
Abstract
The reform of public hospitals is a complex process, involving multiple subsystems and the interaction of related factors. This paper conducts a preliminary evaluation of the joint reform of medication, medical care, and medical insurance in Sanming using quantitative and qualitative methodologies. The method of system dynamics is applied to model the three subsystems of medication, medical care, and medical insurance in Sanming and analyze the cause-and-effect relationship between different factors in the subsystem. Based on the analysis, the evaluation index is determined to evaluate the effect of the medical reform in Sanming. The analysis results show that Sanming’s public hospitals have experienced a comprehensive reform that includes changing the way pharmaceuticals are procured, cutting prescription prices, and raising hospital worker wages. To maximize the hospital revenue structure, the medical insurance payment system was changed. The expense of patient therapy was reduced, and the development of hierarchical diagnosis and treatment was encouraged.
Introduction
In China’s medical and healthcare services system public hospitals are the main body and carriers to provide medical services [1, 2]. From 2010 to 2018, China’s GDP increased by 156.3%, and the number of public hospitals in China increased by 157.8%. At the same time, the average total income of each hospital increased by 236.84%, and the average total costs of each hospital increased by 242.65% [3]. In this context, there were many problems in China’s public hospitals, such as the imbalance between low medical service charge and high pharmaceutical price. By the end of 2020, there had been 16804 county-level hospitals in 2844 counties (or county-level cities), providing services for more than 700 million county residents (50% of the country’s total population) [4, 5]. On the basis of the new healthcare reform in 2009, the government has successively issued relevant documents and policies to emphasize the importance of the comprehensive reform on county-level public hospitals so as to improve hospital efficiency [6]. County-level public hospitals are the center of the medical and health service system of the whole county, and they are the core component of the rural three-tier medical and health service network [7].
In May 2015, on the basis of pilot cities, the State Council of China issued the “Opinions on Implementing Thorough Promotion of Comprehensive Reform of County-Level Public Hospitals”, aiming to break the status quo of doctors’ income depending too much on drug commission. The reform focuses on the management system, operation mechanism, medical service price, salary of medical personnel, and medical insurance payment [8]. So far, many problems have occurred because of the discrepancies of medical level, population and economy among different provinces, as well as the short reform time in most county-level public hospitals [9, 10].
In this paper, the methods and experience of county-level public hospital reform in Sanming were summarized in order to provide a reference for public hospital reform in China and other developing countries.
Background
In 2011, the employees’ medical insurance pooling fund of Sanming, Fujian Province, failed to offset its expenditure, with a loss of 200 million yuan, accounting for 14.42% of the fiscal revenue of the year. Since February in 2012, Sanming had taken the lead in carrying out a comprehensive reform of county-level public hospitals and explored the interaction among medication, medical service and medical insurance. In just one year, Sanming turned the medical insurance fund from deficit to profit. Since the medical reform, the quality of medical services in Sanming’s public hospitals has progressively improved. The total inpatient mortality rate decreased from 0.46% in 2011 to 0.03% in 2020; the total inpatient mortality rate of surgical patients decreased from 0.17% in 2011 to 0.01 percent in 2020; the resuscitation success rate for patients with acute and critical illness increased from 91.98% in 2011 to 96.88% in 2020; from 14,116 in 2014 to 37,089 in 2020, the number of Class III and IV procedures has increased. In March 2021, when inspecting the medical reform in Sanming, General Secretary Xi Jinping of the CPC Central Committee reiterated: “The people’s health is a powerful emblem of socialist growth.” Sanming’s medical reform is a symbol of the people’s power and the fortitude to be the first. In light of local conditions, its experience is worth learning for other cities.” The “Deepening Medical and Health System Reform 2021 Key Work Tasks” was issued by the General Office of the State Council in June 2021, requiring further promotion of Sanming’s medical reform experience, accelerating the linkage reform of the medical service, medical insurance, and medication system, including promoting centralized procurement of drugs and consumables, deepening the reform of medical service prices and personnel salary system, and promoting the reform of mediclaim [11]. In November 2021, the National Health Commission issued the Notice on the Promotion of Experience in the Construction of Hierarchical Diagnosis and Treatment and Medical Consortium in Sanming, summarizing experience in the pilot construction of hierarchical diagnosis and treatment and medical consortium in Sanming [12].
System dynamics analysis of Sanming’s medical reform
The cause-and-effect diagram analysis method from the system dynamics theory is used in this work to analyze Sanming’s medical reform in great detail. Vensim is used to create three subsystems for medical care, medical insurance, and medication. System dynamics is a computer simulation tool that can study causality. This tool has been widely applied in the field of medical research [13, 14, 15, 16, 17]. Therefore, it is suitable for exploring the interaction among these three systems. To provide experience and recommendations for other regions seeking to advance medical reform, this paper investigates the hierarchical diagnosis and treatment system in Sanming from three perspectives: medical care, medication and medical insurance.
Medical care system
The enhancement of the hierarchical diagnostic and treatment system is an essential goal of Sanming’s medical care reform, and the adoption of associated measures is advantageous. Seven feedback loops make up the medical care subsystem (Fig. 1).
Feedback loop 1: Government financial subsidy
Feedback loop 1 shows that the government’s financial support for primary care creates a positive feedback loop by enhancing the efficiency of primary care and encouraging patients to remain there. It in turn stimulates the government to increase financial support for primary care.
Feedback loop 2: Family doctor contracting service
Feedback loop 3: Medical effects of primary care
Family doctor contracting services are at the center of feedback loops 2 and 3. Feedback loop 2 shows that the adoption of family doctor contracting services in primary care not only raises the pay levels and motivation of primary care doctors but also raises the caliber of their medical care, which contributes to better primary care outcomes and increases resident motivation to select family doctor contracting services. Feedback loop 3 demonstrates that as the primary care effect improves, residents are more likely to sign up for family doctor services, which increases the primary care doctors’ workload and leads to better family doctors’ medical care, which in turn improves the primary care effect for the residents.
Feedback loop 4: Remuneration level of primary care doctor
Feedback loop 5: Medical effects of primary care
Feedback loops 4 and 5 show how raising primary care physicians’ compensation levels will help them practice medicine at a higher level, which will enhance the overall effect of primary care and make patients more willing to be referred to primary care institutions for follow-up rehabilitation and other services. This will increase the downtime between visits for primary care institutions, which will increase the downtime between visits for supplementary care institutions. As a result, the rate of downward referrals will rise, medical resources will be better utilized, and the issue of patients only wanting to receive treatment at large hospitals will be reduced. As more patients go to the primary care level, the workload of primary care doctors increases and the level of pay and medical care can be further improved.
Feedback loop 6: Public hospital doctor workload
Feedback loop 7: Remuneration level of public hospital doctor
Feedback loops 6 and 7 demonstrate that when the payment system for public hospital physicians is changed and the cost of medical services is raised to match, it helps to increase public hospital physicians’ motivation, which in turn leads to an increase in the effectiveness of public hospital care, which in turn leads to an increase in the volume of public hospital care, which not only increases doctors’ compensation.
The cause-and-effect diagram of medical care system.
The medication reform of Sanming initiatives were successful and have started to spread to other areas. They have also contributed to the promotion of the hierarchical diagnostic and treatment system (Fig. 2).
Feedback loop 1: Breaking “Medicines Maintain Medical Institutions” system
Feedback loop 2: Breaking “Medicines Maintain Medical Institutions” system
Feedback loops 1 and 2 demonstrate how Sanming has reduced drug prices through zero-rate sales, joint price limit procurement, and the “two-ticket system” for drug procurement, breaking the aberration of “drugs to subsidize medical care” and lowering the number of drug rebates that primary care doctors and other healthcare providers receive. This will lessen the situation where primary-care doctors get drug rebates and primary care facilities depend on pharmaceuticals for their revenue. We can fairly compensate primary care doctors’ pay levels, eliminate the gray income of doctors receiving drug rebates, increase the sunshine income from providing medical services, and encourage the dismantling of the profit-seeking nature of the medical field by increasing the medical income of primary care doctors and the associated financial subsidies.
The cause-and-effect diagram of medication system.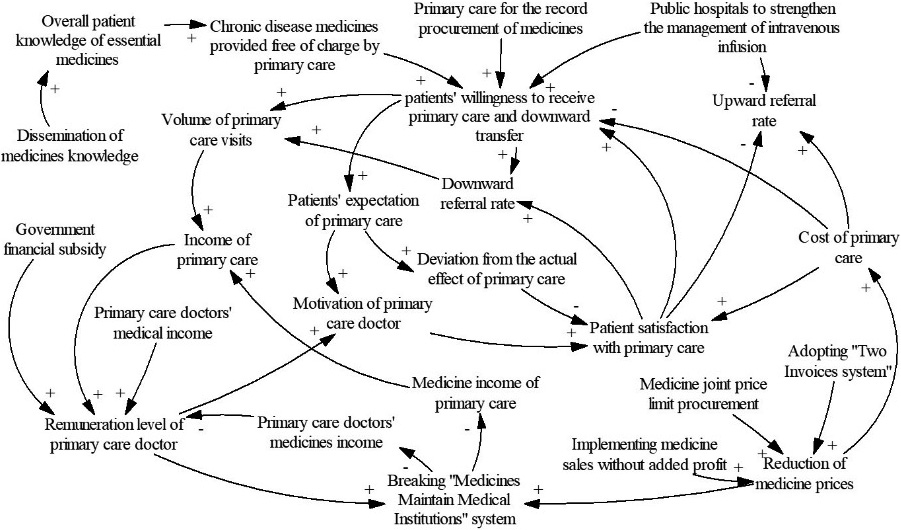
The cause-and-effect diagram of medical insurance system.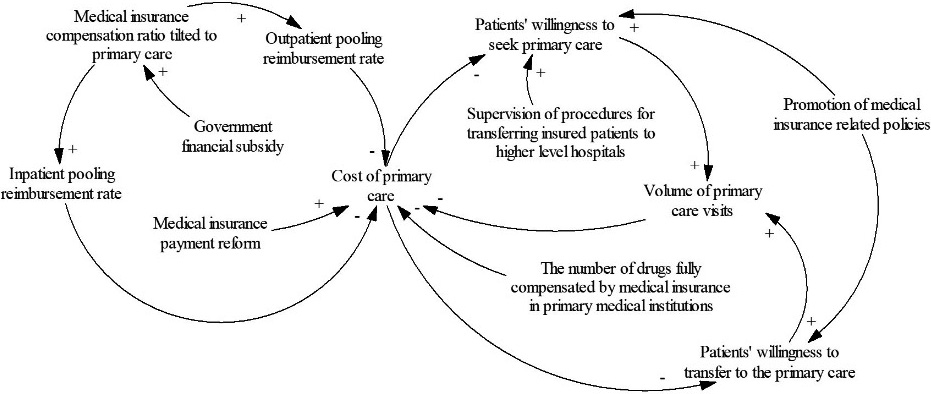
The implementation of the hierarchical diagnosis and treatment system in Sanming has benefited from the reform of the medical insurance (Fig. 3).
Feedback loop 1: Cost of primary care
Feedback loop 2: Cost of primary care
Feedback loops 1 and 2 indicate that the greater the overall number of primary care visits and the lower the average cost of primary care per patient are all index of reduced primary care costs, which will aid in directing patients toward primary care from an economic standpoint.
Evaluation index
Problems in the public hospital reform in Sanming were divided into three aspects: drug management, medical system and medical staff salary structure, and medical insurance payment mode.
Table 1 shows the index for evaluating the impact on drug management of county-level public hospitals, to control the rapid growth of medical expenses and prevent doctors from receiving commission from pharmaceutical sales.
Evaluation index on drug management of county-level public hospitals
Evaluation index on drug management of county-level public hospitals
Table 2 shows the index for evaluating the impact on medical service prices and salary system of county-level public hospitals to improve the income of medical staff and the income structure of hospitals.
Evaluation index on medical service prices and salary system of county-level public hospitals
Table 3 shows the index for evaluating the impact on the medical insurance payment mode to reduce the expenditure of medical insurance funds and promote the hierarchical diagnosis and treatment system.
Evaluation index on medical insurance payment mode of county-level public hospitals
Located in the central mountainous area of Fujian Province, Sanming is a predominantly industrial city with a population of 2.59 million (Fig. 4) [18]. Since 2012, Sanming has issued more than 200 medical reform policies [19]. In 2020, a satisfaction survey of public hospitals were conducted, whose results indicates that the satisfaction of discharged patients and hospital staffs in Sanming ranked 2nd in Fujian Province [20]. In 2019, Sanming had a GDP of 260.156 billion yuan, ranking 6th in Fujian Province. The per capita GDP was 100,800 yuan, ranking 5th in Fujian Province. Sanming has two districts, one county-level city and nine counties. For this study, we selected 22 county-level public hospitals in Sanming. The Sanming government website, Sanming Health Statistics Yearbook, and China Health Statistics Yearbook were used to compile relevant data.
The population of Sanming by district in 2019.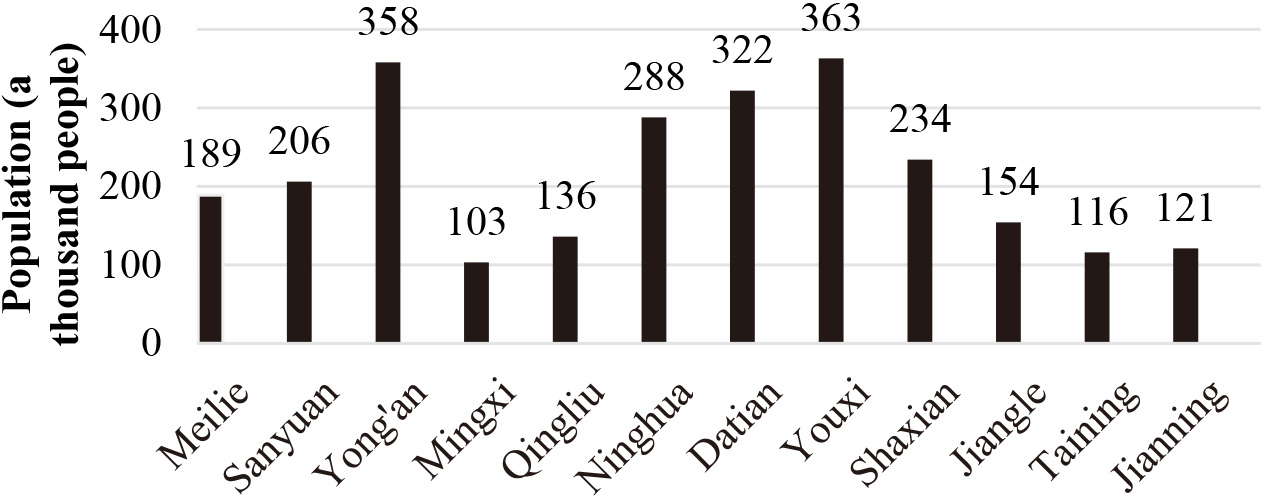
In this paper, the information and data were mainly from the Sanming’s government website and Health Statistics Yearbook of China from 2012 to 2021. Face-to-face interviews and questionnaires were also used to collect information. 300 prescriptions in the first Monday of June 2016 and the first Monday of June 2019 were selected randomly from four county-level public hospitals, with an average of 75 prescriptions per hospital. The proportion of prescriptions involving intravenous infusion drugs was calculated. On the basis of the proportion, it is verified whether the improvement had been made regarding the over-treatment and overuse of drugs.
Reform of county-level public hospitals in Sanming had made the following achievements.
In the medication reform in Sanming, the primary policy for reducing drug prices was the “two invoice system” which means one invoice will be issued when drugs are sold by a pharmaceutical factory to a first-class distributor, and another invoice will be issued when the distributor sells the drugs to a hospital. In this way, constant addition to drug prices can be prevented in the circulation link, and the source of drugs can be traced, which prevents counterfeit drugs from flowing into hospitals. In order to guarantee the smooth implementation of the two invoice system, “whether the hospital receives drug rebate” was incorporated as an indicator for assessing the annual salary of hospital presidents.
In 2016, Sanming Alliance for Joint Purchase of Drug Consumables at Limited Prices (hereinafter referred to as “Sanming Alliance”) was established to ensure the smooth implementation of the limited price purchase of drugs in medical institutions. Sanming Alliance integrated joint procurement, transaction, settlement and supervision processes into a platform which provides various procurement services, covering drugs, consumables (including reagents), and Chinese herbal pieces. It is the first cross-regional joint procurement platform for centralized drug purchase. In 2020, Sanming alliance successfully completed the volume-based procurementof seven drugs non-consistency evaluation. Compared with the prices of generic drugs in use in all participating cities, the overall average decrease was 69.52%, and the maximum decrease of a single variety was 91.63%. Compared with the prices in Sanming, the average decrease was 49.83%, and the maximum decrease was 72.84%. It was estimated that 124 million yuan of drug expenses would be saved every year based on the agreed purchase volume [21].
Changes in drug income, outpatient and inpatient medical expenses per time in 22 county public general hospitals
Changes in drug income, outpatient and inpatient medical expenses per time in 22 county public general hospitals
Comparison of outpatient expenses increase among public hospitals in Sanming, Fujian Province and China.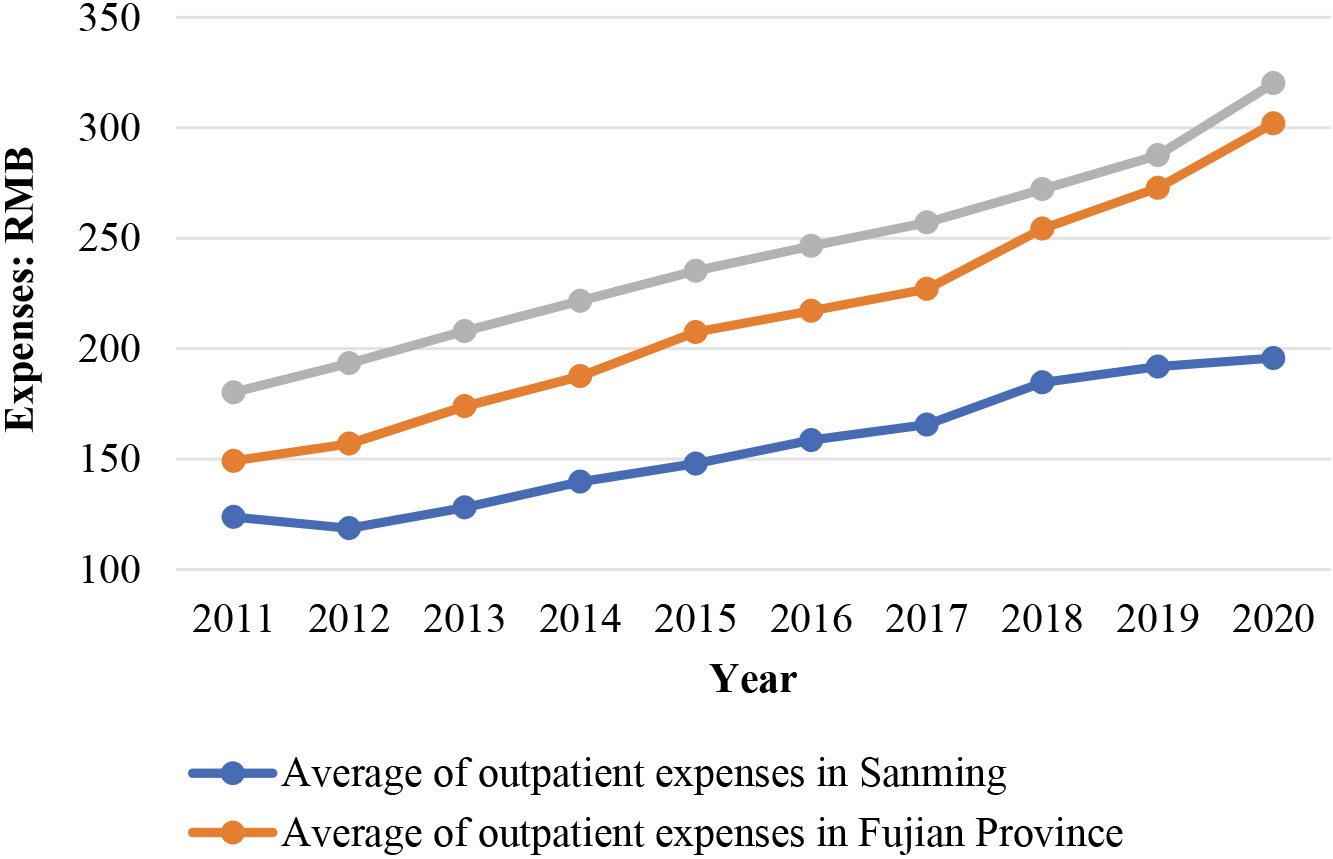
Comparison of inpatient expenses increase among public hospitals in Sanming, Fujian Province and China.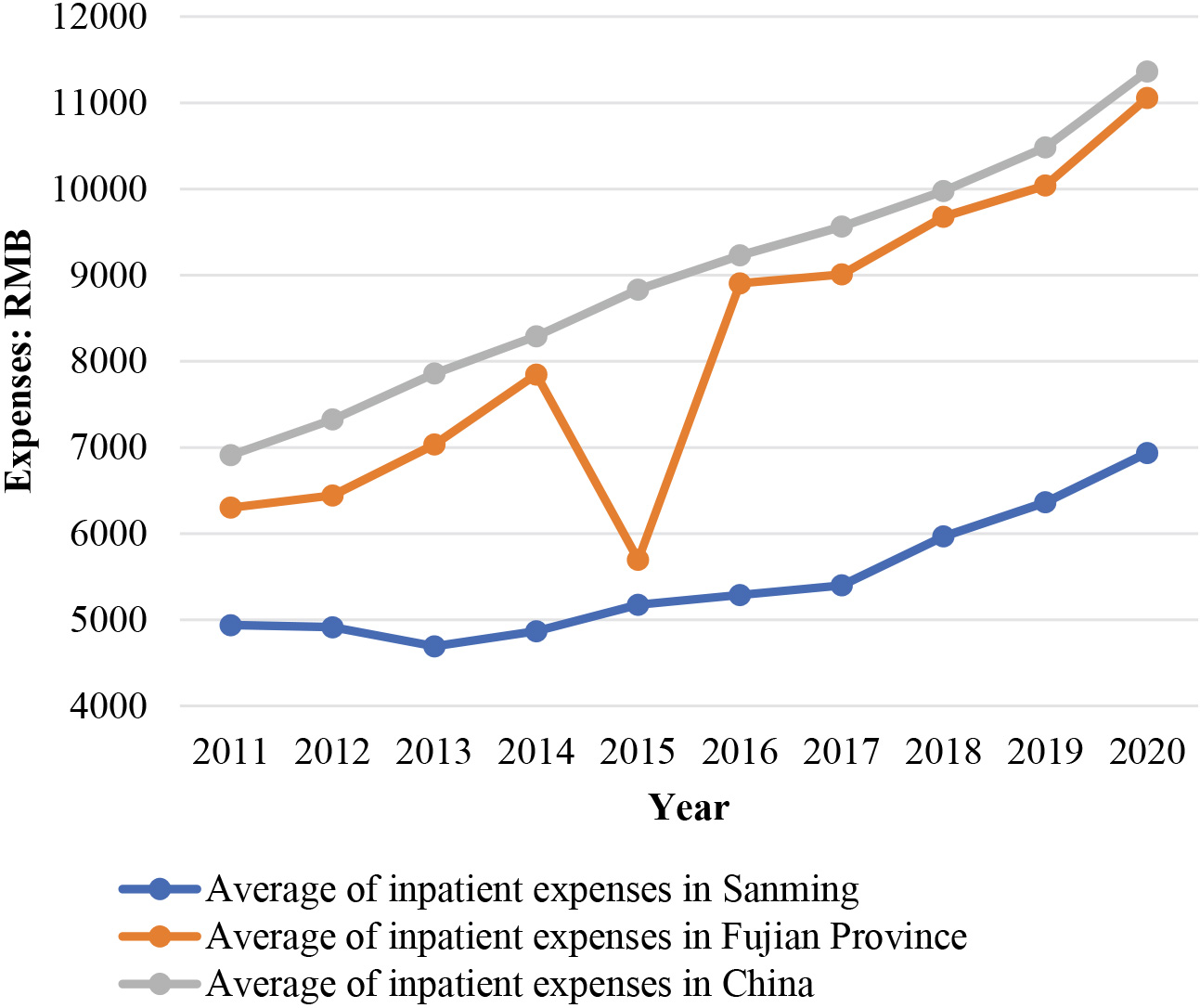
Since the beginning of 2013, all public hospitals in Sanming have started to implement the policy of drug sales without added profit. As for the policy-related losses, the hospitals resolved them by: (1) adjusting the prices of medical service items which shifted the losses by 85%–87%; (2) subsidizing 10% of the losses by the government and forming a sustainable and long-term financial subsidy mechanism; (3) strengthening cost management and improving the operation efficiency of hospitals to resolve the deficit by 3%–5%. To a large extent, due to the change of drug prices, the proportion of total drug revenue
Changes of public hospital service quantity in Sanming, Fujian Province and China
of the 10 public hospitals in the total hospital revenue continued to decline from 2013 to 2020, and the growth rates of neither average outpatient medical expenses per time nor average inpatient medical expenses per time exceeded the assessment requirements in Table 4.
As can be seen in Fig. 5, from 2011 to 2020, the average outpatient expenses of 22 public hospitals at county level and above in Sanming decreased first and then rose slowly, which was lower than the provincial and national levels in the same period. It can be seen in Fig. 6 from 2011 to 2020, average hospitalization expenses per time in the 22 public hospitals in Sanming first decreased and then slowed increased, which was lower than the provincial and national levels in the same period. As shown in Table 5, the number of medical services supplied by Sanming public hospitals kept increasing, but the growth rate kept reducing year by year, which is consistent with the country’s and province’s overall situation. The COVID-19 has considerably limited the amount of medical services available in 2020.
From 2016 to 2019, the proportion of prescriptions, including intravenous infusion drugs rates, fell from 4 percent to 3 percent which indicates that the reform has significantly reduced the rate of intravenous infusion in prescriptions and that the rate of intravenous infusion has been reduced to a lower level. It shows that the reform has indeed changed the prescribing behaviour of health workers, reducing the overtreatment and overmedication.
The evaluation after the reform focuses on the strength of the reform, the service effect, medical staff satisfaction, and medical staff income.
Since 2012, the 22 public hospitals in Sanming have adjusted their medical service prices successively for eight times, with a total of more than 8000 items. Due to factors such as price adjustment, the hospitals’ medical service income increased to 4.874 billion yuan. Through the reform of income distribution for hospitals and doctors, the level of sunshine income was improved, the total salary of hospitals was decoupled from the incomes of drugs and consumables, inspection and testing, beds, etc. Meanwhile, the outpatient and surgical services of medical staff were directly linked to their wages. In 2019, the total salary of the 22 public hospitals in Sanming was 1.406 billion yuan, which was 3.68 times of that in 2011 before the reform was carried out. Meanwhile, the average annual salary of hospital presidents increased from 98,400 yuan to 398,400 yuan. Therefore, it can be inferred that scientific and reasonable adjustment of medical service prices is helpful to improve the income structure of hospitals and to mobilize the enthusiasm of medical staff [22].
Since the reform was carried out, the average annual salary of doctors in public hospitals above the county level in Sanming has been kept increasing. The average income in 2019 increased by 192% compared with that in 2011. As illustrated in Fig. 7, medical reform may have an impact on some physicians’ prospective income, but as doctors’ medical service income rises as a result of the reform, the number of medical workers in Sanming continues to rise and the daily quantity of treatment per doctor decreases. From 2013 to 2018, only about 200 medical staff resigned from public hospitals in Sanming, accounting for only 1% of the total number of health workers [23]. In a questionnaire survey, the managers and doctors interviewed clearly said that their incomes after the reform had indeed increased a lot, especially the income of medical staff in surgical, gynecological and pediatric departments. What’s more, the daily workload of doctors had been reduced. As for the satisfaction towards the reform, all interviewees said they were satisfied.
At Sanming, the family doctor contracting service operates under the “1
Changes in human resource allocation of medical institutions in Sanming after the reform.
Before the reform, Sanming had different medical insurance policies and payment standards, just like many other regions in China. In 2010 and 2013, Sanming implemented municipal pooling of the employee medical insurance fund and new rural cooperative medical insurance fund, respectively. In order to better manage the medical insurance funds, Sanming established a Medical Insurance Fund Management Center. Thirty common and frequently occurring diseases were screened out in the city, based on which single disease payment was implemented in the 22 public hospitals in 2013. In addition to that, different self-payment proportions were set according to different grades of hospitals, which not only promoted hierarchical diagnosis and treatment, but also had unreasonable medical expenses under control. For example, if the verified cost of bronchopneumonia is 2000 yuan, then the patients who have participated in the new rural cooperative medical insurance only need to pay 1160 yuan in a grade-2 hospital, and 1376 yuan in a grade-3 hospital.
In 2013, Sanming started to assess, in a differentiated way, the average outpatient and emergency expenses per time and average discharge expenses per time of the 22 public hospitals in Sanming. Final accounting was made at the end of each year. The excess funds would not be paid, and 60% of the saved funds would be used as rewards. It was required that the annual growth rate of the total income of medical expenses in public hospitals be controlled within 8%. If the growth rate exceeded 12%, this item would be failed. If the growth rate exceeded 15%. If the growth rate exceeded 15%, the president of the hospital wouldn’t get the annual bonus.
Table 6 lists the hospitalization expenses of the patients using the urban and rural resident medical insurance in Sanming. Obviously, since the reform started in 2014, the average hospitalization expenses per time paid by medical insurance and the average hospitalization expenses per time paid by patients in Sanming both have shown an increasing trend, with an average annual growth rate of 8.66% and 14.78% respectively. The average hospitalization expenses of Sanming residents were lower than the national average.
Changes of doctors’ average annual salary and proportion of medical service income in Sanming’s public hospitals
Changes of doctors’ average annual salary and proportion of medical service income in Sanming’s public hospitals
The comprehensive reform of public hospitals in Sanming reduced drug prices, improved the drug procurement mechanism, and cut down medical service charges. Furthermore, it increased the salary of medical staff, altered the medical and insurance payment mode, and indirectly affected the treatment costs of patients. However, other factors that affecting patients’ treatment costs should also be taken into consideration.
After the drug price reform, the overall drug price in Sanming decreased by 30%, the prices of some drugs decreased by 70%–90%, and a few even decreased by 95%. The total consumption of drugs decreased by 20%. Doctors’ prescribing behavior changed, and the rate of intravenous drugs fluids dropped to 3%. Through the “one product, two specifications” (one for domestic products and one for imported products) policy, the number of drug in Sanming public hospitals reduced from 8361 to 1858, with a decrease rate of 78%. This has effectively prevented doctors from choosing drug varieties with rebates when they face the same drugs. Through the comprehensive reform, the drug expenditures of public hospitals in Sanming achieved a negative growth from 810 million yuan in 2011 to 730 million yuan in 2020. Therefore, it can be concluded that the reform had effectively slowed down the growth of drug expenses of public hospitals in Sanming. Furthermore, from 2013 to 2020, the proportions of outpatient medical expenses and medical expenses of discharged patients decreased from 37% and 24% respectively to 35% and 16%. Consequently, the decrease in the proportion of medical treatment expenses can be attributed primarily to the decrease of drug prices.
The average salary of doctors increased significantly after the reform. For instance, in 2011, the average salary was only 56,500 yuan, but it increased to 165,000 yuan in 2019. The proportion of health technical personnel kept increasing year by year. For example, the numbers of health technical personnel and professional doctors per thousand permanent residents also increased from 6 and 2.07 in 2016 respectively to 6.77 and 2.47 in 2019. This indicates that the reform of doctors’ salary system and supervision strengthening of doctor’s prescription behavior has no direct impact on the number of doctors. What’s more, these measures helped retain patients in the county, brought more income and better reputation to the hospitals, and promoted doctor return to their right role [24].
After the reform, the income structure of public hospitals was improved. The proportion of medical service income of public hospitals in Sanming kept increasing, from 32.26% in 2013 to 41.46% in 2020; and the proportion of drug income kept declining, from 28.21% in 2013 to 23.25% in 2020. The hospitals succeeded in transforming their income structure from drug income-oriented to medical service income-oriented, and they started to have an increasing amount of disposable income which promoted their sustainable development. As the medical income in public hospitals increased, it is likely that a sustainable increase will be achieved for the salary of medical staff in Sanming public hospitals. Based on the growth trend of the total medical income and the proportion of medical income in Sanming public hospitals since the reform, the proportion of total paid wages in medical income of Sanming public hospitals will remain about 50% in the next five years.
After the reform, the actual reimbursement rate of urban employee medical insurance in Sanming was about 69%, and that of urban and rural resident medical insurance was about 50%, both higher than the national average. Besides, the medical insurance fund for urban employees in Sanming gradually turned from loss to profit after the reform was implemented. Before that, the medical insurance fund for urban employees could not cover the expenditure, and the loss accounted for about 10%–15% of the local financial revenue of the city in that year. After the reform, in spite of the great pressure posed by the decrease of in-service employees, the increase of retirees, and the continuous decline of the support ratio (the ratio of the number of social security contributors to the number of retirees), the medical insurance fund for urban employees in Sanming was still able to gradually turn from loss to profit. In 2018, the medical insurance fund for urban employees in Sanming had a balance of 104 million yuan. Besides, the urban and rural resident medical insurance continued to operate smoothly, and the utilization rate of funds increased from 82% in 2011 to 96% in 2020, with a year-on-year increase of 1.74 percentage points.
Despite the abundant achievements, Sanming still encountered some problems in the comprehensive reform of public hospitals. First of all, in the drug price reform, because drugs were purchased with the prices under control, it was usually the drug vendors, with low drug prices, who won the orders. In the meantime, drugs were simply divided into imported drugs and domestic drugs in terms of quality, which was too hasty. This practice was controversial, and people were worried that it would lead to uneven drug quality. Secondly, the study was based on the pharmaceutical market of only one municipal city, Sanming, so the bargaining power for some imported drugs, original R&D drugs, high-value consumables and large-scale medical equipment was still weak. After the reform, the overall drug prices dropped. However, the price reduction of imported drugs, which accounted for 22% of the drug categories, was not obvious. The price reduction rate of some imported drugs with a relatively high price reduction rate ranged only within 10%–15%, and the bargaining power was still rather limited. Thirdly, due to the low drug prices, some drugs were out of stock. According to the data of Sanming Medical Management Center, fourteen pharmaceutical manufacturers have given up Sanming market due to the price. At the same time, drugs with low prices and obvious price reduction, such as vitamin B6 and Pentoxyverine, were in extremely serious shortage. Finally, Sanming had implemented medical insurance pooling at the municipal level. Although municipal medical insurance pooling has the advantages of better risk dispersion ability, it may also cause the problem of “the poor helping the rich”. For example, the counties with lower income have more savings in medical insurance funds, and rich counties may have fund overruns. According to Sanming medical insurance fund regulations, the balance of funds should be handed in, and the city should bear 30% (the funds handed in by each district and county) of the deficit part for fund overrun counties. Therefore, part of the deficits of fund overrun counties would be transferred to the fund balance counties, which is not favorable to the social justice redistribution of the counties with lower income.
Conclusion
In this paper, the method of system dynamics is successfully applied to model and analyze the Sanming public hospital reform, and the following conclusions are drawn. Through the comprehensive reform of public hospitals, Sanming has systematically altered the drug purchasing mechanism, reduced drug prices, and increased the salary income of hospital staff. Besides, it improved the income structure of hospitals and changed the medical insurance payment mode. Moreover, it reduced the treatment expenditures of patients and promoted the development of hierarchical diagnosis and treatment. However, there are still some problems in the reform, for example, the simplistic division of drug specifications, the poor bargain power concerning some drugs, the short supply of some sorts of low-cost drugs and the unreasonable management of the medical insurance fund. To give full play to the reform effect, it is suggested that the government evaluate and clarify drug differences and establish a price negotiation mechanism at the national level to effectively improve the bargaining power and strengthen the production capacity of low-price drugs of pharmaceutical enterprises so as to meet the regular demands of hospitals. In addition, the government should also integrate medical insurance as a whole from the provincial and national level so as to promote the redistribution of social equity such as reducing drug prices and increasing the salary income of hospital staff. This paper does not further develop the broad model of public hospital reform; instead, it solely explores and evaluates the three systems of medication, medical care, and medical insurance separately. The authors will keep working toward constructing a systematic and scientific Sanming public hospital reform model in the future.
Footnotes
Availability of data and material
Publicly available datasets were analyzed in this study. The data related to Fujian Province and China are from Health Statistics Yearbook of China from 2012 to 2021. The data related to Sanming are from: