
Abstract
Background:
Risky behaviors are common in Huntington’s disease (HD) and can lead to significant adverse consequences. However, the prevalence and scope of these symptoms have not been studied systematically, and no empirically validated measures are available to screen for them.
Objective:
To test a novel screening tool designed to assess risk-taking behaviors in HD.
Methods:
We administered the Risk Behavior Questionnaire (RBQ-HD) to HD patients and caregivers at Vanderbilt University Medical Center between 2018-2019. Patients completed the questionnaire based on self-report; caregivers provided collateral reports. Clinical and demographic information were obtained from the electronic medical record.
Results:
60 patients and 60 caregivers completed the RBQ-HD. 80% of patients (n = 48) and 91.7% of caregivers (n = 60) reported at least one risky behavior. Adverse social behaviors, impulsive/compulsive behaviors, and reckless driving were the most common behavioral domains reported. Male patients were more likely to report risky behaviors than females (92.3% vs. 70.6%, p = 0.04). The number of risky behaviors reported by patients and caregivers was negatively correlated with patient age (r = –0.32, p = 0.01; r = –0.47, p = 0.0001, respectively). Patient and caregiver reports were highly correlated in matched pairs (n = 30; r = 0.63, p = 0.0002).
Conclusion:
These findings emphasize that risky behaviors are highly prevalent in HD and can be effectively identified through the use of a novel screening measure. We hypothesize that early pathological involvement of frontostriatal and mesolimbic networks may be important factors in the development of these behaviors.
INTRODUCTION
Huntington’s disease (HD) is an autosomal domi-nant, neurodegenerative condition that affects appro-ximately 40,000 people in the United States, with over 200,000 at risk [1]. The characteristic motor signs of HD typically emerge in middle adulthood, although cognitive and psychiatric changes can precede motor onset by decades [2–4] and are often identified as the most burdensome symptoms by patients and caregivers [5]. Behavioral manifestations of HD can be highly variable, including a constellation of executive dysfunction, disinhibition, depression, irritability, anxiety, and obsessive-compulsive symptoms [6–9]. One prominent but under-studied behavioral symptom of HD is a tendency to engage in high-risk, impulsive behaviors. A variety of risky behaviors have been reported in HD, including gambling [10], substance abuse [11], hypersexuality [12], and reckless driving [13], in addition to an increased incidence of criminal activity [14]. These behaviors are dangerous and disruptive and can lead to personal isolation, a loss of stable relationships, and legal consequences. However, the current literature consists mainly of small studies and case reports, and the full scope and prevalence of these symptoms have not been studied systematically.
Despite the susceptibility of HD patients to developing risky behaviors and the significant adverse consequences that these behaviors impart, there are currently no validated measures to screen for them. The Problem Behaviors Assessment-short form (PBA-s) [15] and the Unified Huntington’s Disease Rating Scale (UHDRS) Behavioral Assessment [16] include questions addressing depression, anxiety, apathy, irritability, obsessive/compulsive symptoms, and psychotic features, but neither of these measures assesses risk-taking behaviors or symptoms that may be associated with these behaviors, such as impulsivity, reward-seeking behavior, or risky decision-making. The Disinhibition subscale of the Frontal Systems Behavioral Scale (FrSBe) [17] includes a few questions regarding inhibitory control and impulsivity, but these are limited in scope and do not fully capture the spectrum of behaviors observed in HD. Many of the existing measures used to assess risky behaviors in other populations focus on personality traits or tendencies toward risk-taking but do not assess specific behaviors [18–21], and those that do have limited applicability in HD [22, 23].
In order to address these gaps, we have developed a novel questionnaire to better understand the scope of risky behaviors in HD and have piloted an initial version of this measure in our clinic population. We hypothesize that risk-taking behaviors can be accurately and reliably identified using this novel measure. We have taken a multipronged approach to demonstrate proof of concept and feasibility, with the goal of providing preliminary data to support further development of a validated clinical screening tool. First, we assess reliability and validity of the scale and examine the frequencies of behaviors identified in our clinical population. Secondly, we present correlations with clinical and demographic variables, including age, gender, and CAG repeat length. Finally, we include a qualitative summary of reported behaviors to provide examples of the types of responses that were elicited and to demonstrate the spectrum and severity of this clinical phenomenon.
METHODS
Participants
Participants included 60 patients and 60 caregivers recruited from the Vanderbilt University Medical Center HDSA Center of Excellence between August 2018 –October 2019. Inclusion criteria for patients included having a genetic diagnosis of HD (CAG repeat length ≥36) and the cognitive and physical ability to complete the questionnaire. Inclusion criteria for caregivers included being the caregiver of a patient with HD who is sufficiently knowledgeable about the patient’s condition to complete the study assessments and willing to participate. Exclusion criteria included physical or cognitive impairments that would preclude participants from being able to complete the questionnaire, unwillingness to participate, or lack of sufficient knowledge on the caregiver’s part regarding the patient’s condition. All subjects provided written informed consent prior to participating in the study. The study was approved by the Vanderbilt Institutional Review Board.
Procedures
The Risk Behavior Questionnaire for HD patients (RBQ-HD) was developed based on input from HD clinicians, a review of relevant items from existing questionnaires, and a literature search to identify previously reported behaviors in the HD population as well as other related disorders associated with risk-taking and impulsive behaviors, including frontotemporal dementia, traumatic brain injury, and Parkinson’s disease. The RBQ-HD contains 38 questions that encompass a wide range of risky behaviors, including adverse social behaviors (lying, disrespecting authority figures, mistreating others), impulsive/compulsive behaviors (spending, gambling, eating, internet use), substance abuse, inappropriate sexual behaviors, dangerous driving, illegal activities, arrests, verbal/emotional abuse, and physical abuse. A copy of the scale is included in the Supplementary Material. Patients completed the questionnaire via self-report, and caregivers provided collateral reports on behalf of the patients. Participants were asked whether they (or the patient) had ever engaged in each behavior, and if so when this behavior occurred. Participants were also asked to provide a written description of each endorsed behavior.
The RBQ-HD was administered to patients and caregivers either via Research Electronic Data Capture (REDCap), a secure online survey tool [24], or on paper during a clinic visit, according to participant preference. Completed paper questionnaires were entered into REDCap. Demographic information including age, gender, and CAG repeat length was obtained from the electronic medical record for each patient. CAG-Age Product (CAP) scores were calculated using the standard formula (CAG –33.66)×age [25]. CAP score has been used widely in the HD literature as a marker of disease burden to predict time to motor symptom onset [26]. In general, motor onset typically occurs at a CAP score >400 [27].
The RBQ-HD was scored by calculating the total number of behaviors endorsed for each participant (total behavior score). Proportions of subjects who endorsed at least one behavior were also calculated and compared between groups. Age and CAP score at the onset of each behavior were calculated based on participant report of when the behavior began. Frequency analyses were performed to determine the percentage of patients and caregivers reporting at least one behavior within each domain. Participant comments and descriptions of behaviors were compiled by domain for qualitative analysis.
Data analysis
Statistical analyses were performed in SPSS (26th edition). Crohnbach’s alpha was calculated as a measure of internal consistency. Clinical and demographic information were recorded for all patients and reported as mean (standard deviation). Total behavior scores were compared between groups using Student’s t-test. Chi-square statistic was calculated for categorical variables. Bivariate associations between age, CAG repeat length, and total number of behaviors reported by patients and caregivers were calculated using Pearson correlational analyses. Pearson correlation and intra-class correlation were performed as measures of inter-rater reliability to compare patient self-report and caregiver report for paired data (n = 30). Statistical power analyses indicated that a sample of n = 60 provided adequate power (β= 0.80, α= 0.05) to detect correlations of r = 0.36 or larger. For paired data, n = 30 provided adequate power (β= 0.80, α= 0.05) to detect correlations of r = 0.49 or larger.
RESULTS
Demographics of participant cohort
A total of 60 patients and 60 caregivers completed the RBQ-HD. Thirty of these were paired, resulting in an initial cohort of 90 patients for whom questionnaire data were available from either self-report or caregiver report. Patients were 52% female and had a mean age of 47.5 years (SD 14.7). The mean CAG repeat length for these participants was 45 (SD 5) with a corresponding CAP score of 486 (SD 137) as shown in Table 1.
Demographics of patient cohort (n = 90)
Frequency of risky behaviors
Overall, 48 out of 60 patients (80%) and 55 out of 60 caregivers (91.7%) reported at least one risky behavior. The most frequent types of behaviors reported by both patients and caregivers were impulsive/compulsive behaviors, adverse social behaviors, and reckless driving (Fig. 1). Frequency analyses showing the percentage of patients and caregivers endorsing at least one behavior in each domain are shown in Table 2.

Frequency of behaviors endorsed by domain.
Percent of respondents endorsing each behavior and example quotations by domain
Internal consistency and inter-rater reliability
Cronbach’s alpha for all items in the questionnaire was 0.87 for patient responses and 0.91 for caregiver responses. There were no statistically significant differences between the mean number of risky behaviors reported by patients (M = 5.2, SD = 5.23) and caregivers (M = 5.5, SD = 4.96), t(58) = 0.2280, p = 0.82. Analysis of paired data (n = 30) revealed that caregiver and patient reports were highly correlated (r = 0.63, p = 0.0002) (Fig. 2). Intra-class correlation coefficient for patient-caregiver pairs was 0.77, 95% CI 0.53–0.89.
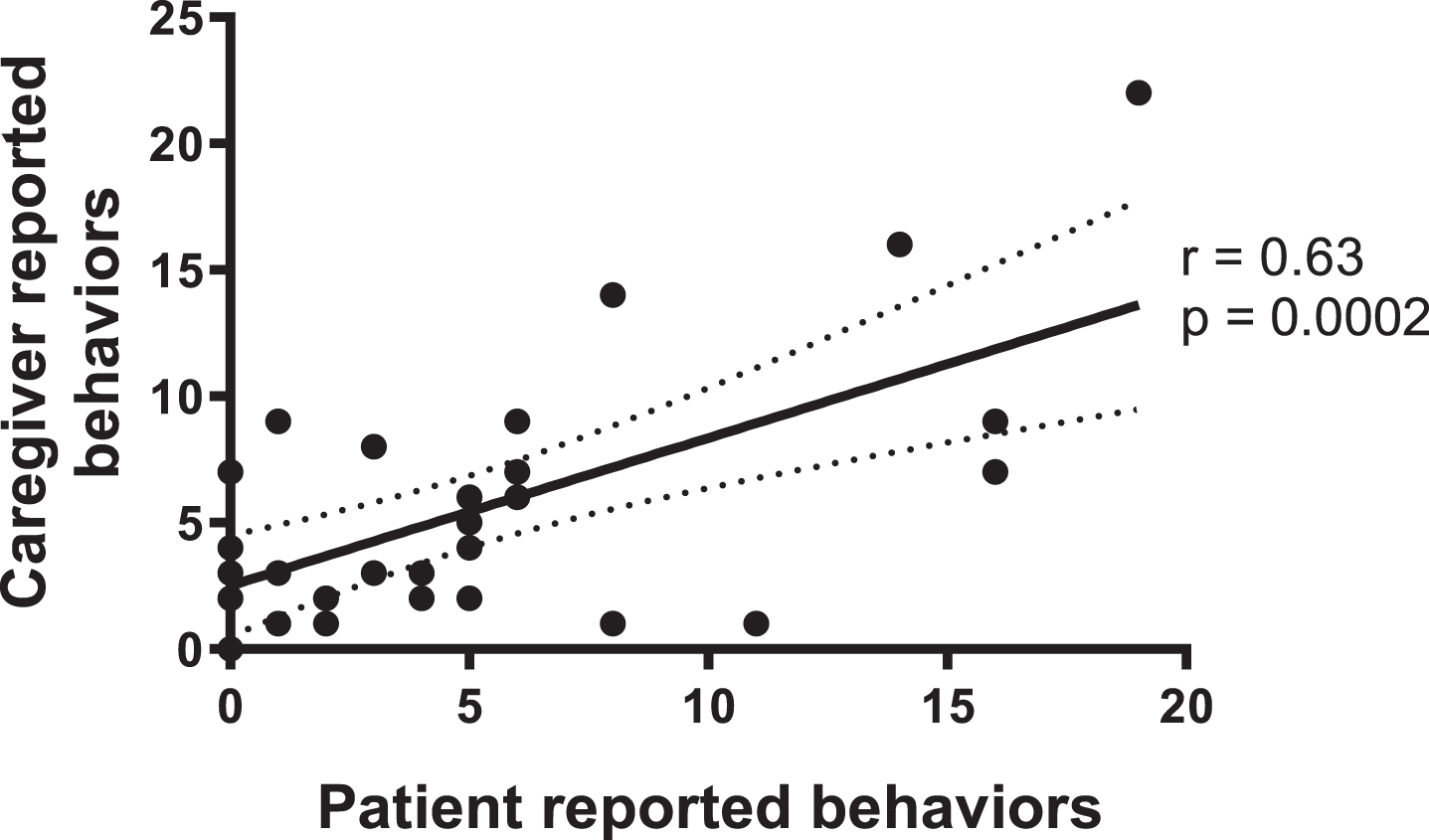
Correlation between patient and caregiver reports (n = 30 patient-caregiver pairs).
Gender differences
Significantly more male patients (92.3%) than female patients (70.6%) endorsed at least one risky behavior, χ2 (1, n = 60) = 4.34, p = 0.04. The proportion of caregivers reporting at least one risky behavior for male patients (94.4%) and female patients (87.5%) was not significantly different, χ2 (1, n = 60) = 0.91, p = 0.34. There were no statistically significant differences between the mean number of risky behaviors reported by male patients (M = 6.54, SD = 5.59) and female patients (M = 4.18, SD = 4.23), t(58) = 1.86, p = 0.07 or by their caregivers [M = 7.14, SD = 6.04 for male patients; M = 5.17, SD = 4.55 for female patients; t(58) = 1.36, p = 0.18)].
Correlations with clinical variables
Total number of risky behaviors reported by both caregivers (r = –0.47, p = 0.0001) (Fig. 3a) and patients (r = –0.32, p = 0.01) was negatively associated with patient age (Fig. 3b). Number of risky behaviors reported by caregivers was significantly associated with patient CAG repeat length (r = 0.44, p = 0.001) (Fig. 4a), although the number of behaviors reported by patients was not (r = 0.14, p = 0.27) (Fig. 4b).
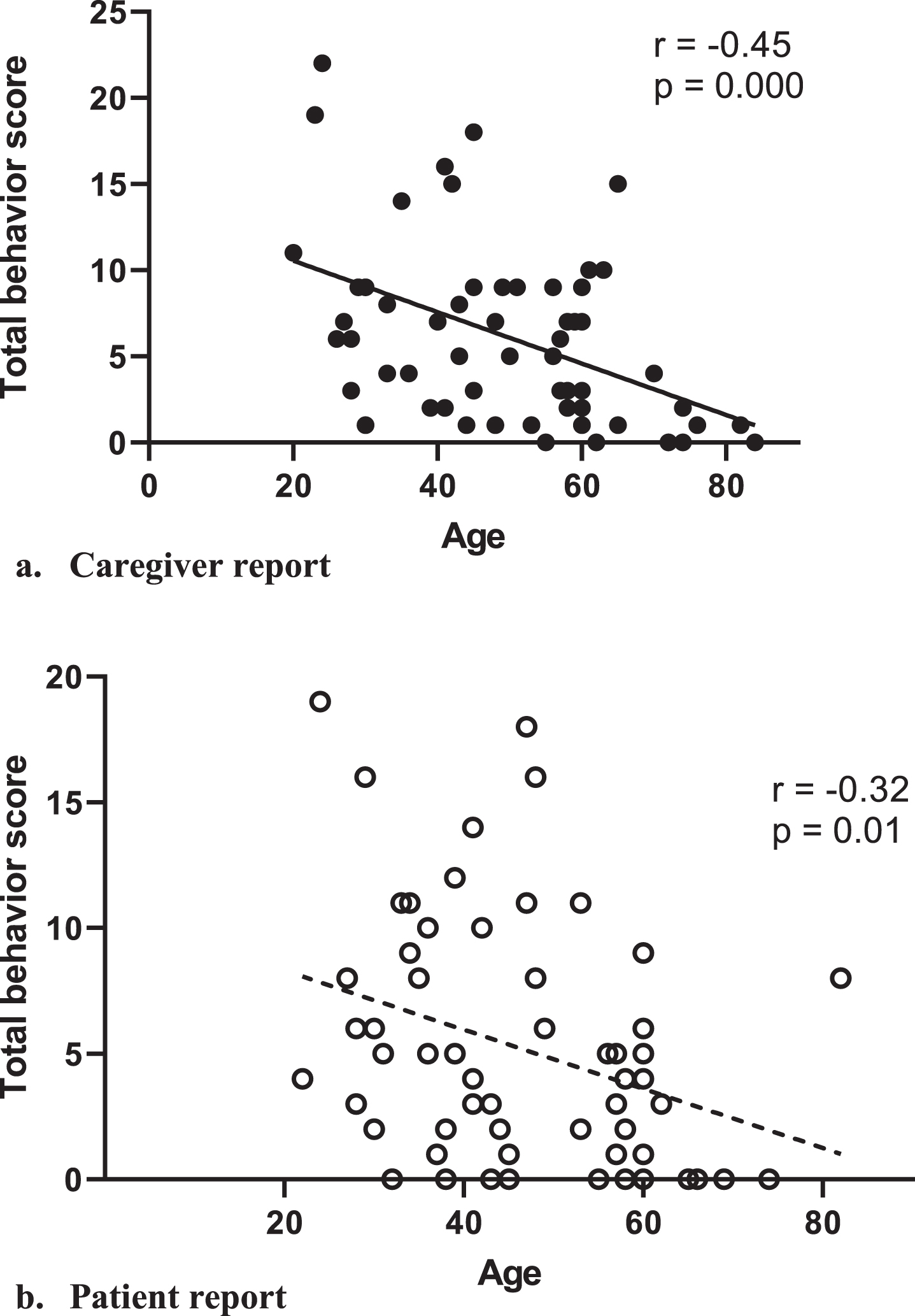
Correlation between total number of behaviors endorsed and patient age.

Correlation between total number of behaviors endorsed and patient CAG repeat length.
The mean age of onset for all risky behaviors reported was 29.2 (SD 16), with a range of 5–59. Of the patients who engaged in risk-taking behavior, 43.6% began participating in these behaviors before the age of 20, and 75.6% before the age of 40. The mean CAP score at onset of risk-taking behavior was 293.76 (SD 163). 75.4% of patients had a CAP score of less than 400 at the time the first behavior was reported.
Qualitative analysis of risky behaviors by domain
Frequency analyses and qualitative descriptions of each type of behavior endorsed are included in Table 2. A description of each behavioral domain and example participant responses is included below.
Domain 1: Impulsive/compulsive behaviors
Impulsive/compulsive behaviors were the most common type of behavior reported by both patients (52%) and caregivers (67%). This domain included questions regarding gambling, impulsive spending habits, compulsive hobbyism, and eating or drinking excessively. 52% of patients described difficulties with these behaviors, including spending too much money and buying things compulsively, as well as excessive interest in hobbies. 67% of caregivers reported observing these behaviors, describing significant financial risk-taking such as buying airplanes or writing checks for down payments on multiple houses, as well as compulsive involvement with hobbies.
Domain 2: Adverse social behaviors
The second most commonly reported category was adverse social behaviors. This domain included question prompts inquiring about behavioral problems and disciplinary action in work and school, acting disrespectfully or dishonestly, and lack of empathy toward others. 50% of patients reported adverse social behaviors, including altercations in school and at work (“fighting all through high school”; “shoved mop at boss and stormed out”) and stealing from family members. 65% of caregivers endorsed these behaviors, including inappropriate behaviors with coworkers and classmates (“placed in state’s custody as teenager; impulsive in school and at work”) and lack of empathy during difficult times (“unable to show empathy for me during my breast cancer”). Nine patients (10%) reported that they had been suspended from school or work, and twelve (13.3%) reported that they had been fired from a job. Similarly, ten caregivers (11.1%) reported that the patient they cared for had been suspended, and eleven (12.2%) reported that they had been fired.
Domain 3: Substance abuse
22% of patients endorsed excessive drug or alcohol use, and 17% of caregivers reported these challenges in those they cared for. One patient described a particularly poignant experience with drug addiction: “Have suffered from different drug addictions over the years. Not drinking. (Some Relatives are alcoholics/ drug addicts too) Used drugs to escape depression/anxiety. Sadness. Life. For fun too. Been in and around a lot of abuse. Verbally, physically, emotionally, psychologically.”
Domain 4: Dangerous driving
Dangerous driving behaviors were also highly reported by both patients and caregivers. 45% of patients reported having driven dangerously or recklessly or having received speeding tickets or other traffic violations. Many also endorsed continuing to drive despite these issues (“Have a revoked license. On 5th or 6th offense currently. No insurance. Recently arrested bc I got pulled over and had no registration or tags on my car”). 53% of caregivers reported dangerous driving behaviors in patients (“Has had over 22 tickets resulting in loss of license”; “had 9 wrecks”; “Going 100 mph and 65 in a school zone”). 26.7% of patients reported having broken traffic laws, and 6.7% reported having received a citation for driving under the influence (DUI). 25.6% of caregivers reported that patients had broken traffic laws, and 3.3% reported DUIs.
Domain 5: Sexual behaviors
28% of patients and 30% of caregivers reported inappropriate sexual behaviors. These ranged from inappropriate exposure, extramarital affairs, and sending explicit messages on social media (“He was private messaging people on Facebook inappropriate things. I deleted his Facebook account and messaging off of phone”), to being arrested on multiple charges of exploitation of a minor.
Domain 6: Illegal behaviors
42% of patients reported that they had engaged in illegal behaviors, while only 15% of caregivers reported being aware of these behaviors. These included burglary (“self-described kleptomaniac”), DUIs and other driving offenses, underage consumption, and aggressive behaviors (“Multiple involvement with law enforcement from teenage years to now. Placed in state custody as a teenager due to aggression in the home. Multiple arrests due to inappropriate behaviors”).
Domain 7: Arrests
23% of patients and 20% of caregivers reported a history of arrests. Reasons for arrests included traffic violations, shoplifting, public intoxication, destruction of property, and exploitation of a minor.
Domain 8: Verbal/emotional abuse
25% of patients reported that they had engaged in verbal and emotional abuse toward others (“I used to yell at my husband and daughter. I threw dishes and things when I was upset. I don’t do it anymore”), and 35% of caregivers reported that they had witnessed these behaviors (“He would start arguments for no reason. His language was abusive. He would get into fights.”; “He will get mad at my daughter who also has HD and will say mean and hurtful things”).
Domain 9: Physical abuse
Finally, 30% of patients reported a history of physical violence toward others, and 28% of caregivers endorsed these behaviors, some with quite jarring descriptions (“Unpredictable out of the blue she slammed me through a glass window”; “he hit our daughter once when she was 14. She never called him dad after that”).
DISCUSSION
We present the results of the first steps in the development of a measure to assess risk-taking behaviors in HD. Our data demonstrate that risky behaviors are highly prevalent in the HD population and can be effectively identified through the use of a dedicated screening tool. Initial analyses indicate that the items are internally consistent, cross-informant responses are correlated, and behavioral scores are associated with clinically relevant biomarkers. Overall, these results demonstrate initial feasibility, acceptability, and proof of concept for this novel clinical tool. The high correlation between patient and caregiver reports on paired data indicates that patients and caregivers can both be reliable and potentially valuable informants.
Our preliminary data demonstrate a wide range of risky behaviors in our clinic population, with the most common types being impulsive/compulsive behaviors, adverse social behaviors, and reckless driving. Illegal activities and arrests were particularly prevalent in this cohort, with 42% of patients reporting involvement in illegal activities and 23% reporting a history of arrests. These findings are in line with previous studies showing similar rates of criminal convictions and arrests in HD patients [14], although the rate of illegal activities as a whole identified in this study is substantially higher than previously reported. A recent retrospective review demonstrated an overall prevalence of criminal behavior in patients with neurodegenerative disorders of 8.5%, ranging from 7.7% in Alzheimer’s disease to 37.4% in behavioral variant frontotemporal dementia [28]. Six out of 30 HD patients (20%) included in this study had a documented history of criminal behavior, half the rate that was identified in our cohort. This discrepancy suggests that these behaviors may not be adequately captured in routine clinical practice or documented in medical records, further emphasizing the need for a validated screening instrument to detect potentially dangerous behaviors before they result in negative consequences.
Our findings also suggest that risk-taking behaviors tend to emerge early in the disease course, often prior to the onset of motor signs and potentially before patients are even aware of their disease status. In our cohort, nearly half of the patients who exhibited risk-taking behaviors reported the initial onset of these behaviors before age 20, and three quarters before age 40. CAP scores at the time of initial behavior onset suggest that the majority of these patients were in the premanifest phase when these behaviors began. These observations align with our clinical experience and suggest that risky behaviors may be an early clinical manifestation of HD. However, it is important to note that this questionnaire was administered as a cross-sectional, historical measure in this initial study, which provided an approximation of the timeline of these behaviors across the disease course but did not allow for the collection of prospective, real time data. Retrospectively, however, patients and caregivers reported risk-taking behaviors beginning in adolescence and young adulthood and subsequently decreasing with disease progression. These observations warrant further investigation in a larger, prospective cohort to clarify the onset and trajectory of these behaviors in HD. Finally, while our findings appear to be in line with previously published literature regarding rates of these behaviors in HD and other neurodegenerative conditions, without a demographically matched control group it is difficult to determine to what degree these behaviors represent a departure from the norm. Adolescence is a well-recognized time of increased propensity toward risky and reward-seeking behaviors in the general population, attributed to developmental changes in the dopaminergic system and prefrontal networks [29]. How HD may impact or amplify these normal developmental trends remains to be elucidated, although recent evidence suggests that brain development itself may be impacted by the pathologic process in HD [30], giving rise to a complex interplay between aberrant neurodevelopment and neurodegeneration across the disease course. The environmental impact of growing up in a family with HD should also be considered, as adverse childhood experiences and exposure to stress have been shown to impair the development of executive function skills and increase risk for psychopathology [31].
There is a strong biological argument for a heightened sensitivity to risk-taking behavior in HD, particularly in the early stages of the disease. Frontal behaviors, including disinhibition and executive dysfunction, emerge during the premanifest period and increase toward the time of motor symptom onset [6]. Prominent disruptions in frontostriatal networks and inhibitory control circuits have been demonstrated during the early prodromal phase of HD [32, 33], and alterations in prefrontal connectivity have been linked to deficits in executive function and response inhibition [34, 35]. Aberrant ventral striatal activation has been demonstrated in response to both reward and punishment in premanifest HD patients [36, 37], suggesting that early pathologic involvement of mesolimbic networks may play a role in the development of risk-taking behavior as well. A predisposition toward high-risk/high-reward choices [38] may increase the likelihood of engaging in these behaviors, while decreased sensitivity to punishment and impairments in learning from a negative outcome [39, 40] may help to explain persistent involvement in these activities despite their negative consequences. Impairments in social functioning [41, 42] and a reduced ability to recognize negative emotions [43] may also make it difficult for patients to understand the impact their behavior has on others. Finally, severe neuropsychiatric comorbidities, including high rates of depression, significant stress, and poor coping skills, are widely prevalent in HD and may lead to maladaptive responses and the emergence of risk-taking behaviors as well [44–46].
This study has several important limitations that should be noted. First, as noted above, this was a cross-sectional study that relied on participant recall of behaviors that occurred across the lifespan. Future prospective studies will allow us to more precisely measure the development and evolution of these behaviors over time. Secondly, as the patient population for this study consisted primarily of symptomatic patients currently receiving care in our HD clinic, there were a limited number of patients under 40 and with a CAP score less than 400. Behaviors in earlier age ranges were therefore reported retrospectively and subject to recall bias, although participants reported a high prevalence of risk-taking behaviors in childhood and adolescence despite these limitations. Further research is warranted to verify these findings in a larger sample size, particularly in younger patients earlier in their disease course. Repeated administration in prospective studies will also allow for the assessment of test-retest reliability and reduce the potential effects of recall bias. The addition of a demographically matched control group in future studies will also allow us to directly compare our results with rates of these behaviors in the general population. Associated cognitive and neuropsychiatric symptoms were also not assessed in this study but will be addressed in future studies. Finally, the initial version of this measure was based upon clinician input and a literature review but did not include direct input from patients. Qualitative data is now being collected from patients and caregivers to guide further development of a revised measure, which will subsequently be submitted to a large, multicenter population for validation.
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.