
Abstract
Background:
Arithmetic word-problem solving depends on the interaction of several cognitive processes that may be affected early in the disease in gene-mutation carriers for Huntington’s disease (HD).
Objective:
Our goal was to examine the pattern of performance of arithmetic tasks in premanifest and manifest HD, and to examine correlations between arithmetic task performance and other neuropsychological tasks.
Methods:
We collected data from a multicenter cohort of 165 HD gene-mutation carriers. The sample consisted of 31 premanifest participants: 16 far-from (>12 years estimated time to diagnosis; preHD-A) and 15 close-to (≤12 years estimated time to diagnosis; preHD-B), 134 symptomatic patients (early-mild HD), and 37 healthy controls (HC). We compared performance between groups and explored the associations between arithmetic word-problem solving and neuropsychological and clinical variables.
Results:
Total arithmetic word-problem solving scores were lower in preHD-B patients than in preHD-A (p < 0.05) patients and HC (p < 0.01). Early-mild HD patients had lower scores than preHD patients (p < 0.001) and HC (p < 0.001). Compared to HC, preHD and early-mild HD participants made more errors as trial complexity increased. Moreover, arithmetic word-problem solving scores were significantly associated with measures of global cognition (p < 0.001), frontal-executive functions (p < 0.001), attention (p < 0.001) visual working memory (p < 0.001), mental rotation (p < 0.001), and confrontation naming (p < 0.05).
Conclusion:
Arithmetic word-problem solving is affected early in the course of HD and is related to deficient processes in frontal-executive and mentalizing-related processes.
INTRODUCTION
Huntington’s disease (HD) is a neurodegenerative disorder caused by an abnormal cytosine-adenine-guanine (CAG) repeat expansion in the huntingtin (HTT) gene [1]. Although clinical diagnosis is based on the presence of unequivocal motor symptoms, progressive cognitive changes and the development of behavioral alterations are also inherent features of HD [2]. Subtle cognitive changes in HD with no apparent impact on activities of daily living can be detected at least a decade before the emergence of motor symptoms [3, 4]. At the time of diagnosis, almost all patients experience some degree of cognitive impairment, and along with the progression of the disease, the deteriorating cognition dramatically impacts functional independence [5, 6].
The clinical presentation of HD and the main cognitive phenotype are strongly mediated by the severe progressive striatal degeneration and frontal-striatal deficits that characterize the disease [7]. However, compelling evidence has shown that brain changes in HD involve the whole brain [8–12]. Thus, although processing speed, attention and executive functions deficits are prominent in HD, cognitive domains and processes such as language, visuospatial/visuoperceptive functions and episodic and autobiographical memory are also affected [13–18].
Regarding cognition and calculation, arithmetic word-problem solving tasks refer to verbal commands presenting problems of varying complexity to be solved mentally through simple mathematic operations (adding, subtracting, multiplying, or dividing). The complexity of the tasks is determined by the semantic and mathematical structure, the context, or the format of how the problems are presented. Such word-problem solving is subserved by several cognitive processes. These include basic number processing (such as number and symbol recognition, or magnitude judgment), simple mathematic computations through calculation or automatic memory retrieval, and complex mathematic computations through sequencing several operations [19, 20]. Accordingly, effective arithmetic word-problem solving depends on the complex interaction of several cognitive processes involving attention and working memory, executive functions, and visuospatial reasoning [21–25]. Additionally, the deployment of other processes is required. These processes include number and symbol recognition, magnitude judgment, simple and sequential calculations, and mental mathematic operations [26]. Many of these processes are topographically and functionally linked to regions extending beyond the frontal cortex and the basal ganglia, regions involving the posterior parietal cortex, the intra-parietal sulcus, the angular gyrus, the supramarginal gyrus, and the perisylvian cortex [27]. Alterations in these regions have been linked to several cognitive dysfunctions, including defective arithmetic reasoning and dyscalculia [28, 29].
Calculation deficits can be found in several neurodegenerative conditions such as Alzheimer’s disease or Parkinson’s disease [21, 30–32]. These deficits can result from primary or secondary forms of acalculia as a function of the trajectory of neurodegeneration, the most affected brain regions, and related processes [33].
Regarding calculation deficits in HD, arithmetic word-problem solving has been found to be affected in this population [34–36]. Specifically, poorer performance in simple subtraction and multiplication tasks has been observed in premanifest gene-mutation carriers and in manifest HD [34, 35], as well as in arithmetic tasks of greater complexity [36]. Previous studies have shown that arithmetic performance correlates with executive functions [36] and the Mini-Mental State Examination (MMSE) [35]. However, only few studies have examined which cognitive domains are involved in performing arithmetic tests. Furthermore, although some studies have suggested that arithmetic word-problem tasks are promising for detecting changes even in premanifest patients, only studies with small samples have been performed to date. Further research is needed in larger cohorts. Consequently, we believe that the pattern of arithmetic word-problem solving performance and related neuropsychological correlates in premanifest and early-to-mild manifest HD is only partially understood.
In the current study we compared performance in an arithmetic word-problem solving task in pre-HD and symptomatic HD compared to healthy controls. Arithmetic tasks have been previously suggested as a promising task to be used in premanifest and early HD. However, the characterization of the pattern of performance in arithmetic tests in this population remains limited. Previous studies showed that HD patients performed solvable problems significantly worse than healthy control subjects, but these results need to be confirmed in larger cohorts [35, 36]. Additionally, few studies have examined correlations of this arithmetic task with other cognitive tasks. Whether arithmetic tasks may be sensitive to the neuropathological progression of HD also remains understudied. Therefore, we studied the associations between arithmetic task performance and an extensive protocol of other neuropsychological tests and clinical variables and evaluate if this could be a promising tool in the HD population.
METHODS
Participants
Between 2018 and 2020, 202 participants were included in a multicenter international HD study coordinated by the Cognitive Phenotype Working Group of the European Huntington’s Disease Network. Study sites were from five European countries (Spain, Italy, Germany, Portugal, and Poland) and all were participants in the Enroll-HD study [37]. Participants recruited for this study were invited to participate after completing their annual Enroll-HD study visit. To all those who agreed to participate, the protocol of this study was subsequently administered.
We did not include participants who had neurological disorders other than HD, or those who had a history of head trauma, drug abuse, non-corrected visual problems, an active major psychiatric event potentially interfering with performance (i.e., delusional syndrome), or severe language difficulties.
Participants scoring below 5 in the Unified Huntington’s Disease Rating Scale Total Motor Score (UHDRS-TMS) [38] and with a diagnostic confidence level (DCL) below 3 were classified as premanifest gene-mutation carriers (preHD) [39]. Participants with a UHDRS-TMS > 4 and a DCL = 4 were classified as symptomatic participants (early-mild HD). To avoid the influence of advanced HD on performance, all HD participants met stage I or II criteria according to the total functional capacity (TFC) scale > 6 [40]. The disease burden score was calculated using the formula: [(CAG –35.5)×age] [41]. The mean estimated time to diagnosis (in years) was calculated for preHD participants according to the model developed by Langbehn [42].
Accordingly, the sample consisted of 165 gene-mutation carriers with a CAG ≥39, and 37 gene-negative healthy controls (HC). The sample of preHD participants was divided into those far-from diagnosis (estimated time-to-diagnosis > 12 years; preHD-A), and those close-to diagnosis (≤12 years estimated time to diagnosis; preHD-B).
All procedures were approved by the local ethics committee at Hospital de la Santa Creu i Sant Pau in Barcelona and reviewed by the institutional review board at each participating institution. The study was conducted in accordance with the 1964 Helsinki Declaration and its later amendments.
Cognitive and behavioral assessment
Global cognitive status was assessed using the MMSE [43] and the Parkinson’s Disease-Cognitive Rating Scale (PD-CRS) [44] as screening measures. These tests were chosen given than the MMSE is part of the Enroll-HD protocol and because the PD-CRS has recently shown to be a reliable method to assess global cognitive status in HD [43, 45]. The specific characteristics of the PD-CRS can be found elsewhere [44, 45] but in short, this instrument is based on nine subtests. These subtests assess immediate verbal memory (maximum score, 12), confrontation naming (maximum score, 20), sustained attention (maximum score, 10), verbal working memory (maximum score, 10), drawing of a clock (maximum score, 10), copy of a clock (maximum score, 10), delayed free recall (maximum score, 12), alternating verbal fluency (maximum score, 20), and action verbal fluency (maximum score, 30), thereby allowing in depth exploration of cognitive functioning [44]. By summing all the raw scores, the total score is obtained (maximum total score, 134). The scale offers also a “fronto-subcortical” (maximum score, 104) and a “posterior-cortical” score (maximum score, 30). To obtain the “posterior-cortical” score we have to add the copy of a clock and the naming subtests raw scores; and to obtain the “fronto-subcortical” score, the other seven subtests raw scores have to be added. To cover other processes of interest, we also included three tasks developed specifically for this study: one that assessed mental rotation, a second that assessed visual working memory and a third that assessed planning. The mental rotation task consisted of a variation of the Vandenberg and Kuse Mental Rotation Test [46]. The task consisted of the serial presentation of nine items of increasing complexity (two and three-dimensional items). Participants were requested to indicate in less than 30 seconds which of the three possible responses were the same figure showed above. The visual working memory task (VWMT) consisted of a variation of the Corsi Block Tapping Task and Institute if Cognitive Neurology (INECO) Frontal Screening [47, 48]. Participants were shown an array of six squares. The researcher then pointed to some of the squares in a specific order and participants were asked to reproduce the sequence of movements the researcher had made. The task had ten problems that participants performed in the same order as the researcher, and ten problems which participants had to demonstrate in reverse order. Similar to the One-touch Stockings of Cambridge task [49], the planning task consisted of cubes of different form and color, stacked in different ways. The participant had to state the minimum number of movements needed in order to reposition the blocks to the base image. The task was presented in a multiple-choice format and the participant chose between one, two, three, four, or five moves for each problem.
Assessment of word-problem solving mental arithmetic
To assess ability to solve arithmetic word problems, we developed a simple multiple-choice arithmetic word-problem solving task (HD-WPA) that consisted of written arithmetic operations. These operations were of increasing difficulty and required addition, subtraction, multiplication, or division.
The complexity was determined by the number of operations—two, three, four, or more—needed to solve the problems.
Participants were required to read the sentence aloud as many times as needed and to choose a response from one of four options within a limit of 60 s (e.g., Helen ’s birthday is 29th June, 11 days later than Anne’s birthday; When is Anne’s birthday? Response options: 17, 18, 29, 11; see HD-WPA task in Supplementary Table 1). The patients were not allowed to take notes but could re-read the task as many times as needed. To ensure understanding of the task, two examples were provided before the task was administered. On continuation, the six consecutive problems were presented one by one. The task was discontinued after two consecutive errors.
Statistical analysis
Sociodemographic data for age, gender edu-cation and clinical variables as CAG, DBS, UHDRS-TMS, and TFC are expressed as means ± standard deviations for continuous variables and as percentages for categorical variables. Comparisons were performed with independent two-tailed t-tests and analyses of variance (ANOVA) for continuous variables, and χ2 test for categorical variables. The significance level was set at p < 0.05.
Using partial correlation coefficients, we analyzed the associations between arithmetic word-problem solving performance, PD-CRS items, mental rotation, visual working memory, and planning. These measures do not have standardized corrected scores and raw scores were used. Therefore, these analyses were conducted controlling for the effect of age, CAG length, UHDRS-TMS, and educational level. CAG was added as covariable to avoid the potential influence of large CAG repeats. However, analysis controlling for age and education can be found as Supplementary Tables 2 and 3. To prevent Type I errors, p-values underwent false discovery rate (FDR) correction for multiple comparisons (p < 0.05). Data analysis was performed using the SPSS v21.0 statistical software package.
RESULTS
Clinical and sociodemographic data
The sample consisted of 165 HD gene-mutation carriers (mean age = 49.3±11; mean years of education = 11.9±4; mean TFC = 11.1±2.0) and 37 healthy controls (mean age = 47.7±11; mean years of education = 11.9±3). As seen in Table 1, from the total HD sample, 31 were classified as preHD (mean age = 40.8±8; mean CAG = 42.9±2.4; mean years of education = 13.3±3; mean TFC = 13) and 134 were classified as early-mild symptomatic patients (mean age = 51.3±11; mean CAG = 43.3±2; mean years of education = 11.5±3; mean TFC = 10.7±2). Among the preHD participants, 16 were classified as far-from estimated time to diagnosis (preHD-A: mean time in years = 18.7±4.8) and 15 as close-to estimated time to diagnosis (preHD-B: mean time in years = 6.4±3.8). PreHD participants were significantly younger than HC [t(66) = –2.72; p < 0.01] but had an equivalent level of education and functional capacity. No differences were found in sociodemographic variables between HC and HD. Compared to preHD, early-mild HD were significantly older [t(163) = –5.6; p < 0.001], had a lower educational level [t(163) = 2.43; p < 0.05], lower TFC [t(163) = 9.3; p < 0.011] and higher UHDRS-TMS [t(163) = –17.6; p < 0.001]. Regarding general cognitive measures, no differences were found between HC and preHD whereas early-mild HD performed significantly lower in all the assessments.
Clinical and sociodemographic characteristics of all sample
1Disease burden score; 2Unified Huntington’s disease rating scale –Total motor score; 3Total functional capacity; 4Mini-Mental State Examination; 5Parkinson’s Disease –Cognitive Rating Scale. aHC vs. preHD; bHC vs. early-mild HD; cPreHD vs. early-mild HD.
Arithmetic word-problem solving performance
As reported in Table 2, no significant differences were found between HC and preHD in the HD-WPA total score [t(66) = –1.4; p = 0.147]. PreHD participants with an estimated “close-to-onset” diagnosis (15 participants) obtained a HD-WPA total score that was significantly lower than that of HC [t(50) = –2.6; p < 0.01] and “far-from-onset” preHD participants (16 participants) [t(29) = 2.2; p < 0.05]. HC solved 100%of the problems that involved two operations, 83.8%of those that involved three operations, and 75.7%of those that involved four operations. PreHD participants solved 87.1%of those problems that involved two operations, 74.2%of problems that involved three operations, and 58.1%of problems that involved four operations. The comparison between frequencies of correct responses as a function of trial complexity showed that accuracy was significantly lower in preHD than in HC in the problems that involved two [χ2 (1, 68) = 5,073, 0.039)] and four operations [χ2 (1, 68) = 3,390, 0.049)]. Looking at the influence of estimated time to diagnosis, we observed that “close-to-onset” preHD participants performed significantly worse than HC in the problems that involved two [χ2 (1, 52) = 8,424, 0.004)] and four operations [χ2 (1, 52) = 4,923, 0.027)]. In accordance with this finding, bivariate correlation analysis showed a significant association between the estimated time to diagnosis and HD-WPA total score performance (r = 0.397; p < 0.05).
Performance on the HD-WPA
aHC vs. preHD; bHC vs. sHD; cHC vs. preHD-A; dHC vs. preHD-B.
In the early-mild HD group, the HD-WPA total score was significantly lower than the score obtained by HC [t(169) = –8.3; p < 0.001]. Participants from early-mild HD group solved 56%of the problems that involved two operations, 36.6%of problems that involved three operations, and 17.9%of problems that involved four operations. As expected, the percentage of correct responses in the early-mild HD group was significantly lower than that in HC and preHD groups for all the trials (Fig. 1).
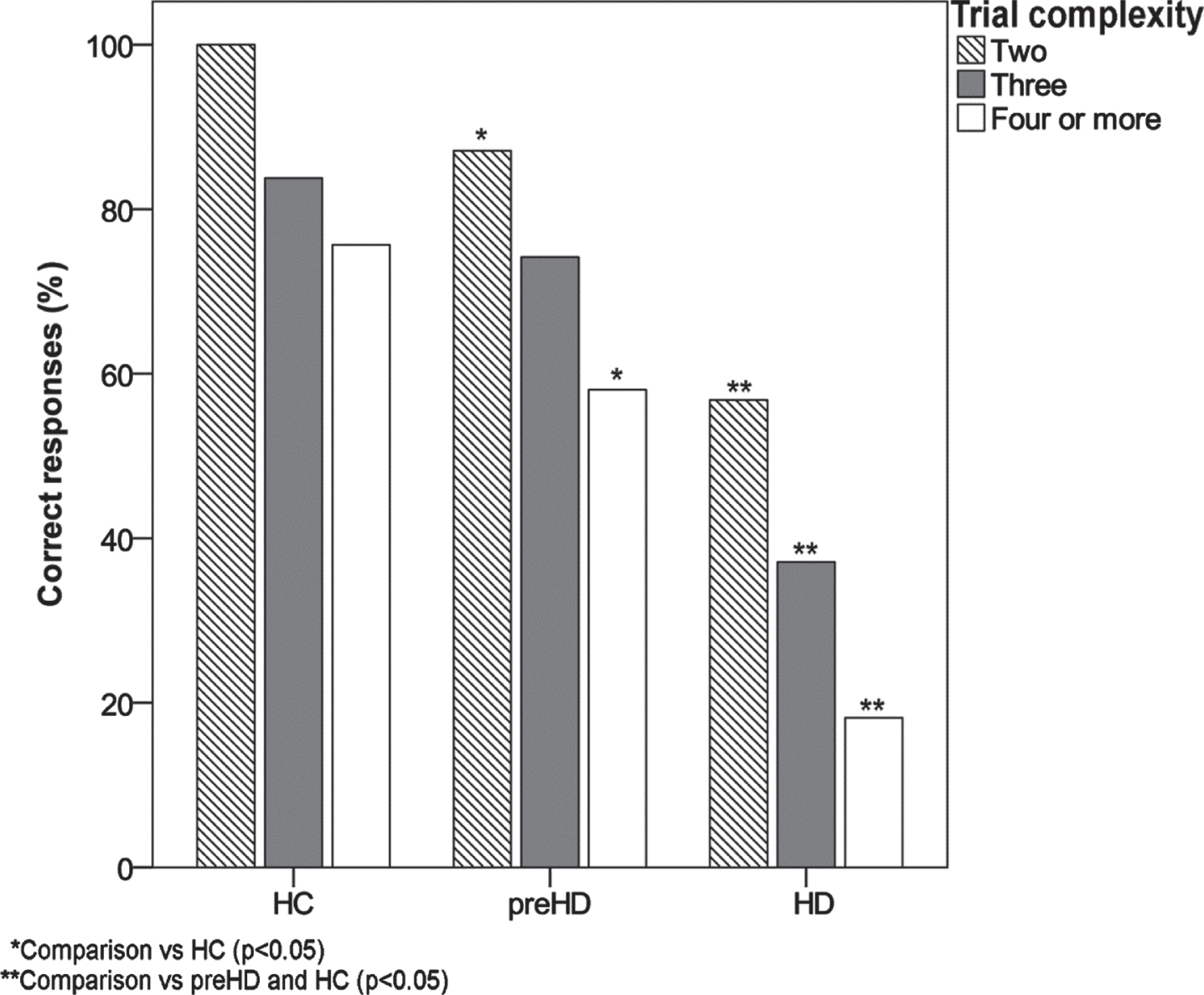
Percentage of correct responses in trials of different complexity.
Correlation analysis
Significant associations were found between the total HD-WPA score and performance in several cognitive measures, including the PD-CRS total score (r = 0.388; p < 0.001), the PD-CRS frontal-subcortical score (r = 0.394; p < 0.001), the PD-CRS posterior-cortical score (r = 0.214; p < 0.005) and MMSE (r = 0.214; p < 0.005). Arithmetic word-problem performance was moderately associated with visual working memory (r = 0.377; p < 0.001), alternating verbal fluency (r = 0.373; p < 0.001), verbal working memory (r = 0.344; p < 0.001) and planning (r = 0.304; p < 0.001). Weaker, albeit significant, correlations were identified for sustained attention (r = 0.291; p < 0.001), action verbal fluency (r = 0.257; p < 0.001), mental rotation (r = 0.280; p < 0.001), delayed recall (r = 0.210; p < 0.001), and clock copy (r = 0.188; p < 0.05). Regarding the operations of different complexity, accuracy in trials with two operations was slightly associated with performance in alternating verbal fluency (r = 0.284; p < 0.001), verbal working memory (r = 0.232; p < 0.001), visual working memory (r = 0.230; p < 0.001), mental rotation (r = 0.196; p < 0.05), and action verbal fluency (r = 0.155; p < 0.05). Trials with three operations were strongly associated with visual working memory (r = 0.403; p < 0.001) and, to a lesser extent, with action verbal fluency (r = 0.278; p < 0.001), alternating verbal fluency (r = 0.268; p < 0.001), verbal working memory (r = 0.266; p < 0.001), planning (r = 0.250; p < 0.005), mental rotation (r = 0.260; p < 0.005), sustained attention (r = 0.225; p < 0.005), delayed recall (r = 0.178; p < 0.05), and confrontation naming (r = 0.176; p < 0.05). Finally, accuracy in trials with four or more operations was significantly associated with visual working memory (r = 0.312; p < 0.001), alternating verbal fluency (r = 0.276; p < 0.001), verbal working memory (r = 0.261; p < 0.005), planning (r = 0.256; p < 0.005), sustained attention (r = 0.224; p < 0.005), delayed recall (r = 0.186; p < 0.05), and mental rotation (r = 0.174; p < 0.05).
DISCUSSION
In the present study we aimed to evaluate performance in arithmetic word-problem solving performance in HD and its relation to a set of neuropsychological measures. We found that global performance was equivalent in preHD and HC participants. However, preHD participants classified as being close-to-onset performed significantly worse than HC, and also worse than far-from-onset participants. Moreover, within the preHD group we found a significant association between estimated time to diagnosis and global performance in mental arithmetic. Global performance was significantly worse in HD participants than in HC, and significantly worse in early-mild HD participants than in preHD. In the symptomatic group, the rate of accuracy was dramatically lower for all the conditions and there was a clear decrease in accuracy as task complexity increased.
Performance in the arithmetic word-problem task was associated with performance in several neuropsychological measures. Specifically, global arithmetic performance and rate of accuracy in more complex operations was associated with measures commonly associated with frontal-executive functions such as working memory, set-shifting, planning, and sustained attention. However, performance was also associated with tasks depending on frontoparietal and cortical-related networks, such as mental rotation, visual working memory, and visuoperceptive/visuoconstrutive abilities.
Working memory, sustained attention, cognitive flexibility and planning have a critical role in arithmetic [21–24]. When a result cannot be simply retrieved from memory because it was not previously learned, these functions allow to decompose, sequence and manipulate information, and maintain a specific rule aiming to solve a problem [50]. The prefrontal cortex and its interaction with the basal ganglia through the frontal-striatal circuits is known to play a central role in working memory, attention, planning and cognitive flexibility. These functions are prototypically affected in HD as a result of the massive degeneration of the whole frontal-striatal architecture [8]. Thus, it is reasonable to assume that executive dysfunction may play a cardinal role in the emergence of arithmetic alterations in HD [51].
In HD, the involvement of posterior-cortical changes has been increasingly recognized as a prominent feature of HD that can be detected years before the onset of its cardinal symptoms [4, 52]. Although these cortical changes have been associated with disrupted performance in several cognitive tasks, their complete functional implications are only partially understood [15, 53–55]. Our data support the critical involvement of defective frontal-striatal-related cognitive processes in the pattern of performance observed in HD. However, the associations that we found between increasing complexity of arithmetic word-problem solving tasks and performance in tasks addressing visuospatial working memory and mental rotation suggest that processes extend beyond those eminently ascribed to the basal ganglia. Although these processes are indissociable from executive functions because of the component of manipulation of information, both processes also involve parietal-dependent components that have previously been found to participate in complex mental arithmetic [56]. This is also the case for the visual imagery component of mental rotation and the storage capacity of visual working memory [57–59]. Accordingly, arithmetic performance in HD may reflect a gradient of subtle-to-prominent disruption of working memory, executive functions, and more posterior-dependent functions such as mental rotation and storage capacity of visuospatial working memory. Future neuroimaging studies may help to elucidate this issue.
Novel therapeutic approaches to delay or even stop the progression of HD are currently under development. Sensitive clinical assessment methods are needed that are sensitive enough to reliably capture subtle differences in premanifest gene-mutations carriers for clinical trials in premanifest HD. Cognitive measures like the Symbol Digit Modalities Test (SDMT) and the Stroop Word Reading Test (SWRT) are known to be sensitive to HD progression from the early stages. The SDMT and the SWRT involves visual processing, attention, and psychomotor speed, similarly to the HD-WPA. The latter, however, requires the deployment of additional and more complex cognitive processes, and thus is suggested to be potentially more sensitive to earliest cognitive changes in HD [60–62].
This work has some limitations. First, the time required to complete each problem in the HD-WPA task was not recorded and could have provided additional information regarding processing speed. Second, language comprehension was not assessed, and thus, although language comprehension deficits are not prominent cognitive features of HD, we cannot infer whether or not they may have influenced task performance through difficulties in the comprehension of more complex sentences. It is of note, however, that language comprehension deficits in HD are usually considered secondary to working memory deficits. Third, the sample of premanifest participants was relatively small, a point that is partly explained by the low participation of this population in research studies. Fourth, the HD-WPA is a short task. Brevity can be an advantage, however, a task with more arithmetic problems may have been useful for better studying the task complexity and the necessary steps to arrive to a solution. Fifth, other analysis such as factor analytic methods and multiple regression may have yielded additional valuable information about the interrelationship of cognitive tasks with the arithmetic tasks, but our sample size precluded these approaches. In the present study, we decided to use correlation analysis to more clearly and directly see the association between HD-WPA and the different cognitive measures. Sixth, we did not take into account the possible influence of neuropsychiatric disturbances and medication in task performance. Finally, the cross-sectional nature of the current study does not allow us to explore the rate of change on arithmetic word-problem solving as a function of progression.
Taken together, our findings suggest that difficulties in arithmetic word-problem solving in individuals with HD can be identified years before motor onset, and that this cognitive function becomes profoundly disrupted in symptomatic patients. Arithmetic word-problem solving in HD is associated with other cognitive processes which are dependent on both frontal-striatal and parietal integrity.
Therefore, arithmetic word-problem solving test seems a promising tool to be used in HD population. However, these results should be considered as preliminary findings and future studies amending the specified limitations of this study should be done.
Footnotes
ACKNOWLEDGMENTS
The authors wish to thank all the study participants and their families for taking part on the study.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.