
Abstract
BACKGROUND:
Semen analysis is a routine predictor of male fertility, and however, measurements of sperm morphology, motility, and concentration do not always evince genomic defects.
OBJECTIVE:
To investigate sperm parameters of renal transplant patients and to evaluate sperm DNA defects.
METHODS:
Seminal samples from 25 healthy controls and 56 transplantation patients were analyzed to evaluate DNA fragmentation by TUNEL. The differences in TUNEL-assay results and seminal parameters were compared between kidney transplant patients and controls.
RESULTS:
Among the azoospermic patients, 37.5% had fathered children before the disease. Three patients receiving sirolimus treatment had oligoasthenoteratozoospermia and infertility. In kidney transplant patients, DNA fragmentation was slightly higher than controls. Total motility (%) of the spermatozoa from the kidney transplant patients (42.2±21.9) was significantly lower (P < 0.05) than those of the control group (64.3±11.9). Moreover, control individuals had significantly higher (P < 0.05) normal morphology (23.2%) compared to the patient group (20.3%). Concerning sirolimus treatment, three patients had severe oligoasthenoteratozoospermia in their ejaculate, and however, DNA fragmentation rates were not significantly higher than those in the remaining individuals of the transplant group.
CONCLUSIONS:
The sperm DNA fragmentation rate in kidney transplant patients was slightly higher than in the control group (P = 0.09). However, the amount of spermatozoa DNA damage may lead to infertility in kidney transplant patients.
Keywords
Introduction
The male genome abnormalities depicted by DNA damage may indicate male-subfertility regardless of the routinely used semen properties [1–3]. Increased proportions of fragmented sperm DNA are associated with poor semen quality [2, 4], but the origin of this damage is still not fully elucidated. Previously published papers have demonstrated nucleus anomalies of spermatozoa [4]. Three factors have been suggested as the cause of DNA damage in the germline: chromatin packaging deficiencies, apoptosis (abortive), and oxidative stress.
Infertility is a common complication in chronic kidney disease (CKD) patients, however, successful kidney transplantation usually enables fertility [5]. Besides, endocrine abnormalities are common in CKD patients and lead to sexual dysfunction, altered mineral metabolism, hyperparathyroidism, and anemia [6, 7]. Erectile dysfunction in men decreased libido, and infertility in both sexes are common clinical problems [8]. Moreover, the male reproductive function may be affected by prescribed immunosuppressive therapy to prevent rejection after transplantation. In this context, it is important to evaluate the influential factors such as medication procedures and the pre-treatment period. Male infertility is also related to impaired spermatogenesis, as indicated by decreased total sperm counts and sperm motility along with elevated levels of sperm abnormality, following the treatment. There is a need for studies on the evaluation of DNA fragmentation in renal transplant patients. Therefore, this study was aimed to investigate the sperm parameters of kidney transplant patients, including sperm DNA defects.
Material and Method
Study population
The present study included 56 kidney transplant male patients (34 married and 22 single) aged 22 to 53 (mean 35.7) years and 25 healthy male controls, with proven fertility (n = 25; initiated a pregnancy within the past year) were selected to evaluate normal semen parameters according to the guidelines of the World Health Organization [9]. This study was approved by the Bursa Uludag University Medical Research Ethical Committee (approval number 2011-11/5). Written informed consent was obtained before the study began. All procedure performed in this study involving human participants was under the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Study design
An experimental clinical trial with an intervention group (kidney transplant patients who received immunosuppressive therapy) and a control group (healthy males) were performed in this study. A complete physical examination (height and weight), was conducted, and moreover, a questionnaire was applied to evaluate lifestyle factors, personal background, medical history, occupational status and environmental factors, sexual and reproduction status, genetic risk factors, and physical activity. Patients who received immunosuppressive treatment for at least three months were included in the cohort. The mean transplantation duration was 41.18±4.38 months, the mean transplant age was 33.84±2.53 years, and the mean immunosuppressive treatment duration was 41.09±4.36 months. We excluded men with abnormal sexual/ejaculatory functions, semen non-liquefaction, immune infertility, and risk factors for infertility (e.g., postvasectomy, varicocele or orchidopexy) as well as men currently receiving infertility treatment (e.g., hormonal treatments). Furthermore, subjects with abnormal karyotype and Y chromosome microdeletions of the azoospermia factor region were excluded from subsequent analyses to avoid spermatogenesis impairment due to Y microdeletions.
Forty-eight out of 56 men with kidney transplantation were found to be appropriate for the study and were included in the study for the assessment of sperm DNA fragmentation damage by the Tdt-mediated dUTP nick-end labeling (TUNEL) assay. Total testosterone levels, follicle-stimulating hormone (FSH), luteinizing hormone (LH), among groups were also determined.
After a recommended three to five-day sexual abstinence period, semen samples were obtained in a private room by masturbation. Conventional semen analysis was performed; after liquefaction at 37°C for 30 min. This analysis included semen volume and sperm concentration and motility, sperm number per ejaculum. Application/report of semen analyses was in agreement with the 2010 WHO laboratory manual [9].
Immunosuppressive therapy
All patients had their first kidney transplantation. In addition, calcineurin inhibitors (CNI) were provided to all patients. CNI treatment consisted of cyclosporine-CsA 6 mg/kg/d or tacrolimus-Tac 0.05–0.1 mg/kg/d) or mammalian target of rapamycin (mTOR; sirolimus) combined MMF (mycophenolate sodium 1440 mg/d or mycophenolate mofetil 2 g/d) or azathioprine (AZA, 100 mg/d) with corticosteroids (methylprednisolone, 500 mg intravenous; afterward, prednisolone, 1 mg/kg/d oral). Additionally, all patients continued basiliximab treatment (20 mg, pre-and post-transplantation, 4 days). To achieve target trough levels, the dosages of CNIs were adjusted as follows:
CsA: first 3 months, 200–300 ng/mL; subsequently, 100–200 ng/mL; and Tac: first 3 months, 8–12 ng/mL; subsequently, 5–8 ng/mL.
Oral prednisolone dosage was tapered to 20 mg/d after 1 month, 10 mg/d after 2 months, and 5 mg/d after 6 months.
DNA fragmentation analysis
the TUNEL assay was performed to determine sperm DNA fragmentation. In this context, an In-Situ Cell Death Detection Kit (Roche Diagnostics) was used as instructed by the manufacturer. Shortly, the spermatozoa were immediately fixed in Carnoy’s solution (2 : 1 methanol/acetic acid) after trypsinization (Trypsin-EDTA) and stored at –20°C for at least 1 h. Sperm pellets were washed with phosphate-buffered saline (PBS), were afterward permeabilized for 20 min with 0.1% (v/v) Triton X-100 (Sigma-Aldrich, St. Louis, MO) in sodium citrate dehydrate (VWR, Fontenay sous Bois, France; 3.4 mmol l–1, pH 6.8), and washed again with PBS. The cells were later incubated with FITC-labelled dUTP and a terminal deoxyribonucleotidyl transferase enzyme (TUNEL solution). The positive control sample was treated with 100μl of DNase (1 U μl–1) (Fermentas, Maryland, USA) at 37°C before incubation with the TUNEL solution for 1 h, and in the negative control samples, TUNEL solution was omitted. The cells were next washed twice in PBS and spread over glass slides. In a dark environment at room temperature, slides were dried and DAPI solution (VECTASHIELD Mounting Medium with DAPI, 1.5μg ml–1; Vector Laboratories, Burlingame, CA) was added to the spermatozoa. The slides were examined by fluorescence microscopy. 200 spermatozoa (at least) were assessed, and the total DNA fragmentation rate was calculated as the number of FITC-positive cells divided by the total number of sperm nuclei (labeled with DAPI). Figure 1 shows a sample area with DNA fragmented and unfragmented spermatozoa.

Sperm cell TUNEL test. Dark green painted cells show sperm cell without DNA fragmentation and light green glittering cells show DNA fragmented sperm cells.
The statistical analysis was performed by using SPSS software v20.0 (IBM SPSS Statistics). The homogeneity of the variances was tested by Levene’s test. An independent samples t-test, compared seminal parameters and DNA damage between the two groups (kidney transplant recipients vs control group). Moreover, a one-way analysis of variance was used to compare data among the groups concerning the effect of the drugs on spermatogenesis. For all two-sided tests, a probability level of P < 0.05 indicates the statistical significance, and a probability level of P < 0.1 points out a tendency.
Results
This study included 56 kidney transplant male patients (34 married and 22 single) aged 22 to 53 (mean 35.7) years and 25 controls (aged 22–50 years, mean 35.5) (P = 0.8). As shown in Table 1, eight (14%) out of 56 men with kidney transplantation had azoospermia and were excluded from sperm DNA fragmentation analysis. In the kidney transplantation group, 16 patients had normozoospermia and the remaining 32 patients had oligozoospermia (n = 1), asthenozoospermia (n = 4), teratozoospermia (n = 6) or a combination of these abnormalities (n = 21). Table 2 shows the seminal parameters of the patients and the control individuals.
Paternity status of the kidney transplant patients
Paternity status of the kidney transplant patients
O: oligozoospermia, A: asthenozoospermia, T: teratozoospermia. *Eight (14%) out of 56 men with kidney transplantation have azoospermia and are excluded from sperm DNA fragmentation analysis. Three out of 8 (37.5%) azoospermic patients had paternity before the incipience of their kidney disease.
Seminal parameters and DNA damage
*P < 0.1.
The sperm DNA fragmentation in kidney transplant patients was slightly higher compared to controls (P = 0.09) (Fig. 2). Spermatozoa motility and morphology of the kidney transplant patients were significantly lower than those of the controls (P < 0.05) (Table 2).
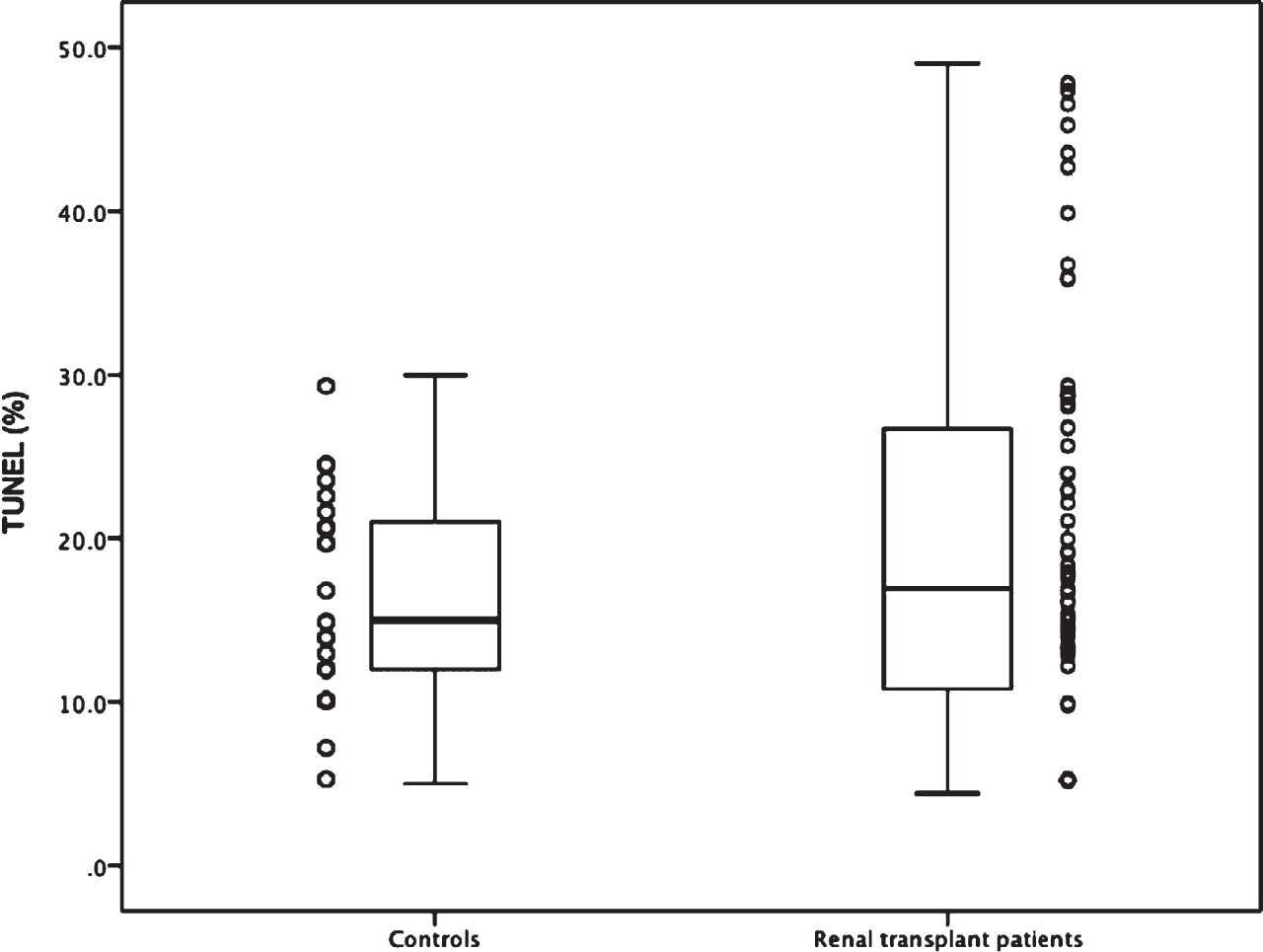
Box plots showing the distribution of sperm DNA fragmentation among the controls and patients using the TUNEL assay.
The post-transplantation duration, which was defined as the duration of the exposure period to immunosuppressive treatment, was less than 12 months for 18 patients after transplantation surgery (four patients, 22.2%, had normozoospermia in this group), 12–24 months for 6 patients after surgery (two patients, 33.3%, had normozoospermia in this group), and 24 months in 24 patients after surgery (ten patients, 41.6%, had normozoospermia in this group). Differences in the sperm DNA fragmentation index did not reach statistically significant levels among these groups (P = 0.835) (Fig. 3).

Box plots showing the distribution of sperm fragmentation among patients according to duration after renal transplantation.
Regarding sirolimus treatment, three patients had severe oligoasthenoteratozoospermia (OAT) and they experienced infertility. The mean of DNA fragmentation index was slightly higher than the mean of those in the remainder of the kidney transplantation group (P < 0.1). In the kidney transplantation group, the sperm DNA fragmentation index was lower in the patients who had normozoospermia (15.6±10.58) than those whose spermogram results showed oligo-, astheno- or teratozoospermia or a combination of these parameters (23.7±13.1) (P = 0.038). The number of patients in the immunosuppression treatment protocol is reported in Table 3.
Immunosupressive treatment protocols of kidney transplant patients
MMF: Mycophenolate sodium or mofetil, CsA: Cyclosporin, Tac: Tacrolimus, AZA: Azathioprine, mTOR: mTOR inhibitor (sirolimus), PRE: Prednisolone, Norm: Normozoospermia.
Testicular volumes (P = 0.13), LH levels (P = 0.97), and total testosterone levels (P = 0.31) were not statistically significant among groups but significantly elevated levels of FSH were observed in the group treated with cyclosporin A + mycophenolate mofetil+steroid (P = 0.028).
Loss of libido, impotence, and infertility due to impaired spermatogenesis and testicular damage are frequently seen in kidney failure [10]. Moreover, hypothalamic-pituitary-gonadal dysfunction characterized by waned sperm maturation is common in these patients [11]. Semen analyses typically show low-volume ejaculate, oligoazoospermia or azoospermia (complete), and decreased percentages of motile sperms. A low spermatogenic activity has been demonstrated by testicular histology. It is characterized by mature spermatocyte insufficiency or germinal element aplasia. The factors associated with the testicular damage in uremia remain unclear. Plasticizers in dialysis-tubing (such as phthalate) may be evaluated as a possible factor in patients with hemodialysis. Moreover, gonadal steroidogenesis might be impaired by uremia. Typically, a decrease is observed in the serum total and free testosterone concentrations. Institution of maintenance dialysis may improve these problems, but normalization often cannot be achieved and quality of life is decreased [12, 13]. Normally, a kidney transplant likely restores sexual activity by six months after successful kidney transplantation; however, the reproductive function might partially remain impaired [11]. Some improvements have been reported in the three main parameters of semen quality (spermatozoa number, motility, and morphology) after kidney transplantation [14] and the sex hormone profile tends to normalize [15]. Prolonged peritoneal dialysis, elevated levels of FSH in pre-transplant duration, and poor graft function may impair recovery of sexual/reproductive activity in these patients [14]. Sperm DNA integrity is a prerequisite for the accurate flow of genetic information. In this respect, sperm DNA damage may cause male infertility regardless of spermatozoa number, morphology, and motility [16]. Although the importance of sperm DNA integrity testing has been adequately demonstrated, there are many questions still to be answered concerning the origins of spermatozoa’s DNA damage.
In this study, the deficiencies in semen parameters of kidney transplant patients were shown. In these patients, the DNA damage amount of the spermatozoa can be interpreted as a considerable factor for unsuccessful reproductive treatment or infertility even if the sperm DNA fragmentation of the kidney transplant patients was not significantly higher compared to the controls (P = 0.09) [17]. For our patient population, the DNA fragmentation percentage was 17.8% ±14.1 in the transplantation group and 16.5% ±6.5 in the control group (P = 0.1), which was lower than the threshold value for infertility (20.05% by TUNEL assay) reported elsewhere [18, 19].
It has been suggested that there is no significant association between immunosuppressive drugs commonly used in kidney transplant patients and adverse effects on patient spermatogenesis or with teratogenic effects on their offspring [18]. Nevertheless, several studies have reported that some of these agents are potentially gonadotoxic with respect to their negative effects on testicular function and fertility [20, 21].
CsA is an immunosuppression enhancer for recipients of kidney transplants [22] and a potential gonadotoxic drug. CsA’s negative influences on reproductive capability have been demonstrated in vivo experiments. In rats, the CsA administration leads to seminiferous tubule degeneration and spermatogenesis impairment, which are unlikely to be secondary to the potential hepatic or nephrotoxic effects of the drug [23]. Moreover, CsA was associated with stimulation of oxidative stress and apoptosis mediation via reactive oxygen species in various cells [24].
Concerning Tac, sperm counts and motility dose-dependently decreased without observation of histopathological testicular injury [21] even though Tac is 50–100 times more potent than CsA [25]. When the drug treatment is stopped, the number of sperms together with motility can return to control levels [21]. In rats, however, spermatogenic damage and Sertoli cell-reduction exist in prolonged subcutaneous administration of Tac (30 to 60 days) [26].
Sirolimus may block spermatogenesis by interrupting the crucial stem cell factor/c-kit system through the rapamycin-sensitive PI3K/Akt/P70S6K/cyclinD3 pathway-inhibition [27]. Therefore, azoospermia/oligozoospermia and infertility may be observed in male kidney transplant recipients with sirolimus treatment [28, 29]. The abnormalities caused by sirolimus administration are similar to CsA but are more severe than those observed with the administration of Tac. Nevertheless, testicular toxicity and infertility by the sirolimus are potentially reversible [20]. In this respect, treatment changing from sirolimus to Tac significantly provides spermatogenesis improvement and the restoration of fertility in kidney transplant recipients after [28, 29].
AZA has been suggested to be genotoxic. It is frequently used in combination with CsA. Information on the effects of AZA on human reproduction is limited. Previously published papers suggest that prednisone might not be associated with sperm cell damage [30]. In addition, the incidence of neonatal malformations in pregnancies fathered by transplant recipients does not increase [15].
Combination therapy used in kidney transplant patients made it difficult to conclude which drug had a more detrimental effect on human spermatogenesis. In our group of patients, 34 patients were on the Tac+MMF+steroid treatment (12 had normozoospermia), five were on the Tac+AZA+steroid treatment (no patient had normozoospermia), 14 on the CsA+MMF+steroid treatment (four had normozoospermia), and three were on the MMF+sirolimus+steroid treatment (none had normozoospermia) (Table 3). There were no statistical differences between the groups regarding the effect of the drugs on spermatogenesis (P = 0.264).
Conclusion
In the present study, undesirable consequences of semen parameters in kidney transplant patients were observed. In this context, sperm motility and morphology were significantly lower in the patients group. Sperm DNA fragmentation of renal transplant patients was slightly higher than controls. Sirolimus impairs testicular function in male recipients of an organ transplant and three patients on sirolimus treatment had severe OAT in their ejaculate. Nevertheless, sperm DNA fragmentation rates were not significantly higher than the rest of the transplant group. FSH levels were significantly higher in the group treated with cyclosporin A + mycophenolate mo-fetil+steroid. Kidney transplantation is the best option for patients with severe kidney damage. Although it provides promising possibilities for the patients to restore their general health, it is worth noting that, some features of reproductive function might remain impaired. Although the difference between the renal transplant patients and control group was not statistically significant regarding sperm DNA fragmentation rate, infertility or unsuccessful assisted reproductive treatments may be partially explained by the DNA damage of spermatozoa. Furthermore, experimental designs with a large number of individuals may be required to confirm the present results and to obtain novel clinical aspects.
Footnotes
Acknowledgments
The data on some parts of the research has been presented as a poster presentation in American Urological Association (AUA) 2014 Annual Scientific Meeting, 16-21 May, Orlanda, USA.
Funding
This research was supported by the Uludag University Scientific Research Projects Centre (grant no. UAP (F) - 2011/75).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Consent to participate and publish
Written informed consent to participate and publish was obtained from all individual participants included in the study.
Compliance with ethical standards
All procedure performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with 1964 Helsinki declaration and its later amend-ments or comparable ethical standards.