
Abstract
Background:
Long-term Huntington’s disease (HD) care is offered in specialized inpatient nursing home units with a focus on individually perceived quality of life (QoL). This is shaped in daily care and interaction, which is often abstract and intangible. Furthermore, different perspectives are involved and may vary.
Objective:
To explore and describe perceived QoL of HD patients from three perspectives: manifest HD patients, family members, and nursing staff.
Methods:
36 patients, 11 family members, and 30 nurses participated in this qualitative study by means of individual interviews and systematic qualitative observations on three units.
Results:
Preservation of identity and autonomy is important for patients. Patients struggle with increasing dependence, and try to cope with the impact, uncertainty, and progressive nature of the disease. All participants emphasize the focus on “being human, not just a patient”. Both patients and family members mention the difficulty of dealing with altered behavior and loss of control. Patients are reliant on a relational approach, and an attitude of unconditional acceptance, trust, and understanding support by the nurses. Nursing staff help patients to focus on preserved abilities, and to continue to engage in personalized preferred social activities. Specific qualifications of the nurses were of major influence on QoL for HD patients.
Conclusion:
This study shows, from the patient as well as family member and nursing staff perspectives, that caring for HD patients requires specific knowledge and skills. Particular nursing approaches and attitude and qualifications of the nursing staff in residential HD care improves the perceived QoL of patients.
Keywords
INTRODUCTION
Huntington’s disease (HD) is an autosomal domi-nant neurodegenerative disorder that slowly progresses after onset, which is usually between 30 to 50 years of age [1]. Besides characteristic motor disturbances and neurocognitive deterioration, neuropsychiatric symptoms are common features of HD [2, 3]. In the advanced stages of the disease, patients become increasingly dependent and are often admitted to a nursing home. Onset, severity, and course of the symptoms vary widely, and are partly defined by the CAG repeat length in the mutant allele of the Htt gene on chromosome 4 [1].
Previous studies have shown that HD symptoms influence quality of life (QoL), affecting all life domains [2, 5]. Perceived QoL is defined by psychological and social factors, physical wellbeing, and functioning in daily life [4–7]. As a consequence of the unpredictable onset and course of HD, patients report a lack of control over their emotions, their behavior, the maintenance of social relationships, and family life [5, 9], which affects their perceived QoL. As the disease slowly progresses, both the patient and his/her family need adequate individual coping mechanisms to accept and adapt to the effects of the disease [7, 8].
The perception of QoL by patients may differ from how other people, like family or caregivers, perceive it [5, 10]. HD patients in an advanced stage of the disease may have (partial) loss of insight or be unaware of symptoms that influence the perceived QoL [11, 12]. Also, after admission to a nursing home, other needs and wishes may influence perceived QoL, e.g., interaction with the nursing staff and an increasing dependency on support may become more important [13, 14].
This study was performed in a Dutch specialized nursing home for HD patients. Care is offered by a highly specialized multidisciplinary team. The nursing staff has a central role in the daily care and support of patients. In addition to general nursing approaches and skills, HD specific nursing approaches have been developed in clinical practice, which focus on the individual in the contextual interaction between nurses and HD patients. These nursing approaches strongly emphasize management of behavioral changes and improvement of QoL, via personalized care and shared decision making. As regular nursing education does not cover HD specific care, the applied nursing approaches are based on practical skills and knowledge. The applied approaches are also defined by individual qualities, the physical environment, and the organizational context, such as the clinical treatment and activities.
In this qualitative study, we explored the relationship between nursing approach characteristics and perceived QoL in HD patients in order to understand and describe this from three perspectives: manifest HD patients, family members, and nursing staff. Perceived QoL refers to how people themselves evaluate and perceive their lives, and therefore, discloses their own subjective evaluation of the domains important to them in their own words. This small study aims to contribute to knowledge about the perception of QoL in HD patients from three perspectives simultaneously in the unique social setting of a specialized nursing home.
METHODS
A qualitative design with an exploratory and descriptive method was applied, grounded in interpretive sociology and ethnography [15, 16]. This study focused on understanding the perspectives and interpretations of three directly involved parties: patients with manifest HD symptoms, family members, and nursing staff [16]. In an exploratory literature search, sensitizing concepts were defined as starting point for the empirical data collection [16, 17], which implies that this qualitative, inductive research did not start with hypotheses or a preconceived notion. In the literature search we focused on QoL, wellbeing, behavior, family caregivers, and coping mechanisms in HD, in accordance with the research question. This resulted in 24 articles after removal of duplicates and a reference search. Articles that were related to genetics, medical/pharmacological treatment, or exclusively premanifest HD gene expansion carriers were excluded. During empirical data collection and analysis, these concepts were further explored. In a continuous and reciprocal interplay between theory, empirical data, and analysis, an iterative approach was used for data collection and analysis, until data saturation was reached [16, 17].
Over a period of 7 months, one researcher trained in social scientific research and in nursing (JE) collected data on three specialized inpatient units for advanced stage HD patients. Multiple methods for data collection were used: a) unplanned and unstructured interviews with patients, b) semi-structured interviews with family members and nurses, and c) qualitative observations. Purposive sampling was used as an ongoing method for selection of the interview participants with a focus on in-depth information and diverse characteristics of the participants to ensure maximum variability in the data [16, 17]. Systematic and detailed observations of interaction and behavior took place at different times of the day in various settings of patients and nurses together. The research methods of prolonged observations in the daily routine and natural setting, and interviewing of the three directly involved parties, aimed to understand and interpret what happens in social interaction and what this means from the perspective of the widest representation of the involved people [16]. As this research project aimed to observe and describe daily care and interaction in order to improve our understanding of the perceived quality of life and care, without an intervention, our institution’s guidelines did not require an ethical review of the study. Nevertheless, at the start and during the entire research project, the researcher identified herself and explained her presence repeatedly. Consent was asked, before and during data collection.
A three-step, thematic analysis method was used to find patterns in the data that represent multiple participants’ perspectives, in an ongoing iterative process. To accomplish this, a first and second round of coding the data of each transcribed interview was conducted, and results were used to guide the next interview. Data collection by interviews stopped when saturation was reached, and no new information came up. Member checking was used throughout the interviews to ensure trustworthiness. Therefore, key messages from the participants were noted and verified. Short field notes were taken during the systematic observations, completed by detailed descriptions afterwards. These descriptions were analyzed similarly to the interview data.
A thematic method was used for the analysis of the data: two rounds after each interview, and the third round after collecting all the data. In the first round, every data-transcript was analyzed by systematically organizing the data in categories from an initial set of codes based on the sensitizing concepts and the research question, followed by a second round of coding where inductively new codes, derived from the data, were identified. When all data were collected, a third round of coding was performed to group codes according to themes [16, 17]. Data derived from multiple methods of data collection, triangulation, were complementary and enforced the trustworthiness and credibility of the data. Furthermore, these quality criteria were strengthened by prolonged engagement in the field of study, detailed self-descriptions, and soliciting feedback on the findings by people familiar with the social context [16, 17].
RESULTS
Of the 51 residential HD patients, 36 patients were willing to participate in one or more interviews. Six of the 15 patients did not participate in an interview because of communication problems but agreed to be part of the systematic observations. The mean time since admission was 2.5 years (varying from 2 weeks to 6.5 years). Eleven family members and 30 nursing staff members were interviewed. More family members were asked to participate, but 10 invited family members did not respond, and 6 family members reported that they did not want to participate as the emotional burden of the disease was already too much. Nursing staff members’ educational levels and experience with HD varied (Characteristics of participants: Table 1).
Characteristics of the interviewed participants
We identified four sensitizing concepts relevant for nursing approaches that influence perceived QoL: identity, relationships, coping with the disease, and daily life. A fifth concept was added during data collection: qualifications of the nursing staff (Fig. 1).
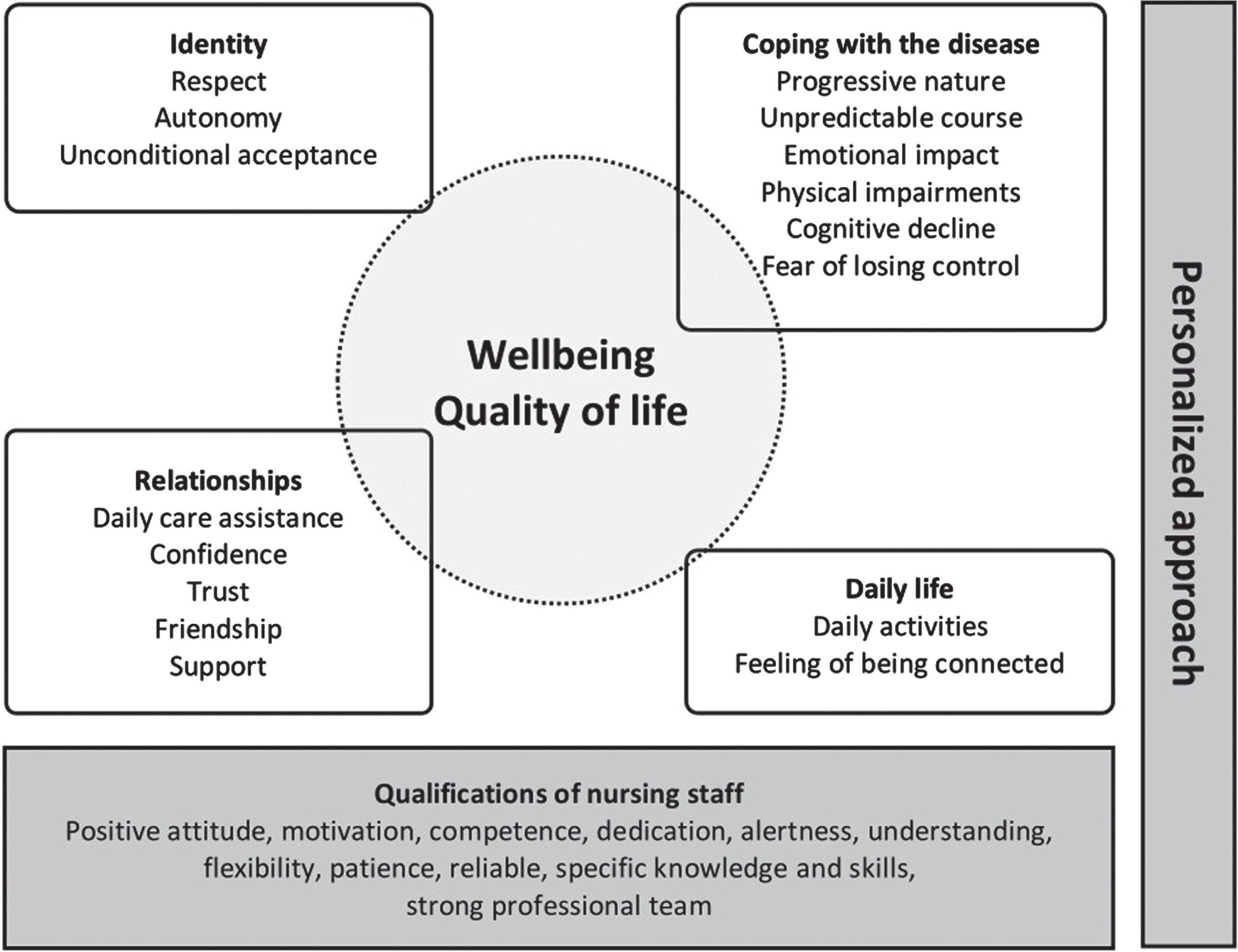
Characteristics of nursing approaches that are related to perceived quality of life.
Identity
All patients emphasized the importance of preserving their identity. They want to maintain their personal values and habits, to be respected for who they are as a person and not just be seen as a patient. Increasing dependence on nursing staff was frequently mentioned in their struggle to preserve their identity, in coping with impairments and the uncertainty of how the disease will progress. Patients acknowledged that as the disease progresses, some aspects that are essential to their identity may change, such as the role they have in their family, their professional functioning, or their religious practices.
Patient: “Almost every night when I go to sleep, I wonder whether I’ll still be able to walk the next day, whether I will be able to talk. This uncertainty, not knowing what is going to happen next and what function you are going to lose. It is impossible to explain what that feels like.”
Every patient mentioned the importance of autonomy, which was confirmed by almost all family members and nurses and observed in daily situations as well. Family members and nurses explained how they try to respect autonomy and promote the independence of the patients. However, sometimes they had to limit autonomy in order to protect the patient, e.g., limiting unrestricted smoking and accompanying them when outside to avoid specific unsafe situations. The nursing staff reported that they regularly discuss the balance between accepting risks and the necessity of safety measures and restrictions.
Nurse: “When we know it is important to her, we may accept a risk. Yes, sometimes this is difficult, but I think quality of life is more important. You have to accept that they could fall or get hurt. We have to accept these risks and talk to them about it.”
All participants emphasized the importance of unconditional acceptance of who they are. Patients, in particular those with earlier experiences of rejection and misunderstanding, need to be able to rely on the nursing staff. Patients mentioned respect and unconditional acceptance by the nurses as important values. Several patients emphasized that they “feel human again” when they are not judged for the changes in their behavior. This was also mentioned by family members:
Family: “They [the nurses] know that it is the disease that causes behavioral problems, not my husband as a person. They do understand that. It shows in the way they treat him, also when he is having difficult moments. They really know what this disease is about.”
Family members stated that neuropsychiatric symptoms are often prominent and may disguise or change a patient’s true identity. Patients mentioned their own changed and often complex behavior, and their difficulties coping with this. They also mentioned feeling misunderstood by others for behavior that they cannot control. Some mentioned a feeling of frustration, while others mentioned embarrassment. These patients emphasized that they could not accept their altered behavior as part of their identity. Both family members and nurses emphasized that changed behavior is often misunderstood by others and can result in social isolation.
Patient: “I know what I do is not fair, at that moment I am unreasonable and stubborn. It is only my perspective, I see it as the truth, even when I am wrong. This is not really me, I cannot help myself, I can’t stop it.”
Relationships
A good relationship between patients and nurses was important to all participants. The overall opinion was that this relationship is essential for patients’ daily care and practical assistance on the one hand, and for having a personal connection based on trust on the other hand. Patients, nurses, and family members all indicated that mutual trust and patient confidence in the nursing staff are crucial preconditions in the relationship between patients and nurses. Patients emphasized that they share a great part of their positive and negative experiences with the nursing staff. Furthermore, nurses help them to structure daily life and to cope with the worsening of the disease and its symptoms. Patients stated that nurses know their “true identity”, help them to cope with “emotional issues”, know their personal wishes, and make them “feel human”. Observations of the interaction between patients and nursing staff showed that the personalized approach and acknowledgement of the patients enhanced the patients’ wellbeing.
Patient: “I have changed, I have lost myself, in all ways. That is Huntington’s, that horrible disease. Suddenly, I can be angry, start cursing and swearing, and I beat them [the nurses]. But I don’t really want to, that’s not who I am. They react calmly or they leave me for a while. But they always come back, and then they are not angry with me. I am ashamed of what I have done, but they don’t blame me.”
Patients stated that their relationship with their family was complicated. According to the nursing staff, several patients had no caring family members, because of broken family ties, other affected family members, or overburdened caregivers.
Nurse: “Many of them have been through so much before they came here. Often there is little to no family left. It is not easy to deal with someone with this disease, especially when their personality or behavior has changed. But family relationships are important to all of them, by family members either being there or being absent.”
Another reported relationship is the relationship between HD patients on the unit. This relationship is experienced as a source of friendship, relevant for mutual support in coping with the disease, and as a possibility to share daily life experiences. However, patients and nurses also mentioned that living together with other patients can be challenging and cause irritation, pity, and inconvenience.
Coping with the disease
Patients, family members, and nurses all reported that the disease has a severe impact on both patients and their families. Patients indicated experiencing the strong emotional impact that living with HD has on their wellbeing. Family members and nurses mentioned that the manifestation of HD is difficult to predict and that the symptoms vary widely. However, awareness of the disease may be impaired in patients, which can result in a discordant impact for patients and their family members.
Family: “It was never easy for him to express emotions, and it is even more difficult now. Although nowadays he is no longer able to hide his emotions. Anger and fear, you see it in his eyes. Moreover, he is nervous and restless, and very demanding. I know that he is frustrated about HD at these moments, about being dependent on others. He is afraid of what will happen in the future.”
With regard to coping with the emotional and behavioral changes, various feelings were mentioned by patients, family members, and nurses. However, the majority of the participants emphasized that patients “try to live life to the fullest, despite the disease”. Patients try to focus on the things that they are still capable of, and family members and nurses try to stimulate and support patients. Several family members and nurses reported that many patients “take it one day at a time”. Nursing staff observed a remarkable resilience among patients in how they cope with the losses caused by HD. Nurses stated being impressed by the perseverance shown by patients in maintaining their independence, their engagement in social activities, and adjustment to the progressing disease.
Patient: “I don’t know how much time I have left, and how the disease will progress. HD is unpredictable, so I want to live now, do everything I possibly can. Next week I may not be able to do these things. So, I try to live life to the fullest, maybe that is the positive side of HD.”
A majority of the patients mentioned an impact of the physical symptoms on their wellbeing. Some of them experienced fear, stress, and frustration as a result of a strong focus on physical symptoms, like motor impairments and swallowing difficulties. Other patients were less focused on or aware of their physical symptoms or they did not bother them. The impact of cognitive impairments on QoL was reported by all nurses and family members, and by most of the patients. Patients expressed a fear of cognitive deterioration, a fear of losing control, and a fear of losing their ability to express themselves.
Daily life
All participants emphasized the importance of daily activities for the perceived QoL of patients. The activities are ideally tailored to individual preferences and preserved abilities, ranging from participation in basic household chores to visiting a concert, football match, or museum. Personal attention, interaction and participation were very important for patients. The majority of participants mentioned feeling connected with other people and society, and a sense of freedom as important for their perceived QoL: freedom to enjoy outdoor activities, freedom to live according to their own values, e.g., to practice their own religion.
Family: “Her religion, her faith, it is important to her. Sometimes, when she is agitated, the nurses read to her from her Bible. That helps to calm her down. I am so happy they recognize this part of QoL for her.”
Qualifications of the nursing staff
Several additional factors that may influence the reported themes were identified and explored in the interviews and observations. The concept of qualifications of the nursing staff was added as influencing QoL. A majority of the participants mentioned a positive attitude, motivation, and competences of the nursing staff. They emphasized the prerequisite of the nurses’ dedication to their work, and in particular to the HD patients. Family members and nurses reported the complexity and comprehensiveness of the disease and its implications for the work of the nurses, also as distinct feature from other patient groups. These participants emphasized the alertness of the nurses in recognizing the needs of patients, and understanding non-verbal behavior, identifying and addressing changes and triggers in behavior.
Nurse: “We care for them over an extended period of time and we develop a close relationship. Knowing their personal preferences helps. Dealing with this disease, especially with the behavioral changes, is complex, like a puzzle. It changes all the time.”
Participants stated that nurses need to show understanding, flexibility, and patience in their interaction with the patients. Family members and nurses both mentioned that nurses need to be reliable, which includes setting limits if necessary. They emphasized that a personalized nursing approach is crucial.
Family: “For him (my son), they provided clarity: On the one hand they allowed him to be himself, make his own choices and refuse most of the help. But on the other hand, they were clear: “Once a week you have to take a shower, whether you like it or not.” This is exactly what he needed. They treated him like a human being, no fighting, no conflicts, but clarity and trust.”
The necessity of a strong professional team was stressed by family members and nurses. Each member of this team must be able to rely on colleagues and create safety, trust, and structure for the patients. Individual and team reflection and alignment were mentioned as contributing to QoL and as major prerequisites for high quality of care. The nurses emphasized that the complexity of HD and the broad variety of symptoms demand continuous attention and a proactive and personalized approach. According to them, dealing with the complexity and progression of the disease require specific knowledge and practical training. They also mentioned close collaboration within the multidisciplinary team as a prerequisite for the management of changing patient behavior.
DISCUSSION
This study shows, from the perspectives of patient, family members, and nursing staff, that caring for HD patients requires specific and distinctive knowledge and skills, mostly developed in practice. Our results show that particular characteristics of nursing approaches in residential HD care can improve the patients’ QoL. Respectful interaction between patients and nurses is crucial for the patients’ preservation of identity and autonomy, sense of trust and safety. Also, support of self-management in daily life, as well as positive and empowering experiences and activities, and meaningful relationships with nurses and other patients are important for the perceived QoL. A professional and open attitude on the part of the nurses, which requires a patient-centered and personalized approach, is often the decisive factor in daily situations, in particular when patients are unable to control their own emotions or behavior.
This study demonstrates that the patients’ perception of wellbeing, often indicated by them as QoL, depends strongly on the nursing staff attitude, especially in relation to behavior that patients are unable to control. Patients need the nurses’ support to manage their behavior, e.g., by offering alternative coping mechanisms, and providing structure and clarity, which enhances patients’ feeling of wellbeing. Patients indicated the importance of an unconditional and consistent attitude on the part of the nurses based on a relationship of trust, even when this is difficult, which makes them “feel human again”. It requires a continuous process of alignment of the nurses to the individual patients, finding a balance between autonomy and restriction, between consistency and flexibility, and with a focus on maintaining mutual respect and trust. The importance of a relational and person-centered approach was emphasized by patients and family members.
HD patients reported that feelings of guilt, shame, and frustration about the changes in their behavior and the impact of the disease, may affect their relationships. Dealing with these feelings requires HD-specific knowledge, and an attitude and approach of the nursing staff, characterized by understanding, flexibility, and patience. It demands a proactive and personalized approach, as patients in an advanced stage of the disease may have only partial insight and awareness of their symptoms, which they only express in confidential conversations. Some nurses expressed discomfort and a lack of experience regarding emotional in-depth conversations with patients, which suggests that patients may not always have the opportunity to express these feelings. In addition to training specific skills and permanent specialized training, we have recommended monthly guided peer supervision sessions or team coaching.
A strength of this qualitative study is the simultaneous in-depth exploration of perspectives of HD patients, family members, and nurses in a unique natural social setting. We consciously decided to use qualitative social scientific methods to uncover the perspectives of the people themselves, in their own words, without the use of scales, measurements or for example one of the QoL assessments. The informal and unstructured nature of the interviews, and the long-term presence of the researcher enabled patients to express themselves in their own pace and both verbal and non-verbal. The systematic observations helped to explore and describe behavior, interaction, and routines of which the participants themselves were unaware. This might explain differences with finding in other studies. The mixed method data collection and the inclusion of participants with a variety of characteristics strengthen the credibility and trustworthiness of the data.
For future studies this type of qualitative research could complement quantitative studies by focusing more in-depth on the perspective of patients and caregivers, and give insight into patterns and behavior participants are unaware of. Qualitative research is recommended for a better understanding of patients’ experience in an advanced stage of HD.
In conclusion, this qualitative study describes the unique relationship between advanced stage HD patients and nursing staff in a residential setting. These patients are often dependent on professional care and live in small social communities with other patients. Attentive personalized nursing approaches based on mutual respect and trust are crucial for their wellbeing.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.