in its early stages. Understanding sex differences in AD risk is crucial for developing effective prevention strategies, given that there are currently no effective treatments for AD. A deeper understanding of these differences can result in better care and treatment for both men and women. It is suggested that we must move beyond the perception that only women are at greatest risk and that AD dementia is simply a “women’s disease”, and instead prioritize the study of sex differences [129].
HORMONE REPLACEMENT THERAPY HISTORY AND CURRENT USE
Despite forms of HRT being available from the end of the 19th century and the discovery of estrogen in the 1920 s, it was not until the 1960 s and 1970 s that estrogen became commonly used, with it becoming the 5th commonly prescribed medication in the US by the mid-1970 s. Usage then plummeted when an association was reported between the use of unopposed estrogen and endometrial cancer. However, its use rose again from the mid-80 s due to the addition of progestin. This was thought to reverse endometrial hypertrophy linked to endometrial cancer [130]. Additionally, the dosage of estrogen was reduced to further decrease the risk of developing endometrial cancer [131].
In 1998, the Women’s Health Initiative, a study of over 27,000 women was commenced, after having recruited women since 1993. It included women with and without uteri. The purpose of this trial was to determine the effects of HRT on different diseases such as invasive breast cancer and cardiovascular disease [132]. The first results were released in 2002 and showed that a combination of conjugated equine estrogens (CEEs) and medroxyprogesterone acetate (MPA) in women with uteri increased the risk of developing coronary heart disease and breast cancer while decreasing the risk of osteoporosis and colorectal cancer [131]. The risk of developing other diseases including stroke, pulmonary embolism, and myocardial infarction also increased. [130]. The trial was discontinued for women with uteri but continued for those without. More results were published in 2004 which showed that women, who had undergone hysterectomies and were taking only estrogen, were at risk of ischemic stroke. The WHI trials were then completely terminated, due to the conclusion that the risks outweighed the benefits [131]. Following this, estrogen use, in combination with progestin and without, dropped 22% and 45% respectively.
Since the release of these results, questions have been raised over the validity of these studies as the average age of participants was 63 years old, more than a decade older than the average age of onset of menopause [132]. Trials have been undertaken since WHI, with Kronos Early Estrogen Prevention Study (KEEPS) being one of the most significant studies [132]. The results of KEEPS demonstrated that HRT does not affect atherosclerosis or blood pressure, increasing high-density lipoprotein, and decreasing low-density lipoprotein. No significant differences were also found in relation to breast cancer or stroke. However, HRT increased triglyceride levels [132]. A sub-study of KEEPS called KEEPS-Cognitive and Affective Study (KEEPS-Cog) was run to further determine the effects of HRT on the relationship between blood pressure and cognition. 662 menopausal women aged between 42 and 59 were participants. The study found that estrogen, progesterone or testosterone did not affect the relationship between blood pressure and cognition [133]. A separate clinical trial, Early versus Late Intervention Trial with estradiol (ELITE), was run to test the ‘critical window’ hypothesis, which states that estrogen has protective effects when it is taken during menopause or shortly thereafter [17, 134]. ELITE concluded that younger women (<60) and those who began HRT within 10 years of menopause had a lower risk of developing coronary heart disease and had lower total mortality than women who started HRT greater than 10 years after menopause [134]. Cognition was not considered in ELITE, however, important to explore the ‘critical window’ hypothesis of HRT concerning cognitive decline. Nonetheless, the WHI study has had a lasting impact on today’s world, with many clinicians, either not prescribing HRT, or being reluctant to. This seems to be due to a lack of recognition of menopausal symptoms having consequences on menopausal women’s quality of life, despite HRT being the most effective treatment for many menopausal symptoms [130, 132].
The British Menopause Society currently recommends a “holistic and individualised approach in assessing menopausal women”, including focusing on lifestyle and diet. HRT should then be carefully considered, with regard to dosage, duration, benefits and risks, all of which should be discussed with the patient. If decided to take HRT, the patient should also have yearly evaluations to review the regimen previously agreed upon and whether it should be continued as is, altered or ended [135] The BMS also recommends that HRT should be prescribed before 60 years of age or within 10 years of menopause, as it is associated with a reduction in cardiovascular mortality. However, women older than 60 may still be prescribed HRT, but it is recommended they start on lower doses and should be administered transdermal patches. Transdermal patches should also be used in women who have risk factors as they are unlikely to cause an increase in stroke and venous thrombosis risk. Women who have premature ovarian insufficiency or premature menopause should be encouraged to take HRT, until at least 51 years old (average age of menopause onset) [135].
HORMONE REPLACEMENT THERAPY CLINICAL TRIALS
In this section, clinical trials are ordered based on the results of the trials. The trials which found an increased risk of AD from HRT are discussed first. Then clinical trials with mixed results or no associations between AD and HRT are presented. Finally, trials which found a decreased risk of AD after HRT usage are then discussed.
A retrospective cohort study, based in South Korea, was carried out from 2002 to 2019 with almost 1.4 million participants. The participants were divided into a Menopausal Hormone Therapy (MHT) group and a non-MHT group and the risk of AD and non-AD dementia was compared [136]. The MHT group were women who were taking Tibolone, estrogen, combined estrogen plus progestin by the manufacturer (CEPM), combined estrogen plus progestin by the physician (CEPP) or transdermal estrogen while they were menopausal [136]. A higher risk of AD, and other forms of dementia, was associated with Tibolone and estrogen, whereas there was no associated risk with CEPM or the transdermal estrogen. For AD, the risk ranged from 4.1% (Tibolone) to 8.1% (Estrogen). A risk of dementia was also associated with later menarche, later onset of menopause, smoking and regardless of MHT, the usage of MHT from 60 years [136].
In a systematic review by Wong et al. [13], 24 randomized control trials (RCTs), cohort studies and case-control studies were analyzed. The aim of these studies differed from preventing AD, to preventing and delaying the onset of AD, or to reducing the risk of AD. These studies were completed between 1994 and 2021 and ranged in sample size from 280 to 4,696,633 [13]. The participants of these studies were primarily women of at least 50–60 years of age and were peri- or postmenopausal. Individual studies had other criteria, such as excluding people who had existing psychiatric illnesses or dementia, or those who had had oophorectomies, hysterectomies, or strokes. Interventions also varied between studies from CEE to estrogen, estradiol, or combined therapy [13]. Of these 24 studies, 15 showed “positive associations for estrogen-only therapy”, while there was no association between estrogen therapy and a reduction in AD found in the other 9 studies. Two of these 9 studies (both RCTs) showed an increased risk if estrogen was combined with progestin, with one of these also showing an increased risk if estrogen was used alone. Of the 15, the evidence of association ranged from a reduction of 2% to a reduction of 96% [13].
Nerattini et al. [15] completed an analysis of 6 RCT reports, from 4 RCTS, and 45 observational reports, consisting of 24 case-control studies, 20 prospective cohort studies and 1 cross-sectional study. The RCTs focused on dementia rather than AD. Nevertheless, it found an increased risk of dementia, from 20% to 125%, in postmenopausal women over 65 with the use of combined therapy of CEE and medroxyprogesterone acetate, when compared with a placebo [15]. No statistically significant risk was associated between oral CEE therapy and dementia. 27 of the observational studies were analyzed for an association between HRT and AD. When a common effect model was applied, no statistically significant results were found [15]. However, when a random effects model was applied, there was an overall decrease in risk association of AD, by 22%. When these same models were applied to studies for associated risk in all-cause dementia, there were no statistically significant results and a decrease in risk association by 19% respectively [15].
Chiu et al. [137] also carried out a retrospective analysis on 787 participants, aged over 50, to determine whether cholesterol levels and HRT played a role in developing or not developing dementia over a 6-year period. Before adjusting for certain variables, it was established that “older age, lower education, lower cognitive performance” among other variables increased the risk of developing dementia, and “regular exercise, a history of hyperlipidemia” decreased the risk [137]. Of the 787 women, 539 did not develop dementia, while 248 did. Of the 539, 68 had been treated with HRT and of the 248, 28 had been treated with HRT. From this, it was concluded that the development of dementia was not impacted by HRT. Chiu et al. [137], however, did note that the evidence was still inconclusive “as not all studies support this finding”. Since the study was also completed in Taiwan, cultural and genetic roles could have had an impact on the results [137]. Furthermore, the types of medications and doses were not analyzed, which may also play a role in the development of dementia [137].
A study completed in Denmark took 5,589 cases of dementia in women (of which 1458 (26.1%) were AD) and 55,890 dementia-free case controls between 2000 and 2018 inclusive [138]. The women were aged 50–60 on 1 January 2000 and had not had a hysterectomy. The study found that women were more likely to develop dementia if they had a shorter education, a lower household income, lived alone or had hypertension, diabetes or thyroid disease. The median age at diagnosis was 70 years old [138]. 1,782 cases (31.9%) and 16,154 controls (28.9%) had taken combined HRT with estrogen and progestin. Most of the women also took an oral administration of HRT. The median age at initiation was 53 in both groups [138]. It was found that the use of HRT increased the overall risk of dementia by 24%, with late-onset and AD at an increased risk of 21% and 22% respectively. A use of 12 years or longer increased the risk of dementia by 74% [138]. When the type of HRT was reviewed, it was found that continuous estrogen-progestin increased the risk of dementia by 31% and cyclic estrogen-progestin increased the risk by 24%, with a use of more than 8 years increasing the risk by 99% and 59% respectively [138]. When age was focused on, it was determined that if estrogen-progestin therapy was initiated between 45 and 50, the risk of dementia increased by 26%, whereas when it was initiated between 51 and 60 the risk was increased by 21%. Associations for progestin-only therapy did not reach statistical significance [138].
Steventon et al. [139] published a study in 2023 on HRT and menopausal factors predicting the volume of the medial temporal lobe, the atrophy of which has been identified as correlating with AD risk and severity. Data on 10,924 women were collected. The women were aged between 47 and 81 [139]. The duration of HRT use was predictive of parahippocampal gyri grey matter, with a longer duration being associated with a larger volume. However, it was not predictive of grey matter volume in other regions [139]. Menopausal age was found to be predictive of grey matter volume in the hippocampus, parahipppocampal gyri, perirhinal cortex, and amygdala. Earlier ages of menopause onset were associated with a lower volume of grey matter in these regions [139]. Reproductive span was also used to predict the volume of grey matter, with a longer timeframe being associated with a larger volume in the same regions associated with menopausal age [139]. The age at HRT initiation and length of time since HRT use were not predictive of grey matter volume anywhere. The study concluded that HRT use did not have a detrimental effect on the brain in later life dementia but that age at menopause onset and reproductive span had a “small but significant effect” [139].
Brown et al. [140] completed a study in 2023 on 72 women. Four groups were created for the participants; women with bilateral salpingo-oophorectomy with no HRT usage, women with bilateral salpingo-oophorectomy with HRT usage, a control group of premenopausal women with ovaries (age-matched to women with bilateral salpingo-oophorectomy) and women in spontaneous menopause without HRT usage [140]. The mean age of the participants was 47 and the mean age at menopause was 44. A memory test was given to the participants, and it was determined that the control group of premenopausal women performed significantly better than women in spontaneous menopause [140]. There was no significant difference between the groups of women who had had a bilateral salpingo-oophorectomy. The brain activity of the groups was then analyzed and it was found that women who had undergone a bilateral salpingo-oophorectomy had a similar level of brain activity to women who had undergone spontaneous menopause, despite being 10 years younger on average [140]. They also found that a trend for functional connectivity differences existed within hippocampal circuits. This shows that the type of menopause undergone may impact memory. The women who had undergone a bilateral salpingo-oophorectomy and did not take HRT showed decreased hippocampal activity but in the group who did take HRT, a level of hippocampal activity similar to a group of mixed-sex younger adults, suggesting that HRT may delay or prevent these changes [140].
A study published in 2024 by Lee et al. analyzed 2,458 women and factors such as reproductive window, parity and HRT use to determine estrogenic effects on cognition in later life. Women were included in the study if they were over 50 years of age in 2012 and were excluded if they were in hospice or if the age at menopause was unknown [141]. The average age of the women was 74.2, the average menarche age was 13 and the average age at menopause was 49. 57% of the women had also used HRT. It was seen that women who had more pregnancies (particularly 4–5+) which reached 20 weeks had a greater decline in global cognition [141]. Women who used hormonal contraception had less decline in global cognition, compared to those who did not, while women who used HRT had a greater decline in cognition, memory and language. The timing of HRT initiation was seen to be important, as women who started HRT within one year of menopause experienced less cognitive decline when compared to women who did not use HRT [141]. However, women who began using HRT 5 years after menopause had an increased decline. The duration of HRT usage was also analyzed, with women, who used HRT for more than 5 years, having a greater risk of MCI, in comparison to women who never used HRT [141].
Vinogradova et al. carried out two nested case-control studies assessing HRT and its link to dementia, based on the type and duration of the HRT, obtaining the data from QResearch and the Clinical Practice Research Datalink [142]. Women who were over 55 and registered between 1 January 1998 and 31 July 2020 were included but were excluded if they had dementia or dementia-related prescriptions. 118,501 cases were used and were matched to 497,416 controls. Before the data was adjusted HRT was seen to increase the risk of developing dementia [142]. Once adjusted, however, no statistically significant associations between estrogen-only or estrogen-progesterone HRT use and dementia were found and were independent of HRT use duration, and consistent for all hormone types. When the women were divided into two groups by age (<80 and≥80), it was found that women in the younger group had a 15% decreased risk of developing dementia when exposed to at least 10 years of estrogen-only HRT [142]. Women in the older group were found to have a 12% decreased risk of developing dementia when exposed to estrogen-progesterone HRT for between 1 and 3 years. Estrogen-only HRT was found to increase the risk of AD by 11%, however, only when it was used for less than one year [142]. When taken for longer, there was no associated risk. Estrogen-progesterone HRT increased the risk of developing AD by 11% when taken for between 5 and 9 years, and 19% when taken for 10 years or more [142].
A study was completed by Kling et al. (2023) [143] to evaluate pituitary-ovarian hormone levels and their associations with cognition and hormone therapy. 362 women who were enrolled in KEEPS and were divided into groups by treatment: 146 women were given a placebo, 109 were given 0.45 mg of oral CEEs daily, and 107 were given 50μg/day t-E2 weekly [143]. All groups were subject to cognitive testing over 48 months. Age, time since menopause onset, race and ethnicity and level of education did not differ between groups [143]. The changes in cognition were non-significant, even when controlling for hormone levels at baseline and 48 months. Higher levels of estrone at baseline were significantly associated with poorer visual attention, executive function, auditory attention and working memory. Therefore, this study suggests that hormone therapy does not play a role in cognitive decline, but that endogenous hormones do [143].
Chen et al. (2022) [144] performed a systematic review with meta-analysis of 10 studies and 2,818 participants, regarding the effects of MHT on memory in postmenopausal women. The duration of the studies ranged from 10 weeks to 3 years and took place from 1992 to 2011 [144]. They performed a pooled analysis of 6 trials, which showed no significant differences between MHT and placebo in immediate and delayed recall of logical memory [144]. A second analysis showed no significant differences in memory between women who were within 5 years of menopause and women more than 5 years postmenopause. Subgroups of estrogen-progestin combination and estrogen monotherapy were then analyzed which showed that they did not differ in delayed recall of logical memory when stratified by time from menopause [144].
Another systematic review by Andy et al. (2024) [145] also analyzed the effects MHT had on cognition. 34 randomized control trials with 27,953 participants (14,914 treated participants, 12,679 placebo participants) were examined. Overall, MHT was seen to have no significant effects on any of the cognitive domains studied [145]. However, MHT in women over 65 was shown to mildly reduce global cognition. When the individual cognitive tests were analyzed, it was found that MHT had no significant effects in midlife. In women over 65, MHT was associated with a reduction in Trail Making Test Part B [145]. In women who had undergone surgical menopause, it was found that estrogen-only therapy improved global cognition. Estrogen-only treatment in women under 65 and estrogen-progesterone treatment in women over 65 were also associated with increased verbal memory. Therefore, this systematic review concluded that MHT effects are dependent on the timing at which it is given, with changes seen depending on the formulation of the MHT [145].
Mills et al. (2023) [24] reviewed 66 observational and clinical studies completed internationally, to try to find a relationship between HRT use and AD. The studies were completed from 1988 to 2022 [24]. The aims of the studies varied with many aiming to find a link between HRT use and AD diagnosis. Other studies used MCI or dementia diagnosis, while others used performances in different cognitive tests, such as Mini-Mental State Examination, and how HRT affected these results for their evaluation [24]. Of the 66 studies, 16 (24.2%) showed no association between HRT and AD, 8 (12.1%) showed a positive association, 26 (39.4%) showed a negative association, and the remaining 16 (24.2%) showed mixed results. The mixed results varied from study to study, with some depending on age at menopause, age at HRT initiation and type of HRT used [24].
One of these observational studies was carried out by Savolainen-Peltonen et al. (2019) [146]. Two control groups were used, one with HRT (25,564 participants) and one without (59,175), and two AD groups were used, one with HRT (26,553 participants) and one without (58,186 participants) [146]. The participants were all over 50 years of age and postmenopausal. Unopposed, opposed and Tibolone were used orally, vaginally and transdermally, and for varying lengths of time from less than 3 years to more than 10 years [146]. The main findings were that long-term use of HRT of greater than 10 years was associated with an increased risk of AD, regardless of whether the HRT was opposed or unopposed. However, vaginal use of HRT did not show this risk [146].
Another observational study by Kim et al. (2022) [147] with over 200,000 postmenopausal participants in two groups (dementia positive and dementia negative). The HRT type, dose and route of administration were not reviewed [147]. The length of duration of HRT use was divided into 3 groups: less than 2 years, 2–5 years, and greater than 5 years. This study concluded that HRT in depressed postmenopausal women decreased the risk of both AD and vascular dementia. It also concluded that a decreased association was found between AD and a lifetime use of oral contraceptives [147].
A third observational study by Yoo et al. (2020) [104] was also reviewed. This study followed four groups of people totaling 4,524,128 people; one with those who did not use HRT and did not develop AD, another with those who used HRT who did not develop AD, one with people who did not use HRT and developed AD and a final group of people who used HRT and developed AD [104]. The type, dosage and route of administration of HRT were not reviewed. The duration of HRT use was a mean duration of 5.74 years [104]. It was found that the risk of dementia was increased in those with later menarche and decreased in those with older menopausal age, showing an association between lifetime endogenous estrogen exposure and AD or dementia development. HRT also decreased the risk of dementia [104].
One of the clinical studies by Shumaker et al. [148]. Four groups were designed, a placebo group, a placebo group without MPA, an HRT group and an HRT group with MPA. 6.35 mg/day of CEE (±2.5 mg/day MPA) was used as the HRT type and it was given orally to postmenopausal women between the ages of 65 and 79 [148]. The opposed HRT was given for 7 years while the unopposed was given for 9 years. This study concluded that unopposed HRT did not decrease the incidence of dementia or MCI. However, due to pooling data, some results did show an increased risk of dementia and MCI [148].
Kang and Grodstein (2012) [20] examined non-HRT users, past HRT users, current unopposed HRT users and current opposed HRT users, who were postmenopausal and between 70 and 81 years of age, screened using Telephone Interviews for Cognitive Status [20]. While the HRT type, dosage and route of administration were not reviewed, the study still showed a worse rate of decline in the past and current users when compared to the never-users. Even when early timing of HRT initiation was taken into account, no protective associations were determined [20].
In a clinical study by Song et al. [103] individuals were divided depending on HRT use and MCI development. Unopposed and opposed HRT were used and given to postmenopausal women between 45 and 74 (mean of 53.4±6.4) [103]. The dose, route of administration, and duration of use were not reviewed. The authors concluded that there was an associated risk between MCI and HRT use when compared to those who did not use HRT [103].
Several studies reviewed by Mills et al. [24] showed no relationship between HRT and AD. In 2002 an observational study by Lindsay et al. [149] was completed. Four groups of participants (control without use of HRT, control with use of HRT, AD without use of HRT, and AD with use of HRT) were created to try to identify any association, if any, between HRT and AD [149]. The 433 female participants in this study were at least 65 years of age and were all postmenopausal. The type of HRT, dosage and route of administration were not reviewed. The study concluded that HRT use was neither a protective nor adverse factor for AD development [149].
Imtiaz et al. also performed an observational study in 2017 [150]. They used opposed and unopposed HRT and administered it orally and transdermally. The dosage was not considered [150]. The 8,195 women were between the ages of 47 and 56 and were a mix of premenopausal, menopausal, and postmenopausal. The use of HRT lasted from under one year to more than 10 years, with a follow up after 20 years. The study found that there was no association between HRT use and AD [150].
A clinical study in 2007 by LeBlanc et al. divided 32 women into two groups of participants, a control group and a group using HRT [151]. This study administered 2 mg of oral 17-β Estradiol daily for 8 weeks [151]. The women were all postmenopausal and given cognitive tests. The study found that there was no difference in cognitive improvement between the HRT group and control group [151].
Maki et al. also ran a study in 2007 with 158 women [152]. One group was given a placebo, while the other group was given HRT. The HRT was administered orally and consisted of 0.625 mg of CEE and 2.5 mg of MPA daily for four months [152]. The participants were between 45 and 55 and were all postmenopausal. A number of cognitive tests were completed, and the study concluded that there were no differences between the groups. Some negative effects on memory were noticed; however, they were not significant [152].
A cohort study performed by Needham et al. (2023) [153] analyzed data from the Medical Research Council National Survey of Health and Development concerning 2,547 women. 1,572 of these women completed a questionnaire annually from the ages of 43 to 54 and, of these, 1,378 had available data regarding menopause [153]. From this data, it was concluded that a later age at menopause had a small positive effect on cognition, particularly in visual processing, associative learning and memory, compared to a younger age at menopause. However, when adjustments were made for reproductive and health-related factors, none of these associations were significant [153].
Park et al. (2024) [154] carried out a study to determine the effects of lifelong exposure to estrogen on the risk of developing dementia. They analyzed data on 273,260 women from the UK Biobank [154]. The data used included age at menarche, age at menopause, reproductive surgeries, parity, age at first birth and HRT usage. Estrogen exposure was found to have an inverse association with dementia, with women who had more estrogen exposure less likely to develop dementia. Factors which were associated with a decreased risk of dementia include later menopause, earlier menarche, fewer than or equal to 3 live births and later age at first birth [154]. Factors seen to be associated with an increased risk of dementia include earlier menopause, later menarche, more than 3 live births and hysterectomy. The study concluded that estrogen has a protective effect against the development of dementia [154].
Branigan et al. ran a study in 2023 [155], looking at women who had had breast cancer and used estrogen-modulating therapies (EMTs), to discern whether or not EMTs are a risk factor for neurological degenerative diseases (NDDs). Included in their definition of NDDs are AD, non-AD dementia, multiple sclerosis, Parkinson’s disease, and amyotrophic lateral sclerosis. Of 725,160 women in the DrugBank database, data on 260,232 women were used in the study [155]. The 260,232 were separated into four groups: without EMT exposure and an NDD diagnosis (4,355), without EMT exposure and without an NDD diagnosis (125,761), with EMT exposure and an NDD diagnosis (3,700) and with EMT exposure and without an NDD diagnosis (126,416). On average the EMT was initiated after 160 days post-diagnosis of breast cancer and was given for 1,210 days [155]. The EMTs used were Selective Estrogen Receptor Modulators (Tamoxifen and Raloxifene), Steroidal Aromatase Inhibitors (Exemestane), and Non-Steroidal Aromatase Inhibitors (Anastrozole/Letrozole). A high level of adherence was observed, ranging from between 89.2% (Raloxifene) to 94.2% (Steroidal Aromatase Inhibitors). Overall EMT exposure was associated with a 15% decrease in risk of NDDs [155]. Tamoxifen was associated with a 56% decreased risk of NDDs and both types of aromatase inhibitors were associated with a 17% decrease in risk of NDDs. However, Raloxifene was seen to have an 18% increased risk of NDDs. They also used SWISS-ADME database to predict whether these drugs would cross the BBB, and they concluded that all the EMTs and estradiol, apart from Raloxifene, can cross the BBB [155]. The authors then modelled interactions between EMTs and brains in Sprague-Dawley rats, and it was determined that the EMTs, apart from Raloxifene, do cross the BBB. E18 rat hippocampal neurons were then isolated, cultured, and treated with EMTs [155]. Significant increases in neuron volume, area, number of branches, and branching pattern complexity were observed. These morphological changes were seen to be comparable to changes caused by estradiol. The study concluded that EMTs act as partial estrogen agonists in neuronal tissue which reduces the risk of AD [155].
The outcomes of clinical trials vary widely, with many studies supporting the use of HRT to prevent AD, while others support the finding that HRT is a factor in AD development. This may be due to the design of the study, from the dosage, duration and type of HRT used to factoring in endogenous estrogen, and reproductive span. It is therefore not possible to give a conclusive answer, based on the current information available, as to whether HRT is a protective or risk factor.
DISCUSSION
We discussed several factors that can impact the outcome of HRT and could potentially lead to controversial findings between studies. Intrinsic factors, such as genetic predisposition due to the inheritance of AD-associated genes, could play a role in HRT outcome. Therefore, the prevalence of genetic biomarkers of AD in study populations of clinical and epidemiological HRT trials needs to be considered [61]. Other factors may include reproductive factors, testosterone or lifestyle factors, namely depression, smoking and alcohol consumption [59, 128].
Two recent longitudinal studies by Oveisgharan et al. [158] followed 1,711 cognitively normal women over an average of 10 years and investigated G protein-coupled estrogen receptors (GPER1 and GPER2) and ER1 and ER2 which are the main mediators of estrogen activity and have several polymorphs [158]. The genetic variants investigated included single-nucleotide variants in ER1 and ER2, GPER2 sequence variants, ER sequence variants with AD-related pathologic indices and ER DNA methylation and RNA expression in cognitive decline. GPER1 was associated with the level of cognition at baseline but not with the rate of decline or AD pathologic indices [158]. However, the rate of decline and tau tangle density were linked to the level of GPER1 DNA methylation, and the rate of cognitive decline was linked to GPER1 RNA expression in the postmortem dorsolateral pre-frontal cortex [158]. ER1 and ER2 were associated with the level of cognition but not with the rate of decline or AD pathologies. ER1 and ER2 DNA methylation levels also had an association with rate of decline and tau tangle density; however, ER2 RNA expression levels were not associated with a cognitive decline [18, 71].
Additionally, the APOE gene has been identified as a possible contributor to the varying results in studies on AD, with APOE2 and APOE3 carriers showing cognitive improvements when HRT is used, whereas APOE4 carriers show cognitive decline [18, 71]. This variation may be explained by the differential effects of estrogen receptor activation, where ERα stimulation by estrogen leads to overexpression of APOE4, potentially exacerbating cognitive decline in APOE4 carriers. In contrast, APOE2 and APOE3 carriers may benefit from the neuroprotective overexpression of APOE2/3, mediated by ERβ downregulation of APOE gene expression and protein levels [72, 159]. In conclusion, the APOE gene plays a significant role in the differing outcomes observed in studies on AD and HRT.
Kunkle et al. (2019) [160] performed a meta-analysis on genes associated with late onset Alzheimer’s disease (LOAD). 46 datasets with 94,437 individuals diagnosed with LOAD, 9,456,058 common variants and 2,024,574 rare variants were identified and analyzed [160]. This study confirmed 20 previously identified risk loci and 5 new loci which play a role in LOAD. APOE was seen to be 332% more likely to cause LOAD, and TREM2 was seen to increase the risk of LOAD by 201% [160]. However, SORL1 was seen to decrease the risk of LOAD by 19% and both CLU and CASS4 were seen to be 12% less likely to cause LOAD [160]. The five new loci identified were: IQCK, ACE, ADAM10, ADAMTS1, and WWOX. IQCK, ADAM10, and ADAMTS1 decreased the risk of LOAD by 8%, 7%, and 7% respectively, while ACE and WWOX increased the risk of LOAD by 32% and 17% respectively [160].
Thornton et al. (2011) [161] also performed a study to help determine genetic factors which may be associated with a risk of AD. The genetic factors studied were APOE and Catechol-O-Methyl Transferase gene (COMT). COMT is responsible for the metabolism of estrogen and has a number of genotypes including COMT methionine/methionine (COMT Met/Met), COMT valine/methionine (COMT Val/Met) and COMT valine/valine (COMT Val/Val). Serum E2 levels were linked to the genotype, with COMT Met/Met having a lower activity, therefore causing an increased E2 level, while COMT Val/Met and COMT Val/Val having a higher activity, therefore causing a decreased E2 level. They found that people with a homozygous genotype had a lower risk of AD, while people with a heterozygous genotype had an increased risk of AD. This result was seen through a synergistic effect with APOE4. However, they did not find COMT having an independent effect on cognition. It may be beneficial to explore this gene further, regarding its independent function and its effect alongside other potential factors relating to AD.
Foret et al. (2022) [162] carried out a study on 274 adults (113 women, 153 men) aged between 40 and 62. The effects of endogenous estrogen on the components of metabolic syndrome, (high waist circumference, high blood pressure, high fasting glucose, high triglyceride, and low HDL-cholesterol), are linked to cognitive decline [162]. The results indicated lower estradiol levels being associated with higher triglyceride levels, a larger waist circumference and white matter hyperintensities. Age had a positive association with white matter hyperintensities, with older people having a greater amount [162].
Other reproductive factors such as maternal age, endogenous estrogen levels and the reproductive period may also be implicated in AD. Barral et al. [163] conducted a longitudinal study on 551 families with 4,559 individuals to determine genetic and phenotypic traits associated with a longer lifespan. The study suggests an association between women with a later maternal age and better cognition in older life [163]. No significant differences were found in APOE4 frequency between earlier and later maternal ages [163]. There is also conflicting evidence regarding maternal age and its link to AD, with other studies showing an increased association between AD and a maternal age of less than 25 and greater than 40 [111, 112]. Based on these results, more research is needed so that a better understanding of this link can be achieved.
A cross-sectional study by Cortés et al. (2023) [164] investigated whether age at menarche, menopause and the duration of the reproductive window affected cognition. Data on 3,630 postmenopausal Hispanic women, with an average age of 59.2 and average reproductive window of 35 years, were analyzed [164]. They established that age at menarche has an inverse association with cognition, while an older age at menopause improved cognition. They also noted an association between a longer reproductive period and better cognitive performance [164]. When the data were not adjusted for education and income, the findings of the study were more stark. The use of OCs did not alter the results. The authors concluded that longer estrogen exposure over a lifetime plays a role in better cognitive performance [164]. These findings highlight the importance of hormonal factors in cognitive aging among postmenopausal women. According to the data analyzed by Needham et al. [153], it was concluded that a later menopause slightly improved cognition, especially in visual processing, associative learning, and memory, compared to an earlier age at menopause. However, these associations became insignificant after adjusting for reproductive and health-related factors [153]. Dementia risk was linked to later menarche, later menopause onset, smoking, and MHT use starting at age 60, regardless of MHT type [136]. The timing of HRT initiation was also crucial; starting HRT within a year of menopause reduced cognitive decline, while starting five years later increased it. Using HRT for over five years also raised the risk of MCI compared to non-users [141]. These findings underscore the complex interplay between hormonal factors and cognitive health, highlighting the importance of individualized strategies for hormone-related treatments in postmenopausal women.
Another factor that can have an impact on HRT outcome which could be explored is testosterone. A 2013 review discussed clinical trials regarding sex steroids and their effects on women and older men in terms of cognition [165]. Some positive effects of testosterone were noted on women, particularly those who had undergone surgical menopause; however, the studies were short-term. In addition, other studies showed a negative effect of testosterone on cognition [165]. It would therefore be useful to study long-term effects of different doses of testosterone to bring clarity regarding the impact on women’s cognitive performance. As mentioned above, low testosterone levels in men have been shown to increase the risk of AD. Androgen production decreases in women over the course of their lifetime [166]. In 2020, Yang et al. [167] concluded an in vitro and in vivo study in mice which reported that dihydrotestosterone had a neuroprotective effect against lipopolysaccharide neuroinflammation, which plays a role in AD and other neurodegenerative diseases [167].
Depression, which is more likely to be diagnosed in women, is another significant risk factor for the risk of AD dementia [118]. There is minimal evidence about the impact of smoking on the efficacy and side effects of HRT, however, women who smoke require higher dosages of HRT in comparison to non-smokers to achieve comparable clinical effects of HRT [123]. A dose-response relationship between smoking and early natural menopause was observed with current smokers and former smokers showing an increased risk of early menopause in comparison to women who never smoked [125]. Low consumption of alcohol may be protective against AD but increased alcohol consumption aggravates AD pathology [128]. Moderate alcohol consumption may increase estrogen levels in women receiving HRT, however, some studies provided no strong evidence on the effect of alcohol on hormones in postmenopausal women [168]. These findings suggest that lifestyle factors play an important role in variable ways in influencing the impact of HRT and AD progression in women. Dementia risk may vary with socioeconomic status, influenced by factors like education, income, wealth, and occupation. Education provides a protective effect against the risk of developing clinical AD in both men and women. A study revealed that women with more years of education performed better in category and letter fluency, continuous series switch rates, picture and auditory naming accuracy, and had faster picture naming latencies [117]. Women, compared to men, are more likely to develop dementia, be older, have lower socioeconomic status, and with conditions such as hypercholesterolemia, obesity, high alcohol consumption, physical inactivity, and depression. When considering risk factors women generally have lower education levels, social contact, and cognitive activity. Conversely, men are more likely to suffer from hypertension, diabetes, hearing impairment, and an unhealthy diet [114]. Parity and childbirth uniquely affect women, influencing hormone levels, health conditions, and lifestyle factors that impact dementia risk. The relationship between parity and dementia risk may also differ by geographical region. For instance, grand multiparous women (those with five or more childbirths) have a higher risk of dementia in European and Latin American populations, while nulliparous women face a higher risk in Asian populations [109]. When examining sex differences in AD, it is crucial to consider the effects of depression, alcohol use, smoking, education, health and socioeconomic status, and geographical and genetic variations.
It is important to speculate about several factors which may play a role in the sex differences seen in AD development, such as the ones considered above and possibly many others. Of the 27 studies discussed above, only 8 were specific for AD and a total of 18 contained a sample size of 1,000 or greater. 6 of the studies fulfil both conditions: Yuk et al. [136], Wong et al. [13], Savolainen-Peltonen et al. [146], Kim et al. [147], Yoo et al. [104], and Imtiaz et al. [150]. This shows that studies focusing on HRT and AD are scarce so more research must be done specifically to determine a conclusive stance on the topic. Within the current studies, discrepancies in final outcomes are obvious. Confounding factors were looked at in some but not all studies such as age at menarche, age at menopause, smoking, age at HRT initiation and length of HRT use. Also, different forms of estrogens were used, which could be the reason for discrepancies. Some results did show an association between HRT and AD, such as Savolainen-Peltonen et al. [146], which concluded that the use of HRT for more than 10 years was associated with AD regardless of HRT type. Other results like those by Imtiaz et al. [150] showed no association. Some other results then showed a protective role of HRT like in the study run by Kim et al. [147]. Meanwhile, other studies had mixed results such as Yuk et al. [136] and Wong et al. [13]. Based on the research reviewed here, it is clear that more large-scale multinational studies considering as many confounding factors as possible have to be completed to explore the relationship between HRT and AD as studies vary widely in their results from showing a positive correlation to a negative one to none at all. Importantly, more studies are required to focus on the impact of HRT on AD risk and disease progression, and considering different aspects of AD pathology.
CONCLUSION
From the current literature discussed in this review, it is unclear whether HRT plays a protective or therapeutic role in AD. Many factors are at play, including elements relating to the HRT itself, as well as genetic, socio-economic, and environmental influences. It is recommended that more research be performed on this topic in an attempt to clarify why there are such discrepancies between studies and ultimately answer the question if HRT is beneficial or harmful in terms of AD. Research in the future should take into account the genetic components, and the individual factors of the women involved such as reproductive span, parity, education, health, socio-economic and lifestyle factors and should also clearly focus on the HRT itself. The genetics and other characteristics of the individual should be explored, as they may explain the reasons behind the variability of different studies. Understanding individual variations in response to HRT will help guide clinicians to make informed and personalized decisions regarding its use for dementia prevention and treatment of menopausal symptoms.
AUTHOR CONTRIBUTIONS
Jessica Sayfullaeva (Conceptualization; Funding acquisition; Investigation; Writing – original draft; Writing – review & editing); John McLoughlin (Conceptualization; Funding acquisition; Investigation; Writing – original draft; Writing – review & editing); Andrea Kwakowsky (Conceptualization; Funding acquisition; Methodology; Project administration; Supervision; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
The work was supported by the University of Galway School of Medicine Summer Research Scholarship (JS, JM and AK) and the Association of Physicians of Great Britain and Ireland Summer Studentship (RIN2215 JS and AK).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.