
Abstract
Background:
Huntington’s disease (HD) is a rare, genetic, neurodegenerative disease. Obtaining population-level data on epidemiology and disease management is challenging.
Objective:
To investigate the epidemiology, clinical manifestations, treatment, and healthcare utilization of patients with HD in Israel.
Methods:
Retrospective population-based cohort study, including 20 years of routinely collected data from Maccabi Healthcare Services, an insurer and healthcare provider for one-quarter of the Israeli population.
Results:
The study cohort included 109 adult patients (aged ≥18 years) diagnosed with HD, with mean age of 49.9 years and 56%females. The most common HD-related conditions were anxiety (40%), behavioral problems (34%), sleep disorders (21%), and falls (13%). Annual incidence rates for HD ranged from 0.17 to 1.34 per 100,000 from 2000 to 2018; the 2018 crude prevalence in adults was 4.36 per 100,000. Median survival from diagnosis was approximately 12 years (95%CI: 10.4–15.3). The most frequent symptomatic treatments were antidepressants (69%), antipsychotics (63%), and tetrabenazine (63%), the only drug approved for the treatment of HD chorea in Israel during the examined period. Patterns of healthcare utilization changed as disease duration increased, reflected by increased frequency of emergency department visits and home visits.
Conclusion:
This retrospective population-based study provides insights into the prevalence, incidence, clinical profile, survival, and resource utilization of patients with HD in ethnically diverse Israel. The findings in this study are generally consistent with the international literature and demonstrate the value of routinely collected healthcare data as a complementary resource in HD research.
INTRODUCTION
Huntington’s disease (HD) is a rare, genetic, neurodegenerative disease resulting from an expansion of the cytosine-adenine-guanine (CAG) trinucleotide repeat in the huntingtin (HTT) gene [1]. A CAG repeat length above 40 is fully penetrant [2]. Most patients with HD experience progressive motor decline accompanied by profound behavioral and cognitive changes [3]. The diagnosis is typically confirmed by a family history or a positive HD genetic test, combined with the characteristic clinical manifestations [3, 4]. The age of HD onset is typically 30–50 years, with a range of 2–85 years [3]. The early onset, increasing disability, and absence of disease-modifying therapies means that patients, their caregivers, and the healthcare system suffer significant burden [5–8].
Systematic literature reviews of the prevalence of HD have shown heterogeneity due to differences in study methods and geographical location. Estimates of prevalence in North America, north western Europe, and Australia ranged from 5.96–13.7 cases per 100,000 between 1993 and 2015, which is higher than Asian countries (0.41–0.70 cases per 100,000) [9–12].
Because HD is a rare disease, one of the greatest challenges is obtaining population-level long-term follow-up data. Enroll-HD, a longitudinal database established in 2013, is currently the largest multinational registry [13, 14]. While observational studies such as Enroll-HD are a valuable source of clinical data, data on disease management, particularly on medications and use of healthcare resources, continue to be limited. Moreover, the Israeli HD community, among others, is not represented in these studies, and long-term data in Israeli patients with HD are lacking.
Previous Israeli HD studies focused mainly on specific subgroups of patients and were conducted in the clinic setting [15, 16]. Although these studies provided valuable findings on the ethnicity-specific distribution of HD among Israelis, they did not investigate the population-based aspects of epidemiology, clinical manifestations, and healthcare resource utilization.
Here, we describe a retrospective population-based cohort study including 20 years of routinely collected healthcare data on patients with HD in the Maccabi Healthcare Services (MHS), to provide representative insights on the real-world disease epidemiology, treatment patterns, and long-term outcomes of HD in Israel.
METHODS
Data source
We used the real-world database of MHS, which is an insurer and healthcare service provider for a quarter of Israel’s population [17]. The population captured by MHS is demographically similar to other Israeli Health Maintenance Organizations (HMOs), with annual attrition rates < 2%[17]. MHS collects diagnoses from hospitals, general practice, specialty clinics, ambulatory clinics, and hospice settings. MHS additionally captures data on medical procedures, imaging, and drug treatments through drug purchases and pharmacy dispensations. All data are linked at the patient level using a unique national patient identifier.
The study was approved by the MHS Institutional Review Board. All patients’ records were de-identified.
Study population
Data were extracted for adult MHS patients (≥18 years) during 2000–2019, with an HD diagnosis defined by at least one record of International Classification of Diseases, Ninth Revision (ICD-9) code (333.4). All diagnoses included in the study were made by a neurologist in the community or hospital clinics, or were documented as a chronic disease diagnosis in the patients’ medical record. HD diagnoses extraction was limited to these settings in order to achieve a higher specificity of case identification in real-world clinical data.
The index date was defined as the earliest HD diagnosis date within the study period. To ensure medical histories completeness and to verify incident cases, patients with < 1 year of continuous MHS membership prior to the index diagnosis or < 1 year of continuous membership after the index diagnosis were excluded from the study. Patients diagnosed with drug-induced chorea, subacute dyskinesia due to drugs, Sydenham’s chorea, or rheumatic chorea documented after the index HD diagnosis were also excluded.
Variable definitions and statistical analyses
Data extraction was performed using the MHS MDClone platform. HD-associated conditions at baseline were identified prior to or within one year after the index date. Behavioral problems were defined by means of all-cause psychiatric visits. First HD treatment was defined as the first drug dispensing (within pre-specified drug classes) after the index date. Because HD treatments are symptomatic, each patient may have received more than one treatment according to the specific symptoms experienced in the course of their disease.
Healthcare resource utilization was described using hospitalizations (including emergency department [ED] visits and intensive care unit [ICU] admissions), home visits, and ambulatory visits, or consultations with any healthcare professionals after the index diagnosis. Healthcare resource utilization was evaluated in intervals of 1, 2–5, and 6–10 years, inclusive, after the index diagnoses.
Annual incidence was defined as the number of new adult HD cases per year in the MHS population divided by the adult MHS population for the corresponding year. Prevalence was defined as the total number of adult HD cases in 2018 divided by the adult population in the MHS database in 2018. Descriptive statistics were presented as mean and standard deviation (SD) or median and interquartile range (IQR), depending on the variable distribution. Counts and proportions were provided for categorical variables. Time from HD diagnosis to death, HD treatment, ED visits and ICU admissions were analyzed using the Kaplan-Meier method.
RESULTS
Study population
After implementing the inclusion and exclusion criteria, the final study cohort included 109 patients (Fig. 1). Nine patients were excluded due to having < 1 year of continuous membership prior to the index date. The annual new HD case counts ranged from 2 to 13 between 2000 and 2018, providing annual incidence rates fluctuating from 0.17 to 1.34 per 100,000. Because HD is a rare disease, the annual case counts and rates were statistically unstable, with no clear evidence of a trend over time. A total of 69 adult patients had HD in the population of 1,580,816 MHS members in 2018, providing a prevalence of HD of 4.36 cases per 100,000 (95%CI: 3.40–5.52).
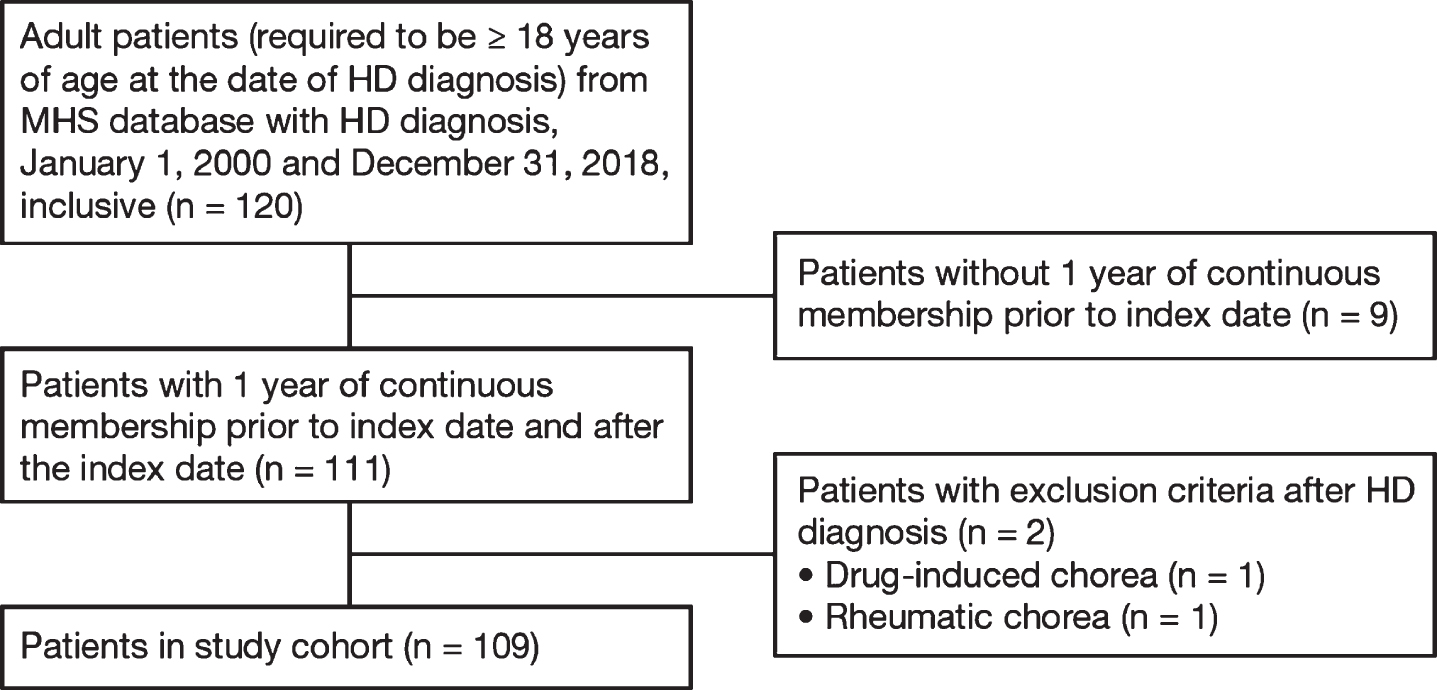
Cohort diagram. The study cohort of adult individuals with a diagnosis of HD between January 1, 2000 and December 31, 2018 was selected from the MHS database. Patients with < 1 year of continuous membership prior to HD index diagnosis, or with pre-specified diagnoses after the HD index diagnosis were excluded.
The mean age at index diagnosis was 49.9 years (SD = 12.9) and slightly over a half of the patients were female (56%). Most patients were of middle (45%) or high (31%) socioeconomic status, with a fifth of patients (21%) having low socioeconomic status. Genetic testing for HD was documented in 44%of patients. The median post-index diagnosis follow-up period was 8.5 years (IQR = 6.7) (Table 1). The most frequent HD-related conditions at baseline were anxiety (40%), behavioral problems (including irritability, personality changes and apathy, which were captured through visits to psychiatrists; 34%), sleep disorders (21%), and falls (13%) (Table 1). Forty-three deaths were documented in the study, with a mean age of death of 58.9 years (SD = 13.3) (Table 1). Information on cause of death was not available. Median survival time from index diagnosis was ∼12 years (95%CI: 10.4–15.3). The study cohort survival curve is shown in Fig. 2.
Demographic and baseline characteristics
HD, Huntington’s disease; IQR, interquartile range; SD, standard deviation.
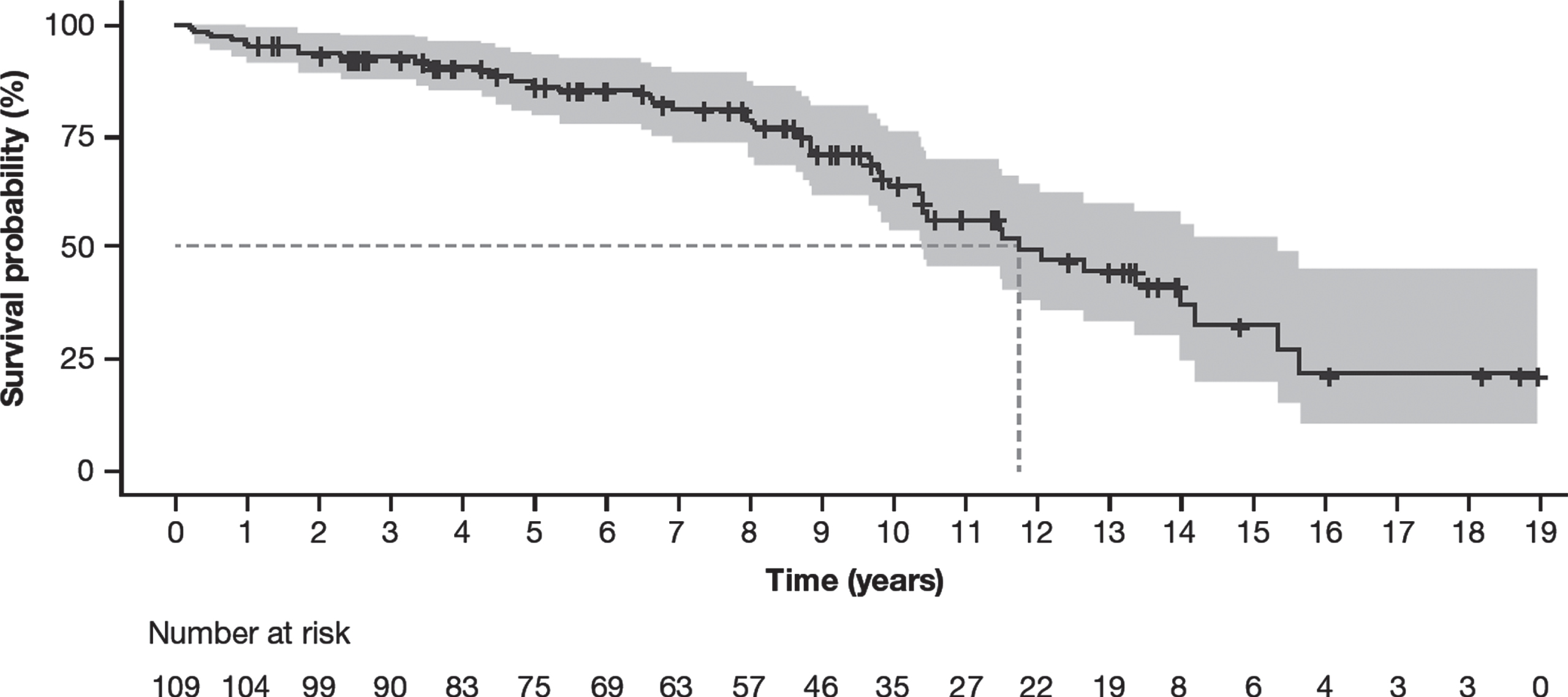
Survival curve of the study cohort. Time from HD index diagnosis to death was analyzed by the Kaplan-Meier method. Median survival time is shown by the dotted line.
Drug treatments
The most frequently used symptomatic treatments were antidepressants (69%), antipsychotics (63%), and tetrabenazine (63%), the only drug indicated for HD chorea treatment in Israel during the investigated period. About half of the patients were treated with antiepileptics (51%), hypnotics and sedatives (54%), and anxiolytics (47%) (Supplementary Figure 1).
The dynamics of drug prescription starting from the index diagnosis are shown in Fig. 3. The drug classes most frequently prescribed soon after the diagnosis were antidepressants, antipsychotics, and drugs in the “other nervous system drugs” Anatomical Therapeutic Chemical (ATC) class. These drug classes were used by over a half of patients within 4 years of follow-up. Within ∼8 years, half of the patients had been treated with hypnotics, anxiolytics, and antiepileptic drugs. The median time for opioid use was 12 years after diagnosis.
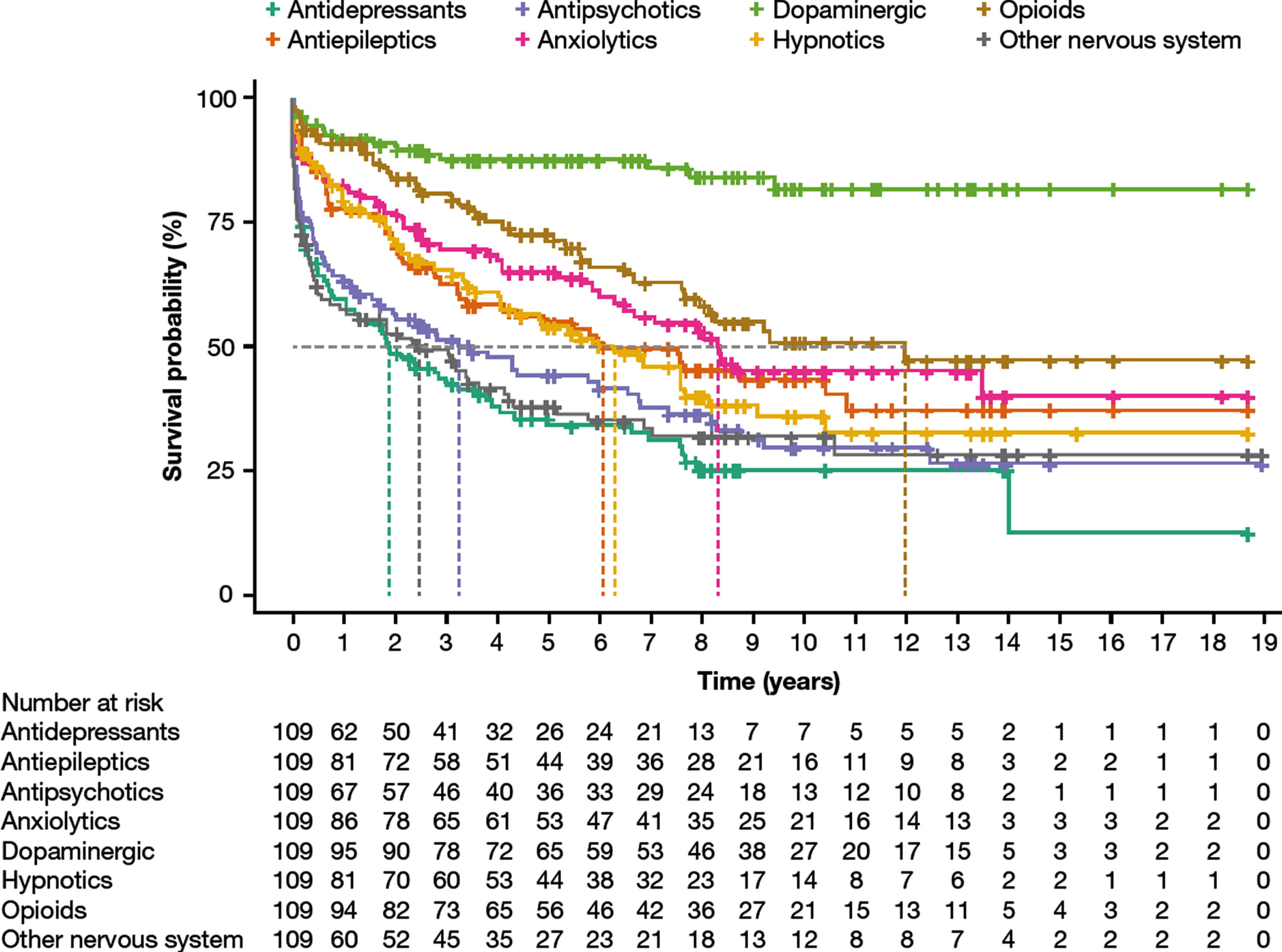
Time from HD diagnosis to drug treatment. Time from HD index diagnosis to the start of drug treatment was analyzed by the Kaplan-Meier method. Median time to first drug use is shown by the dotted lines.
Notably, 27%of tetrabenazine treatment was given prior to the index HD diagnosis. A density plot of tetrabenazine treatment initiation with respect to index HD diagnosis is provided in Supplementary Figure 2. The median time of tetrabenazine initiation (dotted vertical line on the plot) is slightly earlier than the index date (zero point on the horizontal axe) and ranges from ∼10 years before and 8 years after the index date.
Healthcare resource utilization
Seventy-one patients (65%) were admitted to a hospital during the follow-up period. Median time from index diagnosis to hospital admission was 3.0 years (range 1 day–12.2 years; IQR 1.7–5.8 years) and median length of hospital stay was 3 days (range 0–148 days; IQR 1–6 days). Special outcomes of interest were ED visits and ICU admissions (Supplementary Figure 3). Sixty-nine patients (63%) visited the ED at a median time of 3.5 years from diagnosis, and there were eight ICU admissions (7%); as less than half of the study group had ICU events, no median time was reached for this outcome.
The percent of patients with all-cause ambulatory visits, all-cause ED visits, and home-based medical visits during the first year, 2–5 and 6–10 years after the index diagnosis is presented in Fig. 4. The results indicate that patients with HD utilized ambulatory care with high frequency throughout the study follow-up. The frequency of ED visits and home visits gradually increased with time from index diagnosis.
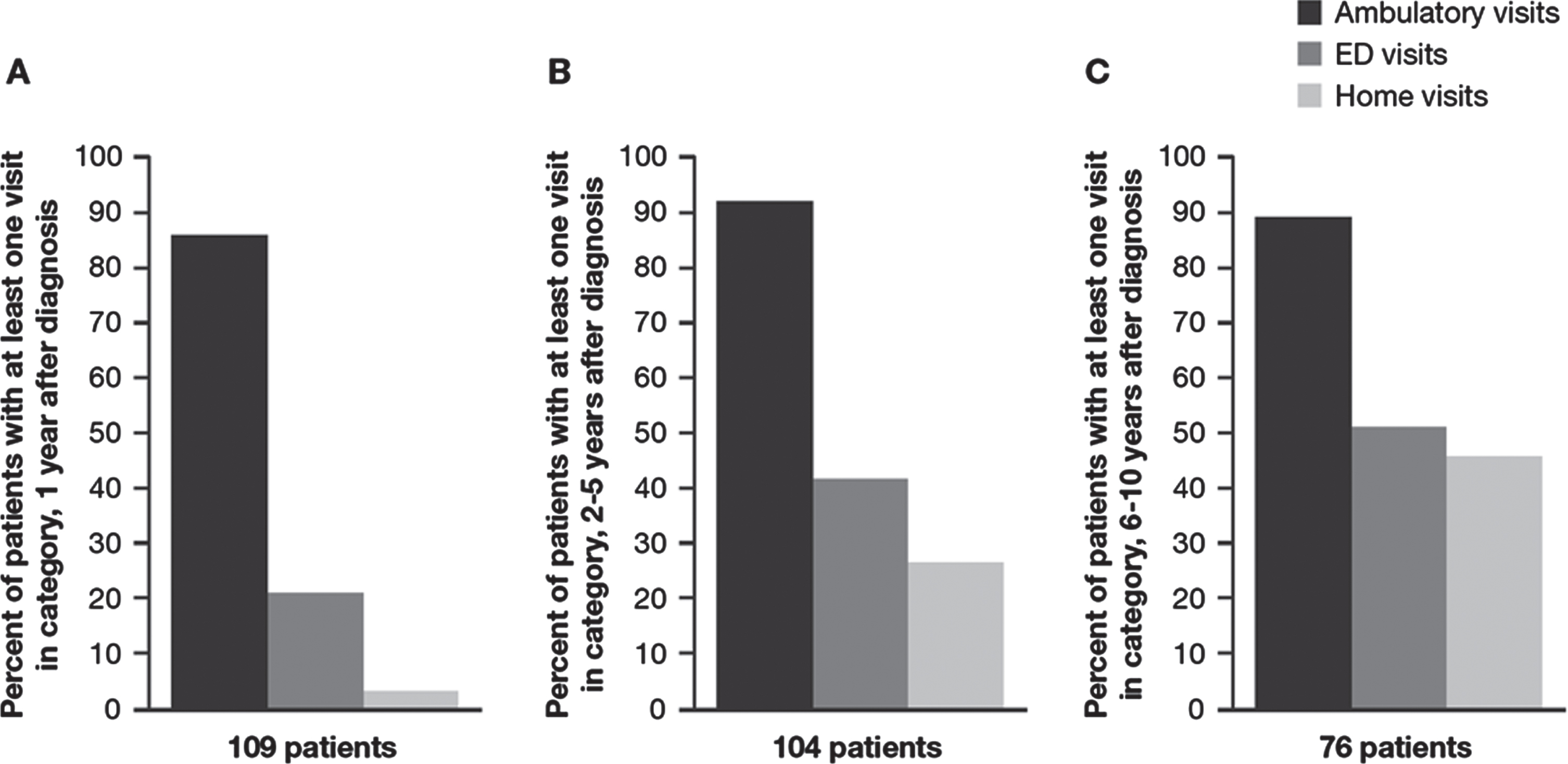
Patterns in HD healthcare resource utilization over time. Percentage of patients with at least one ambulatory visit, ED visit or home visit after (A) 1 year; (B) 2–5 years; (C) 6–10 years following HD index diagnosis.
DISCUSSION
To the best of our knowledge, this is the first study describing the epidemiology, clinical manifestations, and healthcare resource utilization of patients with HD in Israel, using population-based data from a large national health plan. In addition to the importance of this investigation for Israeli public health policy, our study puts forward several potential advantages of MHS real-world data in the investigation of neurodegenerative diseases such as HD. Specifically, our study was able to capture 20 years of routinely collected patient-level data with a median follow-up of > 8 years from diagnosis and a median of 12 years prior to diagnosis. The treatment patterns in MHS are captured through pharmacy drug purchases and dispensations, which show a strong correlation with actual drug consumption and may represent a stronger proxy than drug prescriptions [18–21]. Thus, the comprehensive and longitudinal nature of routine care data provided an overview on medication and healthcare resources use throughout the HD course. Since MHS population does not significantly differ demographically from other Israeli health plans [17], our results are considered generalizable to the Israeli population.
The crude adult prevalence of HD in our study was 4.36 per 100,000 MHS members. This is at the lower end of HD prevalence in Europe (2.1–13.5 per 100,000) [22–24] and substantially lower than reported in North America (13.7 and 17.2 per 100,000 in the general and Caucasian population, respectively) [10, 22], but similar to that in Cyprus (4.64 per 100,000), which is geographically close to Israel [25]. The annual HD incidence in our study ranged from 0.17 to 1.13 cases per 100,000 during 2000–2018, which is lower than the average annual incidence of 1.59 per 100,000 in the US during 2004–2016 [10, 26]. Other analyses, based on medical records in Italy, UK, and Germany, report incidences of 0.3, 0.7, and 1.8 per 100,000, respectively [24, 27]. Overall, our findings show that Israel, with its ethnically diverse population, has an HD prevalence within the range of published global estimates. Caution is advised when comparing prevalence estimates, as studies may use different age criteria. This study describes the prevalence of HD in an adult population (≥18 years); however, it would be expected that the prevalence of HD in the overall population would be lower, owing to the relative rarity of pediatric HD [12]. The lower prevalence may also be accounted for by differences in the HD case definition used. This study used a conservative means of ascertaining HD cases according to a specialist neurologist or chronic diagnosis of HD, with index date defined as the earliest HD diagnosis documented in these sources. Other studies may define HD cases as any record of HD across available medical records, and index date as age of motor symptom onset.
Survival time, at a median of 12 years (95%CI: 10.4–15.3) from index diagnosis in our study, was lower than demonstrated in previous studies, which reported a range of 15–25 years [28–32]. These studies use a range of methodologies to address survival, with differences in the case definition of HD index diagnosis, differing data sources, death reporting and follow-up periods. Due to the information truncation prior to observation period start, a number of prevalent cases identified during the initial years of our study may have been misclassified as incident cases. This may have resulted in shorter follow-up time from HD diagnosis to death, translating into shorter median survival time. In addition, this limitation may be responsible for at least some of the annual HD rate instability in our study, as cases diagnosed prior to early years of observation may have been included in the counts of these early years.
The mean age of HD diagnosis in our study was ∼50 years (SD ∼13), which is consistent with previously published registry data [5, 29]. The female-to-male ratio was 1.3, similar to that published in US and other countries [10, 33–36], but higher than reported in UK and Germany, where males predominated [24, 26]. The mean age of death in our study was 58.9 (SD = 13.3) years, similar to previous reports [29].
In our study the genetic HD test was performed as part of the diagnostic process, with 44%of the patients having performed the test. In other Western countries, a predictive HD testing is performed among ∼10 and 20%of those at risk, with global estimates of HD testing range between 5 and 45%[12, 37]; however, predictive testing for HD was not examined in this study. HD testing has been performed in MHS since 2002, as part of the diagnostic confirmation in patients with suspected HD. As HD is an autosomal dominant disorder, testing may be delayed or else not performed if perceived to be unnecessary, given a family history and a characteristic clinical presentation.
The baseline rates of anxiety (40%) and other behavioral problems (34%) in our study were as expected, based on the comparison with previous studies using rating scales for diagnosis [38]. Falls were reported in 13%of patients in our study, which is lower than previously described [39, 40]. Accurate measurement of fall frequency is, however, a known methodological challenge in HD research, as it relies entirely on patient self-report [39].
The range of HD treatments was consistent with current treatment recommendations targeting the cognitive, motor, and behavioral manifestations of HD [8]. The drug classes used most frequently were in line with HD registry studies, where antidepressant and antipsychotic use was found to be common [24, 35]. It is of note, that these treatments rates in our study population are substantially higher than those reported in the general Israeli population [41, 42]. Opioid use in our study (39%) was close to the prevalence of pain found in a European HD registry (41%) [43]. This is of importance, as it has been suggested that pain assessment in patients with HD may be difficult [8], and leads to inadequate pain management. It should be noted that opioid use may be related to HD, or other comorbidities, but this was not explored in the current study.
The only drug specifically indicated for HD chorea in Israel during the study period was tetrabenazine, which was used by the majority of our cohort (63%). The observation that 27%of tetrabenazine treatment was given prior to index diagnosis indicates that treatment was initiated based on chorea manifestation during the onset of motor symptoms or the prodromal phase of illness, but prior to final diagnosis of HD. While the diagnostic workup of HD is initiated when the patient exhibits motor symptoms, the exact date of diagnosis is not straightforward, and neurologists may prescribe tetrabenazine during the disease stages when motor signs are present, but diagnostic confidence is less than 99%[44, 45]. This could explain the gap between the symptomatic treatment initiation, and date of final HD diagnosis documented in patient’s record. Tetrabenazine treatment distribution around the index diagnosis in our study was equal to the distribution of chorea events around index HD diagnosis in the PREDICT-HD study [36]. This demonstrates that the start of symptomatic treatment relatively to HD diagnosis in our study is consistent with previous large observational studies.
Our study provides information on HD management changes over an extended period of time. High prevalence of depression (44%), sleep impairments (23%), and other behavioural disorders (37%) on or before the year of diagnosis represent treatable symptoms that may be missed in patients whose HD diagnosis is not acknowledged by the healthcare system. Increased awareness of these behavioural problems across HD families, healthcare systems and employers would have a positive impact on the access to symptomatic therapies and help to improve quality of life in HD patients and their families. Our results indicated that disease management became resource demanding soon after the diagnosis [5, 46]. Each examined post-diagnosis interval showed a high utilization of ambulatory services with a marked addition of hospital- and home-based treatments after the first year. Given the disease progressive nature, it is likely that those who had the diagnosis for a longer time had a more severe disease and were more impaired, which would explain the increase in utilization of hospital- and home-based care. Together these findings are important for acknowledging the burden of disease on the patients and healthcare services up to 20 years after a diagnosis. Similarly to studies using US health insurance claims data, Maccabi claims and electronic health records real-world data may be used to derive healthcare utilisation costs specific to HD patient in Israel, which may help drive healthcare policy discussions and discussions on local drug reimbursement of future disease modifying therapies as they become available.
Limitations
This study was a retrospective analysis of structured healthcare data and has limitations relating to the observational design. While the study captures comprehensive data, some clinical information was not fully available in tabular format amenable to analysis (including certain symptoms, disease-specific-scales, CAG repeat length, cause of death or causes of visits to ED/ICU). Clinical data generated outside of MHS clinics, such as mental health care, may be an additional source of underreporting, although, due to Israel’s national insurance plan, the extent of such missing data is overall likely to be small. It should be noted that, although health insurance is mandatory in Israel, individuals may be enrolled in insurance plans other than MHS; therefore, the results reported in this study may not be generalized to other demographics. Finally, because HD is a rare disease, the final cohort size was limited to 109 patients, despite the fact that this was a population-based study comprising > 3 million historic and concurrent MHS members. Multiple data sources from various countries would be needed to further characterize the course and population-level impact of this devastating disease.
Conclusions
This retrospective population-based study offers an important perspective on the prevalence, incidence, clinical profile, survival, and resource utilization of patients with HD in Israel. These real-world data provide insights that can inform healthcare planning and public health decision-making, thus demonstrating the value of routinely collected healthcare data as a complementary resource in HD research.
Footnotes
ACKNOWLEDGMENTS
This project was funded by F. Hoffmann-La Roche Ltd. Editorial assistance was provided by Bill Kadish of Parexel and Matt Gooding of MediTech Media (UK) with funding from F. Hoffmann-La Roche Ltd.
CONFLICT OF INTEREST
Natalie Gavrielov-Yusim, Michael Martinec, Athanasios Siadimas, Spyros Roumpanis, Hannah Furby and Asif Jan are employees of F. Hoffmann-La Roche Ltd. At the time of this study, Preciosa M. Coloma was a full-time employee of, and owned shares in, F. Hoffmann-La Roche Ltd. Yael Barer and Inbal Goldshtein have no conflict of interest to report.