
Abstract
Background:
Due to high prevalence of cognitive impairment in Huntington’s disease (HD) gene mutation carriers, even before onset of motor symptoms, cognitive screening is important for the optimal management of patients. The Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) are widely used, but the validity for HD has only been evaluated in few studies with important limitations.
Objective:
To evaluate the discriminative validity of the MMSE and the MoCA for the assessment of cognitive dysfunction in HD gene mutation carriers, independently of motor manifestation and furthermore, to report estimated probabilities for cognitive impairment with different score ranges on the MMSE and the MoCA.
Methods:
106 pre-motor-manifest and motor-manifest HD gene mutation carriers and 40 non-HD gene mutation carriers were administered the MMSE, the MoCA, and an extensive neuropsychological battery with operationalized criteria for cognitive impairment. The same physician and the same neuropsychologist performed all examinations; blinded to one another.
Results:
The area under the receiver operating characteristic (ROC) curve was 0.70 for the MMSE and 0.82 for the MoCA. The latter correctly diagnosed 82% of the cognitively impaired and not-impaired HD gene mutation carriers and non-HD gene mutation carriers, whereas the MMSE only diagnosed 73% correctly.
Conclusions:
The MMSE and the MoCA can both be used as cognitive screening tests in HD gene mutation carriers, but both have important limitations. Our results indicate that the MoCA is a better cognitive screening test for HD than the MMSE. In addition, our study provides estimated probabilities for cognitive impairment with different score ranges, which may be used as clinical guidelines in the interpretation of results from the two tests.
Keywords
INTRODUCTION
Huntington’s disease (HD) is an autosomal-dominant, progressive neurodegenerative disorder, characterized by a triad of motor, cognitive, and psychiatric symptoms caused by an expanded CAG trinucleotide repeat in the Huntingtin gene [1]. The clinical diagnosis has traditionally been based on the presence of motor symptoms alone, but cognitive dysfunction is one of the hallmarks of HD and may precede the onset of motor symptoms by many years [2–4]. As the cognitive decline has a progressive nature over time, cognition can be considered a key target for symptomatic treatment. Furthermore, cognitive symptoms contribute significantly to impaired functioning and have a great impact on patients’ daily lives. Thus, it is essential to identify the first signs of cognitive impairment and to follow the patients with ongoing cognitive evaluations.
Neuropsychological examination is the ‘gold standard’ for the assessment of cognitive deficits, but such testing is time-consuming and requires specialist knowledge. Cognitive screening instruments are widely used to assess possible cognitive impairments, but very few studies have investigated the discriminative validity of such tests in HD.
The cognitive profile of HD reflects the degeneration of the striatum and the dysfunction of frontostriatal circuits. This disruption leads to early cognitive changes, predominantly in the domains of executive functioning, psychomotor speed, and attention [5, 6].
The Mini-Mental State Examination (MMSE) [7] is the most commonly used screening test for neurodegenerative diseases, but the test may have ceiling effects and it lacks items to assess executive functions and complex attention [8]. More recently, the Montreal Cognitive Assessment (MoCA) [9] was developed to detect mild cognitive impairment (MCI) and capture performance deficits in a wider array of cognitive domains and range of difficulty than is achieved by the MMSE [9].
To our knowledge, only three previous studies have compared the use of the MMSE and the MoCA in patients with HD [10–12]. However, none of the studies used a neuropsychological test for cognitive impairment. One study compared the results of 53 motor-manifest HD gene mutation carriers on the MMSE and the MoCA and found that significantly more patients were classified as cognitively impaired at given cut-off scores on the MoCA compared to the MMSE [10]. The authors concluded that this finding might indicate that MoCA is superior to the MMSE for assessing HD gene mutation carriers. However, this study lacked a ‘healthy’ control group and did not use neuropsychological tests to classify cognitive impairment. Two other studies compared the same instruments in cohorts of 39 [11] and 104 [12] motor-manifest HD gene mutation carriers (both with healthy controls), with the assumption that the HD gene mutation carriers were all cognitively impaired, and the healthy controls not cognitively impaired. The former study found the MoCA to be superior to the MMSE, whereas the latter study found that the two instruments were equally good. Thus, the previous studies have methodological limitations, among these a lack of classification for cognitive impairment. In a small study including only 20 HD patients, the MoCA was compared to results from a brief standardized battery of neuropsychological tests. It was concluded that the MoCA is a suitable tool for assessing cognitive dysfunction in patients with HD, but the study did not include the MMSE [13].
The objective of the present study was to evaluate the discriminative validity of both the MMSE and the MoCA as tools for the assessment of cognitive dysfunction in HD gene mutation carriers. We aimed to compare the results from these instruments to a cognitive classification by a standardized and comprehensive neuropsychological battery previously validated as being sensitive to cognitive dysfunctioning in HD [2]. Finally, we aimed to report estimated probabilities for cognitive impairments with different score ranges on the MMSE and the MoCA for clinical use.
METHODS
Participants
Participants were recruited from January 2012 to March 2013 from the Neurogenetics Clinic, Danish Dementia Research Centre, Rigshospitalet. A total of 106 HD gene mutation carriers with a CAG repeat ≥39 and a Unified Huntington’s Disease Rating Scale-99 total motor score ≤55 (UHDRS-TMS) [14] were eligible for inclusion. Furthermore, only participants with a score of ≥24 on the MMSE and ≥19 on the MoCA were included, because the neuropsychological testing was thorough and too demanding for patients with more severe cognitive impairment.
HD gene mutation carriers with a UHDRS-TMS score of >5 were classified as motor-manifest HD gene mutation carriers (N = 55), and if the score was ≤5, indicating no substantial motor signs, they were classified as pre-motor-manifest HD gene mutation carriers (N = 51).
In addition, 40 non-HD gene mutation carriers (who were offspring of an HD gene mutation carrier and had been genetically tested with a CAG repeat length <30) were included. Exclusion criteria were other neurological illness, ongoing alcohol or drug abuse, and having a native language other than Danish. All individuals had undergone genetic counselling and were informed of their genetic status prior to (and independent from) study enrolment.
Procedure
The study was approved by the Ethics Committee of the Capital Region of Denmark (H2-2011-085), and written informed consent was obtained from each participant before enrolment.
All participants had a minimum of two planned visits. At one visit psychiatric screening, Hamilton Depression Rating Scale-17 (HAM-D17) [15, 16], physical, neurological examinations (including UHDRS-TMS) and cognitive screening (MMSE and MoCA) were completed. At another visit neuropsychological testing was performed. The two visits were conducted in random order, and 83% of the evaluations were conducted within 14 days of each other and only three (2%) of the evaluations were performed more than three months apart. All evaluations were performed blinded to one another, and the same physician and the same neuropsychologist conducted all examinations.
Cognitive screening instruments
The same physician performed the cognitive screening of all participants, namely 106 HD gene mutation carriers and 40 non-HD gene mutation carriers, using both the MMSE and the MoCA. Scores for both tests range from 0–30 points. In each case, higher scores indicate better performance. The instruments were administered during the same visit, and always in the same order. The MMSE was administered in the beginning of the visit and the MoCA was administered later (with several other assessments in between). The overlapping items (e.g., orientation questions) were always repeated and never copied from the MMSE to the MoCA.
The MMSE remains the most frequently used cognitive screening instrument and was developed by Folstein, Folstein & McHugh [7]. It is administered in about 10 minutes, and assesses different cognitive domains: Orientation: time and place (10 points) Registration: repetition of three nouns (3 points) Attention and calculation: serial subtraction (5 points) Episodic memory: Recall of three nouns (3 points) Language: naming two objects (pencil and wrist watch) (2 points), sentence-repetition (1 point), following a verbal command (3 points), reading (1 point), and writing (1 point) Visuospatial function: copying two overlapping pentagons (1 point)
The MoCA is a more recent cognitive screening instrument developed by Nasreddine and colleagues in 2005 [9], initially designed for detecting MCI.
It is administered in about 10 minutes, and assesses different cognitive domains: Episodic memory: recall of five nouns after 5 min (5 points) Visuospatial function: Clock-drawing test (3 points) and cube copying (1 point) Executive function: modified Trail making test B (1 point), phonemic fluency (1 point), verbal abstraction (2 points) Attention: target detection using tapping (1 point), serial subtraction (3 points), and digit span forward and backward (2 points) (6 points) Language: Animal-naming (lion, camel, rhinoceros) (3 points) and sentence repetition (2 points). Orientation: time and place (6 points)
Classification of cognitive impairment based on neuropsychological examination
The same neuropsychologist performed the neuropsychological testing of all participants, blinded from the results from the physician visit, and blinded from HD carrier status. All participants were tested with a battery of neuropsychological tests. Attention/Psychomotor speed was assessed with Trail Making Test A & B [17] (only completion time used for analyses) and Symbol Digit Modalities Test [18]. Memory was assessed with the Selective Reminding Test, both immediate recall (errors were recorded) and delayed recall (retention interval 10 minutes) [19] and Rey Complex Figure Test (recall 3 minutes) [20]. Visuospatial functions were assessed using Rey Complex Figure Test [20], Ravens Progressive Matrices (set 1) [21], and a modified version of the Block Design Test [22]. Executive functions were assessed with the Stroop test (only performance on the incongruent version was used for analyses, completion time) [23], and we also applied three verbal fluency tests: Category fluency (animals, 1 minute) and Lexical fluency (s-words and a-words, 1 minute); these measures were analysed separately. The performances on the specific tests in the neuropsychological battery have been published elsewhere [2].
The method for classifying cognitive impairment was determined prior to study enrolment and has also been used in other studies [24, 25].
The tests were administered in a fixed order. General IQ levels were estimated using the Wechsler Adult Intelligence Scale (WAIS) Vocabulary subtest – raw score, DART (Danish Adult Reading Test), an equivalent of the NART [26], and an education index score. The education index score (range, 8–17) was calculated as the sum of years of schooling (range, 7–12) and the level of post-secondary education stratified into groups (range, 1–5) based on a method previously used by Mortensen and Gade [22].
Based on the neuropsychological examination, all participants, HD-gene carriers as well as non-HD gene carriers, were classified as cognitively impaired or not impaired. To evaluate impairment on the neuropsychological tests we used regression-based normative data based on 80 healthy participants, retrieved from a database at the Department of Neurology, Rigshospitalet, Copenhagen University Hospital. For each participant, expected scores for each test were generated from factors based on regression analyses including age, education index, WAIS Vocabulary subtest, and DART. The difference between the expected score and the observed score was used to evaluate whether the result on each neuropsychological test was impaired. A score in the lowest 10% was categorized as impaired. The following criteria for classifying a patient as cognitively impaired were applied: a) if four (or more) test performances were categorised as impaired; b) if all test performances in a domain (except psychomotor-speed/attention) were impaired; c) if performances on all tests in the psychomotor speed/attention domain, and if at least one other test, were below the cut-off.
Statistical analyses
Group comparisons were performed using one-way analysis of variance (ANOVA) and Dunnett’s post-hoc test for pairwise comparisons (2-sided). Based on the neuropsychological assessment, all participants were classified as cognitively impaired or not impaired. Within group comparisons of performance on the MoCA and MMSE between participants classified as cognitively impaired or not impaired were performed for each group (non-HD gene carriers, pre-motor-manifest HD, and motor-manifest HD) using independent samples t tests.
Using receiver-operating characteristic (ROC) analyses, we examined the ability of the two screening instruments to differentiate between cognitively impaired and not impaired participants. The ROC analyses yield sensitivity and specificity statistics, and a graphical representation of how well each instrument classifies cognitively impaired and not impaired participants beyond a chance level (50%). The optimal cut-off scores for discriminating between the two groups were determined using Youden’s Index J (sensitivity + specificity-1) [27].
Likelihood Ratios (LR) were calculated and combined with pre-test odds in order to estimate post-test odds and post-test probability for cognitive impairment. The positive LR (LR+) is the probability of a positive test result in cognitively impaired participants / probability of a positive test result in not cognitively-impaired participants (SN/(1-SP)), pre-test odds are pre-test probability/ (1-pre-test probability), post-test odds are pre-test odds*LR+, post-test probability is post-test odds/(1+ post-test odds) [28].
Statistical analyses were performed using SPSS version 22 for Windows with a two-tailed level of significance set at 0.05.
RESULTS
Table 1 shows demographic information and clinical characteristics for HD gene mutation carriers and non-HD gene mutation carriers. The motor-manifest HD gene mutation carriers were significantly older, significantly less educated, had significantly lower scores on the DART and Vocabulary, and, furthermore, they had significantly higher scores on HAM-D17 relative to the non-HD gene mutation carriers. The only significant difference between motor-manifest and pre-motor-manifest HD gene mutation carriers was in age. The pre-motor-manifest HD gene mutation carriers were significantly younger than the non-HD gene mutation carriers. The motor-manifest HD gene mutation carriers scored significantly lower on both the MMSE and MoCA relative to pre-motor-manifest HD gene mutation carriers and non-HD gene mutation carriers.
Demographic information and clinical characteristics for HD gene mutation carriers and non-HD gene mutation carriers shown as mean (SD) (range)
†Significant difference from non-HD gene mutation carriers, p≤0.05. ‡Significant difference from non-HD gene mutation carriers, p < 0.001. *Significant difference from pre-motor-manifest HD gene mutation carriers, p < 0.001. aDanish Adult Reading Test, bWechsler Adult Intelligence Scale, cUnified Huntington’s Disease Rating Scale Total Motor Score, dHamilton Rating Scale for Depression-17, eMini-Mental State Examination, fMontreal Cognitive Assessment.
Using the classification for cognitive impairment, 2/40 non-HD gene mutation carriers were classified as cognitively impaired on the neuropsychological test battery, comparable with the lower 5% of a normal distribution.
Table 2 shows within-group comparisons of performances on the MMSE and MoCA between participants classified as cognitively impaired and not impaired, based on the neuropsychological test battery. The analyses in Table 2 were controlled for age, education, DART-score, WAIS vocabulary subtest, and HAM-D17. The motor-manifest HD gene mutation carriers classified as cognitively impaired scored significantly lower on MoCA than the motor-manifest HD gene mutation carriers classified as not impaired. This difference was not found for the MMSE. There were no significant differences on the MMSE and MoCA between cognitively impaired and not impaired participants in the pre-motor-manifest group and the non-HD gene mutation carriers.
Within group comparisons of cognitively impaired and not cognitively impaired participants’ test performances on the MMSE and the MoCA for HD gene mutation carriers and non-HD gene mutation carriers
Note: Results are shown as mean (standard deviation). *Significant difference from not cognitively impaired motor-manifest HD gene mutation carriers, p≤0.05. aMini-Mental State Examination, bMontreal Cognitive Assessment.
Of the seven pre-motor-manifest HD gene carriers classified as cognitively impaired on neuropsychological testing, only one person scored 25, and the rest scored in the range 27 to29 on the MoCA. All seven scored 29 or30 on the MMSE.
Using ROC analyses, the discriminative validities of the MMSE and MoCA were examined as compared to neuropsychological assessment (Table 3 and Fig. 1). The Area under the curve values demonstrate that both screening instruments significantly discriminated between cognitively impaired and not impaired participants; however, the MoCA yielded higher sensitivity and specificity than the MMSE at the point of maximum sensitivity and specificity, and a higher percentage of correctly diagnosed. Youden’s J was 0.35 for the MMSE and 0.50 for the MoCA.
Discriminative validity statistics for the MMSE and the MoCA
Note: AUC = Area under the (receiver operating characteristic) curve; P = Probability value; SN = Sensitivity; SP = Specificity. *At the point of maximum combined sensitivity and specificity. aMini-Mental State Examination, bMontreal Cognitive Assessment.
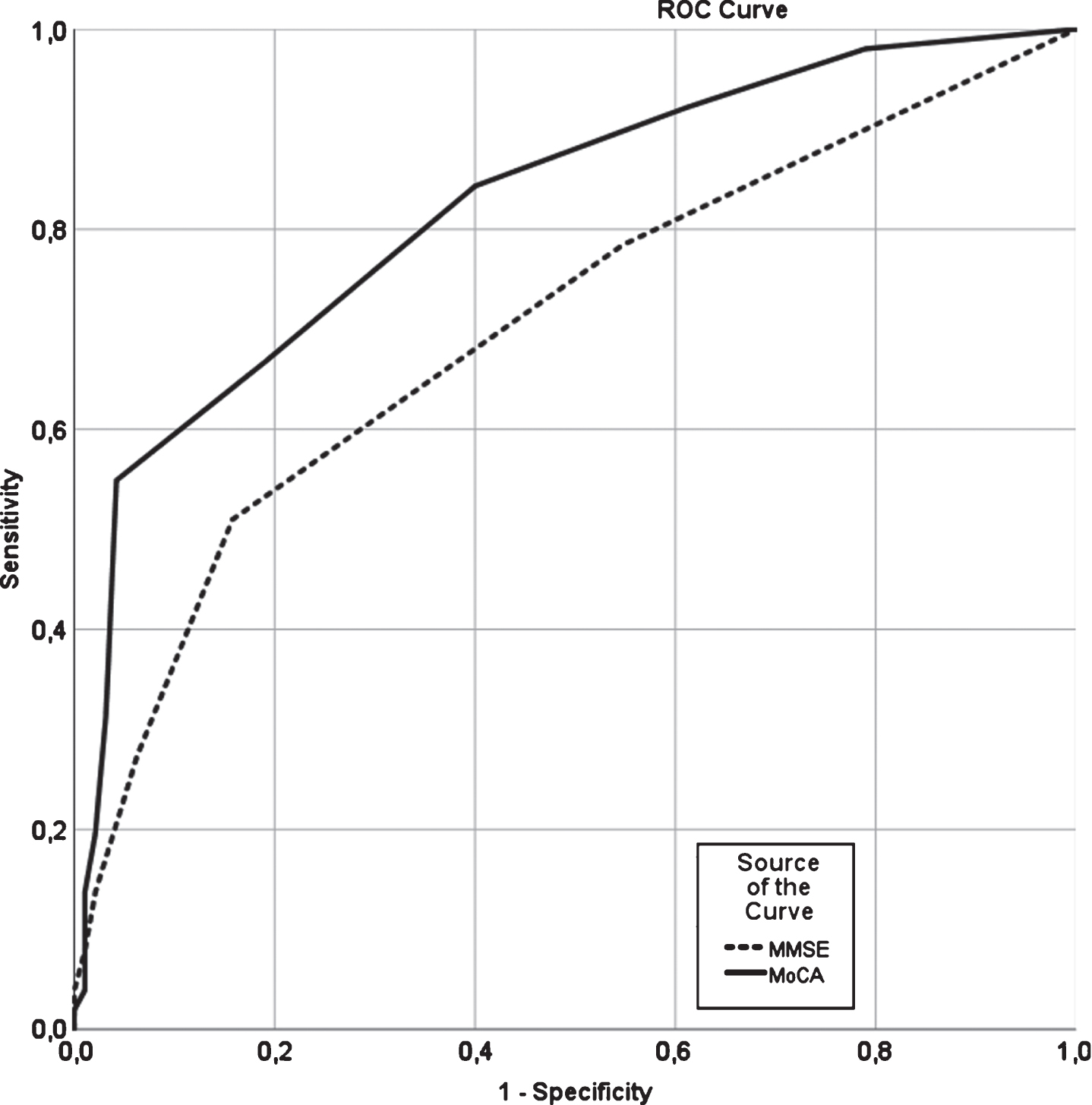
Receiver operating characteristic curve showing the Mini-Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MoCA) discriminative capability in cognitively impaired and not cognitively impaired HD gene mutation carriers and non-HD gene mutation carriers. MMSE: (AUC (95% CI) = 0.703 (0.611–0.796); p = 0.001), MoCA: (AUC (95% CI) = 0.822 (0.749–0.895); p = 0.001).
Table 4 shows the probability of cognitive impairment at different score ranges on MMSE and MoCA. Rather than using a single, fixed cut-off for optimal discrimination between groups (Table 3), it is clinically more relevant to consider the LRs and post-test probabilities associated with the full score range and categorize performances accordingly (Table 4). As a rule of thumb, LR’s ≥10 have a large positive impact on post-test probability, LRs between 5–10 have a moderate impact, LRs between 2–5 have a small impact whereas an LR around 1 has no effect on post-test probability [29]. From this analysis it can be estimated that a MoCA score range of ≤25 is associated with a high-moderate probability of cognitive impairment, whereas an MMSE score range of ≤26 is only associated with moderate probability of cognitive impairment.
Likelihood ratios for a positive test result, post-test odds, post-test probability and estimated probability of cognitive impairment associated with selected score ranges on the MMSE and the MoCA
MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment.
DISCUSSION
The clinical diagnosis of HD has traditionally been based on the presence of motor symptoms alone, but cognitive dysfunction is one of the hallmarks of the disease, and may precede the onset of motor symptoms by many years [2–4]. Therefore, it is essential to identify such early cognitive impairments.
Neuropsychological assessment provides a cognitive profile and may be considered to be the ideal for cognitive evaluation, but such testing is time-consuming and is not available in all neurogenetics clinics. Short cognitive screening tests are less comprehensive, but are widely used for brief evaluations.
Even where cognitive screening tests are typically part of routine assessment in HD gene mutation carriers, their validity has only been studied in very few studies all of which have methodological differences and important limitations. The present study has investigated the ability of two of the most commonly-used screening instruments, namely the MMSE and the MoCA, to identify cognitive impairment as classified by a large neuropsychological battery validated in HD gene mutation carriers [2]. These instruments were applied in a comparatively large cohort of both motor-manifest and pre-motor-manifest HD gene mutation carriers.
Our results showed that both the MMSE and the MoCA had important limitations with respect to identifying patients with and without cognitive deficits, as defined by the neuropsychological assessment. The area under the ROC curve was 0.70 for the MMSE, which is typically considered “fair”, and 0.82 for the MoCA, generally considered “good”. However, the sensitivity at the point of maximum combined sensitivity and specificity was only 51% for the MMSE (cut-off 28/29) and 55% for the MoCA (cut-off 25/26). These results indicate, that clinicians using such cut-off scores may misclassify their patients. Approximately half of the HD-gene-carriers would be categorized as ‘cognitively intact’, but some of them have cognitive deficits on more comprehensive neuropsychological tests. This may have important consequences for both the patients and caregivers. Detecting the first signs of cognitive impairment can be important to be able to take the precautions needed, for example, to maintain a job, and to get the social services needed to maintain a good quality of life. Furthermore, our results indicate that the discriminative validity of the screening tests is poor in pre-motor-manifest HD gene carriers, with less cognitive impairment than the motor-manifest carriers. Only one of the seven cognitively impaired pre-motor-manifest HD carriers scored below the cut-off on the MoCA and none of the seven was identified by the optimal cut-off on the MMSE.
Despite the poor sensitivity, the above cut-offs for MMSE and MoCA are the most optimal in our cohort. Both instruments are widely used, and there have been published more than 100 studies about the use of the MMSE and more than 20 studies about the use of MoCA for classifying dementia [30]. In a large Cochrane review aimed to determine the diagnostic accuracy of the MMSE at various cut points for dementia in people aged 65 and over, 15 studies used a cut-off 24/25, and 10 studies used a cut-off 25/26, for a dementia yes/no distinction [31]. Both cut-offs are considerably below the optimal cut-off for the MMSE in our study (28/29) for detecting cognitive impairment.
One of the reasons for the considerable difference in MMSE cut-offs in our study compared to its use in broader dementia diagnostics could arise from the selection of items on the MMSE, that may be more suitable for memory disorders such as Alzheimer’s disease than for HD, characterized by attentional and executive impairments rather than memory problems. The MoCA was originally developed to detect MCI using a cut-off score at 25/26 [9], which, in contrast to the MMSE cut-offs, is consistent with the optimal cut-off for MoCA in our study.
Compatible with the above comparison of generally-used cut-off scores and the optimal cut-offs in our cohort, our results indicate that impairment on the MoCA has a stronger association with impaired results on neuropsychological testing than low scores on the MMSE. The MoCA correctly diagnosed 82% of the cognitively impaired and not cognitively impaired HD gene mutation carriers and non-HD gene mutation carriers, whereas the MMSE only diagnosed 73% correctly.
MoCA’s superiority over the MMSE may be explained by the selection of items on the MoCA, which may be more optimal for the cognitive difficulties of HD. However, further analyses of correspondence between results on neuropsychological testing and affected domains on the screening instruments is beyond the scope of the present article.
Another possible explanation for the superiority of the MoCA is that it contains items that seem more demanding than those of the MMSE. Therefore, the MoCA might be more sensitive for detecting milder cognitive impairment [9].
Despite the extensive use and many publications regarding the MMSE and the MoCA, only three previous studies have investigated the use of both instruments for HD [10–12]. Two of the studies compared performances of motor-manifest HD gene mutation carriers with those of healthy controls, on the MoCA and the MMSE, assuming that the HD gene mutation carriers were all cognitively impaired [11, 12], and the third study lacked a healthy control group, while only comparing the results of motor-manifest HD gene mutation carriers on the MMSE and the MoCA at different cut-off points [10]. Most importantly, none of the three studies used a comprehensive test for cognitive impairment in the evaluation, which is a serious limitation. Only a small study including 20 HD patients, compared the MoCA with results from a brief standardized battery of neuropsychological tests, and found it to be a suitable tool for assessing cognitive dysfunction in HD [13]. However, the study did not include the MMSE.
In the present study, we had a comparatively large cohort of HD gene mutation carriers (N = 106) and a group of non-HD mutation carriers (N = 40), and used a classification based on a neuropsychological battery as the comparison base for cognitive impairment in the discriminative validation of the screening instruments. Since cognitive deficits often occur before the onset of motor symptoms in HD, we did not restrict our analyses to motor-manifest HD gene mutation carriers but also investigated cognitive symptoms in pre-motor-manifest HD gene mutation carriers.
In addition to evaluating the discriminative validity of the instruments, we also provided an overview of score ranges and probability of cognitive reduction for both instruments for clinical use. Even though our analyses show that neither of the instruments is optimal for identifying cognitive impairment in HD gene mutation carriers compared to a full neuropsychological assessment, both instruments are widely used in HD gene mutation carriers (and other patient groups) and this may be relevant dependent on the intended purpose. To our knowledge, probabilities for cognitive impairment on cognitive screening tests have not been described previously in HD gene mutation carriers.
When using cognitive screening instruments, there are several methods for interpreting the result and evaluating the cognitive function of the patient. One can choose to use a fixed cut-off score indicating cognitive impairment or not. However, this yes/no distinction, for optimal discrimination between groups, does not provide very useful information of the continuum of cognitive function. From a clinical point of view an estimate of the probability of whether the performance of a given patient is impaired given his or her specific score seems more useful. This probability can be estimated by combining the LR associated with the patient’s specific score with the pre-test odds of the condition of interest. Calculating post-test odds and post-test probabilities for any specific score may optimize case-finding and clinical decision-making compared to a traditional fixed cut-off approach. From our analyses, we have provided estimated probabilities for cognitive impairment with different score ranges on the MMSE and the MoCA for HD gene mutation carriers. These can be used as clinical guidelines when using the MMSE and the MoCA for cognitive screening in HD.
The present study is not without its own limitations. We applied predefined criteria for cognitive impairment, earlier used for HD gene mutation carriers [2]. Choosing specific criteria for cognitive impairment was necessary in order to conduct the present analyses, but such a cut-off is an arbitrary distinction on what is a continuum of cognitive function. We believe our criteria are consistent with rather obvious cognitive impairment, which would suggest that the cognitive screening instruments are even poorer at identifying milder cognitive dysfunction than our study shows.
The included HD gene mutation carriers in our cohort all had MMSE scores >23 and MoCA scores >18, indicating at worst only rather mild cognitive impairment. Consequently, our cohort only includes the reasonably well-functioning HD gene mutation carriers and is not representative of the HD population in general. This was chosen because the study was comprehensive with several examinations over two days and was thus not suitable for more severely impaired patients. We assume that more severe cognitive impairment would be more likely to be correctly classified on both screening instruments. Therefore, it is reasonable to think that our results would have been different if our cohort had also included more severely cognitively impaired HD gene mutation carriers.
In attempting to evaluate the usefulness of the MMSE and the MoCA for classifying cognitively impaired and not impaired persons, it is a limitation of our study, that it does not include healthy controls, who did not grow up in HD-families.
In summary, the MMSE and the MoCA can be used as cognitive screening tests in HD gene mutation carriers. But results from these tests should be interpreted with some caution as they both have limitations identifying patients with and without cognitive impairment, as defined by comprehensive neuropsychological testing. For HD where most of the gene mutation carriers will develop cognitive impairment even in the earliest phases (and in some cases before motor symptoms occur) neuropsychological assessment will be relevant to identify possible cognitive impairment. However, our results indicate that the MoCA is a better screening test for cognitive deficits associated with HD than the MMSE. This finding is in line with those from other studies [11, 12], and findings from studies of other disorders involving frontal and subcortical networks [32–38]. In addition, this study provided estimated probabilities for cognitive impairment with different score ranges on the cognitive screening tests, which may be used as a clinical guideline in the interpretation of results from the MMSE and the MoCA.
We do not have any specific recommendations for the use of these screening instruments for HD in clinical practice. However, our study does indicate that the MMSE cannot be recommended as a screening tool for HD, and furthermore that a score of 25 or below on the MoCA is a clear indication of cognitive impairment. Referral to a neuropsychological assessment and more thorough cognitive evaluation should never solely be based on results from the screening tests, but should also depend on the individual patient and circumstances, possible cognitive complaints and the need of a more detailed profile of the cognitive functions.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank the Danish Health Foundation and the Danish Ministry of Health for support to the Danish Dementia Research Centre. We also thank Emeritus Associate Professor Thomas W. Teasdale for proofreading of the final manuscript.
Ida Unmack Larsen and Tua Vinther-Jensen were both supported by grants from Copenhagen University. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.