
Abstract
Background:
Psychiatric symptoms are widely prevalent in Huntington’s disease (HD) and exert greater impact on quality of life than motor manifestations. Despite this, psychiatric symptoms are frequently underrecognized and undertreated. Lack of awareness, or anosognosia, has been observed at all stages of HD and may contribute to diminished patient self-reporting of psychiatric symptoms.
Objective:
We sought to evaluate the impact of anosognosia on performance of commonly used clinical rating scales for psychiatric manifestations of HD.
Methods:
We recruited 50 HD patients to undergo a formal psychiatrist evaluation, the Problem Behavior Assessment-Short Form (PBA-s), and validated self-report rating scales for depression, anxiety, and anger. Motor impairment, cognitive function, and total functional capacity were assessed as part of clinical exam. Patient awareness of motor, cognitive, emotional, and functional capacities was quantified using the Anosognosia Rating Scale. Convergent validity, discriminant validity, classification accuracy, and anosognosia effect was determined for each psychiatric symptom rating scale.
Results:
Anosognosia was identified in one-third of patients, and these patients underrated the severity of depression and anxiety when completing self-report instruments. Anosognosia did not clearly influence self-reported anger, but this result may have been confounded by the sub-optimal discriminant validity of anger rating scales.
Conclusion:
Anosognosia undermines reliability of self-reported depression and anxiety in HD. Self-report rating scales for depression and anxiety may have a role in screening, but results must be corroborated by provider and caregiver input when anosognosia is present. HD clinical trials utilizing patient-reported outcomes as study endpoints should routinely evaluate participants for anosognosia.
INTRODUCTION
Psychiatric symptoms affect 87–99% of Huntington’s disease (HD) patients [1, 2]. Commonly observed psychiatric manifestations of HD include depression, anxiety, irritability, anger, apathy, obsessiveness, and delusions [1, 3]. These symptoms worsen quality of life (QOL) to a greater extent than motor aspects of the disease [4–6]. Moreover, depression [7, 8], anxiety [7, 8], and irritability [5] are associated with increased likelihood of suicidal ideation and attempts. Despite their prevalence and detrimental effects, psychiatric symptoms in HD are under-recognized and infrequently addressed in clinical settings. There are limited placebo-controlled studies that assess treatments for these symptoms [9, 10], and thus, clinicians must rely on clinical experience and consensus guidelines when taking care of patients [11–13].
Numerous challenges hinder accurate identification, quantification, and treatment of psychiatric symptoms in HD. These include frequent co-occurrence of symptoms, imprecise diagnostic classification (e.g., apathy), reduced insight and/or impaired cognition limiting patients’ ability to self-report symptoms, and limited access to mental health providers familiar with HD. A host of clinical rating scales have been employed to screen for neuropsychiatric symptoms and/or quantify their severity [14, 15], but as highlighted recently in the Movement Disorders Society Committee on Rating Scale Development, there is need for further validation of many of these scales in HD populations [14]. Reliability of self-report scales is a particular concern in HD as many patients exhibit anosognosia, or lack of insight. Anosognosia may occur in the context of cognitive decline, but it has been observed at early, and even pre-motor manifest, stages of HD [16, 17]. The impact of anosognosia on symptom measurement is critical to determine, since self-report behavioral and QOL scales are increasingly utilized as endpoints in clinical trials and in routine clinical care.
The primary objective of this study was to evaluate the impact of anosognosia on diagnostic performance of commonly used clinical rating scales for psychiatric manifestations of HD. We recruited 50 HD patients to undergo assessments of psychiatric symptoms through a formal psychiatrist evaluation, the Problem Behavior Assessment-Short Form (PBA-s) (administered by certified, non-physician staff), and validated unidimensional symptom rating scales, comprised of self-report and caregiver-report measures. We hypothesized that the PBA-s ratings would closely align with the psychiatrist evaluation and that self-report measures would provide acceptable, but less robust, validity compared to the PBA-s.
METHODS
Between December 2018 and August 2019, we prospectively recruited and enrolled 50 HD patients from the Vanderbilt University Medical Center Level 1 Huntington’s Disease Center of Excellence. Eligible subjects included any adult patient (≥18 years of age) with a clinical diagnosis of HD and at least one psychiatric symptom. Patients were excluded who had severe cognitive, behavioral, or communicative symptoms that precluded completion of the psychiatric interview and/or rating scales. Both patients and primary caregivers provided written consent to participate. The study was approved by the Institutional Review Board of Vanderbilt University Medical Center.
Psychiatrist evaluation
All patients completed a standard psychiatric interview performed by a board-certified psychiatrist with extensive clinical experience in HD (J.S.). A caregiver or other knowledgeable informant participated in the interview for 42 patients. Identified symptoms and disorders were classified per Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) criteria, when applicable. Apathy and anosognosia are not well defined in the DSM-V [14]. At the completion of the interview, the psychiatrist used a 4-point Likert scale (“absent,” “mild,” “moderate,” “severe”) to rate the severity of six neuropsychiatric symptoms: depression, anxiety, apathy, obsessive-compulsive behaviors, agitation/irritability, and psychosis. These six symptoms were selected based on prior literature defining five subscales of the behavioral section of the Unified Huntington’s Disease Rating Scale (UHDRS): depression, apathy, obsessive-compulsive behaviors, irritability/aggression, and psychosis [3]. For this study, anxiety was also incorporated because it is independently associated with suicidal ideation [8] and impacts functional ability and QOL [18].
PBA-s
The PBA-s is a validated, semi-structured interview comprised of 11 items, with each item, as listed in Table 3, addressing a specific neuropsychiatric manifestation of HD [2, 19]. The PBA-s was selected for use in this study because it has demonstrated good reliability, is widely used in clinical care and in clinical research, and is less time-intensive than its parent 40-item instrument, the Problem Behaviors Assessment in HD [19]. For each PBA-s item, severity and frequency of a neuropsychiatric symptom are rated on a 5-point scale. Traditionally, severity and frequency ratings are multiplied to generate an overall item score. However, a recent Rasch analysis identified psychometric problems with this approach, leading some investigators to advise that frequency and severity scores be considered independently [20]. In accord with this recommendation, PBA-s severity and frequency scores were analyzed separately in this study. The PBA-s was administered in neurology clinic by certified, non-physician staff experienced with the scale. A caregiver or other knowledgeable informant participated in the semi-structured interview for 48 patients.
Unidimensional symptom rating scales
Unidimensional symptom rating scales consisted predominantly of self-administered questionnaires validated in non-HD populations. The only two non-self-administered scales were the Hamilton Anxiety Rating Scale (staff-administered) and Family Version of the Frontal Systems Behavior Assessment (caregiver-reported). The Hamilton Anxiety Rating Scale (HAM-A) is not strictly a patient-reported outcome, given that the patient’s response to each item is interpreted and then rated by the interviewer. For the purposes of this study, the HAM-A is grouped with other self-report scales because it relies predominantly on patient response, with no caregiver input. Due to budgetary and participant fatigue considerations, the Self-Report Version of the FRSBe was not used. Scales were administered either in person at the same visit as the PBA-s or online in the week prior via a secure, HIPPA-compliant online platform (REDCap) [21, 22]. Properties of the scales are outlined in Table 1.
Clinical Rating Scales
At the same visit the PBA-s was conducted, trained personnel administered the Montreal Cognitive Assessment (MoCA) [23], UHDRS Motor Assessment (UHDRS-Motor) [24], UHDRS Total Functional Capacity (UHDRS-TFC) [25], and Anosognosia Rating Scale [26]. The Anosognosia Rating Scale is an instrument in which identical, 8-item forms are provided separately to a patient and his/her clinician. Each is asked to rate the patient’s ability to perform the following: ambulate, coordinate hand/finger movement, speak, remember, concentrate/attend, sit still and quietly, retrieve words, and control emotion. Items are rated on a 5-point Likert scale ranging from “extremely poor” (–2) to “exceptionally well” (+2). The clinician rates the patient following a clinical interview and examination and is blinded to the patient’s responses. A patient total score and a provider total score are tabulated by summing individual item scores on the respective forms. A difference score is then calculated by subtracting the patient’s total score from the clinician’s. A rating of anosognosia is present if the participant score is 6 points greater than the clinician score.
The psychiatry evaluation and in-clinic assessments were pre-specified to occur within two weeks of each other in order to mitigate confounding from temporal fluctuation in symptoms. The psychiatrist was blinded to rating scale results, and neurology staff were blinded to the psychiatrist assessment.
Statistics
Shapiro-Wilks test was used to ascertain normality of variable distributions. Significance threshold was set at 0.05 for all statistical tests. Raw scale scores were used for calculations of reliability, validity, and classification accuracy.
To assess internal consistency, we calculated Cronbach’s alpha for unidimensional rating scales, as well as for patient and clinician forms of the Anosognosia Rating Scale. A minimal acceptable cutoff of 0.70 is acceptable based on prior psychometric analyses of neuropsychiatric rating scales in HD [27]. For PBA-s Severity, PBA-s Frequency, and psychiatry ratings, each constituent scale item was treated independently, rather than in aggregate, so Cronbach’s alpha was not calculated for these measures.
To determine convergent and discriminant validity, we conducted a multi-trait multi-method analysis, constructing correlation matrices based on psychiatrist evaluation, PBA-s, and unidimensional rating scales. Spearman’s rank correlations were used since cohort scores for multiple scales were non-normally distributed.
To assess classification accuracy, we performed a receiver operating characteristic (ROC) analysis. Psychiatrist ratings were dichotomized into “absent” and “present,” the latter category encompassing “mild,” “moderate,” and “severe” ratings. This binary metric served as the reference standard for the ROC analysis. We sought to determine classification accuracy of the scales as screening tools. As such, sensitivity was prioritized over specificity, with a desired sensitivity of greater than or equal to 0.90 for each scale.
Lastly, to evaluate anosognosia impact, participants were grouped based on the established cut-off from the Anosognosia Rating Scale (Difference Score ≥6 consistent with anosognosia) [26]. Between-group comparisons were performed with Wilcoxon-rank sum test statistic.
RESULTS
Descriptive
Fifty-seven patients consented to participate in the study. Seven were unable to attend the two separate study visits within two weeks and were not included in the analysis. Thirty-five patients underwent psychiatry evaluation, PBA-s, and in-clinic scales on the same day. Of the 15 patients evaluated on separate days, 8 were assessed by psychiatry first and 7 by neurology staff first. One patient was unable to return for psychiatry evaluation until 6 weeks following the PBA-s visit; for all other patients, the two study visits occurred within 2 weeks of each other. Table 2 outlines the clinical characteristics of patients who completed both study visits. Ninety-two percent of patients were taking prescribed psychotropic medications at the time of the in-clinic assessments.
Cohort Clinical Characteristics
*Mean (standard deviation). #CAG-age product score, as per Zhang 2011 [48]. ∧Staging classification as per Thompson 2012 [37]. +Medication use at time of in-person clinic assessments.
Per psychiatrist evaluation, 96% of patients had at least one of the six target symptoms; 84% had two or more, 52% had three or more, and 16% had four or more. Over half (52%) of patients exhibited concurrent depression and anxiety. Other frequently co-occurring symptoms included anxiety and apathy (40%); anxiety and agitation/irritability (32%); depression and apathy (30%); depression and agitation/irritability (28%); and apathy and agitation/irritability (22%). Table 3 shows mean scores and standard deviations for all assessments; internal consistency reliability is reported where appropriate. Figure 1 shows the severity distributions for depression, anxiety, apathy, and agitation/irritability by assessment method. Psychosis and obsessive-compulsive behaviors were infrequent, each being observed by the psychiatrist in only 8%.
Neuropsychiatric Symptom Scores by Assessment Method
+Likert scale ratings for psychiatry evaluation: 0 “absent,” 1 “mild,” 2 “moderate,” 3 “severe”.

Percentage of Patients in Given Severity Classification, by Rating Scale. Reference cutoffs for scales other than the PBA-s are based on non-HD populations. For purposes of cross-scale comparison in the figure, some scale classifications are modified: PHQ-9 ratings of “moderate” and “moderately severe” are collapsed into ”moderate,” HAM-A ratings of “moderate-to-severe” (the most severe category for that scale) are included in “severe,” and PBA-s Severity ratings of “minimal” and “mild” are collapsed into “min/mild.” PBA-s Frequency ratings are not shown. “Psych-” prefix denotes psychiatrist rating. *FrSBe-Apathy T-score classification: absent <65, mild ≥65 and <75, moderate ≥75 and <85, severe ≥85.
Reliability
Cronbach’s alpha exceeded 0.90 for all NeuroQOL/PROMIS measures and FrSBe-Apathy, while it ranged between 0.80 and 0.90 for PHQ-9, HAM-A, and both Patient and Clinician Forms of the Anosognosia Rating Scale.
Convergent validity
Table 4 contains the correlation matrix for psychiatry ratings with PBA-s Severity item scores, unidimensional rating scale scores, and relevant clinical measures. The correlation matrix for PBA-s Severity and Frequency item scores with rating scale scores is available in the Supplementary Material. Subsequent results and discussion focus on PBA-s Severity, though in general, similar trends were observed for both Severity and Frequency items.
Correlation Matrix for Psychiatry Severity Ratings
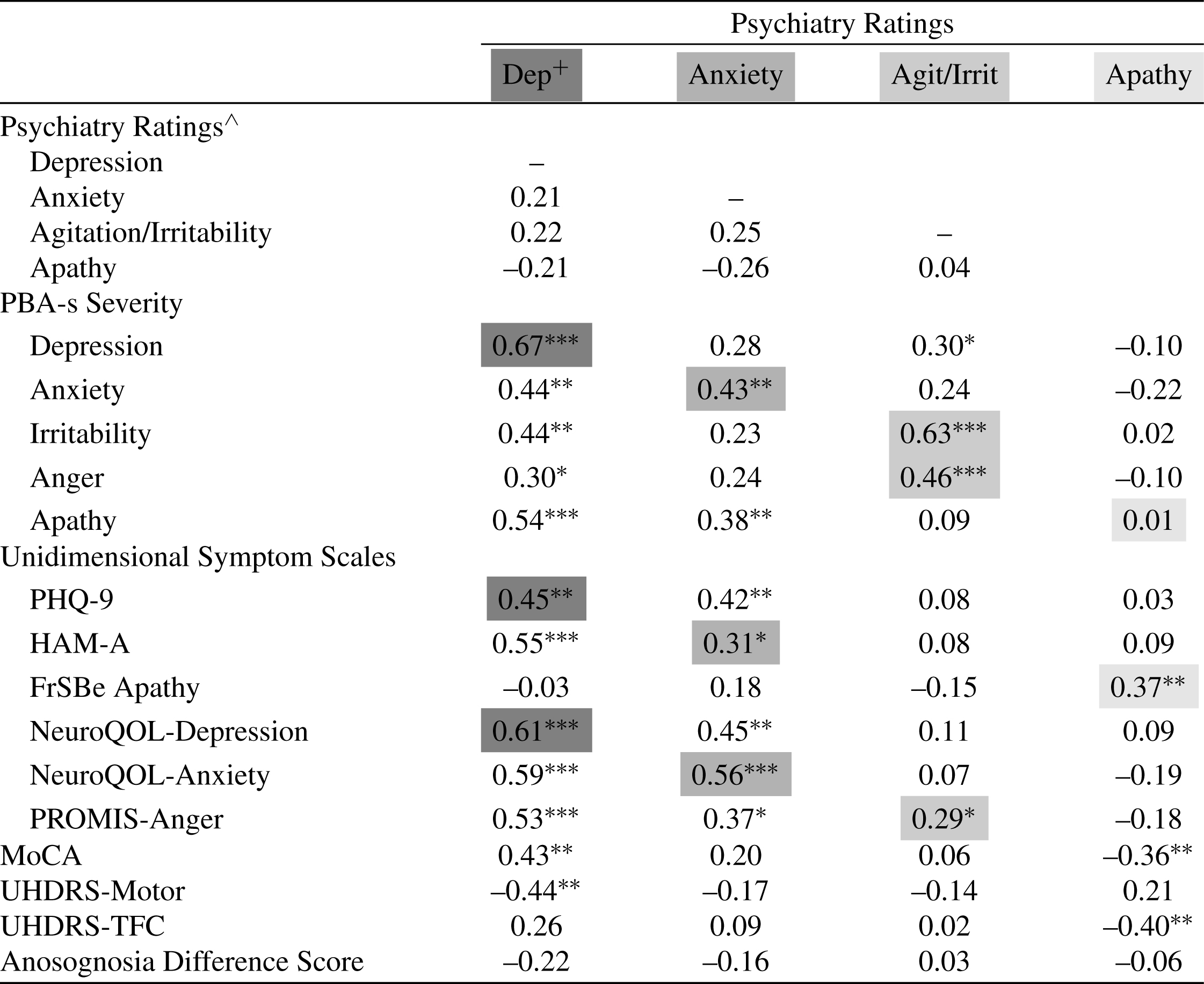
*p < 0.05; **p < 0.01; ***p < 0.001. +Shared gray shading indicates shared underlying construct. ∧Correlation coefficients for ordinal psychiatrist ratings with raw scale scores.
Psychiatry ratings correlated strongly (ρ > 0.60; see Table 4 for significance levels) with scores for PBA-s Depression Severity, PBA-s Irritability Severity, and NeuroQOL-Depression; moderately (0.40 < ρ< 0.60) with scores for PBA-s Anxiety Severity, PBA-s Anger Severity, PHQ-9, and NeuroQOL-Anxiety; and mildly (0.20 < ρ< 0.40) with scores for HAM-A, PROMIS-Anger, and FrSBe-Apathy. Psychiatrist apathy ratings did not correlate at all with PBA-s Apathy Severity scores. Prevalence of obsessive-compulsive and psychosis symptoms was insufficient to permit meaningful correlational analysis. Unidimensional symptom scales for depression, anxiety, and anger exhibited moderate convergent validity (ρ> 0.40) with counterpart PBA-s items (see Supplementary Material). PBA-s Apathy Severity and FrSBe-Apathy scores showed only mild correlation (ρ= 0.31).
Discriminant validity
Psychiatry ratings for depression, anxiety, agitation/irritability, and apathy were not statistically significantly correlated, consistent with good discriminant validity. PBA-s Anger Severity also demonstrated relatively good discriminant validity. However, scores for many of the PBA-s Severity items significantly inter-correlated: Apathy and Depression (ρ= 0.62); Depression and Anxiety (ρ= 0.49); and Irritability with both Depression (ρ= 0.42) and Anxiety (ρ= 0.45). Scores for unidimensional rating scales also frequently correlated with each other across symptom constructs. In particular, there was strong correlation (ρ> 0.60) between many of the anxiety and depression measures (see Supplementary Material).
Associations with motor, cognitive, and functional measures
UHDRS-Motor score significantly negatively correlated with psychiatry depression rating (ρ= –0.44), PBA-s Apathy Severity score (ρ= –0.52), and PROMIS-Anger score (ρ= –0.40), suggesting these symptoms lessen as motor scores worsen. MoCA score positively correlated with psychiatry depression rating (ρ= 0.43), indicating cognitive decline is associated with less severe depression. UHDRS-TFC score negatively correlated with psychiatrist apathy rating (ρ= –0.40) and FrSBe-Apathy score (ρ= –0.43); PBA-s Apathy Severity and Frequency score did not have a significant correlation with UHDRS-TFC score.
Sensitivity and specificity
Table 5 shows area under the curve (AUC) values of PBA-s Severity and unidimensional symptom rating scales for the most prevalent psychiatric symptoms. All scales showed acceptable AUC, with exception of PROMIS-Anger and apathy measures.
ROC Analysis
+Lowest cutoff possible failed to provide >90% sensitivity. #Raw scores used, as opposed to T-scores.
Anosognosia impact
More than one-third (34%) of patients displayed anosognosia. There was no significant relationship between Anosognosia Rating Scale Difference Score and scores for MoCA (ρ= –0.23, p = 0.11), UHDRS-Motor (ρ= 0.13, p = 0.37), or UHDRS-TFC (ρ= 0.14, p = 0.33). Anosognosia Rating Scale Difference Score correlated mildly with PBA-s Apathy score, but not with psychiatry apathy rating, FrSBe-Apathy score, or any other PBA-s Severity score. Anosognosia Rating Scale Difference Score moderately correlated with PHQ-9, NeuroQOL-Depression, and Neuro-QOL Anxiety scores, indicating that diminished insight is associated with lower severities of self-reported depression and anxiety.
Stratifying by anosognosia status, significant between-group differences emerged for PHQ-9, NeuroQOL-Depression, HAM-A, and NeuroQOL-Anxiety scores (Table 6). In contrast, no between-group differences were evident for psychiatry or PBA-s ratings of depression and anxiety. Groups diverged on PBA-s Apathy score but not on psychiatry apathy rating or FrSBe-Apathy score. Anger and irritability measures, MoCA score (z = 1.57, p = 0.12), UHDRS-Motor score (t = –0.76, p = 0.46), and UHDRS-TFC score (t = –0.63, p = 0.54) did not differ between those with anosognosia and those without anosognosia.
Comparison of Neuropsychiatric Symptom Ratings by Anosognostic Status
*ADS = Anosognosia Rating Scale Difference Score. +n = 47, comprised of 15 with ADS≥6 and 32 with ADS < 6.
DISCUSSION
Two main findings emerged from this study comparing patient-reported ratings to structured interviews (PBA-s) and expert psychiatric assessments of HD patients. First, structured interviews (PBA-s) are effective at detecting clinically relevant symptoms of depression, anxiety, and irritability, but may suffer at distinguishing apathy from depression. Second, select unidimensional rating scales have utility in assessing HD psychiatric symptoms, but anosognosia does influence self-reporting of depression and anxiety. In our relatively early stage cohort, anosognosia was present in more than one-third of patients, and the degree of anosognosia did not correlate significantly with typical measures of disease severity (UHDRS-Motor, MoCA, UHDRS-TFC). These results align with prior studies observing anosognosia at early and even pre-motor manifest stages of HD [16, 17]. We discuss the implications of these findings for clinical practice and research applications.
Depression and anxiety
PBA-s Depression, PBA-s Anxiety, and the NeuroQOL instruments all showed acceptable convergent validity and classification accuracy. These measures corresponded more closely to psychiatrist ratings and performed better on ROC analysis than PHQ-9 or HAM-A. All depression and anxiety scales exceeded the acceptable AUC cutoff of 0.70 [27, 28], but only the PBA-s items permitted sensitivity of 90% or better accompanied by specificity of greater than 70%. With the exception of the psychiatrist evaluation, discriminant validity of all depression and anxiety measures was relatively poor. The high degree of inter-correlation between depression and anxiety scales suggests two, non-mutually exclusive possibilities: selected scales do not adequately distinguish between these symptoms (e.g., PHQ-9 is quantifying both depression and anxiety) and/or the severity of these symptoms truly co-varies. Depression and anxiety have been observed to frequently co-occur in HD [18], and more than half of our cohort was diagnosed with concurrent depression and anxiety by the psychiatrist. Despite their prevalent coexistence in our sample, the psychiatrist discriminated well between depression and anxiety while the rating scales did not.
The relatively poor specificity of depression and anxiety self-report scales in HD is due in part to anosognosia. Patients with anosognosia had lower scores on the PHQ-9, NeuroQOL-Depression, HAM-A, and Neuro-QOL-Anxiety, and the extent of anosognosia inversely correlated with each of these measures. These findings suggest that patients with diminished awareness have less severe depression and anxiety. However, by both psychiatrist and PBA-s interview, those with anosognosia were determined to have similar degrees of depression and anxiety as those without anosognosia. Both psychiatry evaluation and PBA-s incorporated provider and informant input, which likely accounts for their superior convergent and discriminant validity compared to the scales relying on patient-report without collateral information. Taken together, it is evident that anosognosia impairs reliable self-reporting of depression and anxiety in HD, and accurate assessment of these symptoms requires interviews with both the patient and an informant (preferably a caregiver).
The prevalence and scope of anosognosia in HD has become increasingly apparent in recent years [16]. Based on an analysis of the PREDICT-HD cohort, half of HD patients are unaware of motor symptoms at the time of motor diagnosis [29]. Awareness of memory deficits, on the other hand, appears intact at early disease stages but declines with disease progression [30]. While several studies have explored anosognosia as it pertains to cognitive and motor manifestations of HD, little research has been devoted to patient self-awareness of psychiatric symptoms [16]. A previous study noted good agreement between HD patients and their caregivers when both were asked to rate patient depression with the Beck Depression Inventory [31]. In our study, we did not identify anosognosia by comparing scores from identical patient-report and informant-report rating scales for individual psychiatric symptoms. Rather, we utilized an anosognosia scale that evaluates insight into broad functional, motor, and emotional domains. Unawareness in HD is not uniform across symptoms or capacities so measures that probe patient insight into multiple facets of the disease may detect anosognosia more readily [16].
Importantly, these results do not necessarily suggest patient perspective is less integral to care in the presence of anosognosia. Insight into deficits may vary across symptoms, with retained awareness in some domains and reduced awareness in others. Furthermore, the variability of anosognosia in HD over time is unclear so insight may fluctuate between clinical assessments. Beyond these pragmatic factors, consideration must be given to the ethical principles of medical decision-making, a discussion of which is beyond the scope of this article [32]. Findings from this study do emphasize the need to regularly involve reliable collateral informants for patients with some degree of anosognosia.
Anger and irritability
Psychiatrist evaluation of agitation/irritability converged well with PBA-s Irritability Severity, moderately with PBA-s Anger Severity, and poorly with PROMIS-Anger. This suggests the constructs of agitation and irritability only partially overlap with the construct of anger. Scores on PBA-s Anger Severity, PBA-s Irritability Severity, and PROMIS-Anger correlated strongly, but these measures demonstrated relatively poor discriminant validity in the context of comorbid depression and anxiety. Evidence from our study and others does suggest a true co-occurrence of agitation and irritability with depression and anxiety. The psychiatrist identified coexisting depression and agitation/irritability in over one-fourth of our sample and coexisting anxiety and agitation/irritability in one-third. Prior research has shown that irritability parallels depression [33] and anxiety in HD [1, 33]. A study of 294 pre-manifest and manifest HD patients found that PROMIS-Anger correlated moderately with PBA-s Depression and PBA-s Anxiety, a finding replicated in our own study [27]. While evidence certainly indicates an authentic relationship between the constructs of agitation, irritability, and anger and those of depression and anxiety, lack of rating scale specificity may be inflating the extent of the observed relationship. In support of this possibility, we found no significant correlation between psychiatry ratings of agitation/irritability, depression, and anxiety.
Anosognosia did not appear to impact self-reported anger, but there was a non-significant (p = 0.09) interesting effect of lower PROMIS-Anger scores in those with reduced insight. Agreement between patients and caregivers on irritability has previously been shown to be only fair, this discrepancy widening as patient cognition deteriorates [31].
Apathy
Apathy measures in this study exhibited poor convergent validity. Psychiatrist evaluation and FrSBe-Apathy likely captured the apathy construct most accurately, given their modest correlation with each other and their superior discriminant validity relative to PBA-s Apathy. Additionally, psychiatry and FrSBe-Apathy ratings negatively correlated with functional capacity, and the former negatively correlated with cognitive function, mirroring known trends in HD. Apathy is the neuropsychiatric symptom most strongly linked with disease progression [34, 35].
Studies using alternate methods for identifying apathy in HD have arrived at highly variable prevalence rates, from 34% –76%, indicating that beyond differences in the populations sampled, assessment techniques may influence apathy detection [36]. Although conceptually distinct, apathy can be difficult to clinically separate from depression [37], made more challenging by the fact that these symptoms often co-occur [38]. The psychiatrist identified concurrent depression and apathy in 30% of participants, but the severities of these symptoms did not correlate. In contrast, PBA-s Apathy correlated moderately with multiple depression measures, leading us to postulate that PBA-s Apathy was at least partially tapping into depressive symptoms. Both depression and apathy can present with blunted interest, psychomotor slowing, loss of energy, and amotivation, but depression is typically accompanied by feelings of dysphoria whereas apathy is not [39]. Both symptoms can manifest in early stages of HD [3, 41], but with advancing stages the prevalence of apathy increases [34, 35] and that of depression decreases [40]. Thus, careful interrogation, with particular attention to dysphoria, and longitudinal evaluation are essential to differentiating these two common neuropsychiatric symptoms in an individual patient.
The presence of anosognosia did not appear to influence psychiatrist or caregiver ratings of apathy. No self-report measures of apathy were collected in this study so we cannot comment on anosognosia’s impact on this symptom.
This study had several limitations. First, we excluded patients in more advanced stages of HD, though this was necessary to ensure participants were able to complete the study protocol. Second, as we recruited patients with at least one psychiatric symptom noted by a clinician, our sample population may not reflect the broader cross-sectional prevalence of these symptoms in HD. However, this design facilitated assessment of rating scale discriminant validity. Third, few patients in our sample manifested obsessive-compulsive behaviors or psychosis, precluding meaningful comparison of these PBA-s items to psychiatrist evaluation. In the REGISTRY study of 1,993 HD mutation carriers, obsessive-compulsive behaviors were observed in 25.8% and psychosis in 4.1% [3]. In that study, each of these symptoms was associated with clinical markers of more advanced disease, including longer disease duration, greater motor impairment, and lower functional capacity. Given this, the low prevalence of obsessive-compulsive symptoms and psychosis is not unexpected in our predominantly early stage cohort. A larger sample population, inclusive of patients with more advanced disease, is needed to study anosognosia as it relates to these psychiatric symptoms of HD. Fourth, as a consequence of the observational nature of our study, the vast majority of patients were taking psychotropic medications, which themselves can induce or exacerbate neuropsychiatric symptoms. For example, selective serotonin reuptake inhibitors (SSRIs) carry a known risk of engendering apathy [42], and antipsychotics and benzodiazepines may cause emotional blunting and/or sedation that could be interpreted as evidence of depression and/or apathy. The prevalence of moderate and severe apathy and depression in our cohort aligned with findings from larger HD samples [3], but ultimately, disentangling the effect of pharmacotherapy on neuropsychiatric manifestations of HD will require controlled clinical trials, cross-sectional evaluation of patients not taking psychotropic medications, and/or serial assessments of patients following psychotropic medication adjustment. Lastly, 30% of study participants underwent psychiatry evaluation and in-clinic assessments on different days, which introduces a potential confound since psychiatric symptoms vary over time. We speculate the impact of this relatively narrow inter-visit time window on study findings was minimal.
Future research should prioritize development and validation of clinical rating scales for screening neuropsychiatric symptoms in HD and quantifying their severity [14]. Crucially, efforts should be made to clarify the impact of anosognosia on reliability of these scales. Ultimately, research activities in this arena should enhance recognition and facilitate treatment of neuropsychiatric symptoms in HD, with the ultimate goal of bettering patient quality of life.
In conclusion, existing standardized rating scales are valuable tools for identifying and quantifying psychiatric symptoms, but they require validation in HD populations. The PBA-s and NeuroQOL measures show superior psychometric properties compared to generic depression (PHQ-9) and anxiety (HAM-A) scales in HD. The NeuroQOL instruments performed well as screening tools, and they have the advantage over the PBA-s of being self-administered and time-efficient. However, self-report scales are less reliable measures of symptom severity in patients with anosognosia. Systematic screening for anosognosia is imperative in clinical trials using patient-reported outcomes, as unreliable self-report has the potential to compromise clinical endpoints. Routine monitoring of anosognosia over the course of a study should permit recognition of and statistical correction for this confound. For psychiatric symptom screening and quantification, the PBA-s is an appealing instrument given its scope and relative ease-of-use following appropriate rater training. The PBA-s administered by certified, non-physician staff exhibited acceptable psychometric properties and overall good agreement with psychiatrist ratings of common HD psychiatric symptoms, apathy being a notable exception. The FrSBe-Apathy subscale completed by a caregiver functioned as an adequate screen for this symptom. The prevalence and frequent co-existence of psychiatric manifestations in HD necessitates comprehensive, systematic evaluation for these symptoms.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank the study participants and study coordinators involved in this research.
The authors independently designed and conducted the study, and prepared the manuscript. The study described in manuscript was funded as an investigator-sponsored study by Teva Branded Pharmaceutical Products, R&D, Inc., who provided a courtesy medical review of the manuscript.