
Abstract
Background:
Despite the abundance of clinical tools, sleep disorders are still not routinely evaluated in patients with Huntington’s disease (HD). Sleep disturbances can exacerbate cognitive impairment and mood disorders and seriously affect the life of the patients and their families.
Objective:
The current study was designed to investigate sleep quality and its association with clinical symptoms in HD. As an exploratory aim, we also evaluated sleep quality in caregivers of patients with HD.
Methods:
Twenty-nine patients with HD and 22 caregivers completed a series of self-reported questionnaires about sleep quality and pattern, cognitive function, and depression and anxiety symptoms. Spearman correlation analyses were performed to ascertain the association between sleep quality and severity of self-perceived clinical symptoms.
Results:
The primary sleep complaints reported by the patients were related to waking up in the middle of the night or early in the morning; and increased sleep latency. Seventeen of 29 HD patients (59%) and 12 of 22 caregivers (55%) were classified as “poor” sleepers. Worse sleep quality among HD patients was associated with greater severity of anxiety and depression symptoms. Importantly, a decline in sleep quality was associated with decreased self-perceived cognitive function for both HD patients and caregivers.
Conclusion:
Increasing awareness and improving our understanding of sleep dysfunction in HD is imperative for individuals with HD and indirectly, their caregivers. Regularly incorporating sleep assessments when evaluating HD patients should be considered to address this troublesome nonmotor symptom.
INTRODUCTION
Huntington’s disease (HD) is an autosomal dominant, fatal neurodegenerative disease caused by an expansion of CAG nucleotide repeats in the huntingtin gene (HTT) on chromosome 4p [1]. HD is clinically characterized as a triad of symptoms including motor, psychiatric and cognitive symptoms and has historically been classified as a movement disorder requiring the presence of motor symptoms (mainly chorea) for the clinical diagnosis of the disease. The nonmotor features, however, are also exceptionally important and can occur many years before individuals are determined to have motor manifest HD. HD gene carriers may experience nonmotor symptoms that encompass cognitive and behavioral features [2, 3] and neuropsychiatric symptoms, in particular, are problematic components of the clinical spectrum of HD which may be present throughout the disease course, from the prodromal period until late stages of the disease [4].
Disturbed sleep is a common, but underreported nonmotor feature of HD. By using objective measures of sleep quality such as polysomnography and actigraphy, studies have reported sleep disturbances in virtually all HD gene carriers. The sleep disturbances observed in HD include circadian rhythm disturbances [5], increased sleep onset latency, sleep fragmentation and frequent nocturnal awakenings, reduced sleep efficiency, delayed and shortened rapid eye movement (REM) sleep, and increased periodic leg movements [6–9]. Nevertheless, self-report of sleep problems in HD might be reduced because patients with HD do not present excessive daytime sleepiness (EDS) [7, 10] or do not report it, likely due to anosognosia (impaired self-awareness of deficits), a common feature of HD [11]. As a result, sleep dysfunction in HD is likely to be underdiagnosed by clinicians and underreported by patients [10], a phenomenon that impacts directly on patients’ adequate treatment. When asked directly about the quality of their sleep, almost 90% of patients with HD acknowledged having sleep problems [12]. Most of them (∼60%) rated sleep difficulties as either “very important” or “moderately important” components of their overall health problems [12]. Of note, an elegant study showed that the increased nighttime to daytime activity in HD gene carriers was mirrored in the activity profiles of the patients’ neurologically normal carers, indicating a “knock-on” effect of patients’ disturbed sleep [13].
Notwithstanding the high prevalence and the availability of clinical tools, sleep disorders are not routinely evaluated in patients with HD. It is not clear the exact nature of sleep complaints as well as their association with other symptoms of the disease. Therefore, the present study was designed to assess quality and patterns of sleep in patients with HD and to evaluate whether sleep changes are associated with clinical variables, including neuropsychiatric symptoms. We used self-report questionnaires, as patient-reported outcomes can evaluate all aspects of health, being a direct assessment of symptoms (observable and unobservable behaviors) [14]. As an exploratory aim, we also evaluated sleep quality in caregivers of patients with HD. In addition to the symptoms experienced by HD gene carriers, caregivers of HD patients are subject to their own substantial physical, emotional, and financial strain, a phenomenon known as caregiver burden. Identifying sleep dysfunction and addressing its relationship with clinical symptoms among HD gene carriers and their caregivers provides an opportunity to improve the quality of life of both groups.
METHODS
Subjects and clinical scales
After obtaining informed consent, 29 HD gene carriers as well as 22 caregivers were enrolled in this study. Participants were recruited from the Huntington’s Disease Society of America (HDSA) Center of Excellence at The University of Texas Health Science Center at Houston. HD gene carriers were aware of their HD gene and clinical status—either clinically diagnosed (i.e., a diagnostic confidence level (DCL) = 4 in the UHDRS [15]) or premanifest and gene positive determined through genetic testing (genotype larger CAG allele≥36)—prior to the date of questionnaire administration. After obtaining the participants’ written consent, the demographic and clinical data obtained were collected, including CAG repeat length. Participants received the self-completion questionnaires and were instructed to ask for help if they have any questions. HD gene carriers were allowed to receive assistance from their caregivers.
Participants completed a series of self-report questionnaires, spanning a diverse array of items relevant to sleep, anxiety, and disease-specific quality of life variables. The Pittsburgh Sleep Quality Index (PSQI) was included to assess sleep quality and pattern. The PSQI is a 9-question instrument that differentiates “poor” from “good” sleep quality by measuring seven areas (components): subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medications, and daytime dysfunction over the last month [16]. They also completed the University of Cambridge HD Sleep Questionnaire, a detailed questionnaire developed in 2010 to identify sleep disturbances in HD and modelled on sleep questionnaires used for Parkinson’s disease (PD) patients. This questionnaire contained 45 questions that focused on different sleep-related issues such as duration, quality of sleep, abnormal nocturnal behavior and quality of life [17]. Participants were also asked to complete the Epworth Sleep Scale (ESS), a questionnaire designed to measure the subject’s general level of daytime sleepiness. Participants were asked to rate on a 4-point scale (0–3) about their chances of having dozed off or fallen asleep while engaged in eight different activities, such as while sitting down and talking to someone or watching television [18]. The ESS has been extensively used in patients with HD and PD. The STOP questionnaire was used as a screening tool for obstructive sleep apnea (OSA). The STOP is a concise and easy-to-use questionnaire which includes four yes/no subjective questions about
The NeuroQoLv2.0 Cognition Function–Short Form was used to evaluate self-perceived cognition. The Neuro-QoL is an NINDS-funded system of patient reported outcome measures for neurology clinical research, which was designed to provide a precise and standardized way to measure health related quality of life in neurological disorders. It is an 8-question instrument designed and validated to evaluate perceived difficulties in cognitive abilities (e.g., memory, attention, and decision making, or in the application of such abilities to everyday tasks (e.g., planning, organizing, calculating, remembering and learning) [21]. In addition, the Hospital Anxiety and Depression Scale (HADS) was used to determine the levels of anxiety and depression that participants were experiencing. The HADS is a self-administered 14-item scale (seven items relate to anxiety and seven relate to depression) that has been widely used for screening of depression and anxiety symptoms in patients with neurological disorders, including HD [22].
Statistical analyses
Data were presented as mean±standard deviation and median or as median followed by the 25th and 75th percentiles. For HD gene carriers, Spearman correlations were performed in order to determine associations between the PSQI component scores and global score, and the scores obtained in the HD Sleep Questionnaire, HADS-D, HADS-A, Neuro-QoL v2.0, and STOP. Additionally, we performed correlation analyses checking the relationship between PSQI component scores and CAG-age product (CAP) score and number of CAG repeats.
All statistical tests were two-tailed and were performed using a significance level of α= 0.05. Statistical analyses were performed using SPSS software version 26.0 (SPSS Inc., Chicago, IL, USA), as well as GraphPad Prism 5.0 (GraphPad Software, Inc., La Jolla, California, EUA).
RESULTS
Twenty-nine HD gene carriers (52.72±12.22 years; 20F/9M) and 22 caregivers (54.75±13.81 years; 12F/10M) completed the questionnaires. The demographic and clinical characteristics of HD gene carriers and caregivers included in this study are shown in Table 1. Figure 1 shows the individual subcomponents contributing to the global PSQI score for each study participant (HD gene carriers and caregivers). Table 2 presents the correlations between clinical variables and PSQI subscale scores.
Demographic and clinical characteristics of HD gene carriers and caregivers included in this study.
HD, Huntington’s disease; PSQI, Pittsburgh Sleep Quality Index; ESS, Epworth Sleep Scale; HADS-D/A, Hospital Anxiety Depression Scale-Depression/Anxiety.
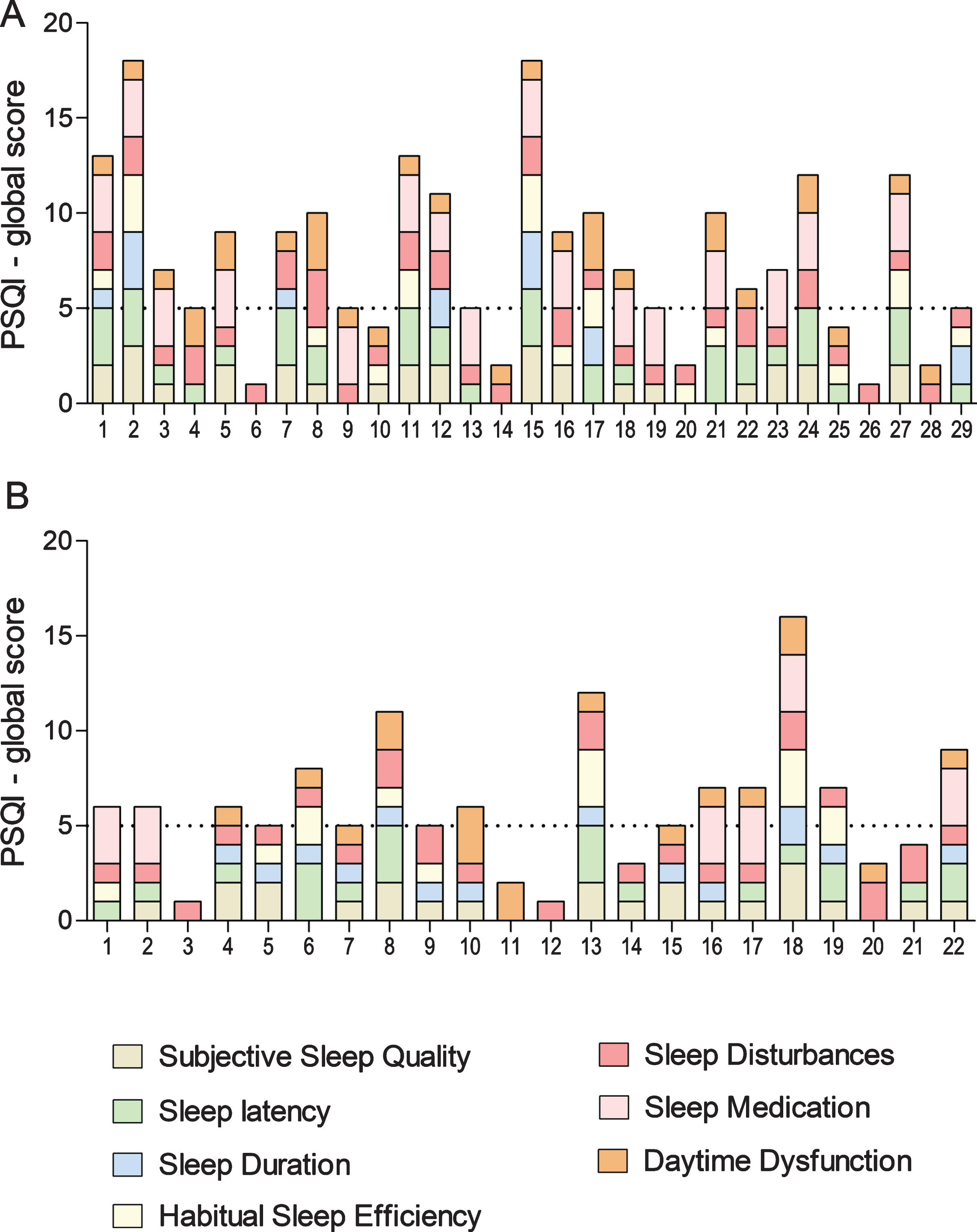
Individual Pittsburgh Sleep Quality Index (PSQI) scores. The subcomponents contributing to the global PSQI score for each (A) HD gene carrier and (B) caregiver are shown. A PSQI global score above five (dashed line) distinguishes between “good” and “poor” sleepers.
Correlations between clinical variables and Pittsburgh Sleep Quality Index (PSQI) subscales
HD gene carriers
Seventeen out of the 29 (59%) HD gene carriers had a PSQI global score >5, where a score >5 distinguishes between “good” and “poor” sleepers with 90–98% sensitivity and 84–86% specificity [16]. Based on component 6 of the PSQI, we observed that 16 out of the 29 (55%) HD gene carriers used sleep medication (prescribed or over the counter) at least once per week in the past month (Fig. 1).
Five of 29 (17%) of HD gene carriers received ESS scores≥11, which is a diagnostic cutoff for excessive daytime sleepiness (11–12 = mild, 13–15 = moderate, 16–24 = excessive) [18]. Of those five patients, one displayed mild EDS, three had moderate EDS, and one had excessive EDS.
We observed significant positive correlations between the total score of the HD Sleep Questionnaire and PSQI global and PSQI components, except daytime dysfunction (PSQI 7) (Table 2). This component includes questions such as “during the past month, how often have you had trouble staying awake while driving, eating meals, or engaging in society?” and “during the past month, how much of a problem has it been for you to keep up enough enthusiasm to get things done?” Though it was not significantly correlated with the HD Sleep Questionnaire, daytime dysfunction was significantly associated with HADS-D and HADS-A scores (i.e., more severe daytime dysfunction was associated with worse scores on the anxiety and depression scales). Interestingly, no significant correlation existed between the daytime dysfunction component of the PSQI (PSQI 7) and a similar measure of daytime dysfunction: the ESS. The only significant finding including the ESS was a positive correlation with the sleep disturbances component of PSQI (PSQI 5). Worse scores at the sleep disturbances component of PSQI (PSQI 5) were also significantly associated with worse anxiety (HADS-A score), and OSA symptoms.
Regarding sleep duration (PSQI 3), habitual sleep efficiency (PSQI 4), and use of sleep medication (PSQI 6), their only significant correlations were with the HD Sleep Questionnaire (positive correlations). In addition to the HD Sleep Questionnaire, subjective sleep quality (PSQI 1) correlated positively with HADS-D and HADS-A (Table 2).
Better scores in the Neuro-QoL v2.0 questionnaire were significantly associated with higher sleep latency (PSQI 2) and the PSQI global score. The negative correlation can be explained by the Neuro-QoL v2.0 scale design. A higher score in the Neuro-QoL v2.0 indicates a better self-perceived cognition, whereas in the PSQI and all other questionnaires higher scores coincided with increased severity or dysfunction. The Neuro-QoL v2.0 and HD Sleep Questionnaire were the only items that were significantly correlated with the PSQI global score.
Additionally, no significant correlation existed between the scores in the clinical scales and CAG-age product (CAP) score or number of CAG repeats.
Alcohol ingestion was frequently reported (68.2%) among HD gene carriers, as well as caffeine consumption (86.4%). There was no significant difference between alcohol users and nonusers regarding PSQI items, the HD Sleep Questionnaire, ESS, STOP, NeuroQoL v2.0, or HADS scores. The analyses comparing smoking status and caffeine consumption were not performed due to the lack of statistical power. Similarly, illicit drug use was excluded, with all respondents denying illicit drug use. In future studies, a broader range of social and demographic variables among HD gene carriers could be compared to sleep quality questionnaires.
Caregivers
Twelve out of the 22 (55%) caregivers had PSQI global score >5, thus being considered poor sleepers. The percentage of poor sleepers in the caregiver population was similar to that of the HD gene carriers in this study: 55% versus 59%, respectively. Based on component 6 of the PSQI, we observed that 6 out of the 22 (27%) caregivers used sleep medication (prescribed or over the counter) at least once per week in the past month (Fig. 1). The percentage of sleep medication users was approximately halved in the caregiver group (27%) compared to the HD gene carriers (55%).
Fewer significant correlations with the PSQI existed for caregivers compared to HD gene carriers. The HD Sleep Questionnaire was significantly correlated with PSQI components 1–4 and the global score. Among caregivers, the ESS showed a significant negative correlation with use of sleep medication (PSQI component 6), a result different from what we observed among HD gene carriers. Similar to HD gene carriers’ results, caregivers showed no significant correlation between daytime dysfunction evaluated in the PSQI (PSQI component 7) and the ESS. However, daytime dysfunction was significantly correlated with the HADS-D and STOP questionnaires (positive correlations). Finally, the NeuroQoL v2.0 and PSQI global scores established a significant negative correlation.
From their ESS scores, caregivers met the diagnostic criteria for excessive daytime sleepiness at a higher percentage than HD gene carriers. Six of 21 (29%) caregivers who completed the ESS received scores≥11. However, none of the caregivers received a score indicative of severe EDS, only one had moderate EDS, and five had mild EDS.
Similar to HD gene carriers, alcohol use was frequent among caregivers (71.4%), as well as caffeine consumption (85.7%). Also, there was no significant difference between alcohol users and nonusers regarding PSQI items, the HD Sleep Questionnaire, ESS, STOP, NeuroQoL v2.0, or HADS scores. Only one out of the 21 carers (4.8%) reported cigarette use and, here again, the analyses comparing smoking status and caffeine consumption were not performed due to the lack of statistical power.
DISCUSSION
By comparing the results of PSQI component scores to the remaining questionnaires, we were able to identify novel associations regarding sleep among HD gene carriers. A decline in subjective sleep quality (PSQI 1) was associated with heightened depression and anxiety scores (HADS). Increased sleep latency (PSQI 2) and a decline in overall sleep quality (PSQI global) were associated with decreased self-perceived cognitive function (NeuroQoL v2.0). A higher degree of sleep disturbance (PSQI 5) was associated with increased anxiety (HADS-A). When evaluating individual questionnaire scores—as opposed to analyzing the relationship between questionnaires—many HD gene carriers in this study displayed a heightened level of sleep dysfunction (PSQI, HD Sleep Questionnaire, ESS), anxiety (HADS-A), depression (HADS-D), and impaired cognitive function (NeuroQoL v2.0), which is in agreement with classically associated sleep and behavioral symptoms in HD. As previously shown, sleep and circadian rhythm abnormalities in HD are associated with depression and cognitive deficits [7]. The significant correlations discovered in this study regarding self-perceived sleep quality, mood, and quality of life serve to bolster this evidence.
Considering a cutoff PSQI global score > 5, the percentage of poor sleepers in our study (55% of caregivers and 59% of HD gene carriers) was higher than the observed in the general population (36%) [23]. Sleep dysfunction existed for both HD gene carriers and their caregivers, but to varying degrees. PSQI component 7 was significantly correlated with HADS-D for HD gene carriers and caregivers. The Neuro-QoL v2.0 was significantly correlated with the PSQI global score for both groups. Finally, the HD Sleep Questionnaire was significantly correlated with PSQI components 1–4 and the global score for both HD gene carriers and caregivers.
Improving sleep quality in HD is a complex task. In addition to impaired motor and cognitive function in HD patients, medications prescribed to treat motor and neurobehavioral symptoms may negatively impact sleep quantity and quality. Patients may turn to sleep medications to seek improvement in their sleep quality, as exemplified by the 55% of HD gene carriers in this study who used some form of sleep medication. Unfortunately, these medications often also have unwanted side effects. As observed in this study, the high frequency of alcohol and caffeine consumption among HD gene carriers can be a target for providers to encourage moderation and promote good sleep hygiene.
Our results must be interpreted taking into account the study design limitations. The severity of HD gene carriers’ anosognosia and cognitive impairment and their impact on self-report questionnaires should not be ignored. Patients with profound cognitive impairment were excluded from the study, which limits the ability to capture the full degree of sleep dysfunction among manifest HD gene carriers. Anosognosia is another important, yet difficult variable to quantify, although correlation has been established between loss of awareness of memory deficit and disease progression [24]. Quantitative assessments such as actigraphy and polysomnography could be used in tandem with self-report sleep questionnaires in order to foster a more comprehensive understanding of sleep quality. The cross-sectional design of the current study is also a limitation, as it prevents any causality analysis. Longitudinal studies are warranted in this regard since they would provide data on causality and symptoms progression. Lastly, we did not assess motor symptoms. Future studies focusing on the relationship between motor issues and sleep quality are needed for a better understanding of the HD clinical picture.
Sleep disturbance in HD is an underreported, incredibly important nonmotor symptom that can occur throughout the course of disease. Disrupted, insufficient sleep can negatively impact mood and cognition, which are affected in HD. Increasing awareness and improving our understanding of sleep dysfunction in HD is imperative for individuals with HD and indirectly, their caregivers. Regularly incorporating sleep assessments when evaluating HD patients should be considered to address this troublesome nonmotor symptom.
Footnotes
ACKNOWLEDGMENTS
We would like to thank the HD community for their active participation in this project. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Erin Furr Stimming receives research funding from Roche/Genetech, Cures within Reach, Vaccinex, Uniqure, CHDI and HDSA.