
Abstract
BACKGROUND:
Direct oral anticoagulants (DOAC’s) are frequently used for different indications. Within the group of DOAC’s one representative is the factor Xa inhibitor rivaroxaban. In general, there are some clinical conditions where laboratory monitoring of DOAC’s can be important.
OBJECTIVE:
The aim of this study is to establish a mass spectrometric method for the determination of rivaroxaban plasma levels from citrate plasma samples and to make some considerations about the clinical interpretation of the results.
METHODS:
To determine the rivaroxaban plasma levels a triple quadrupole mass spectrometer equipped with an electrospray ionization ion source was used in combination with an ultra-performance-liquid-chromatography (UPLC) system.
RESULTS:
The results revealed that the mass spectrometric method is well suitable for the determination of rivaroxaban plasma levels in a routine laboratory. Last but not least the results from 36 patient samples showed that there is a wide variability within the peak and trough levels. The majority of patients showed trough levels above the safety threshold for surgical treatment in an emergency.
CONCLUSION:
For routine laboratories which already have a mass spectrometer it is a good option to apply this technique for the determination of rivaroxaban plasma levels.
Keywords
Introduction
Anticoagulation is a progressively increasing therapy in the aging society. Here, the group of Vitamin-K-Antagonists (VKA) is frequently used for different indications [1]. Examples are the treatment and therapy of acute venous thromboembolism as well as the thromboprophylaxis in patients with atrial fibrillation [1]. However, this class of anticoagulants shows some important disadvantages [1]. They involve the pharmacokinetic properties, the need of frequent laboratory monitoring as well as dose adjustments [1]. Furthermore, there are different factors like the diet, comedications and genetic variations which influence the anticoagulant activity of these drugs [1].
Since a few years the group of the so called direct oral anticoagulants (DOAC’s) is available as an alternative to VKA. A more predictable pharmacokinetic profile as well as fewer drug and food interactions are important advantages of these substances [1]. It is also important that in most cases a fixed dose without a frequent laboratory monitoring can be used for treatment or prophylaxis [1].
In general, the group of DOAC’s involves factor Xa inhibitors and thrombin inhibitors [2]. In both cases the substances act by binding to the respective coagulation factor which leads to an inhibition of the coagulative activity [2]. One commonly known representative of the group of factor Xa inhibitors is rivaroxaban, which is normally administered in a dose of 20 mg once daily in patients with atrial fibrillation [2]. In patients with renal insufficiency a dose reduction might be necessary depending on the creatinine clearance (CrCl) [2].
Although a fixed dose of rivaroxaban is used in most cases there are some conditions where monitoring of rivaroxaban plasma levels is of relevance. Especially in patients with acute liver or renal failure the determination of the plasma levels can be important due to the risk of accumulation [3]. Besides other indications for monitoring are extremes of body weight, unexpected thrombosis under treatment, severe traumata as well as bleedings [3]. Also in advance of urgent surgical interventions it might be important to determine the rivaroxaban plasma level in order to get information about possible bleeding risks [3].
Concerning laboratory monitoring of DOAC’s there are different methods which can be used for this application. Initially, it is possible to use special functional coagulation assays [3]. Especially for the determination of rivaroxaban plasma levels an anti-factor Xa assay which is calibrated against the drug is well suitable [3]. Normally, this is a chromogenic assay where the test system consists of factor Xa and a synthetic factor Xa substrate which is bound to a chromophore [4]. After cleavage of the substrate by factor Xa, the chromophore undergoes a color change, which can be quantified [4]. The extend of the color change is now directly proportional to the enzyme activity of factor Xa [4]. If rivaroxaban is present in the sample which is added to the test system it will promote factor Xa inhibition and therefore less factor Xa is available to cleave the substrate [4]. The consequence is a reduced color change. This principle in combination with calibration standards with known concentrations of rivaroxaban can be used to quantify the plasma level in the sample.
Beside the functional tests another alternative way to determine the plasma levels of DOAC’s is to use liquid chromatography mass spectrometry (LC/MS) [5–11]. In general this system consists of two different elements. At first a liquid chromatography system is used to chromatographically separate the target analytes in solution and to separate them from the sample matrix especially. In the second step an electrospray ionization (ESI) triple quadrupole mass spectrometer is used for the specific detection of the target analytes according to their molecular mass.
The aim of this study was to establish a LC/MS method for the determination of rivaroxaban from citrated plasma samples in a routine laboratory and also to make some considerations about the clinical interpretation of the results.
Materials and methods
Chemicals
In general, only LC-MS grade solvents were used. Water as well as methanol (MeOH) were purchased from Biosolve (Dieuze, France). Acetonitrile (ACN) was bought from Honeywell (Morristown, USA). Dimethyl sulfoxide (DMSO), formic acid (98%, mass spectrometry grade) as well as the internal standard dabigatran-D3 (100 μg/ml in ACN with 10% 0.01 N hydrochloric acid) were from Sigma Aldrich (St. Louis, USA). Last but not least rivaroxaban was purchased from Combi-Blocks (San Diego, USA).
Instrumentation
The liquid chromatography system was an Acquity UPLC (ultra-performance-liquid-chromatography) system from Waters (Milford, USA) equipped with a sample manager and a column manager. The column which was used for chromatographic separation of the target analytes was a Waters CORTECS UPLC C18 column (1.6 μm; 2.1×150 mm). For detection a Waters Xevo TQ MS triple quadrupole mass spectrometer equipped with an ESI ion source was applied.
Chromatographic conditions
A solvent combination of water as solvent A and acetonitrile as solvent B was used. In both cases 0.1% formic acid (FA) were added to the solvents. The column temperature was set to 55°C. The total amount of time for one analysis was five minutes. To achieve an optimal chromatographic separation of the compounds the following gradient elution profile was used: 0–0.4 min (90–90% A); 0.4–1.5 min (90–40% A); 1.5–2.5 min (40–40% A); 2.5–2.51 min (40–0% A); 2.51–4.0 min (0–0% A); 4.0–4.01 min (0–90% A); 4.01–5.0 (90–90% A). The flow rate was set to 0.5 ml/min. In general, 20 μl of the sample were injected into the system.
MS conditions
All measurements were done in positive ionization mode. Multiple reaction monitoring (MRM) was used to detect the target analytes with a high sensitivity and specificity. Here, argon was used as the collision gas. The mass transitions as well as the analyte specific cone voltage and collision energy are shown in Table 1. The capillary voltage was set to 0.45 kV. The desolvation temperature was 600°C and the source temperature 130°C. Last but not least the desolvation gas flow was set to 1000 l/h.
Mass transitions as well as analyte specific cone voltages and collision energies which were used for the detection of rivaroxaban and dabigatran-D3 (internal standard)
Mass transitions as well as analyte specific cone voltages and collision energies which were used for the detection of rivaroxaban and dabigatran-D3 (internal standard)
Due to solubility issues the rivaroxaban stock solution was prepared in DMSO with a concentration of 5 mg/ml. The Dabigatran-D3 stock solution was delivered as a ready-to-use product with a concentration of 100 μg/ml in acetonitrile and 0.01 N hydrochloric acid. Working solutions were made by dilution with the respective solvent as shown below.
For the preparation of the calibration standards the rivaroxaban stock solution was diluted to 10 μg/ml by using a water/acetonitrile solution (90:10, v:v) with 0.1% FA. Then calibration standards with concentrations of 500 ng/ml, 250 ng/ml, 125 ng/ml, 25 ng/ml and 12.5 ng/ml were prepared by dilution with rivaroxaban free citrate plasma. For quality control purpose quality control samples with concentrations of 200 ng/ml and 50 ng/ml were prepared by using the same principle.
For protein precipitation of the citrate plasma samples prior to injection into the LC/MS system a methanol/acetonitrile solution (30:70, v:v) containing the internal standard dabigatran-D3 with a concentration of 200 ng/ml was prepared (precipitation reagent).
To achieve optimal results during chromatographic separation of the compounds it is important to adapt the solvent composition of the sample to the solvent conditions on the column. For this purpose a water/acetonitrile solution (90:10, v:v) with 0.1% FA was made (dilution reagent).
Sample preparation and storage
Citrated whole blood samples were taken from the routine reserve sample storage of the Institute of Laboratory Medicine before they were thrown away. Only samples from patients taking rivaroxaban and where the medical doctor wants to determine the rivaroxaban level were included. Another inclusion criterion was that the time interval between last drug intake and sample collection by the medical doctor was known. This is important to identify peak and trough levels. Finally, the citrated whole blood samples were centrifuged at 2800× g for 5 min and the supernatant was stored at –18°C until analysis.
Prior to analysis 50 μl of the supernatant of the samples were mixed with 150 μl of the precipitation reagent and vortexed for at least 20 seconds to perform a protein precipitation. This was also done with the calibrators as well as the quality control samples. After protein precipitation the samples were centrifuged at 20000× g for 10 min. Than 100 μl of the supernatant were transferred into micro reaction tubes and a second centrifugation step at 20000× g for 10 min was done. Finally, 50 μl of the supernatant were transferred into an autosampler vial containing a limited volume insert and 200 μl dilution reagent were added. This solution was then injected into the UPLC-ESI-MS system. In the end the measured rivaroxaban values were multiplied with factor 1.1 to compensate the dilution effect of the citrate solution in the citrate plasma samples.
Ethics statement
All plasma samples which were used in this study were waste from routine laboratory diagnostics. Therefore, there was no need for an ethic approval. The respective samples were originally collected for routine diagnostics and no collection was done specifically for the purpose of this study. Further, the samples were anonymized prior to the use in this study and no medical or personal data of the patients were recorded. Solely the time interval between drug intake and sample collection was recorded for this study. However, this information is crucial for the routine diagnostics and therefore it was already known. None of the authors was directly involved in the sample collection.
Assay validation
To validate the performance of the assay different parameters were acquired. At first the limit of detection (LOD) and the limit of quantification (LOQ) were determined. To identify the LOQ a 25 ng/ml calibrator was diluted until the signal-to-noise ratio was 3:1. The concentration at this point represents the LOD. For the investigation of the LOQ calibration standards with decreasing concentrations were measured in multiple technical replicates. The LOQ was determined as the concentration level at which the standard deviation within the technical replicates is above 10%.
Next, the linearity of the method was investigated by measuring calibration standards with rivaroxaban concentrations of 500 ng/ml, 250 ng/ml, 125 ng/ml, 25 ng/ml and 12.5 ng/ml. A linear regression was performed to investigate linearity.
Recovery and precision were determined by using spiked blank citrate plasma samples with a rivaroxaban concentration of 20 ng/ml (low concentration range) and 100 ng/ml (high concentration range). These samples were measured in ten technical replicates within one run to determine intra-day recovery and precision. For the investigation of inter-day recovery and precision the samples were measured in five technical replicates at four consecutive days.
Last but not least an inter-laboratory comparison was performed by sending 13 citrated plasma samples to a partner laboratory and comparing the results. The partner laboratory used a comparable method to determine the rivaroxaban plasma levels.
To make some considerations on the clinical interpretation of the rivaroxaban levels 36 routine samples including trough and peak levels were measured and the results were summarized.
Statistical analysis
For the analysis of the results and generation of plots the statistics software R was used [12]. The method comparison was done by using a Passing-Bablok-Regression analysis as well as a Bland-Altman-Analysis.
Results
The Waters CORTECS UPLC C18 column produced excellent chromatographic results. Well resolved peaks as well as a good separation of the compounds were achieved. The retention time of the internal standard dabigatran-D3 was 1.33 min. Rivaroxaban produced a clear peak at a retention time of 2.02 min. An example chromatogram of a blank citrated plasma sample spiked with 25 ng/ml of rivaroxaban is shown in Fig. 1.

Example chromatogram of a blank citrated plasma sample spiked with 25 ng/ml rivaroxaban. The internal standard dabigatran-D3 elutes at a retention time of 1.33 min (a) and the analyte rivaroxaban at a retention time of 2.02 min (b).
During assay validation different parameters were tested. To get some information about the sensitivity of the method at first the LOD and LOQ were investigated. Here, for rivaroxaban a LOD of 0.5 ng/ml and a LOQ of 5 ng/ml were identified.
Next, linearity in a concentration range from 12.5 ng/ml to 500 ng/ml was investigated by measuring five calibrators with known concentration. In this concentration range the coefficient of determination was 0.999 (see Fig. 2).
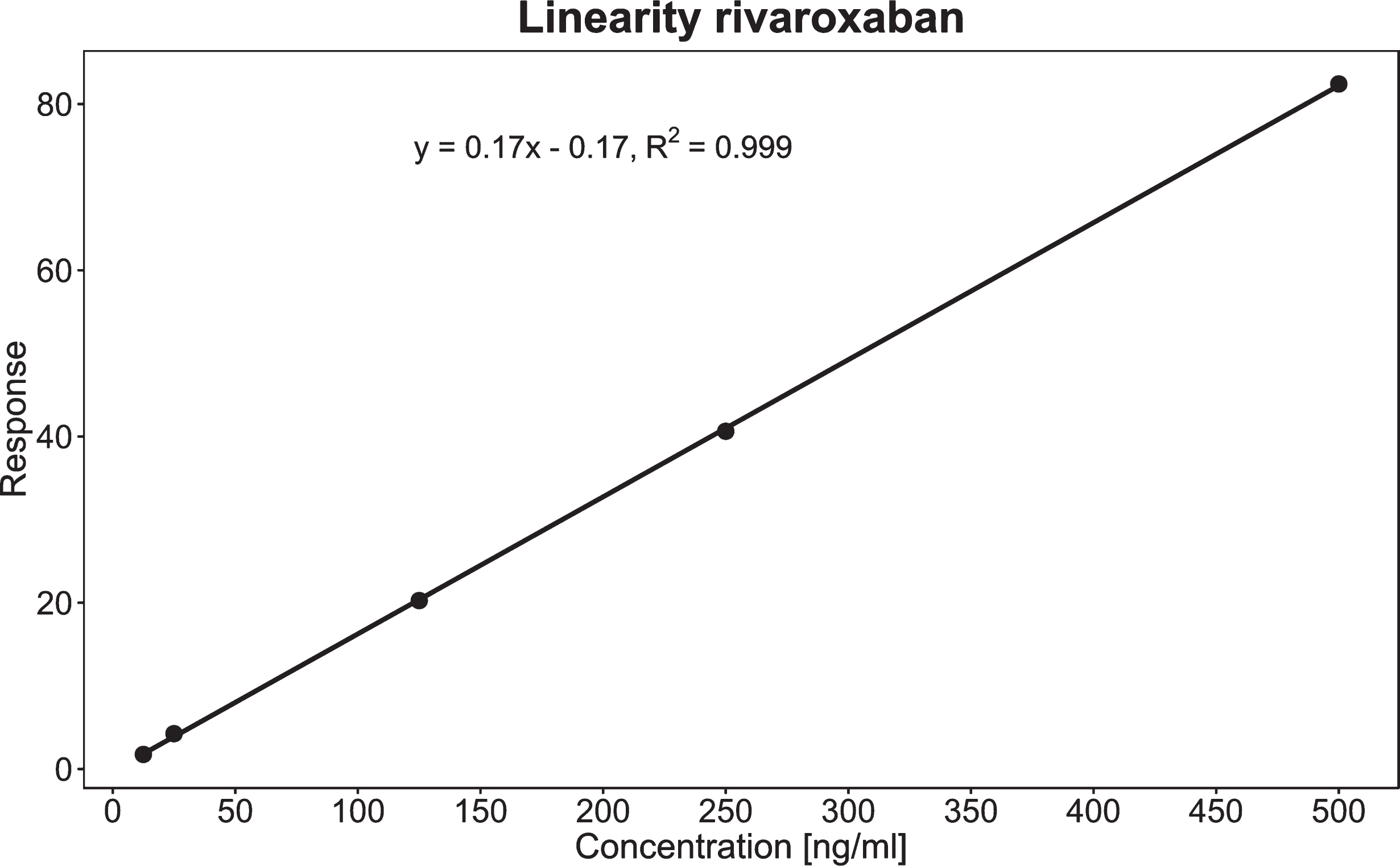
Linear regression analysis to identify the linearity of the developed method in a concentration range from 12.5 ng/ml to 500 ng/ml.
The intra-day recovery was 104.6% in the low concentration range and 104.8% in the high concentration range (Table 2). The coefficients of variation (VK) were 4.6% and 4.8% respectively. Inter-day recovery in the low concentration range was 100.1% with a VK of 11% (Table 2). In the high concentration range a recovery of 114.0% and a VK of 8.1% were achieved.
Intra-day as well as inter-day recovery and precision in the high concentration range (100 ng/ml) and the low concentration range (20 ng/ml)
Finally, a laboratory comparison was done by sending 13 routine samples to a partner laboratory comparing the results. For comparison a Passing-Bablok-Regression analysis as well as a Bland-Altman-Analysis were performed (Fig. 3). The regression line of the Passing-Bablok-Regression shows an intercept of –32.1 (95% confidence interval: –105.9–3.8) (Fig. 3A). The slope of the regression line is 1.5 (95% confidence interval: 1.08–2.03) (Fig. 3A). To proof the equality of both methods the confidence interval of the intercept must include 0 and the confidence interval of the slope 1. This condition was only met for the intercept but not for the slope. Therefore, the results of the Passing-Bablok-Regression analysis indicate that there is a slight proportional difference between the results obtained by both laboratories. However, a constant difference was not detected.
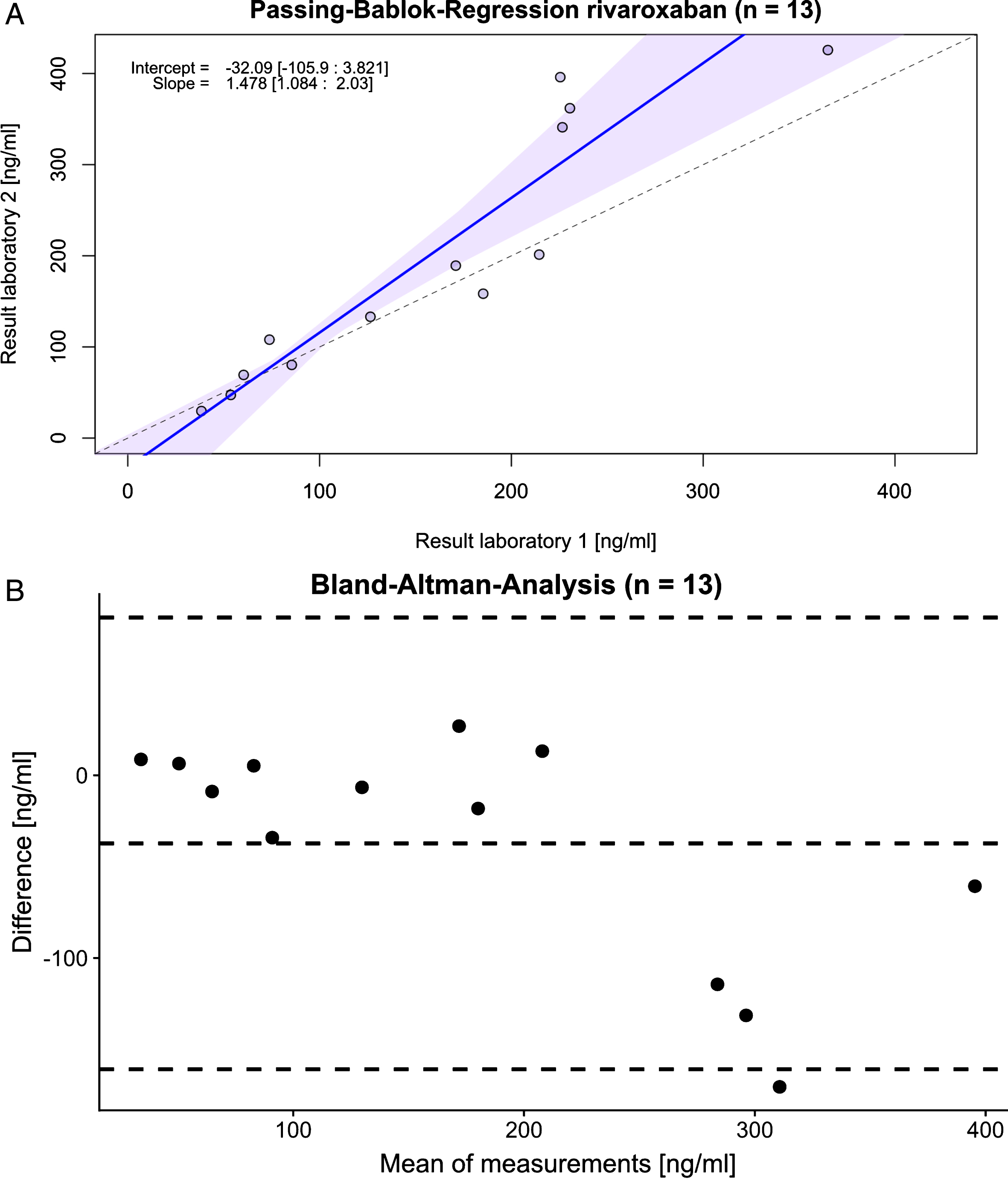
Comparison of the rivaroxaban levels in 13 routine samples determined in our laboratory (laboratory 1) with a partner laboratory (laboratory 2). In both laboratories LC-MS was used for determination. A) Passing-Bablok-Regression analysis of the results. B) Bland-Altman-Analysis of the results.
Furthermore, the Bland-Altman-Analysis also revealed that there was a relevant difference between both laboratories especially in the high concentration range above 200 ng/ml (Fig. 3B). One can see that the results from our laboratory in this concentration range were generally lower compared with the partner laboratory. In the lower concentration range below 200 ng/ml the difference between both laboratories was quite small.
Last but not least 36 routine citrated plasma samples were measured to make some considerations about the clinical interpretation of the results (Fig. 4). The boxplot shows that there is a clear concentration difference between peak levels and trough levels of rivaroxaban. 14 patients had peak levels and 22 showed trough levels respectively. It is also important that there was a large variation within both groups. The peak levels ranged from 113.7 ng/ml to 576 ng/ml; the trough levels from 13.9 ng/ml to 292.8 ng/ml. It was also recognizable that most of the patients showed trough levels above 30 ng/ml (19 of the 22 patients).
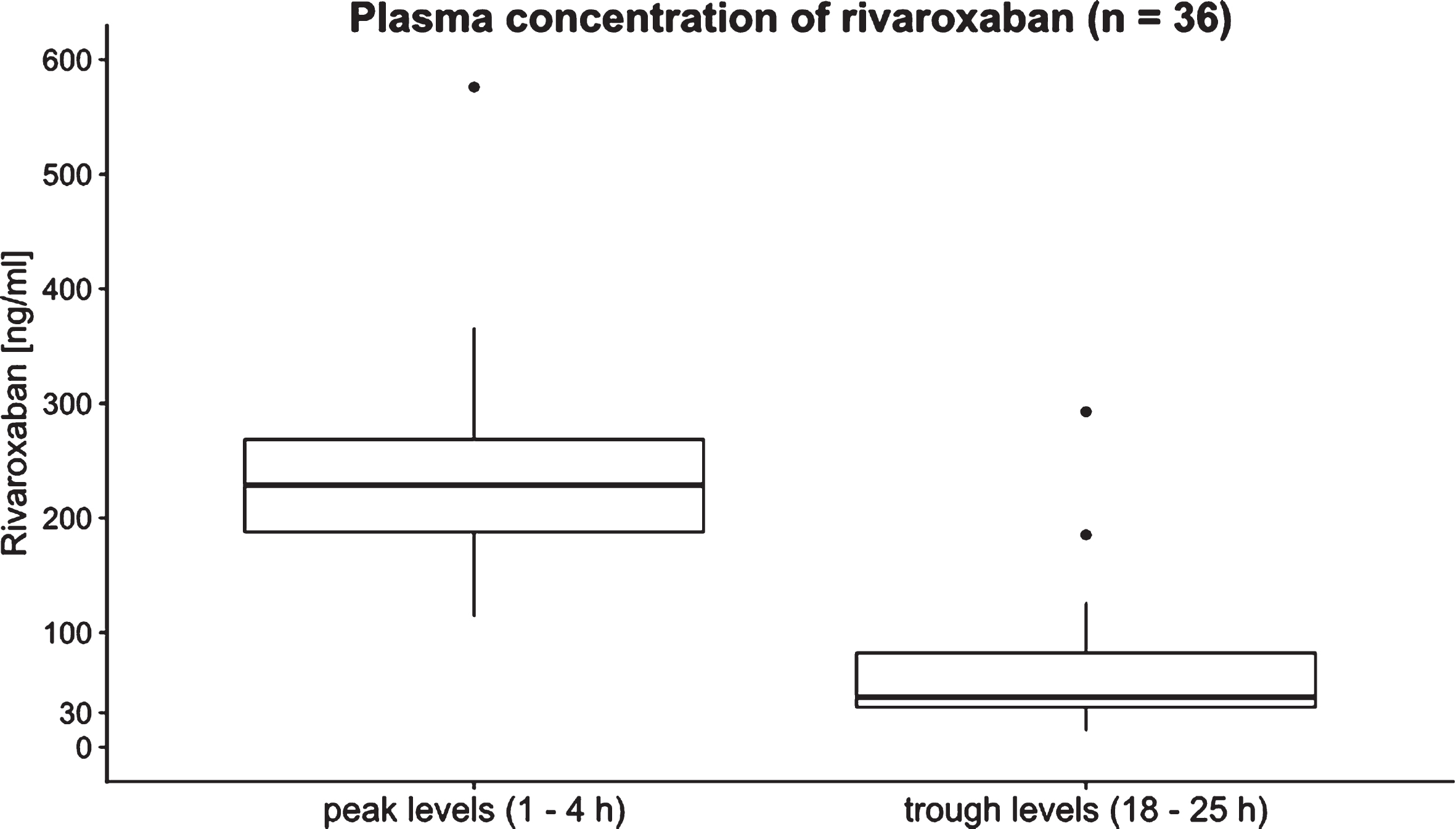
Rivaroxaban plasma levels of 36 patient taking rivaroxaban. 14 peak levels and 22 trough levels were measured.
The main aim of this study was to develop a mass spectrometric method which can be used under routine conditions for the determination of rivaroxaban plasma levels of patients taking this medication. The most important advantage of mass spectrometry in comparison to functional coagulation assays for the determination of DOAC plasma levels involves the specific and direct detection of the analyte. The functional tests detect the DOAC levels by the anticoagulant activity of these compounds. When using mass spectrometry, the target analytes are very specifically detected by their molecular mass. Therefore, the risk of interferences with other anticoagulant active substances which might be present in the patient sample is low. Important disadvantages of mass spectrometry involve the high costs of such instruments and the need for trained personal to operate the instruments. Therefore, the mass spectrometric determination of the DOAK levels is better suitable for laboratories which already have a suitable instrument.
Under routine conditions analytical methods should be fast and cost effective. Therefore, only a simple protein precipitation using an acetonitrile/methanol solution was selected for sample preparation of the citrated plasma samples instead of a more complex sample preparation technique like solid phase extraction (SPE). The big advantage of a simple protein precipitation is that it is fast and easy to perform. Even if more complex sample preparation techniques would produce cleaner extracts we did not observe any problems with the protein precipitation for this application and decided to use this technique under routine conditions.
The validation measurements which were performed during the method development process indicate that the developed method is well suitable for this application. Regarding sensitivity the LOD and LOQ indicate that the mass spectrometric method is sensitive enough to detect even low levels of rivaroxaban in patient samples. Although the LOQ is around 5 ng/ml we decided to use a concentration of 12.5 ng/ml as the lowest calibration point because lower concentrations are not relevant for the clinical interpretation of the results. The investigation of linearity revealed an excellent linearity in the concentration range from 12.5 ng/ml to 500 ng/ml. Samples with a concentration above 500 ng/ml require an additional dilution step with rivaroxaban free plasma to achieve levels in the calibrated concentration range. The investigation of recovery revealed a good recovery within one batch as well as within different batches on different days. Also, the intra-day as well as the inter-day precision are in an acceptable range. These results indicate that the variation within multiple technical replicates of the same sample is quite low.
Last but not least during the validation process a laboratory comparison was performed by sending 13 routine samples to a partner laboratory and comparing the results. The Passing-Bablok analysis indicated that there was a slight proportional difference between both laboratories. This was confirmed by the Bland-Altman-Analysis. Here, it was shown that there was a relevant difference in the concentration range above 200 ng/ml. In this concentration range lower levels were obtained in our laboratory in comparison to the partner laboratory. An explanation for this problem might be that a different calibration range was used by the partner laboratory. It is also possible that an adaption of the internal standard concentration in our method would lead to more accurate results in the high concentration range. However, this difference was accepted because a larger, method dependent variation in the high concentration range has only a minor influence on the clinical interpretation of the results.
Standardization in general is an important point to take into consideration when talking about analytical methods for the determination of DOAC plasma levels. Recently some proficiency testing schemes for the determination of DOAC plasma levels were established. The results from a study of Tripodi et al. indicated that the analytical assays for the DOAC measurement perform reasonably well and a relative small interlaboratory variability was observed [13]. Although there is the possibility to participate in proficiency testing schemes, until today to our knowledge no certified reference materials (CRM) for the determination of DOAC plasma levels is available. Concerning the interlaboratory comparability a CRM would be ideal for calibration and quality control of the respective analytical methods.
After successful validation of the mass spectrometric method 36 routine samples were measured. The large variability in the peak and trough levels is in concordance with the concentration ranges presented in a work of Samuelson et al. [14]. Due to this large variability the clinical interpretation of the rivaroxaban levels is quite difficult. Basically, the plasma level determination allows you to separate peak from trough levels and to see whether the patient takes his medication. Therefore, the plasma level determination can be used to get some information about the patient’s compliance. However, due to the wide variability the interpretation of the actual concentration value is mainly important to identify the bleeding risk in case of urgent surgery. Based on the data from the ROCKET-AF design study Pernod et al. mentioned a concentration of 30 ng/ml as an acceptable safety threshold for surgical treatment in an emergency [15]. In patients with plasma levels below this threshold an operation without delay should be possible [15]. For rivaroxaban concentrations above 30 ng/ml a delay of the operation might be necessary if possible [15]. The delay interval depends on the actual concentration [15]. In our sample collective the majority of patients had trough plasma levels above 30 ng/ml. Therefore, we conclude that the determination of rivaroxaban plasma levels is important in patients requiring urgent surgical treatment under rivaroxaban therapy even when the last drug intake was 24 hours ago. Depending on the results a delay of the surgical intervention might be necessary if possible. However, we did not collect the samples by our self and had only a small samples size. Therefore, the results should be confirmed in a larger, well defined patient population. Also, special attention should be given to patients with a reduced kidney function because of the risk of rivaroxaban accumulation.
Finally, for the future it is also important to include apixaban, dabigatran and edoxaban in the DOAC panel and to perform similar measurements for these compounds.
Conclusion
The results of the study indicated that liquid chromatography mass spectrometry is well suitable for the determination of rivaroxaban plasma levels in a routine laboratory. In general, it is important to think about the standardization of such assays to achieve a good interlaboratory comparability. To reach a high level of standardization a CRM might be helpful. Last but not least the data from the small sample collective indicated that there are patients with trough level above 30 ng/ml even 24 hours after the last drug intake. Therefore, it is important to determine the plasma levels prior to emergency surgery in patients taking rivaroxaban even when the last intake is 24 hours ago. Depending on the concentration a delay of the surgical intervention might be necessary (if at all possible).
Footnotes
Acknowledgments
None.