
Abstract
Background:
Huntington Disease-Like 2 (HDL2) is a rare autosomal dominant disorder caused by an abnormal CAG/CTG triplet repeat expansion on chromosome 16q24. The symptoms of progressive decline in motor, cognitive and psychiatric functioning are similar to those of Huntington’s disease (HD). The psychiatric features of the HDL2 have been poorly characterized.
Objective:
To describe the neuropsychiatric features of HDL2 and compare them with those of HD.
Methods:
A blinded cross-sectional design was used to compare the behavioural component of the Unified Huntington’s Disease Rating Scale (UHDRS) in participants with HDL2 (n = 15) and HD (n = 13) with African ancestry.
Results:
HDL2 patients presented with psychiatric symptoms involving mood disturbances and behavioural changes that were not significantly different from those in the HD group. Duration of disease and motor performance correlated (p < 0.001) with the Functional Capacity score and the Independence score of the UHDRS. HD patients reported movement dysfunction as the first symptom more frequently than HDL2 Patients (p < 0.001).
Conclusion:
The psychiatric phenotype of HDL2 is similar to that of HD and linked to motor decline and disease duration. Psychiatric symptoms seem more severe for HDL2 patients in the early stages of the disease.
INTRODUCTION
Huntington Disease-Like 2 (HDL2) is an autosomal dominant disorder caused by an abnormal CAG/CTG expansion mutation. Despite its rarity, it is considered the Huntington’s disease (HD) phenocopy most akin to HD, as they have clinically indistinguishable motor, cognitive and psychiatric phenotypes that progress and culminate in premature death [1].
Phenotypic descriptions of the neurological and neuropsychological symptoms of HDL2 are available [2, 3]. However, the psychiatric presentation of HDL2 has been poorly characterised, despite this being a core aspect of the clinical presentation of HDL2, and one which seems to precede the motor symptoms [4]. There are only 16 publications, which refer to neuropsychiatric aspects of HDL2. Table 1 compiles these data, which mostly involve a brief, and often vague, mention of psychiatric symptoms as part of clinical case descriptions that focus on other aspects of HDL2.
Summary of the psychiatric description available for case studies on HDL2
*Only article dedicated to the neuropsychiatry of HDL2.
Overall, these reports suggest that HDL2’s phenotype includes depression, personality/behavioural changes, aggressive behaviour, irritability followed by social withdrawal, apathy and sleep disorders. In contrast to HD, hallucinations, impulsivity and anxiety were infrequent and obsessive-compulsive symptoms have not been reported in HDL2. What we know of the neuropsychiatry of HDL2 is limited, but seems to resemble the behavioural and emotional presentation of HD. Specifically, the psychiatric symptoms are insidious and present throughout the course of both illnesses. In order to improve the characterization of the neuropsychiatric differences between HDL2 and HD, we conducted a blinded cross-sectional study comparing the behavioural and functional aspects of the UHDRS [5] from a sample of HDL2 cases and an equivalent sample of HD participants. The relatively high frequency of HDL2 in South Africa allowed us to ascertain this cohort.
METHODS
Sample recruitment and design
Twenty eight patients with a genetically confirmed diagnosis (HDL2 n = 15 and HD n = 13) were recruited through the Division of Human Genetics at the National Health Laboratory Service (NHLS) and the University of the Witwatersrand and took part in a research study designed to investigate the clinical phenotype of HDL2 [2]. The study used a cross-sectional design where an experienced neurologist (DGA) assessed the participants using the UHDRS, which is a research tool developed to monitor HD/HDL2 in terms of disease progression and assesses four domains of clinical performance namely motor function, cognitive function, functional capacity and behavioural/psychiatric abnormalities [5]. Clinical interviews with the patients and an unaffected collateral informant were used to obtain biographical and medical history. The age of onset was defined as the age at which the participants (and informant) reported their first movement symptom. The researchers were blind to the specific diagnosis (HD or HDL2) of the participants. Given that all HDL2 participants have African ancestry [6], only patients with an HD phenotype and African were recruited, to protect the blinding.
Ethical considerations
The study received ethical clearance from the Human Research Ethics Committee of The University of the Witwatersrand (M140872). An independent genetic counsellor provided detailed information about the study to patients and their families/carers during individual sessions, where she obtained formal consent.
Data analyses
SAS version 9.4 for Windows was used to conduct all analyses, with a 5% significance level. Independent samples t-tests compared groups on all continuous variables. Where data did not meet the assumptions of this test, the Wilcoxon rank sum test was used. The Fisher’s exact test compared categorical variables between groups. Comparisons of UHDRS total scores between groups were done with a General Linear Model with the score as the dependent variable, and disease group, the selected covariate, and their interaction, as the independent variables. The non-significant interactions were removed from the model for parsimony (see Supplementary Tables 1–4).
RESULTS
The two patient groups with HD and HDL2 respectively were not significantly different in terms of demographics (gender, race, and age), use of legal psychoactive substances, pharmacological treatment, and medical history, which included seizures, myoclonus, head injury with no loss of consciousness, HIV, hypertension, and psychiatric hospitalisations) (Tables 2 and 3).
Frequencies and comparisons between HDL2 and HD in all categorical demographic and clinical history variables
Frequencies and comparisons between HDL2 and HD in all continuos demographic and clinical variables
HD and HDL2 were significantly different in two clinical variables: disease duration and in showing movement dysfunction as the first symptom (more prevalent in HD than in HDL2) (Tables 2 and 3). Although the HD patients had been living with symptoms for longer than the HDL2 patients, the clinical features between the groups were not significantly different. The remaining clinical variables (repeat length, age of onset [reported age of first movement abnormality] and age of diagnosis) were not significantly different between the HDL2 and HD groups (Table 2).
The results yielded by the UHDRS Behavioural Assessment Severity items indicate that patients with HDL2 presented, at the time of the assessment, with a variety of neuropsychiatric symptoms that involved mild to severe presence of sadness, irritability, anxiety, obsessions, compulsions, low self-esteem, disruptive/aggressive behaviour, and delusions. Hallucinations were rare and suicidal thoughts were absent (Table 4). The UHDRS Behavioural Assessment Frequency items revealed that disruptive behaviours, depression, anxiety, and irritability were the most frequent symptoms for HDL2 patients. (Table 5). The scores on the general components of the UHDRS Functional Assessment (Table 7) indicate that the majority of the HDL2 patients were not able to perform a full time job. A small group needed full time assistance with the activities of daily living but none of the patients had full time care.
Frequencies and comparisons between HDL2 and HD in all categorical variables in the UHDRS
UHDRS Behavioural Assessment Frequency items
No significant differences between HD and HDL2 were found in the specific items of severity and frequency of the behavioural symptoms (Tables 4 and 5), in any of the UHDRS-FAS (Table 6), and in the General Assessment items of the UHDRS (Table 7). Similarly, comparisons between HDL2 and HD in the psychiatric components of the UHDRS, namely, Behavioural Assessment Severity Total, Behavioural Assessment Frequency Total, Independence Scale, and Functional Capacity Total, did not yield significant differences between groups when controlling for any of the covariates (Supplementary Tables 1–4).
UHDRS Functional Assessment Specific Tasks
UHDRS Functional Assessment General
Significant relationships were observed between the Functional Capacity score and the UHDRS Motor Testing Total score covariate (Fig. 1), between the Functional Capacity score and the duration of disease covariate (Fig. 2), between the Independence score and the UHDRS Motor Testing total score covariate (Fig. 3), and between the Independence score and the duration of disease covariate (Fig. 4) for both HDL2 and HD. Specifically, these analyses of covariance estimated a decrease in the Functional Capacity score of 0.14 units (95% CI 0.09–0.19) for every 1-unit increase in the Motor Testing total and a decrease in the same score of 0.7 units (95% CI 0.3–1.0) for every 1-year increase in disease duration. Moreover, the Independence score was estimated to decrease by 0.86 units (95% CI 0.66–1.06) for every 1-unit increase in the Motor Testing total and to decrease by 4.3 units (95% CI 2.8–5.8) for every 1-year increase in disease duration.
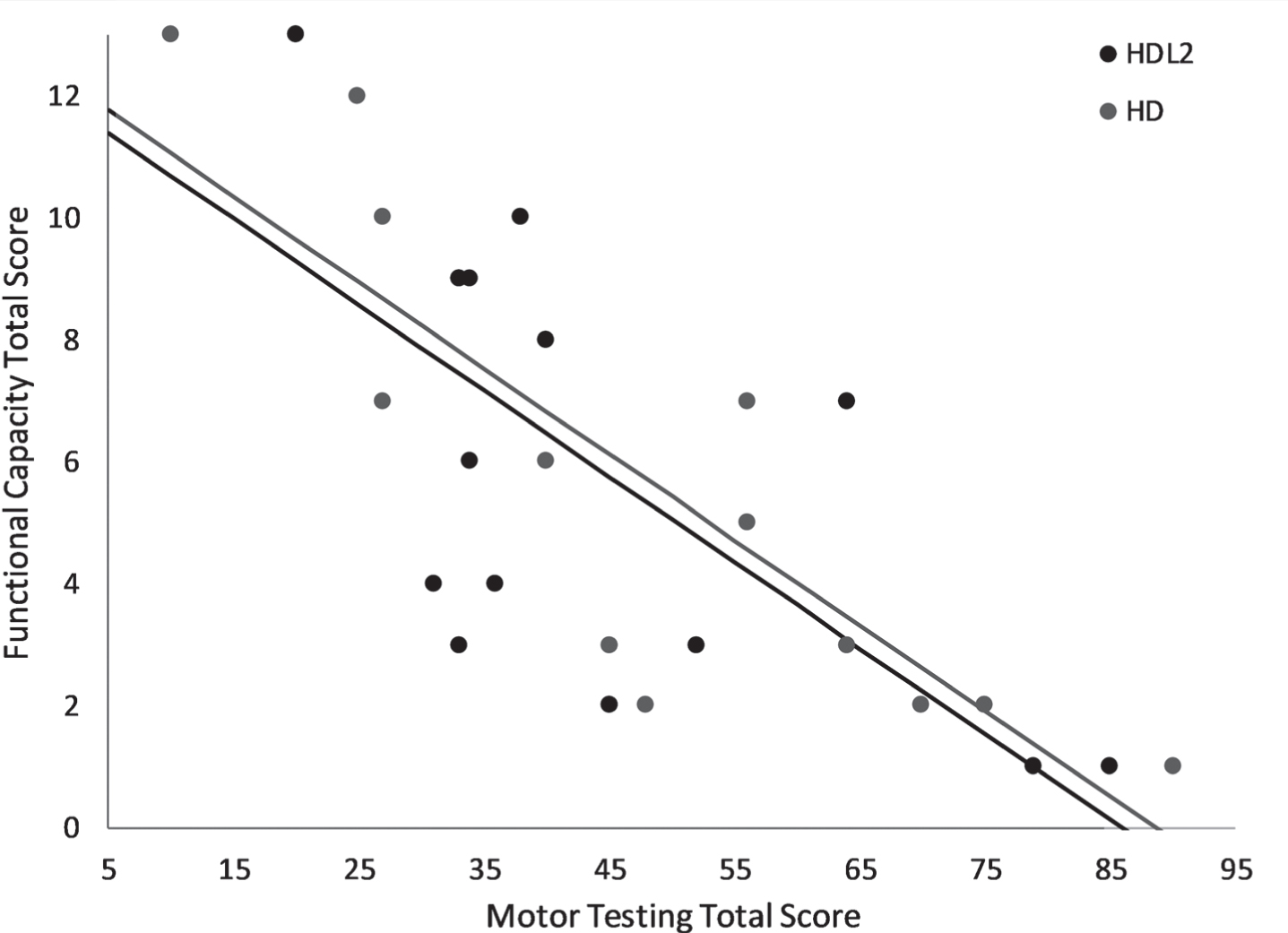
Analysis of covariance between Functional Capacity Total score and Motor Testing Total score.
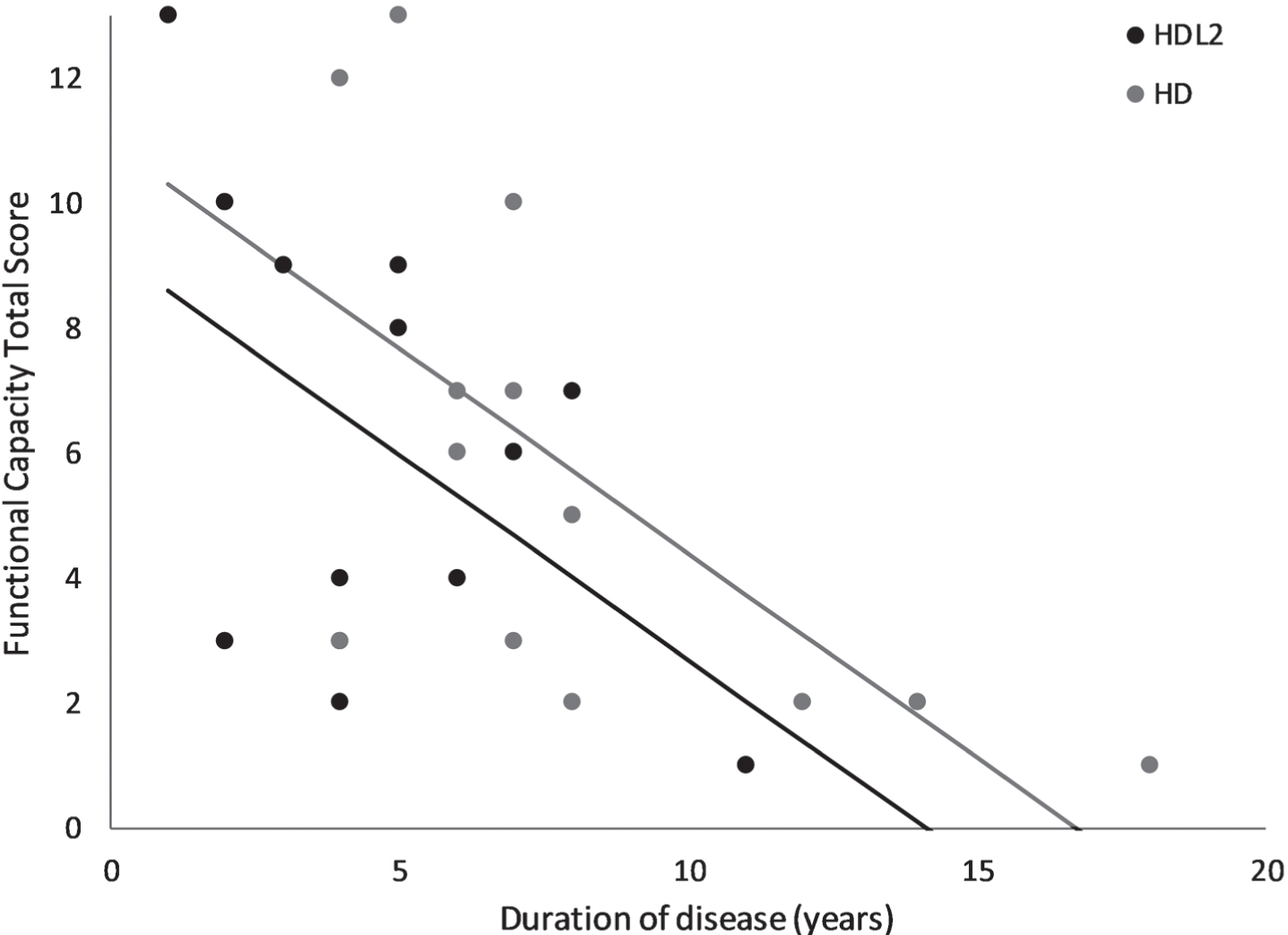
Analysis of covariance between Functional Capacity Total score and duration of disease.
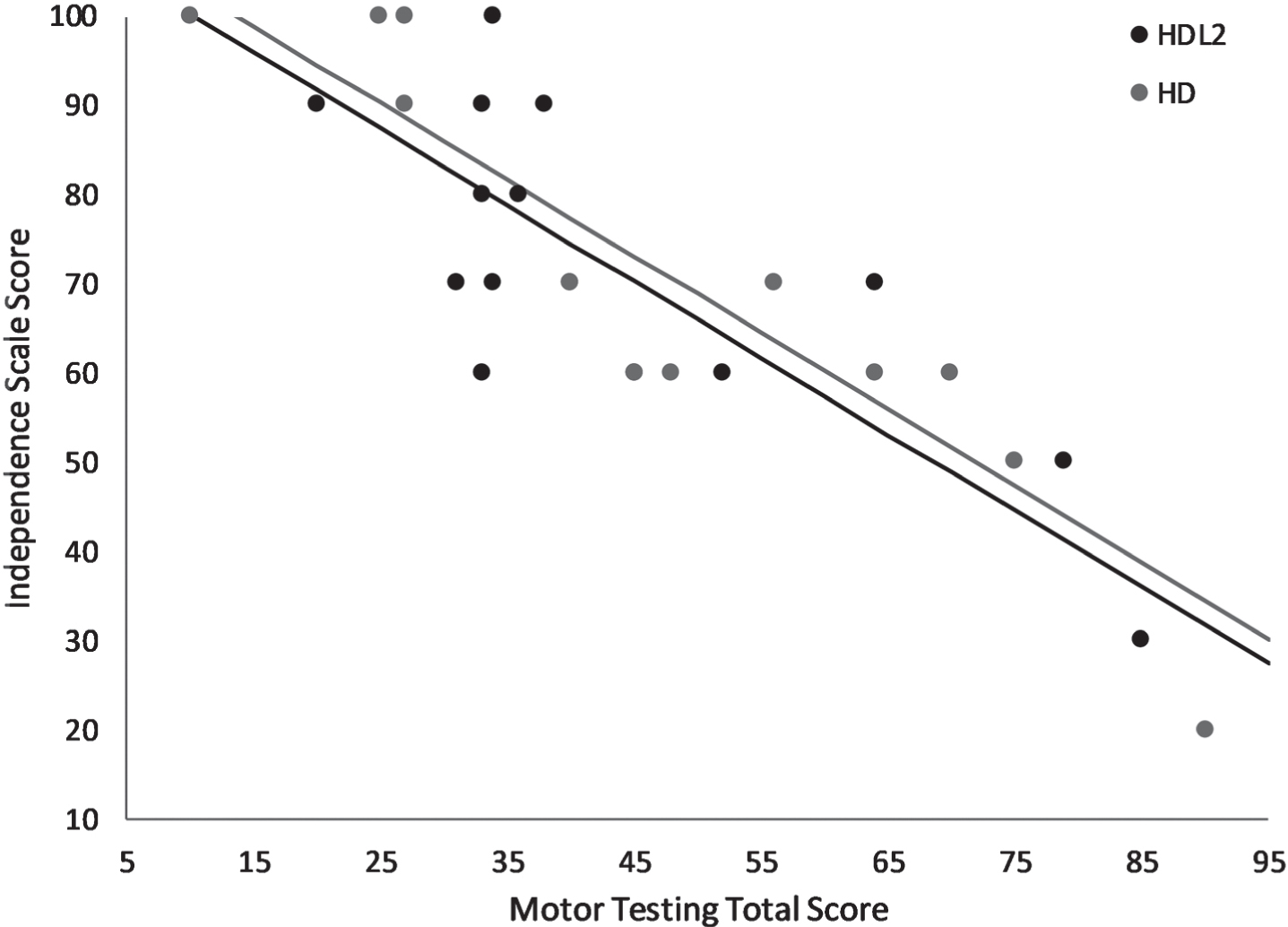
Analysis of covariance between Independence Scale score and Motor Testing total score.
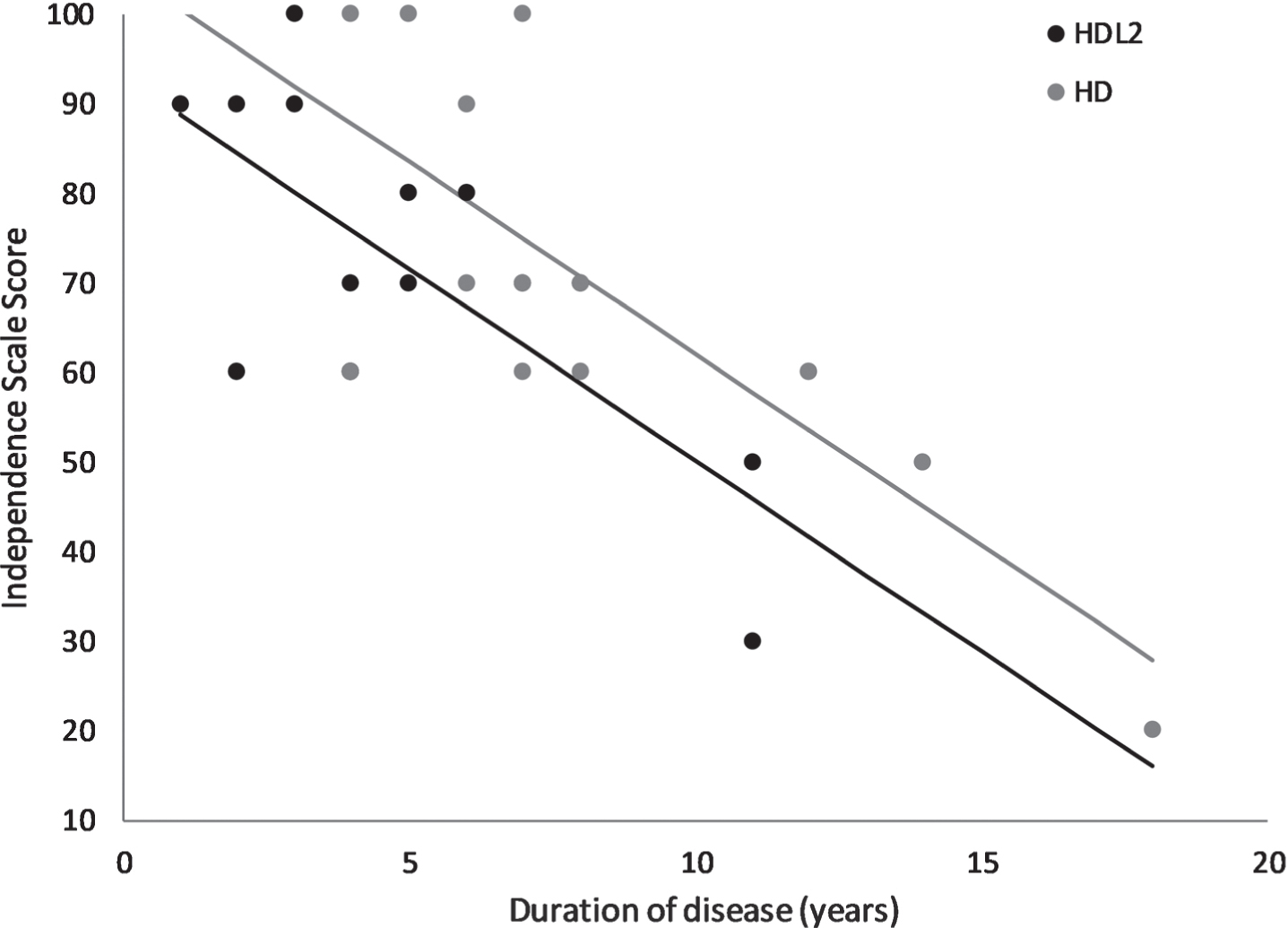
Analysis of covariance between Independence Scale score and duration of disease.
DISCUSSION
The neuropsychiatric presentation of the HDL2 cohort studied is varied in terms of type and severity of symptoms. Nevertheless, our findings suggest that the most common and frequently experienced symptoms (mild to severe) by the HDL2 patients include sadness (82%), anxiety (27%) and irritability (13%). It is challenging to make comparisons with the existing HDL2 literature given not only its scarcity, but also the brief and sometimes non-systematic description of the emotional and behavioural changes of the HDL2 patients. Nevertheless, similar to our findings, depression appears to be prominent [4, 7–11], whereas, and in contrast to our results, anxiety was only noted in two cases [9, 10] and irritability in one [9].
In congruence with our results, no suicidal ideation or planning has been reported in the literature for HDL2. This was unexpected considering that HD is a disease with an increased risk for suicidal ideation compared to the general population [12] and that suicide is considered a public health problem in South Africa [13]. Given the importance of this variable and its therapeutic implications, future studies should explore suicidal risk in HDL2 while considering country-specific moderators [13, 14].
No specific significant differences between the neuropsychiatry of HD and HDL2 as assessed by the behavioural components of the UHDRS were observed, supporting the idea that the phenotypes of these diseases are clinically indistinguishable [1]. For both, disease duration and the UHDRS Motor Testing Total Score have a significant relationship with the Functional Capacity and Independence scores, as might be expected [5]. One of the limitation of this study was that we did not use the Problem Behaviour Assessment for Huntington’s Disease (PBA-HD), which is a reliable tool specifically designed to measure psychiatric symptoms in HD [15]. Future studies should consider the incorporation of the PBA-HD to track the presence and severity of neuropsychiatric symptoms in HDL2.
An important finding is that motor symptoms were identified as the first sign of the disease significantly more for HD than HDL2 (100% vs 40%, respectively). This suggests that, despite the similarities in terms of the psychiatric phenotype in this cohort of patients, the HDL2 group reported non-motor symptoms as the first sign of the disease more frequently. Although this is a retrospective and subjective assessment, it could indicate that psychiatric and cognitive issues possibly precede the motor symptoms in HDL2 as has been previously suggested [4]. This hypothesis should be tested by conducting longitudinal studies that incorporate the assessment of non-motor symptoms from individuals in the premanifest stages of HDL2.
Moreover, our results show that despite the fact that all the patients in the HD group reported an earlier age of onset, HDL2 patients sought molecular diagnosis three years earlier than the HD group. This would suggest that although HDL2 patients report a later onset than the HD patients, they seek help earlier and get a molecular diagnosis earlier [16], suggesting an increased severity and more rapid progression. Previous reports on our cohort [2] indicate that both HDL2 and HD have an almost identical linear correlation between age of onset and repeat length, but despite this, HDL2 patients request medical attention earlier which elicits the diagnostic testing. This presentation of HDL2 cases earlier in the disease course compared to HD patients has been previously reported [16].
When these results are considered together, it can be hypothesised that the psychiatric presentation in HDL2 maybe more disruptive for patients at the initial stages of the disease manifestation, which brings patients and their families to the health practitioner earlier. This would accentuate the importance of understanding the neuropsychiatry of HDL2, especially in the prodromal stages, as well as the importance of psychiatric and psychological care of patients at risk. It is also possible that the progression of HDL2 is faster, and therefore there is a shorter period between perceived onset and time of diagnosis. This hypothesis is supported by the imaging studies that show greater volume loss in HDL2 cases compared to HD cases, specifically in the thalamus [17]; as well as the phenotype studies that revealed a trend for the motor symptoms in HDL2 to be more severe compared to HD [2]. Thus, longitudinal studies in HDL2 that pay careful attention to the psychiatric symptoms, along with the motor and cognitive ones, are necessary, as the rate of progression may be an important difference between otherwise clinically similar diseases. Better characterisation of the early psychiatric manifestations in HDL2 is needed. The presence of psychiatric symptoms in the absence of a movement disorder may delay the diagnosis and therapeutic management of HDL2.
Important limitations of this study involve the lack of controls for medical and psychiatric history. We included participants with neurological and immunological conditions (such as traumatic brain injury, epilepsy and HIV) that are linked to psychiatric symptomatology, which may reduce the potential for generalisation of our findings.
Conclusions
The neuropsychiatric presentation of the patients with HDL2 in this study was varied, although sadness, irritability and anxiety seem to be the most prominent symptoms. The Functional Capacity scores and the Independence scores of the UHDRS were significantly correlated to the Motor Testing Total score and duration of disease. No significant differences in the neuropsychiatric presentation (as assessed by the UHDRS) of HDL2 and HD were found. Significant differences in disease duration and movement as the first symptom between HDL2 and HD may potentially be interpreted as the psychiatric symptoms being more severe for HDL2 in the prodromal stages. Shorter times between the reported onset and molecular diagnosis in HDL2, when compared to HD, may be indicative of a more rapid progression rate for HDL2. Longitudinal studies are necessary to understand HDL2 better in itself and in relation to HD.
CONFLICT OF INTEREST
The authors do not have a conflict of interest to declare.
Data availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Footnotes
ACKNOWLEDGMENTS
Mrs. Marianne Gomes provided genetic counselling to all potential clinical participants. Dr Petra Gaylard provided assistance with the statistical analyses.
This study was financed by the Medical Research Council’s Self-Initiated Research Grant entitled “The clinical and genetic profile of Huntington disease like 2 (HDL2) in South Africa”.