
Abstract
INTRODUCTION
Huntington disease (HD) is a progressive neurodegenerative disease consisting of motor, cognitive, and psychiatric symptoms. There is currently no treatment known to slow worsening of disease progression [1]. However, several potential disease modifying or symptomatic therapies for HD are currently under development [2, 3]. Retaining enrolled participants is critical for all clinical studies, especially those for rare diseases such as HD, where fewer individuals may be available to participate. Participant retention reduces the problems of bias and decreased power associated with missing data in the analysis of clinical trials for prospective HD therapies [4].
Most clinical trials in HD use specific numerical scores of one or more components of the Unified Huntington’s Disease Rating Scale (UHDRS) to determine eligibility to participate. The UHDRS is a clinical rating scale developed by investigators of the Huntington Study Group and later updated in 1999 (UHDRS 99), consisting of 4 components: motor, behavioral, cognitive, and functional assessments [5]. A change in the score of a specific UHDRS assessment, such as total functional capacity (TFC), often serves as the primary outcome variable for HD trials. All three studies included in this analysis used change in TFC score and/or death as the primary outcome variable [6–8].
To our knowledge, investigation of factors that may be associated with withdrawal from HD clinical trials has not been previously reported. To better understand what factors may be associated with increased probability of withdrawal, we performed analyses of HD participant retention in three clinical trials including; coenzyme Q10 and remacemide in HD (CARE-HD), a pilot study of minocycline in HD (DOMINO), and coenzyme Q10 in HD (2CARE) (Table 1) [6–8].
Baseline characteristics of the CARE-HD, DOMINO, and 2CARE cohorts
Values are mean (standard deviation) or percentage unless otherwise indicated. N/A = not available.
MATERIALS AND METHODS
Clinical trials analyzed
The CARE-HD trial was a randomized, double-blind, placebo-controlled trial with a 2×2 factorial design to determine if treatment with coenzyme Q10 300 mg twice daily and/or the NMDA receptor antagonist remacemide hydrochloride 200 mg three times daily would slow functional decline in HD, as measured by the TFC score. A total of 347 participants with early stage HD were enrolled at 23 sites between July 1997 and June 1998 and treated for 30 months. Treatment with coenzyme Q10 and/or remacemide failed to slow functional decline in early HD [6].
The DOMINO trial was a futility design trial assessing the potential for minocycline to slow disease progression in HD. A total of 114 participants were enrolled at 12 sites and randomized (3 : 1) to minocycline 200 mg/day or placebo between April 2006 and November 2008. The primary outcome variable was the change in TFC from baseline to 18 months. The results of the study provided insufficient evidence to justify proceeding with a phase III clinical trial assessing the ability of minocycline to slow progression of HD [7].
The 2CARE study was a randomized, double-blind, placebo-controlled trial assessing the effect of coenzyme Q10 2400 mg/day on functional decline in HD, as measured by a combination of change in TFC score and time to death over 60 months. Participant enrollment was completed in June 2012 with 609 subjects enrolled at 49 sites; however, an interim analysis indicated futility of coenzyme Q10 and the study was halted in July 2014 [8].
All studies were run by the Huntington Study Group, an academic research consortium. These clinical trial protocols were approved by the institutional review board/ethics committee at each participating center, and all participants provided written informed consent. The studies were performed in accordance with the Declaration of Helsinki and Good Clinical Practice. This analysis was approved by the Steering Committee of each clinical trial.
Classification of reasons for study withdrawal
To determine reasons study participants withdrew from the CARE-HD, DOMINO, or 2CARE studies, study databases were investigated in detail. A narrative description of each individual withdrawal was recorded in the study database at the time that the site learned of the participant’s withdrawal. Based on this description, the reason for withdrawal was classified into one of eight categories including: death, disease progression, adverse events, difficulty traveling, interest in other clinical trials/medications, loss of interest/desire to participate, loss to follow-up, or other. When a participant did not indicate the reason for withdrawal and the study site attempted to contact the participant without response, the reason was classified as “loss to follow-up.” In circumstances where withdrawal was determined to be for multiple reasons and not one initiating primary reason, the reason was classified as “other.” In situations where a participant moved away from a study site and was unable to transfer to another site, the reason was classified as “other.” Prior to data analysis, the narrative descriptions were read and classified by two independent neurologists. Any discrepancies were further reviewed by a third neurologist and statistician and discussed among the four individuals to come to a final consensus regarding classification of a case.
Statistical analysis
Kaplan-Meier curves were used to describe the distribution of time to withdrawal from study participation for each study. Cox proportional hazards models were used to examine the associations between demographic and clinical characteristics and the outcome of time from randomization to withdrawal from the study. For variables that were measured longitudinally, baseline values as well as time-dependent values were considered as possible predictors. Times were censored at the end of follow-up for those who did not withdraw from study participation. Associations with a p-value less than 0.01 (two-tailed) were considered to be statistically significant. Statistical analyses were performed using SAS software, Version 9.4.
RESULTS
Reasons for withdrawal
Probabilities of withdrawal at 12 months varied across the three clinical trials analyzed: CARE-HD (2.9%), DOMINO (10.5%), and 2CARE (5.9%) (Fig. 1). The reasons for withdrawal varied slightly among the three studies. Mean percentages for each category across studies revealed that loss to follow-up was the most common reason for withdrawal (23.2%), followed by death (15.9%), loss of interest/desire to participate (15.2%), adverse events (11.3%), interest in other clinical trials/medications (7.1%), disease progression (5.0%), and difficulty traveling (4.0%) (Fig. 2). The category of “other” reasons was especially common in the CARE-HD trial (31.6%).
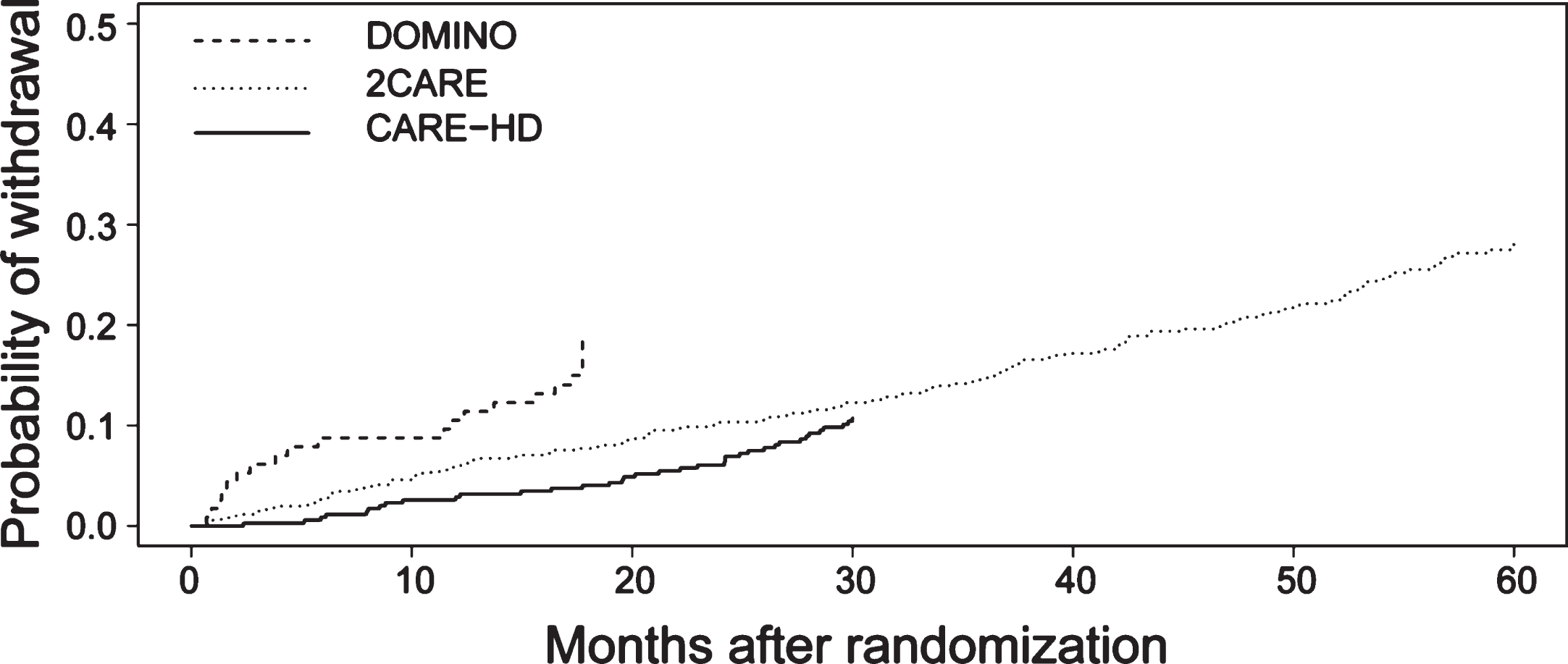
Kaplan-Meier curves showing the estimated probabilities of participant withdrawal in three Huntington disease clinical trials.
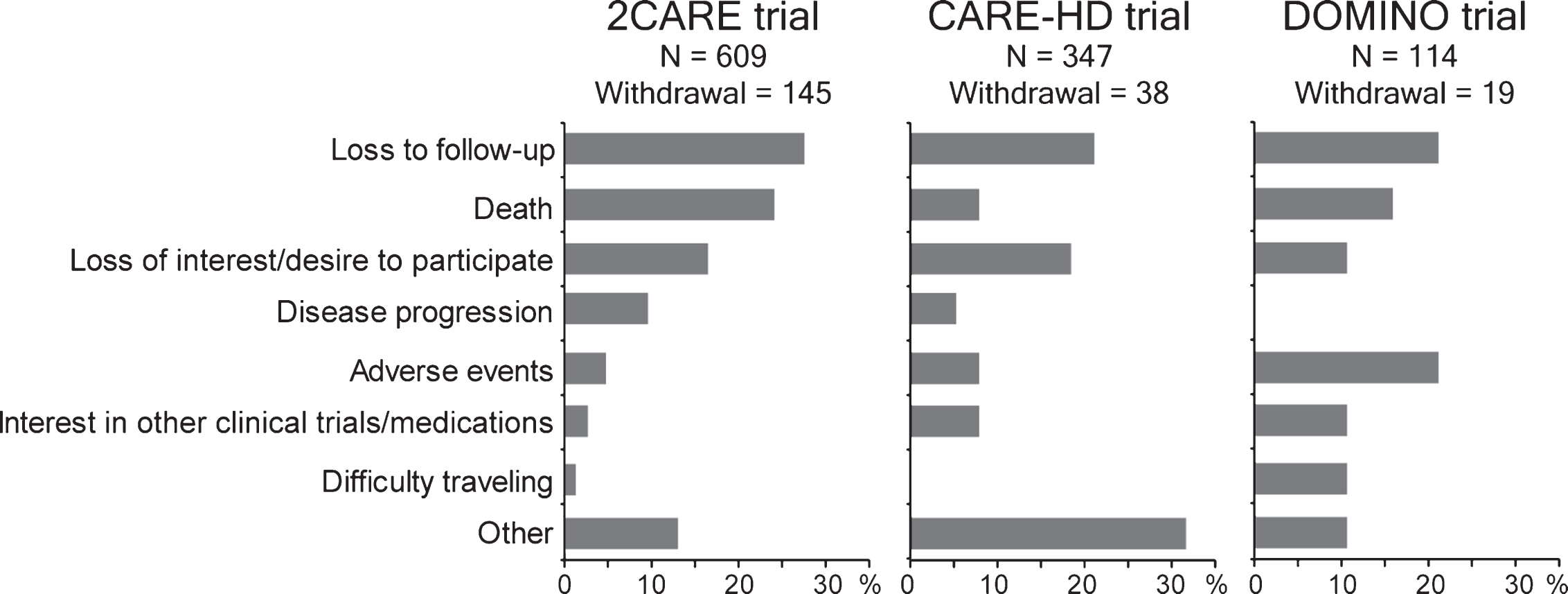
Reasons for withdrawal in three Huntington disease clinical trials.
Associations between baseline characteristics and time to withdrawal
In the CARE-HD study, no baseline participant characteristics were significantly associated with shorter time to withdrawal, although tendencies for association were indicated by worse symbol digit modalities test and functional assessment scores (0.01 < p < 0.05) (Table 2). In the DOMINO study, only scores on the verbal fluency test and independence scale indicated tendencies for association (0.01 < p < 0.05) and no characteristics were significantly associated with time to withdrawal (Table 3). In the 2CARE study, baseline characteristics associated with shorter time to withdrawal included worse UHDRS total motor, functional assessment, and independence scale scores. Also, worse scores on the symbol digit modalities test, Stroop interference test, behavioral assessment, and TFC indicated tendencies for association with time to withdrawal (0.01 < p < 0.05) (Table 4). Gender, marital status, education level, ethnicity, and age were not associated with time to withdrawal in any of the three trials.
Associations between baseline characteristics and time to withdrawal in CARE-HD
†Marital status could not be analyzed because this information was not collected.
Associations between baseline characteristics and time to withdrawal in DOMINO
†Ethnicity could not be analyzed due to the absence of withdrawal events in African-American participants and the small number of non-Caucasian participants overall.
Associations between baseline characteristics and time to withdrawal in 2CARE
*Significantly associated with time to withdrawal.
Associations between time-dependent variables and time to withdrawal
In both the CARE-HD and DOMINO trials, none of the time-dependent variables examined were found to be associated with time to withdrawal (Tables 5 & 6). In the 2CARE trial, time dependent variables associated with shorter time to withdrawal included worse total motor score and scores on the symbol digit modalities test, behavioral assessment, functional assessment, independence scale, and TFC (Table 7).
Associations between time-dependent variables and time to withdrawal in CARE-HD
Associations between time-dependent variables and time to withdrawal in DOMINO
Associations between time-dependent variables and time to withdrawal in 2CARE
*Significantly associated with time to withdrawal.
DISCUSSION
Early withdrawal of participants has an impact on the statistical power and interpretability of a study, so understanding the reasons for its occurrence is important. Screening potential trial participants for certain baseline characteristics that are associated with higher withdrawal rates, and potentially excluding those individuals from enrollment in a trial, may preserve statistical power. However, this consideration should be balanced with the ability to recruit trial participants. Identification of time-dependent covariates that are associated with earlier time to withdrawal may also permit identification of participants at greater risk of withdrawal. These participants could then benefit from more targeted efforts for retention.
Analyses of three clinical trials assessing pharmacologic therapies in individuals with HD revealed some of the common reasons for study withdrawal for HD participants. These reasons included loss to follow-up, death, loss of interest/desire to participate, adverse events, interest in other clinical trials/medications, disease progression, and difficulty traveling. The most common reason for withdrawal varied slightly among the three trials, which may have been due to specific eligibility criteria, treatment safety profile, and duration of follow-up. It should be noted that the reasons for withdrawal reported in the original trial publications may differ from those reported here due to the more detailed process for categorizing reasons for withdrawal in the current investigation.
Loss to follow-up was the most common reason for withdrawal when examining the mean percentage across the three trials, but the percentage of withdrawals due to this reason varied among the trials: 21.1% of withdrawals in CARE-HD, 21.1% in DOMINO, and 27.6% in 2CARE. Longer duration of follow-up in 2CARE (60 months), compared to CARE-HD (30 months) and DOMINO (18 months), may partly account for these findings. In addition, follow-up visits in 2CARE were scheduled at 6-month intervals, which may have influenced the rate of loss to follow-up. Interim phone calls to participants/caregivers may contribute to maintaining good relationships between enrolling sites and participants. The 2nd most common reason for withdrawal was death (15.9%). The percentage of withdrawals attributed to death was highest in 2CARE (24.1%), which may also be due to the longer duration of follow-up in this study.
Loss of interest/desire to participate was the 3rd most common reason for study withdrawal, but was least frequently seen in DOMINO. This may be due to the shorter duration of follow-up in this study. Adverse events were the 4th most common reason for study withdrawal with the highest percentage being in DOMINO. This may be secondary to greater intolerance of minocycline compared to coenzyme Q10. In DOMINO, there were 4 withdrawals due to adverse events in the minocycline group and none in the placebo group. Future studies that allow dosage reductions in the setting of adverse events, assess more well-tolerated drugs, or allow follow-up evaluations off of study drug may allow greater retention in a study. Of the other three categories used, disease progression is unfortunately inevitable; however, withdrawal for this reason may be reduced by enrolling individuals with higher baseline TFC scores or having a shorter duration of follow-up. In future trials, withdrawal due to difficulty traveling may be reduced by several methods including: requiring the participation of a caregiver who will accompany the subject to study visits, providing paid transportation to study sites for participants, or allowing telemedicine study visits in place of some clinical site visits. A participant’s interest in other trials cannot be easily anticipated so it would be more difficult to address this.
The average probability of withdrawal at 12 months for these trials was 6.4%. The numbers of participants who withdrew from the DOMINO (n = 19) and CARE-HD (n = 38) trials were low, causing decreased power to detect significant associations of predictors with time to withdrawal in these studies. However, a considerably larger number of withdrawal events was observed in 2CARE, likely due to the larger sample size and longer duration of follow-up. In 2CARE, worse baseline total motor score and worse functional assessment and independence scale scores were associated with shorter time to withdrawal. Time-dependent variables in 2CARE that were associated with a shorter time to withdrawal included these same variables in addition to worse scores on the symbol digit modalities test, behavioral assessment, and TFC. Evaluation of all 3 studies indicated that gender, marital status, education, ethnicity, and age were not associated with time to withdrawal.
One of the limitations of this study is the use of subjective categorization of withdrawal reasons. The categorization process was strengthened by having two independent evaluators (both neurologists) analyze cases of withdrawal, followed by common consensus of categorization between these two individuals and an additional statistician and neurologist. Another limitation is the performance of multiple statistical tests. To mitigate this issue, we used a relatively stringent significance level of 0.01 (two-tailed). Nevertheless, we consider this work preliminary and hypothesis generating rather than confirmatory. In addition, we could not analyze other factors that may have affected withdrawal rate that were not available for analysis such as socioeconomic status, health of caregiver, child care issues, owing a car, and the ability to drive independently.
There are several aspects of the selected studies that should be considered when attempting to generalize our results to future HD clinical trials. The trials considered here were designed and executed by an academic research consortium with investigators having subspecialty expertise and being devoted to HD research and clinical care. Also, understanding of the disease process continues to evolve among patients and caregivers in the HD community, as does an appreciation of the importance of clinical trials. Advances in technology such as wearable sensors, e-diaries, and telemedicine visits may also have a profound effect on retention in future HD clinical trials.
Although not examined in this study, another design feature that may increase retention in HD clinical trials is the requirement of a caregiver or individual that could give consent for future study related activities if a participant lost capacity for decision making during the course of a prolonged trial. Since this was a requirement in the 2CARE trial we were unable to examine the effect of the presence or absence of this factor in our analysis. The 2CARE study also added the option of follow-up via telephone for some visits later in the trial if a person had difficulty getting to a clinical trial site. Future clinical trials may also address difficulty with traveling by including the option of completing some visits via telemedicine. However, clinical trial visits using telemedicine technology produce their own challenges, including feasibility and reliability of study assessments and investigator licensing regulations that may vary by state and country [9].
Ultimately, if the objective of a clinical trial in HD is to assess the neuroprotective effect of an intervention, eligibility criteria requiring higher baseline functional status and better behavioral and motor scores on the UHDRS assessments would likely be advantageous. Previous studies have shown that strategies to improve protocol adherence and participant retention may include enrolling people at early disease stages such as in amyotrophic lateral sclerosis clinical trials [10]. In line with this hypothesis, higher executive control and visual memory performance was shown to be associated with treatment completion in borderline personality disorder clinical trials [11]. On the other hand, restricting eligibility criteria may have implications on recruitment rate, which both add to the duration and cost of the trial. Additional studies are needed to examine the impact of eligibility criteria on enrollment, recruitment, and statistical power.
CONFLICTS OF INTEREST
Merit Cudkowicz has provided consultation for Biohaven, Mitsubishi Tanabe Pharma, Biogen, Immunity Pharma, Karyopharm, Cytokinetics, and Denali Therapeutics. Nazem Atassi has provided consultation for Biogen and Mitsubishi Tanabe Pharma. Other authors have no conflicts of interest to report.
Footnotes
ACKNOWLEDGMENTS
The authors thank the CARE-HD, DOMINO, and 2CARE trial participants, their family/caregivers, investigators and coordinators. This work was funded by the Huntington Study Group, the Uehara Memorial Foundation and the Toyoaki Foundation.