
Abstract
Background:
Huntington disease (HD) is a neurodegenerative disorder characterized by motor impairments (including chorea), along with behavioral, psychiatric, and cognitive symptoms. Tetrabenazine was the first US Food and Drug Administration (FDA)-approved treatment for chorea related to HD.
Objective:
To examine pharmacologic treatment patterns among patients using tetrabenazine, including reasons for treatment initiation, non-initiation, dose adjustments, and discontinuation, and to quantify the burden of chorea based on healthcare resource utilization.
Methods:
In this retrospective patient chart review, neurologists were recruited from the Medefield (http://www.medefield.com) opt-in panel, and selected ≤5 medical charts based on the criteria provided and abstracted data on demographics, disease history, healthcare resource use, and treatment patterns.
Results:
138 neurologists participated and 512 HD patient charts were reviewed. Among these patients, 26.4% did not initiate tetrabenazine. Most HD patients (66.5%) received a tetrabenazine dose ≤50 mg. The most common reasons for stopping upward titration were optimal chorea control (55.5%), intolerability of higher doses (31.2%), and reaching the maximum recommended dosage despite suboptimal chorea control (11.4%). Chorea severity and non-persistence to tetrabenazine were associated with increased emergency room visits, hospitalizations, and days hospitalized.
Conclusions:
Although tetrabenazine was the sole FDA-approved treatment for HD chorea until April 2017, more than one-quarter of respondents never initiated therapy. Tetrabenazine dosing was lower than predicted, and many patients experienced adverse symptoms of intolerability at high doses. New safer and more tolerable treatment options, such as deutetrabenazine, may improve treatment outcomes and reduce healthcare resource use.
INTRODUCTION
Huntington disease (HD) is a hereditary, multifaceted neurodegenerative disorder, characterized by motor dysfunction, progressive cognitive impairment, and behavioral-emotional dysregulation [1–3]. Chorea is the most prominent motor feature of HD and affects about 90% of adult-onset HD patients [4, 5]. Chorea is characterized by abnormal, involuntary, writhing movements that may increase the risk of injury, and interfere with daily functioning, and can increase social stigma for both patients and their caregivers [4, 5].
Tetrabenazine, a vesicular monoamine transporter 2 (VMAT2) inhibitor, was approved by the US Food and Drug Administration (FDA) as the first treatment of HD chorea in 2008 [6]. Dosing of tetrabenazine is individualized, starting at 12.5 mg/day and increased by 12.5 mg/day weekly until satisfactory control of chorea is achieved or intolerable adverse events (AEs) occur [7]. It is recommended that dosages of 37 mg/day or greater be given in a three-times-a-day regimen [7]. For dosages up to 50 mg/day, the maximum recommended single dose is 25 mg [7]. Poor cytochrome P450 2D6 (CYP2D6) metabolizers should receive a maximum single dose of 25 mg and maximum daily dose of 50 mg [7]. Extensive and intermediate CYP2D6 metabolizers should receive a maximum single dose of 37.5 mg and a maximum daily dose of 100 mg [7].
In a randomized, double-blind, placebo-controlled, US study of tetrabenazine in patients with HD chorea (TETRA-HD), tetrabenazine was efficacious at improving the primary endpoint, the Unified Huntington’s Disease Rating Scale Total Maximal Chorea score (TMC), as compared with placebo (mean change±standard error [SE]: –5.0±0.5 vs –1.5±0.7, P < 0.0001) [8]. In the TETRA-HD study, the average dosage attained at the end of the maintenance phase (Week 12) was approximately 75 mg [8, 9]. More patients receiving tetrabenazine (90.7%, 49/54) experienced AEs compared with those receiving placebo (70.7%, 21/30; P = 0.01) [8]. Most common AEs (occurring in over 10% of the tetrabenazine group and at least 5% more frequently than was seen in patients given placebo) were drowsiness/somnolence, insomnia, fatigue, depression, agitation, anxiety, and nausea [8]. A total of 51.9% (28/54) of patients given tetrabenazine had to stop dose escalation or reduce the dose due to AEs (sedation, akathisia, parkinsonism, depression, and other) [8]. In an open-label extension of the TETRA-HD study, patients continued to show improvements in TMC after 80 weeks of treatment (mean change from baseline±standard deviation [SD]: –4.6±5.5 units; P < 0.001) [10]. The mean daily dose of tetrabenazine at Week 80 was 63.4 mg [10]. The most common treatment-emergent, moderate to severe AEs (>5% of subjects) were sedation/somnolence, depressed mood, anxiety, insomnia, akathisia, fatigue, agitation, fall, dysphagia, and dystonia [10]. Between Weeks 24 and 48, 84.1% (37/44) of patients stayed on the same dose or had a decrease in dose, a trend that continued between Weeks 48 to 80 (86.4% [38/44] of patients) [10].
The primary objective of this study was to examine pharmacologic treatment patterns, including physician reasons for initiating or not initiating tetrabenazine, dosing, and reasons for dose adjustments and/or discontinuation among patients using tetrabenazine in the real-world US population. The secondary objective was to quantify the burden of chorea based on healthcare resource utilization.
METHODS
Study participants
Neurologists were recruited to participate in this retrospective patient chart review from the Medefield (http://www.medefield.com) opt-in panel of physicians via an e-mail invitation from December 2016–April 2017. Potential physician respondents provided consent and were provided with screening questions to ensure eligibility. Physicians were required to be neurologists (board certified or board eligible), actively practicing for at least 5 years, personally involved in the treatment of patients with HD, and had to have at least 3 patients with HD under their care. After providing consent, eligible neurologists selected up to 5 qualified medical charts based on the following criteria: patients at least 18 years old, diagnosed with HD, and experienced chorea. Physicians provided data via an online data collection form on demographics, disease history, healthcare resource use, and treatment patterns.
Study procedure
Qualitative interviews conducted with neurologists (n = 5) were used to inform the development of the chart review survey. The specific focus of these interviews was to understand how clinicians manage patients HD chorea patients and their experiences with tetrabenazine therapy. We pilot-tested the survey to ensure content validity of the survey before the data collection form was developed.
Neurologists were asked to select charts from the most recent patient visits meeting the inclusion criteria. Data were pulled from notes from physical examinations, prescription data, and nurse records, as appropriate. The final patient data set included the demographics, health history, healthcare resource use, and treatment information of each patient.
Data abstracted to the data collection form included physician characteristics, physician disease-management approaches, patient demographics, patient health history, including chorea and HD diagnosis, patient treatment history, and patient healthcare resource utilization. Physician disease-management approach data included chorea severity distribution among their patients, symptom treatment patterns, treatment patterns based on chorea severity, and the factors that contribute to the decision for chorea treatment. For chorea severity, physicians were asked to either provide Unified Huntington’s Disease Rating Scale (UHDRS) scores or to rate chorea severity (mild, moderate, or severe). Treatment history data in patients using tetrabenazine included the initial dose, duration of the titration period, maintenance dose, dosage changes, reason for dosage changes, and reasons for discontinuation. Treatment history data in patients not using tetrabenazine included reasons for not initiating treatment. Patient healthcare resource utilization data included the number of office visits, hospitalizations, and emergency room visits in the past 12 months.
The study was conducted in accordance with the current Declaration of Helsinki and was consistent with International Conference on Harmonization Good Clinical Practices, Good Epidemiology Practices, code of standards and ethics for survey research, and other applicable local laws and regulatory requirements. Pearl Pathways Independent Review Board approved this project as an exempted retrospective study and determined that informed consent was not required. All data was de-identified and anonymously entered by the physicians via a secure online data collection platform (Ipsos Healthcare) designed for the study. Only authorized study personnel had access to the raw data, and all data storage or transfers were done securely.
Statistical analysis
All analyses for this study were conducted using SAS v9.3 and R v3.3. Physician demographics and practice characteristics, as well as patient demographics, health history, and disease history were reported descriptively. Based on the programming of the survey, all relevant questions required a response, though options for “unknown” or “data unavailable” (or similar values, as appropriate for the specific question) were available. As a result, missing data was kept to a minimum. If missing data were observed for an outcome variable, case wise deletion was conducted; no imputation strategy was implemented. The burden associated with tetrabenazine-related dose adjustments was reported descriptively using frequencies and percentages for categorical variables and counts, means, and standard deviations for continuous variables. The number of physician visits, emergency room visits, and hospitalizations were reported descriptively using counts, means, and standard deviations. Differences between healthcare resource use as a function of chorea severity and discontinuation were also examined. One-way analysis of variance (ANOVA) was used to test for statistical difference, with P-values ≤0.05 representing a significant effect of chorea severity within the groups examined.
RESULTS
A total of 138 board-certified/board-eligible neurologists participated in this retrospective analysis (Fig. 1, Table 1). Most of the neurologists were male (113/138, 81.9%), aged 41–60 years, with a mean (SD) of 15.8 (7.0) years in practice, and 22.5% (31/138) were from a Huntington’s Disease Society of America (HDSA) Center of Excellence [11]. These physicians identified and reviewed 512 eligible patient charts (Table 2). A majority of the patients were male, with a mean (SD) age of 45.7 (13.6), a mean (SD) time since HD diagnosis of 5.4 (5.4) years, and a mean (SD) chorea duration of 4.4 (4.7) years. More than 50% of HD patients were on disability or unemployed and more than 40% were on government-issued insurance. Less than one-fifth of patients had been genotyped for CYP2D6 and about one-third (32.2%) of patients had UHDRS scores collected.

Study flow chart A total of 138 board-certified/board-eligible neurologists participated in this retrospective chart review analysis.
Demographics of participating neurologists
HDSA, Huntington’s Disease Society of America; SD, standard deviation; VA, Veterans’ Affairs.
Patient demographics from eligible HD patient charts
HD, Huntington disease; HMO, health maintenance organization; POS, point of service; PPO, preferred provider organization; SD, standard deviation; VA, Veterans’ Affairs.
All patients in this study experienced chorea, with only 4.7% of patients experiencing chorea as their sole symptom. Other frequent symptoms included impaired gait/posture/balance (56.8%), difficulty focusing (46.7%), depression (45.7%), and difficulties with fine motor coordination (40.6%).
Tetrabenazine use in patients with HD chorea
Of the 512 HD patient charts reviewed, 377 (73.6%) patients were initiated on tetrabenazine for the first time (mean daily maintenance dose 48.7 mg) and 135 (26.4%) patients did not initiate tetrabenazine. Of patients not initiating tetrabenazine, all but 17 were prescribed other medications. The most common reasons for not initiating tetrabenazine were a history of depression (38.5%), issues with reimbursement or accessibility (29.6%), and a history of anxiety (21.5%).
Tetrabenazine dosing and titration
Of the 377 patients who used tetrabenazine for their HD chorea, approximately half (47.7%) were prescribed a twice daily regimen and 36.1% were prescribed a once daily regimen. The most common initial doses were 12.5 mg (178/377; 47.2%), and 25 mg (126/377; 33.4%). The mean (SD) initial total daily dose of tetrabenazine for all patients who received tetrabenazine (N = 377) was 22.9 (12.6) mg.
About one-third of patients (114/377; 30.2%) did not have their dose titrated up, 66.7% (76/114) of whom were prescribed a daily dose of 25 mg or less. The mean (SD) dose of tetrabenazine among those who did not have their dose titrated up was 28.6 (13.1) mg. For patients whose dose was not titrated, their initial dose was considered their stable dose.
Over two-thirds of patients (263/377; 69.8%) were titrated until a clinically optimal dose was achieved, with the dose-titration period lasting a mean (SD) of 7.1 (6.1) weeks. Among patients who had a dose titration (n = 263), the mean stable dose was 57.5 (25.0) mg, and a majority of these patients (175/263; 66.5%) received a dose of 50 mg or less. The dose distribution for these patients was as follows: 25 mg (31/263; 11.8%), 37.5 mg (43/263; 16.3%), 50 mg (101/263; 38.4%), 75 mg (51/263; 19.4%), 100 mg (35/263; 13.3%), and other (2/263; 0.8%). These dosing options were chosen based on US availability of 12.5 mg and 25 mg tablets and the FDA recommended maximum dose of tetrabenazine of 100 mg per day.
While dose titration was stopped mainly due to achieving optimal chorea control (146/263, 55.5%), a total of 31.2% (82/263) of patients stopped titration due to intolerability of higher doses, and 11.4% (30/263) reached the maximum recommended daily dose without optimal chorea control (Fig. 2).

Reasons for stopping titration in patients who had a dose increase (N = 263) While dose titration was stopped mainly due to achieving optimal chorea control (146/263, 55.5%), a total of 31.2% (82/263) of patients stopped titration due to intolerability of higher doses, and 11.4% (30/263) stopped because they reached the maximum recommended daily dose without optimal chorea control.
Of the patients who initiated tetrabenazine, 23.1% (87/377) discontinued tetrabenazine therapy (Fig. 3). The most common reasons for discontinuation (multiple reasons could contribute to discontinuation) were ineffective treatment of chorea (42/87, 48.3%), patient or caregiver request to discontinue (34/87, 39.1%), and AEs or tolerability issues (33/87, 37.9%), depression (26/87, 29.9%), and reimbursement, access, or, co-pay issues (21/87, 24.1%).
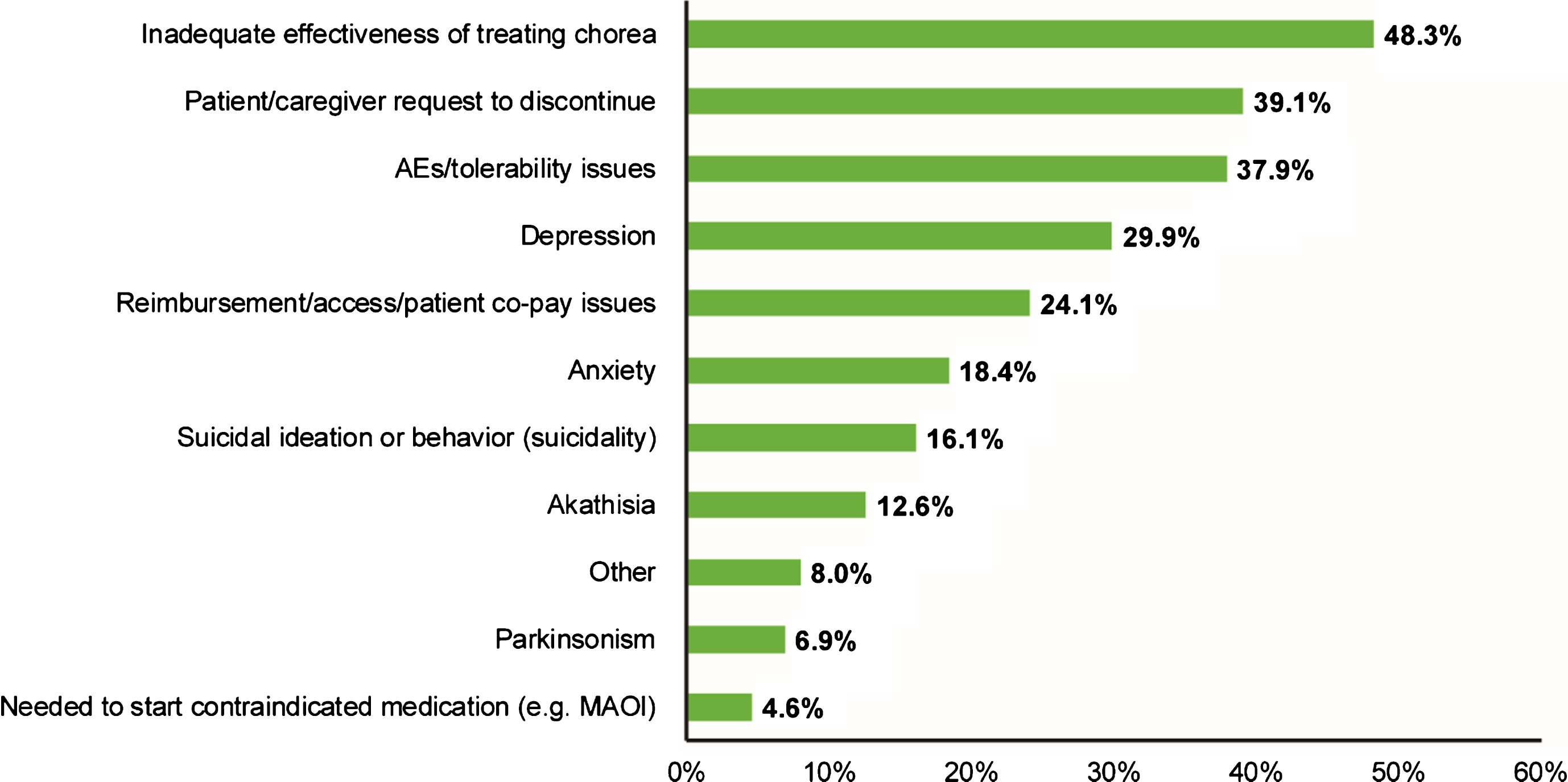
Reasons for discontinuing tetrabenazine therapy (N = 87) Of the patients who initiated tetrabenazine, 23.1% (87/377) discontinued tetrabenazine therapy. The most common reasons for discontinuation (multiple reasons could contribute to discontinuation) were ineffective treatment of chorea (42/87, 48.3%), patient or caregiver request to discontinue (34/87, 39.1%), and AEs or tolerability issues (33/87, 37.9%).
Healthcare resource utilization and severity of HD chorea
Among the total patient cohort, 39.8% (204/512) patients had mild chorea, 44.3% (227/512) had moderate chorea, and 15.8% (81/512) had severe chorea. Compared with patients with moderate or mild chorea, patients with severe chorea had more emergency room visits (severe [mean±SD]: 0.8±1.6; moderate: 0.5±1.1; mild: 0.2±0.6, hospitalizations (severe: 0.7±1.3; moderate: 0.3±0.7; mild: 0.1±0.6, and days hospitalized (severe: 5.6±18.0; moderate: 1.0±3.1; mild: 0.4±1.5) in the 12 months before the chart review (one-way ANOVA showed statistical difference between mild, moderate, and severe groups, P < 0.001 for all measures) (Table 3). Differences in healthcare resource use between those who discontinued tetrabenazine and those who persisted on tetrabenazine were also observed. Those who discontinued reported more ER visits, hospitalizations, and days hospitalized (all P < 0.05) (Table 4). There were more inpatient admissions and longer average length of stay, contributing to higher healthcare resource costs. There were no differences in the number of office visits based on disease severity or tetrabenazine use. Given the nature of the study (chart review), cost information was not available for further analysis.
Healthcare resource utilization in the past 12 months by chorea severity
All P values compare severe chorea to mild and moderate; CI, confidence interval; ER, emergency room; HD, Huntington disease; SD, standard deviation.
Differences in healthcare resource utilization in the past 12 months between HD patients who discontinued and persisted on tetrabenazine (N = 377)
All P values compare patients who discontinued tetrabenazine with those who persisted with tetrabenazine. CI, confidence interval; ER, emergency room; HD, Huntington disease; SD, standard deviation.
DISCUSSION
We conducted a retrospective chart review of patients with HD via an online data collection form to examine treatment patterns and the clinical context of these treatment patterns. Although previous studies have shown that tetrabenazine is efficacious at reducing chorea in HD patients, results from this study suggest that many HD patients may not be able to tolerate higher doses or fail to achieve optimal chorea control despite receiving the maximum dose.
Tetrabenazine dosing patterns from this study differ slightly from the findings of previous studies of tetrabenazine use in HD chorea patients [8, 10]. A majority of the HD patients in TETRA-HD required more than 50 mg/day dosages for optimal chorea control, and were receiving approximately 75 mg/day at Week 12 [9]. During the open-label extension of TETRA-HD, most patients received either 50 or 75 mg/day [10]. In the current study, the mean dose observed was generally lower (48.7 mg/day), with a majority of the patients receiving 50 mg/day or less. These findings suggest that HD patients may not be receiving the doses needed for optimal chorea control in clinical practice.
While a slight majority of patients stopped titration of tetrabenazine because they achieved chorea control, a large portion of patients (42.6%) stopped titration due to intolerability at higher doses or because they reached the maximum dose without achieving optimal chorea control. This is consistent with the findings from the TETRA-HD trial where dose escalation was discontinued or study drug dose was reduced because of one or more adverse reactions in 52% of patients [8]. Similarly, a majority of patients in the open-label study (84–86%) stopped dose escalation or had a decrease in dose [10]. This finding suggests both that poor tolerability may prevent many patients from reaching an optimal dose for chorea control. The most common reasons for discontinuing tetrabenazine were inadequate efficacy, patients or caregivers request to discontinue, and AEs or tolerability issues, further suggesting that poor efficacy and tolerability may contribute to physician, patient, or caregiver decisions to discontinue tetrabenazine treatment. Almost one-quarter of patients were discontinued due to reimbursement, access, or co-pay issues, suggesting that tetrabenazine costs may also limit its use.
In addition, we found that more than 25% of the HD patients identified were never treated with tetrabenazine, despite the fact that tetrabenazine was the only FDA-approved treatment for HD chorea until April 3, 2017. Many HD patients were not initiated on tetrabenazine due to comorbid depression or anxiety, suggesting that physicians may be hesitant to prescribe tetrabenazine due to concerns about mood-related tolerability given extant psychiatric comorbidities [8]. Of the 135 patients who did not initiate tetrabenazine, all but 17 were prescribed other medications, suggesting their symptoms warranted treatment; however, we cannot exclude the possibility that some patients had symptoms that were too mild to treat.
Based on healthcare resource utilization over the previous 12 months, increased severity of chorea was associated with increased numbers of emergency room visits, hospitalizations, and days hospitalized, suggesting that inadequate treatment of chorea, which worsens as HD progresses, may lead to a greater burden on healthcare resources. However, we cannot rule out the possibility that the increase in hospitalizations was due to other comorbidities such as dysphagia or psychiatric complications, or falls not related to chorea. Overall, healthcare resource utilization was significantly higher in patients who discontinued tetrabenazine than in patients who persisted on tetrabenazine. This chart review study indicates that physicians may be unable to titrate to the optimal dose, highlighting the potential unbalanced risk–benefit profile of tetrabenazine. The findings from this study highlight the need for additional treatment options that are efficacious and associated with better tolerability for HD chorea.
There are some limitations to the analyses. First, the study was underpowered to assess the relative contribution of comorbidities other than chorea to the increased healthcare burden of patients with Huntington disease. In addition, the mainly descriptive nature of the survey questions and characteristics of the study may have compromised the external validity of the data. Several steps were taken to ensure data quality, including conducting the pilot test of the data collection form, using skip logic to make sure respondents were only asked relevant questions, checking ranges to minimize erroneous responses, and having multiple researchers periodically check the survey to assure the accuracy of the program. To mitigate the likelihood that physicians might select patient charts preferentially and introduce bias into the sample, physicians were asked to select the most recent cases. Because the physicians in the study were members of an online panel, it is possible they may differ demographically from the general population. We attempted to minimize this bias by recruiting physicians from a panel with broad and diverse representation.
Another limitation is the potential subjective nature of the assessments. For chorea severity assessment, only 30% of patients had reported UHDRS scores available, and the remainder of the assessments were based on the neurologists’ ratings. Although not strictly specified, based on the inclusion criteria for neurologists in this study, the physician sample likely consisted of movement disorder specialists who were able to accurately estimate chorea severity in their patients. While the current study population differed in sex distribution from the open-label study (31% vs 65% female, respectively) this study may represent a more ethnically diverse population of patients with HD (70% vs 95% Caucasian) [10].
Although many patients with HD chorea initiate therapy with tetrabenazine, more than 20% of them are unable to continue treatment. Many HD chorea patients who were prescribed tetrabenazine experienced poor tolerability issues at high doses, potentially resulting in suboptimal dosing and discontinuation of therapy. New safer and more tolerable treatment options, such as deutetrabenazine [12–14], may improve treatment outcomes, and minimize healthcare resource use. Further study of deutetrabenazine is needed to determine whether tolerability, efficacy, clinical outcomes, and healthcare utilization are improved in clinical practice.
CONFLICT OF INTEREST
Daniel O. Claassen Grant support: NIH/NINDS, Michael J. Fox Foundation, Huntington Disease Society of America, Vaccinex, AbbVie, Auspex Pharmaceuticals. Consulting fees: Teva Neuroscience, Lundbeck, Acadia, AbbVie.
Ravi G. Iyer Employee of Teva Pharmaceutical Industries.
Bijal Shah-Manek was an employee of Ipsos Healthcare at the time of the study.
Marco DiBonaventura was an employee of Ipsos Healthcare at the time of the study.
Victor Abler was an employee of Teva Pharmaceutical Industries at the time of the study.
Victor W. Sung Consultant: Teva and Lundbeck.
Footnotes
ACKNOWLEDGMENTS
This study was funded by Teva Pharmaceutical Industries, Petach Tikva, Israel. We thank Kristen Hokenson, PhD (Chameleon Communications International with funding from Teva Pharmaceutical Industries) for editorial assistance in the preparation of this report.