
Abstract
BACKGROUND:
Hepatitis E virus (HEV) infection is being recognized as a major concern in developed as well as industrialized countries, especially for immunocompromised patients at risk of developing chronic hepatitis E.
OBJECTIVE:
We developed an HEV specific interferon gamma release assay (IGRA) for assessing T cell responsiveness to HEV antigens in resolved hepatitis E patients (RHE).
METHODS:
8 RHE patients and 13 HEV seronegative healthy controls (HC) were tested for IFNγ- and IL2-secretion in whole blood after challenge with recombinant HEV ORF2 genotype 1 and ORF2 genotype 3 antigens.
RESULTS:
The developed IGRA test differentiated by trend between the RHE group and HEV seronegative HC. RHE patients showed a stronger IL2 response to ORF2 genotype 1 or genotype 3 (180±47 and 171±39 pg/ml) compared to HC (96±34 pg/ml and 65±20 pg/ml). IFNγ responses were negligible.
CONCLUSIONS:
HEV specific IGRAs using IL2 as a marker should help to further clarify prior exposure to HEV.
Introduction
Hepatitis E Virus (HEV) infections are not limited to the tropics but also occur in industrialized nations of the western world [1]. While HEV genotype 1 and 2 infections are present in tropical countries with reduced hygienic conditions, genotypes 3 and 4 are transmitted zoonotically by consumption of swine meat and can be acquired autochthonously in Europe or the US [2, 3].
Serological tests for the detection of anti-HEV IgG and IgM antibodies are largely available in Europe, but none of these tests has been approved by the FDA for use in the US. There is a huge variability between these assays and the gold standard for anti-HEV IgG and IgM detection still needs to be defined [4–6].
In addition to serological tests, HEV could be detected directly by PCR. A WHO standard allows comparison of different HEV-PCR-methods and quantitation of the virus [7].
The aim of the present study was to develop an HEV specific interferon gamma release assay (IGRA) for assessing T cell responsiveness to HEV antigens in resolved hepatitis E patients (RHE).
Methods
Patient selection
Resolved hepatitis E patients (n = 8) previously treated at the hepatitis outpatient department of the University Medical Center Hamburg-Eppendorf were enrolled in the study for which all patients gave written consent and which was approved by the Ethics Committee of the Hamburg Chamber of Physicians (PV4551). HEV seronegative healthy donors of the blood transfusion service at the University Medical Center Hamburg-Eppendorf were enrolled in the study as healthy controls (HC, n = 13). Additional clinical data for all patients and HC was provided (Table 1).
Characteristics of all subjects included in the study
Characteristics of all subjects included in the study
aThe data are shown as means±standard deviations. bHC = healthy controls, RHE = resolved hepatitis E.
The recall antigen pool CEFT was purchased from JPT, Germany (#PM-CEFT) and solved in sterile dimethyl sulfoxide (DMSO; #RO/A9941/000100, Th. Geyer, Germany) 25 mg/ml followed by storage at –20°C. CEFT antigen pool consisted of antigenic peptides from human Cytomegalovirus (HHV-5; CMV), Epstein-Barr virus (HHV-4; EBV), Influenza A and Clostridium tetani. This positive control pool contained 27 peptides selected from defined HLA class I and II-restricted T-cell epitopes. Considering the high vaccination frequency against Influenza and C.tetani and the high prevalence of CMV and EBV in the general population in Germany recall antigen responses were expected for all patient samples. Staphylococcus aureus enterotoxin B superantigen (SEB) was obtained from Sigma Aldrich GmbH, Germany (#S4881) and stored 1 mg/ml in sterile, endotoxin-free H2O and –20°C. Synthetic HBV peptide libraries of HBcAg and HBsAg were purchased from JPT, Germany (#PM-HBV-CP and #PM-HBV-lEP, respectively) and solved in sterile dimethyl sulfoxide (DMSO; #RO/A9941/000100, Th. Geyer, Germany) 50 mg/ml followed by storage at –20°C.
Recombinant HEV antigens ORF2 genotype 1 and ORF2 genotype 3 were kindly provided by EUROIMMUN AG, Germany, and stored at –20°C. The recombinant antigens were produced heterologously in E. coli RosettaBlue (DE3)pLacI (Novagen/Merck KGaA, Germany) and after bacterial lysis purified by immobilized metal chelate affinity chromatography using Ni-NTA sepharose (Qiagen, Hilden, Germany) as described in detail for another recombinant protein [8].
Cytokine release assay in whole blood ex vivo
Venous blood was collected from hepatitis E patients and HC into sterile 7.5 ml Lithium Heparin Monovettes (Sarstedt, Germany). 1 ml of whole blood was then dispensed into sterile, pyrogen free 2 ml tubes with screw caps (Sarstedt, Germany) within 4 h of collection pre-loaded with sterile 0.9 % (w/v) NaCl solution (negative control), SEB (1st positive control), recall antigen CEFT (2nd positive control) or HEV antigens. In all tubes, glucose (2 mg/mI final concentration; pre-diluted in sterile 0.9 % (w/v) NaCl solution; #HN06.1, Carl Roth, Germany) was used to further enhance cytokine secretion, which had been tested before using various antigens (data not shown).
Thus, whole blood was stimulated with a total volume of 120μl/ tube of NaCl & glucose (negative control), 120μl/ tube SEB & glucose (1μg/ml final concentration after dilution out of stock, 1st positive control), 120μl/ tube recall antigen CEFT & glucose (10μg/ml final concentration after dilution out of stock, 2nd positive control) or 120μl/ tube HEV antigens (10μg/ml final concentration after dilution out of stock). SEB served as a 1st positive control due to its superantigenic properties by cross-linking MHC molecules with T-cell receptors, which proved the general stimulability of all samples. CEFT was introduced as a 2nd positive control to prove the functionality of antigen presenting cells in all samples in terms of antigen processing and presentation.
The tubes were closed and incubated at 37°C for 24 h. Thereafter, plasma supernatants were aspirated, pooled, stabilized with 0.045 % (w/v) NaN3 and stored at –20°C until assayed for cytokines within the next 7 days. A 5 % (v/v) CO2 atmosphere was proven to be unnecessary (data not shown) and yielded results comparable to stimulation in the presence of CO2.
IFNγ and IL2 ELISAs
Detection of global amounts of IFNγ and IL2 in human plasma was conducted using ELISA MAX Deluxe Sets from Biolegend, Germany: IFNγ (#430106) and IL2 (#431806). The manufacturer’s Avidin-horseradish peroxidase conjugate was replaced by PolyHRP80 streptavidine conjugate (#SP80C, SDT Reagents, Germany) in order to achieve a tenfold better lower limit of detection. Lower limit of detection (Background + 3x S.D.) was generally at 2 – 5 pg/ml for IFNγ and IL2, respectively. Initial dilution of control and test samples was performed described as follows: negative control (NaCl) 1/5, 1st positive control (SEB) 1/2500 for IFNγ and 1/500 for IL2, 2nd positive control (CEFT) 1/50 for IFNγ and 1/25 for IL2, test samples (ORF2 genotype 1 and ORF2 genotype 3) 1/5. If a test sample’s absorbance value fell outside the maximum standard curve range, these samples were subsequently retested with a tenfold higher dilution, e.g. 1/5 → 1/50, 1/500 → 1/5000, 1/2500 → 1/25000. A seven-point standard curve from 1 – 64 pg/ml IFNγ or IL2 was used for quantitation. Standards, controls and test samples were measured in duplicate. The samples were analyzed using Magellan software (version 6.5) equipped on a Tecan M200 plate reader.
Data analysis
Software
The ELISA data was analyzed using SigmaPlot software (Systat Software Inc., version number 12.2) and GraphPad Prism software (Graphpad Software Inc., version number 6.04).
Statistical analysis
Descriptive statistics and unpaired Student’s t-test were performed using SPSS Statistics software (IBM, version number 22), SigmaPlot software (Systat software Inc., version number 12.2) and GraphPad Prism software (Graphpad Software Inc., version number 6.04).
Results
RHE patients show strong IL2 responses towards HEV ORF2 genotype 1 and ORF2 genotype 3 antigens
Two major HEV antigens, ORF2 genotype 1 and ORF2 genotype 3, were tested in an HEV specific cytokine release assay with 8 RHE patients and 13 HEV seronegative HC. Stimulation of whole blood with sterile 0.9 % (w/v) NaCl solution (negative control), SEB (1st positive control) and CEFT (2nd positive control) confirmed the viability of all collected samples (Table 2).
Positive and negative controls
Positive and negative controls
aThe data are shown as means±standard error of mean (S.E.M.). bHC = healthy controls, RHE = resolved hepatitis E.
Recombinant ORF2 genotype 1 and ORF2 genotype 3 antigens elicited significantly stronger IL2 responses in RHE patients than HC (Fig. 1 b, Table 4; 180±47 and 171±39 vs. 96±34 and 65±20 pg/ml). ORF2 genotype 1 and ORF2 genotype 3 antigen challenge did not lead to significantly different IL2 responses in RHE patients (Fig. 2 b, 180±47 vs. 171±39 pg/ml).

Recombinant HEV ORF2 antigens elicit stronger IFNγ and IL2 responses during HEV-specific T cell stimulation in whole blood of RHE patients. n = 13 HC and n = 8 RHE patients, for each tested HEV antigen. Every HC or patient was tested against HEV antigens ORF2 genotype 1 and ORF2 genotype 3. (a) IFNγ, (b) IL2. Lower limit of detection (Background + 3x S.D.) was at 2 – 5 pg/ml for IFNγ and IL2. All values are given as mean concentration pg/ml±S.E.M. Unpaired Student’s t-tests, following symbol pinpoints significant differences: *. One symbol equals 0.05, two symbols 0.01, three symbols 0.001.
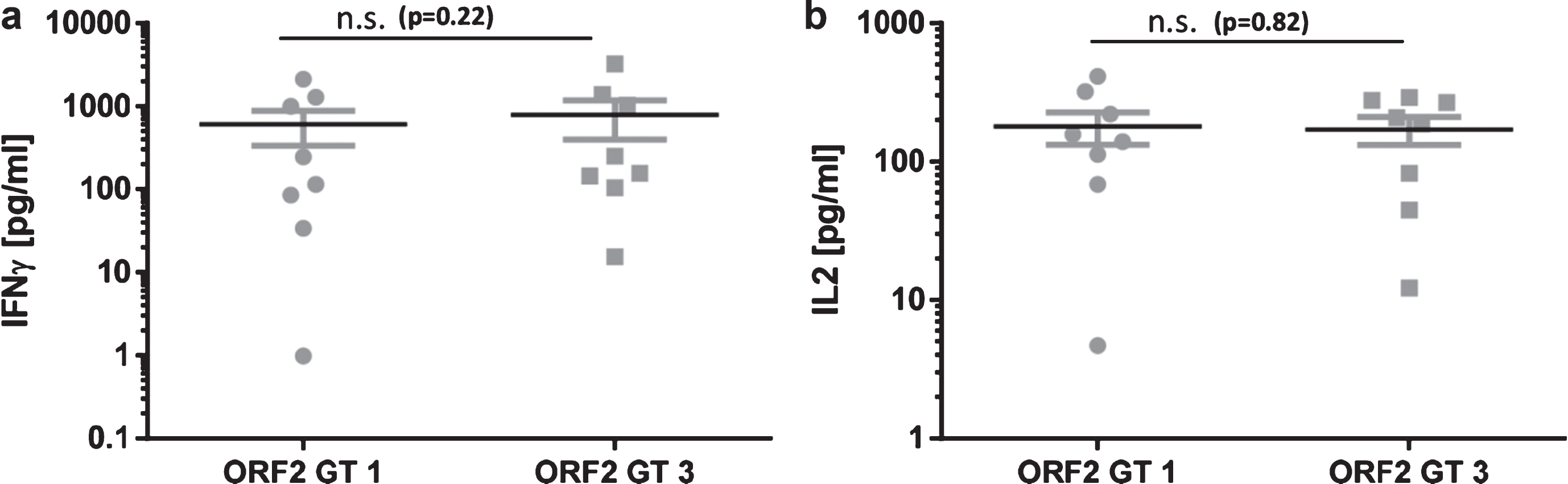
ORF2 genotype 1 and ORF2 genotype 3 antigen challenge does not lead to significantly different cytokine responses in RHE patients. n = 8 RHE patients, for each tested HEV antigen. Every patient was tested against HEV antigens ORF2 genotype 1 and ORF2 genotype 3. (a) IFNγ, (b) IL2. Lower limit of detection (Background + 3x S.D.) was at 2 – 5 pg/ml for IFNγ and IL2. All values are given as mean concentration pg/ml±S.E.M. Paired Student’s t-tests, following symbol pinpoints significant differences: *. One symbol equals 0.05, two symbols 0.01, three symbols 0.001.
Interestingly, IFNγ responses were not significantly different between RHE patients and HC (Fig. 1 a, Table 4). ORF2 genotype 1 induced IFNγ synthesis in whole blood of RHE patients and HC (613±276 and 454±208 pg/ml), while ORF2 genotype 3 elicited comparable IFNγ responses (792±391 and 557±143 pg/ml). ORF2 genotype 1 and ORF2 genotype 3 antigen challenge did not lead to significantly different IFNγ responses in RHE patients (Fig. 2 a, 613±276 vs. 792±391 pg/ml).
Taken together, cytokine release assays using ORF2 antigen challenge in whole blood and IL2 as a marker are able to depict the responsiveness of HEV-specific T cells in RHE patients.
We have established a protocol which is capable of analyzing the responsiveness of HEV-specific T cells using whole blood directly for testing without further sample preparation
IL2 responses after recombinant HEV ORF2 stimulation allow limited assessment of HEV specific cellular immunity in whole blood
The developed IGRA test differentiated by trend between the RHE group and HEV seronegative HC, but was not able to detect HEV genotype 1 or genotype 3 specific T cell responses using recombinant HEV ORF2 genotype 1 and ORF2 genotype 3 antigens.
Since imported HEV infections (genotype 1) are associated with higher transaminases, INR and bilirubin levels compared to autochthonous cases (genotype 3) [9], we aimed at detecting HEV genotype specific cellular immune responses by IGRA. However, ORF2 genotype 1 and ORF2 genotype 3 antigen challenge did not lead to significantly different IFNγ and IL2 responses in RHE patients and only IL2 allowed limited assessment of HEV specific cellular immunity in whole blood.
Our group demonstrated in recent studies that the toll like receptor (TLR) agonists lipteichoic acid (LTA), Poly(I:C) and CpG constitute potential costimulating reagents in CMV and HBV specific IGRAs [10, 11]. LTA, Poly(I:C) and CpG strengthen IFNγ synthesis after challenge with synthetic CMV pp65 peptide, native CMV lysate or recombinant pp65 in seropositive HC, whereas seronegative HC remain unaffected. The same accounts for hepatitis B vaccinated healthy blood donors after challenge with HBsAg in whole blood. These findings might offer solutions to overcome the limitation of this HEV specific IGRA especially regarding the distinct IFNγ and IL2 background in HEV seronegative HC after antigen challenge (Table 3, HC group). HEV specific immune monitoring using IGRAs can help to predict the course of chronic HEV infection in transplant patients and might be even more effective in combination with viral load monitoring if HEV specific IGRAs are enhanced by costimulating TLR agonists. Moreover, the risk of pregnant women to develop fulminant hepatic failure could be predicted together with confirming positive serology and understanding the mechanisms of chronic infection [1, 12].
ORF2 genotype 1 and ORF2 genotype 3 stimulations
aThe data are shown as means±standard error of mean (S.E.M.). bHC = healthy controls, RHE = resolved hepatitis E.
Conflict of interests
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
We thank all blood donors participating in this study. We further thank Katharina Heinzel (Brandenburg Medical School, University Hospital Brandenburg, Center of Internal Medicine II, Brandenburg, Germany) for excellent technical assistance.
The work was supported by the Ministry for Science, Research and Cultural Affairs of Brandenburg through the grant of the joint project “Konsequenzen der altersassoziierten Zell- und Organfunktionen” of the Gesundheitscampus Brandenburg.