
Abstract
BACKGROUND:
Limb-threatening ischemia is one of more important problem of fundamental and practice modern angiology. Despite the development of modern diagnostic and therapeutic approaches good results, Limb-Threatening Ischemia deserves special attention and occupies a special place among medical, biomedical and socio-economic problems. A comprehensive study will make it possible to develop new approaches, the result of which should be a decrease in the total number of diseases, as well as a minimization of complications leading to large-scale tissue losses and amputations.
OBJECTIVE:
We set out to develop a new non-invasive method for studying microcirculation in patients with limb-threatening ischemia.
METHODS:
We investigated control group and adults of both sexes (age: 50–75 years) with a confirmed diagnosis of the claudication. Men and women in ratio 1 : 1 in control and target groups.
RESULTS:
The research results showed that the original microcirculation coefficient calculated according to our algorithm in patients with intermittent claudication was 70% better than in the control group and 120% of patients were worse than in patients with Limb-Threatening Ischemia.
CONCLUSION:
Our research team created an original so called coefficient of microcirculation. In order to determine it, we studied the blood flow in the pulsations on the left and right side of the posterior tibial arteries of the legs at rest (names of lines SIN F, DEX F) and during post-ischemic hyperemia in the same lines. The study of microcirculation based on the microcirculation coefficient is very informative. The importance of this methodology for studying the total peripheral blood flow and arteriolar response is due to fundamental and clinical developments, as well as financial costs. Considering the technique described in the article can be easily mastered by medical personnel, it is easy to use in the inpatient and outpatient sectors, its use does not require large areas of the medical facility, the equipment is not expensive and the test itself does not cause inconvenience to the patient, then we can recommend including the described method is included in the list of functional diagnostic tests as a direct and quantitative method for determining microcirculation (without special costs on the part of medical institutions, insurance companies and the patient).
Introduction
Lower limb ischemia is one of the global problems related to blood circulation. The medical term “Limb-Threatening Ischemia” has been widely used in the literature and in clinical practice since 2010 [1–3].
The definition indicates and shows on the development of the risk of loss of tissue and limbs on the amid lack of blood circulation in the lower extremities. This may be due to blockage (occlusal) or narrowing of the arteries, which is the basis of oxygen starvation and deficiency of nutrients in tissues. This disrupts the robota and endurance of the muscles, accompanied by pain, atrophy of tissues and necrosis begins, which is ultimately the cause of deep inevitability and mortality.
Despite the development of modern diagnostic and therapeutic approaches with good results. Limb-Threatening Ischemia deserves special attention and occupies a special place among medical, biomedical and socio-economic problems.
A comprehensive study will enable new approaches to be developed, which should lead to a reduction in the overall number of diseases and minimize complications leading to major tissue loss and amputations. Limb-Threatening Ischemia is a collective term and can describe diseases with various pathogenesis at different stages. Atherosclerosis, thrombangiitis, endarteritis, diabetic lesions of blood vessels, etc. can provoke ischemia, which will lead to tissue loss. Due to different development mechanisms and the characteristics of the disease, there is no uniform information on the epidemiological situation in our country.
However, if we take into account that 3% of the population have a diagnosis of claudicatio and 5% of them can develop critical ischemia for 5 years, the frequency of critical ischemia is 300 cases per 1 million population per year. About 90% of all amputations are performed due to severe lower limb ischemia. 25% of patients with critical ischemia will require an amputation of the lower leg or thigh, so the incidence of critical ischemia will be 500–1000 patients per 1 million population per year. Critical ischemia is observed about five times more common in diabetics, and 10% of patients with diabetes develop trophic disorders in old age. In European countries, the number of amputations performed annually in patients with critical limb ischemia is on average from 180 to 250 cases per 1 million population [4–6]. In this context, the problem of the pathogenesis of clinical manifestations, diagnosis and treatment of patients are becomes extremely relevant.
Unfavorable epidemiological data elevate limb-threatening ischemia to a disease level that deserves special attention from basic and applied research.
It should be noted that the average age of patients with disabilities associated with limb-threatening ischemia falls within the pre-retirement population. Thus, in addition to the direct material costs, limb-threatening ischemia contributes to a reduction in the working-age population, which has an even more negative impact on healthcare in general. Due to the urgency of the problem and considering socio-economic factors, it is necessary to develop preventive measures aimed at studying the microcirculation. From our point of view, physical methods of studying microcirculation could detect the disease at the primary stage [7–9], which would reduce the percentage distribution of the disease in the population, and would also reduce the percentage of severe disability and mortality in a cohort of people with arterial insufficiency [10–12].
Irrespective of the mechanism involved in the development of limb-threatening ischemia, there is a decrease in perfusion pressure and blood flow occurs in the distal part of the affected limb as a result of hemodynamic, biochemical and hematological disturbances. Due to the stenosis or occlusion of the main arteries, the blood flow is so small that the presence of compensatory mechanisms (mainly collateral blood flow) does not help and severe microcirculatory disorders develop in the distal segments of the limb develop. Reduced capillary perfusion is due to the collapse of precapillary arterioles (irreversible dilatation) at low transmural pressure. Arteriolar vasospasm and microthrombosis develop, then, as a result of interstitial edema and swelling of endothelial cells, capillary occlusion develops, aggregation of blood cells increases, their rigidity increases and local components of the immune system are activated [13]. In addition to rheological disturbances, there is a violation of the coagulation/anticoagulation mechanism. Fibrinogen, prothrombin and fibrin degradation products increase with a tendency to fibrinolysis deficiency due to increased plasma levels of tissue plasminogen activator inhibitors. Endotoxicosis develops, which, against the background of pronounced rheological disturbances, leads to irreversible blockage of the microvasculature in the distal parts of the limb, and primary gangrene develops. Thus, the role of the microcirculation is dominant in the development of limb-threatening ischemia. One of the decisive factors in the unfavourable treatment for limb-threatening ischemia is the late presentation of patients to the doctor, the severity of the initial condition, and the presence of severe concomitant pathology. In this regard, it is important to develop methods for studying the microcirculation in order to determine predisposition to the disease at an early stage.
From our point of view, physical methods of studying the microcirculation could detect the disease at the primary stage, which would reduce the percentage distribution of the disease in the population, and would also reduce the percentage of severe disability and mortality in a cohort of people with arterial insufficiency. There is a recommended algorithm for diagnosing limb-threatening ischemia. It includes a medical history, a clinical examination, and the use of physical and instrumental tests. One of these is Doppler ultrasound of the affected arteries and measurement of the ankle brachial index. Doppler ultrasound of the arteries shows impaired blood flow in the affected arterial pathways, assessing the lesions and the degree of stenosis. The ankle-brachial index is a measurement obtained by dividing the systolic blood pressure by the pressure recorded in the upper arm. Systolic blood pressure is measured at the patient’s ankle just above the ankle. In chronic arterial insufficiency of the lower limbs, the value of the Ankle-brachial index changes heterogeneously. This is due to different degrees of damage to the left and right limbs [14]. The informative value of such studies is undeniable, but the assessment of microcirculation requires more attention.
Another technique used to assess the condition of the lower extremities in arterial insufficiency is photoplethysmography, which is based on the measurement of the blood volume in the microvascular bed of the tissue. The intensity of the transmitted radiation depends on the amount of blood located between the receiver and the source (see Fig. 1). The wavelength of the emitted light, 980 nm, is chosen so that the main absorption occurs by red blood cells in the arterial section. The signal therefore depends on the number of red blood cells, i.e. on the local concentration of red blood cells (local hematocrit) entering the area between the source and the receiver. The gradient of changes in hematocrit during one measurement is small and the intensity of the light recorded by the receiver is inversely proportional to the volume of blood located in the lumen area. This method is more informative from the point of view of assessing microcirculation, because it determines the correlation between the quality of the blood flow and the hematocrit, which is in principle, is one of the constitutive links of microcirculation. However, this method does not capture the nature of erythrocyte aggregation and deformation, which determine the laminarity of the blood circulation that should be present in the lower extremities.
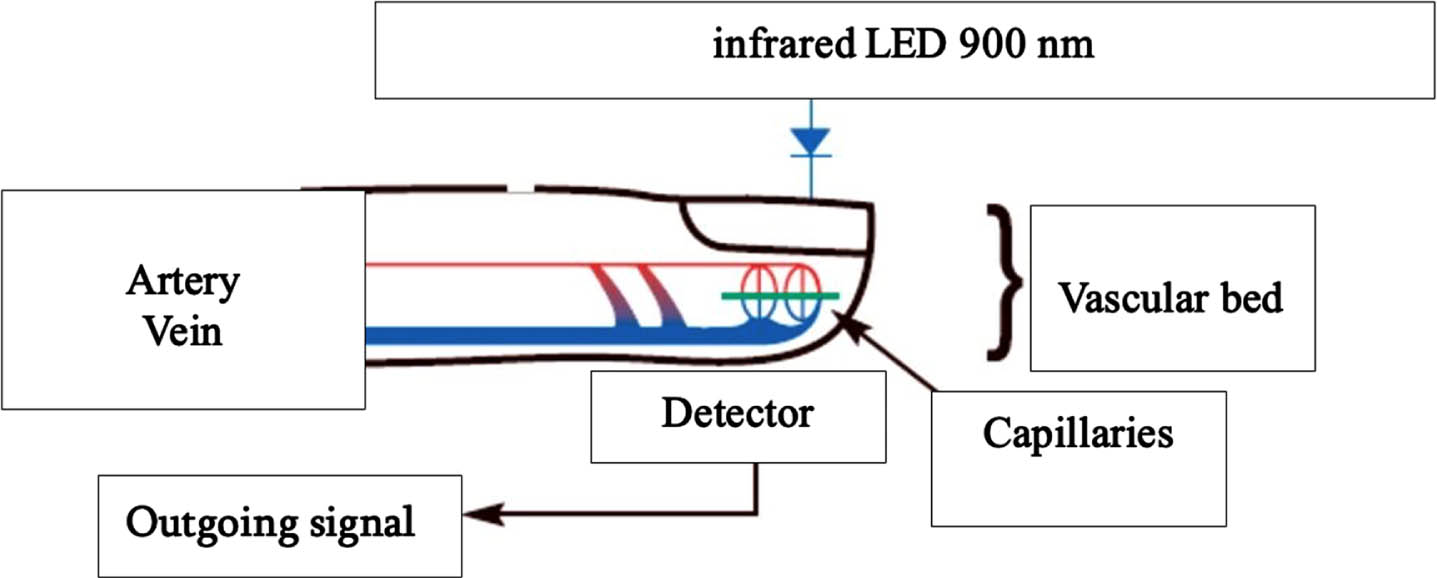
Scheme of photoplethysmography.
Another method used to plan surgical interventions for the treatment of limb-threatening ischemia is radiocontrast aortoarteriography. The principle of this method is to scan the abdominal aorta. The introduction of radiocontrast and the acquisition of a series of x-rays of the arterial bed of the lower extremities is the essence of the method [1]. Due to its deep invasiveness, high cost, and special requirements for the material and technical base of a healthcare institution, as well as for the medical staff, this method cannot be considered as easily accessible.
Despite the uniqueness of X-ray contrast aortoarteriography for assessing microcirculation in patients with limb-threatening ischemia, it is unacceptable [15]. Adequate methods must be used for screening activities. The adequacy of a research method is the selection of a strategy that can most accurately answer the quantitative and qualitative question about the phenomenon under study, using more direct and faster links than others.
Appropriate methods needs to be used for screening activities. The appropriateness of a research method is the selection of a strategy that can most accurately answer the quantitative and qualitative question about the phenomenon under study, using more direct and faster links than others [16]. Despite the uniqueness of X-ray contrast aortoarteriography for assessing microcirculation in patients with limb-threatening ischemia, it is unacceptable.
We set out to develop a new non-invasive method to study the microcirculation in patients with limb-threatening ischemia.
Health control
Healthy adults of both sexes (age: 50–75 years) without concomitant diseases with normal blood pressure and with a normal body mass index (men and women in a ratio of 4 : 5). n = 9.
Patients
Adults of both sexes (age: 50–75 years) with a confirmed diagnosis of the claudication. n = 18. (Men and women in the same ratio of health control. Inclusion criteria of patients: these are adults of both sexes (age: 50–75 years) with a confirmed diagnosis of the claudication without concomitant diseases with normal blood pressure and with a normal body mass index (men and women in ratio 4 : 5). Exception criteria of patients: these are adults of both sexes (age: >75 years) with limb-threatening ischemia, Ischemic rest pain with confirmatory hemodynamic studies; diabetic foot ulcer or any lower limb ulcer present for at least 2 weeks; gangrene involving any part of the lower limb or foot; specifically excluded are patients with pure venous ulcers, pure traumatic wounds, acute limb ischemia (symptoms present for 2 weeks or less), embolic disease, and non-atherosclerotic chronic vascular conditions of the lower extremity (e.g., vasculitis, Buerger’s disease, radiation arteritis). Male to female ratio 1 : 1. This is first patient group – target group. We investigated second patients’ group for comparative control for target group. These are adults of both sexes (age: >75 years) with limb-threatening ischemia, Ischemic rest pain with confirmatory hemodynamic studies; diabetic foot ulcer or any lower limb ulceration present for at least 2 weeks; gangrene involving any portion of the lower limb or foot; patients with pure venous ulcer, pure traumatic wounds, acute limb ischemia (symptoms present for 2 weeks or less), embolic disease, and non-atherosclerotic chronic vascular diseases of the lower extremity (e.g., vasculitis, Buerger disease, radiation arteritis). n = 12 (male to female in ratio 1 : 1).
Methods
Our research team created an original so called coefficient of microcirculation. In order to determine it, we studied the blood flow in pulsations on the left and right sides of the posterior tibial arteries of the legs at rest (names of the leads SIN F, DEX F) and during post-ischemic hyperemia in the same leads.
The studies were carried out using Doppler device sensors with an original scheme (Fig. 2). The Doppler effect consists of a specific change in the frequency of ultrasound vibrations depending on the speed of the source of sound vibrations, where the source is red blood cells. The diameter of the red blood cell does not exceed 7 microns in the absence of hematological pathologies. Depending on the calibre of the vessels, the blood flow has different velocity profiles. Red blood cells determine the velocity profile, and depending on the contour of the shear vectors with different velocities (Magnus effect), the movement profile of the erythrocytes changes and the movement of the erythrocyte membranes is undulated into a continuous flow. By directing the ultrasound signal to the tibial arteries (SIN F, DEX F), at an angle of 45° we record the reflection of this signal by the red blood cells of the flowing blood, and by the frequency shift of the incident and reflected signals we determine the linear speed of the blood flow in the corresponding resistive arteries formed during the branches of this artery. (In some articles we meet definition of resistance arteries, that is the same of resistive arteries [17–19].
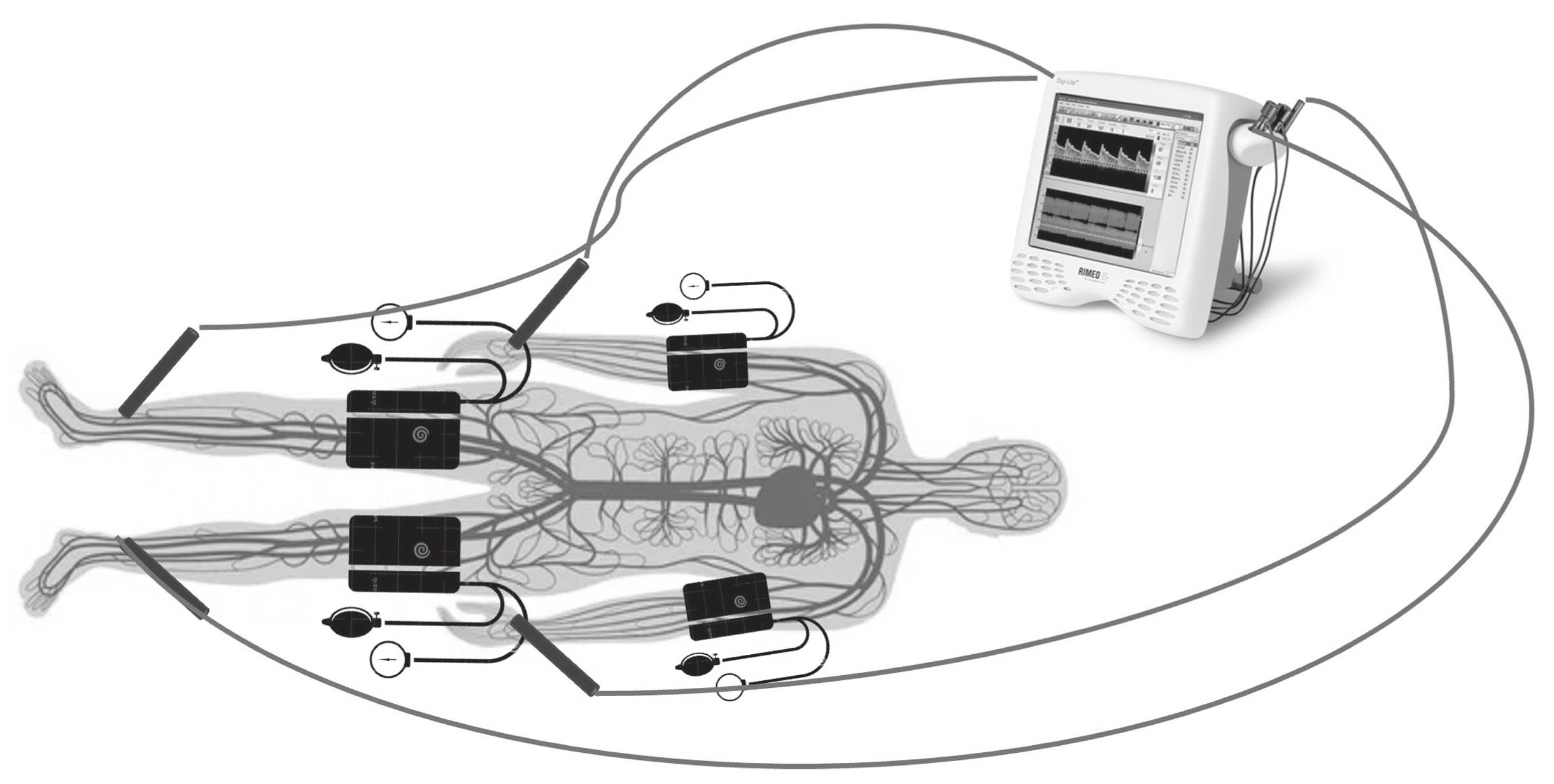
Scheme of study of microcirculation.
The blood flow velocity measured in the resistive arteries depends on the state of the corresponding resistive arteries formed during their branching. The dynamics of changes in blood flow velocity in the posterior tibial arteries in the leads after post-ischemic hyperemia can be used to assess the state of the branching of the resistive arteries and the blood supply to the microcirculation. Experimental ischemia was induced by compression of the brachial and patellar arteries (Fig. 2). The blood flow trace in one of the leads has three different fragments: resting state – normal (background) blood flow, ischemia – absence of blood flow, post-ischemic hyperemia – increased blood flow (Fig. 3). The blood flow velocity curve was processed using analogue texture analysis routines (Tas-Plus, Leitz) [16].
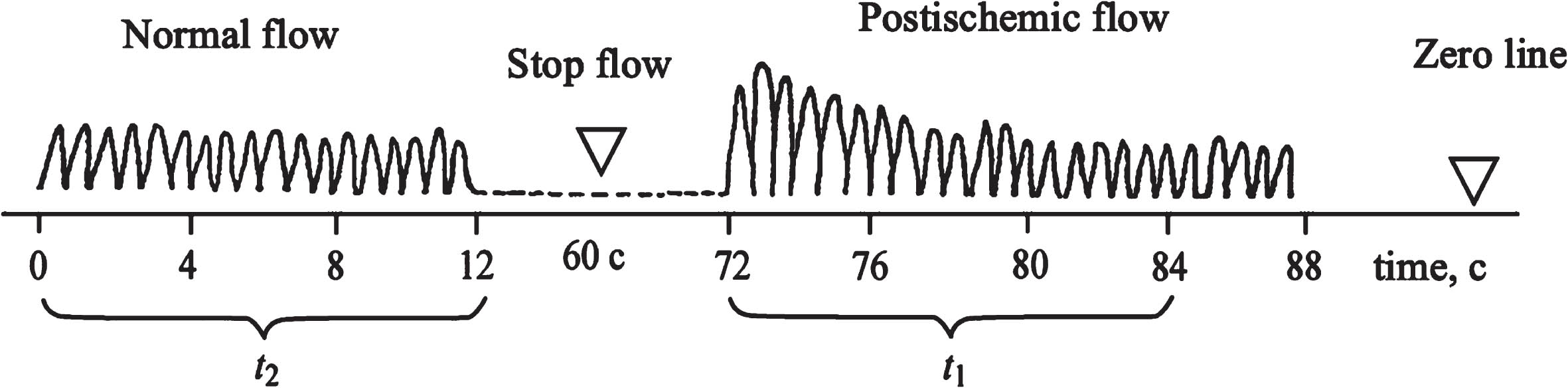
Scheme of the linear blood flow curve in one of the leads.
To develop the technique, we used an ultrasound device “Dop 8/4” (Germany) with four inputs. To record normal (background) blood flow, the sensor was placed in the area of good audible pulsations on the wrists and medial ankles, and the pressure in the sphygmomanometer cuffs placed on the brachial and patellar arteries was increased to stop blood flow. 60 sec after compression and evacuation of the air from the cuff, the pressure in the cuff dropped to zero and post-ischemic reactive hyperemia developed. Blood flow recording continued until the rate of increased blood flow was restored.
In leads SIN F, DEX F, which correspond to the left and right pulsation points on the feet, normal background linear blood flow was recorded in the form of a curve on the recorder. Background volumetric blood flow is equal to the sum of discrete velocity values, which takes all points of the curve during the time interval t. Therefore, volumetric blood flow in lead SIN F is equal to ∑V1t, in lead DEX F – ∑V2t. The average background blood flow is equal to the total background blood flow divided by 2, i.e. ∑∑Vit/2 = (∑V1 +∑V2+) * t/2, where t is the time interval at which phonoscopic blood flow is recorded. Total postischemic hyperemia is the sum of the increased volumetric blood flow in two leads SIN F, DEX F: ∑∑Viposttipost, where Vipost is the increased linear velocity during postischemic hyperemia, tipost is the time interval at which the increased linear velocity during postischemic hyperemia reaches normal background values [15]. To describe the reactions of resistive arteries in both leads, which control peripheral resistance and microcirculation, we introduced the microcirculation coefficient k, which is the ratio of the total post-ischemic blood flow to the average value of the volumetric background blood flow: k = Spost/Sbackground =∑∑Viposttipost/∑∑Vit.
After a series of aromatical transformations, we get: k = 2(∑V1t1 +∑V2t2)/(∑V1 +∑V2)t, where t1, t2 are the time intervals at which the increased post-ischemic blood flow in different leads returned to normal background values. [k] = 2∑Viposttipost/∑Vit., k – is original coefficient of microcirculation.
This method, due to its non-invasiveness, has a number of advantages. The non-invasiveness of the methods is one of the decisive features for evaluating the technique [19].
An analysis of arithmetic mean, standard deviation and t-Student’s criteria calculated using Origin 8.1 (Micro Soft., 2023).
All subjects were informed of their inclusion in the study. Informed consent was signed. The Ethical Committee of the Society of Rheologists granted permission for the research protocol (405133029_2, May 29, 2023).
Results
The research results showed that the initial microcirculation coefficient calculated according to our algorithm in patients with intermittent claudication was 70% better than in the control group and 120% of patients were worse than in patients with limb-threatening ischemia (see Table 1).
Mean of coefficient of microcirculation in control group, patients with claudication and with Limb-Threatening Ischemia. M±m
Mean of coefficient of microcirculation in control group, patients with claudication and with Limb-Threatening Ischemia. M±m
It was found out that the microcirculation coefficient of the patients was significantly different from that of the control group and corresponded to the clinical manifestation of the disease.
As we can see from the results, even such a seemingly harmless disorder as intermittent claudication already causes a change in the microcirculation coefficient, and in case of serious disorders, the change in the microcirculation coefficient is critical.
Intermittent claudication occurs when there is insufficient oxygen supply to meet the metabolic demands of skeletal muscle. Intermittent claudication is a common manifestation of peripheral arterial disease which includes atherosclerotic narrowing of arteries in the extremities. Although this condition is not critical, it is the background to more complex diseases that directly lead to limb-threatening ischemia [21–29].
That is why we consider two different diseases to illustrate the changes in the microcirculation, in order to confirm the validity of the original coefficient, the calculation of which we describe in this paper.
This difference is due to the fact that as the arterial bed branches, the number of vessels connected in parallel and in series-increases exponentially. Small branches of the arterial network (small-caliber intra-organ arteries, arterioles) form the resistive part of the vascular bed, where the greatest pressure drop in the circulatory system occurs, and the blood flow loses its pulsating character. In the walls of these vessels there are many smooth muscle cells that actively change the vascular lumen, which significantly affects the peripheral resistance to blood flow. Smooth muscles of resistive vessels regulate tissue blood flow by responding both to signals originating in the tissues and circulating in the blood, and to signals arriving along nerve fibers [17]. The microcirculation coefficient calculated by us is responsible for the functional state of resistive arteries.
Located at the atomic boundary between the venous and arterial segments, resistive arteries, being similar to certain circulatory taps, ensure the transfer of blood to the peripheral segments [21–29]. The functional state of the resistive arteries depends on the endothelial factor, and the elasticity of the vessels determines the tone of the resistive arteries. Resistive arteries are responsible for the intravascular state of the blood, and also play an indirect role in angiogenesis, in ensuring the relative parallelism of coagulation/anticoagulation, constriction/dilatation. Normal blood supply to all organs and tissues, the constancy of the level of total blood pressure is largely due to the peripheral resistance of the circulatory system, for which resistive arteries are responsible. Resistive arteries are involved in the development of compensatory and pathological processes in the regional circulatory system and microcirculation. The aim of our work was to study resistive arteries as a diagnostic marker of the microcirculation in patients with limb-threatening ischemia.
Microcirculation is a complexly organized system that ensures the orderly movement of blood, lymph, tissue fluids, and the absorption and release of biochemical substrates, metabolites, and physiologically active substances. It is the state of microcirculation that most determines the value of total peripheral vascular resistance; in this regard, microcirculation is a potential diagnostic target. Small arteries and arterioles play a major role in providing resistance to blood flow belongs to. Remodelling of resistive vessels, including media hypertrophy, wall thickening and reduction of vascular lumen, is associated with stabilization of microcirculatory disorders. Structural and functional changes are manifested by increased vasoconstriction and decreased vasodilater capacity, caused by a decrease in the synthesis of vasodilating substances and/or an increase in the production of vasoconstrictive substances. In increasing the resistance to blood flow in the microvasculature, a decrease in the density of arterioles per unit of tissue is also important [27, 28].
Microcirculatory disorders play a major role in the occurrence and development and progression of target organ damage and increase the risk of developing ischemic diseases [6].
To slow down the rate of progression of target organ damage, there is an urgent need to obtain objective data on the state of microcirculation.
In this regard, we introduced the concept of the microcirculation coefficient, which logically determines the degree of reaction of resistive arteries to regulate blood flow velocity, and a mathematical calculation identifies the functional state of resistive arteries with the percentage of increased blood flow during post-ischemic (reactive) hyperemia to background blood flow (normal blood flow without influence).
The continuous movement of blood through vessels of different structure and function can generally be represented as arterial and venous segments communicating through an extensive network of microvessels. Obviously, assessment of the microcirculation is particularly relevant to the pathogenesis, prevention, treatment and prognosis of limb-threatening ischemia. The coefficient of microcirculation depends on the violation of the thickness, structure and shape of the vessel, which affects the permeability of the vessel and the transcapillary exchange. The level of microcirculation is the key in the cardiovascular system, while the other levels are designed to ensure its main function – transcapillary exchange. Blood with dissolved oxygen and nutrients necessary for tissue metabolism is transported from the vascular space to the capillary system [6]. This process follows the laws of diffusion and is determined by the gradient of intra- and extravascular hydraulic pressure and the gradient of intra- and extravascular oncotic pressure, which ensure fluid retention in the vessels and return of interstitial fluid. The ratio of these gradients is the basis for the diffusion of fluid in the arterial part of the capillary and its reabsorption in the venous part. The oncotic pressure of the blood is relatively constant under normal conditions. Therefore, is capillary hydrostatic pressure is the determinant of the intensity of transcapillary exchange and the supply of nutritients to tissues [4, 5]. The remaining parts of the cardiovascular system are responsible for establishing and maintaining hydrostatic pressure [1, 4].
Therefore, the method we propose for assessing microcirculation is very important, as it allows resistive arteries to be studied in two parallel lines. During working hyperemia, against a background of dilation of resistive vessels and an increase in blood flow rate, capillary blood pressure increases with increased blood filtration accompanied by an increase in hematocrit, which ensures the supply of tissues with the required amount of oxygen. Under resting conditions, an increase resistive vessel tone is accompanied by a decrease in blood flow, a decrease in capillary pressure, increased reabsorption of tissue fluid, a decrease in hematocrit and the conversion of some capillaries into plasma capillaries – “blind”. Hydraulic pressure in capillaries does not always reflect system pressure. In pathological cases, it may change independently of changes in blood pressure levels [27, 28].
Dilatation of the arterioles leads to an increase in capillary pressure even in the presence of reduced blood pressure, with consequent increase in extravasation and blood thickening increase with progressive impairment of peripheral circulation. If, under normal conditions, the level of capillary pressure is related to the tone of the pre-capillary resistive vessels that regulate blood flow, in pathological cases the difficulty of blood outflow from the capillaries due to contraction or mechanical compression of the post-capillary drainage vessels – venules and veins – is of crucial importance. On the basis of these fundamental laws, we have determined the microcirculation using a new technique which makes it possible to estimate the microcirculation coefficient.
The microcirculation coefficient is equal to the percentage of the increased post-hyperemic blood flow in four leads simultaneously to the average background blood flow in the period of time that is required to transform the peaks of the blood flow curve into the discrete harmonic function of the blood flow wave.
The need to evaluate the peripheral system is dictated by the active involvement of the microcirculation in the development of diseases caused by congestion and spasm. All physiological processes, and even more so pathophysiological phenomena, develop at the level of the microcirculation. Therefore, considering the microcirculation as a diagnostic and therapeutic focus will provide an opportunity to study the problem, which will help to plan new preventive approaches through the introduction of new screening programmes.
Conclusion
The study of microcirculation based on the microcirculation coefficient is very informative. The importance of this methodology for studying the total peripheral blood flow and arteriolar response is due to fundamental and clinical developments, as well as financial costs. Considering that the technique described in the article can be easily mastered by medical personnel, it is easy to use in both in-patient and out-patient settings, its use does not require large areas of the medical facility, the equipment is not expensive and the test itself does not cause inconvenience to the patient, then we can recommend including the described method is included in the list of functional diagnostic tests as a direct and quantitative method for determining microcirculation (without special costs for medical facilities, insurance companies and the patient).
Based on the study of the microcirculation coefficient, it is possible to diagnose the blood supply of organs and tissues, adjust treatment tactics, and implement preventive measures. It is necessary to continue population studies that will allow us to better understand the pathogenesis of various types of circulatory pathologies, as well as using the technique to study diseases associated with dysfunction of resistive arteries.
Conflict of interest
None to report.