
Abstract
This study assesses the possible side effects of various doses of dapagliflozin. Dapagliflozin is a hypoglycemic agent that inhibits sodium-glucose co-transporter-2 (SGLT2) to remove excess glucose from the body through urination. Hence, dapagliflozin increases the risk for urinary tract infection (UTI) compared with other hypoglycemic agents. Clarifying the side effects of dapagliflozin at different doses and whether these effects are influenced by gender or other factors is significant. Through reviewing the literature on dapagliflozin treatment, we performed a meta-analysis of factors affecting UTI. We then determined the correlation of dapagliflozin treatment with UTI from the pooled data. Each dosing, gender group, or dapagliflozin added to other drugs for diabetes reported a percentage of contracting UTI. Basing on a reference number of pretreatment probability in UTI among patients with diabetes mellitus, we obtained the post-treatment probability in contracting the infection through the meta-analysis. We assessed the risk factors of UTI due to dapagliflozin administration on the basis of the results of odds ratio, regression analysis, and t-test. Considering the add-on-response relation, we recommend that the best add-on hypoglycemic agents to achieve low-risk UTI and control blood glucose are metformin or glimepiride. We also recommend that the best dosage of dapagliflozin is at 1 mg or 2.5 mg.
Introduction
Type 2 diabetes mellitus is the most common and dangerous disease worldwide. Although many drugs are available for diabetes treatment, this disease still causes high morbidity and mortality rates worldwide [1, 2]. The increased prevalence of diabetes has raised the proportion of cardiovascular diseases attributable to diabetes. The need for diabetes control is thus necessary [3]. In 2013, the first sodium-glucose co-transporter-2 (SGLT2) inhibitor was launched. The use of SGLT2 inhibitors is a novel strategy for treating type 2 diabetes [4]. SGLT2 inhibitors reduce blood glucose by the mechanism of the kidney, which starts an SGLT2 upregulation and increases glucose reabsorption along the proximal tubules [5, 6]. SGLT2 inhibitors block glucose reabsorption, thereby reducing calories, weight, blood pressure, and cardiovascular complications [7]. However, accumulated glucose in the urine serves as a nutrient for bacteria, which could cause urinary tract infection (UTI) [8, 9]. UTI results from unfavorable predisposing lesions, such as congenital abnormalities, gall stones, indwelling catheter, prostatic hypertrophy, obstruction, or neurological deficits, which interfere with the normal flow of urine and urinary tract defenses. To date, SGLT2 inhibitors canagliflozin, dapagliflozin, and empagliflozin are used to treat type 2 diabetes mellitus and the drugs has been approved by the Food and Drug Administration (FDA) and European Medicines Agency.
Among the three drugs, dapagliflozin has usually been reported that its side-effect of UTI is prominent for patients taking certain amount of doses [7, 10]. Thus, clarifying the side effects of dapagliflozin at different doses and whether these effects are influenced by gender, age, or other factors is significant. Risk factor is a variable associated with an increased risk of UTI. Identifying the risk factors can also help physicians make a benefit–harm assessment and caution patients using dapagliflozin.
Method
Data sources and study selection
This study was conducted in accordance with a protocol and followed the standard guideline for conducting and reporting a systematic review involving a network meta-analysis [11]. We searched the PubMed Central® biomedical digital database for any studies published in English or Chinese from inception until 12 June 2017 with the keyword “dapagliflozin” limited in human use. Then, we included studies with the keyword “urinary tract infection.”
Subsequently, we excluded all studies without participant number information. UTI outcomes comprised clinical diagnoses of UTI and signs, symptoms, and events suggestive of UTI. Then, we manually examined for additional relevant publications.
Incidence of UTI with or without dapagliflozin
We carried out a network meta-analysis, an alternative to the Bayesian approach. Data from 12 trials were pooled to evaluate the correlation of UTI probability (UTI%) with taking dapagliflozin or placebo. The rate of UTI with and without dapagliflozin was calculated, and the binomial test was used for analysis. The null hypothesis is that the two populations (dapagliflozin and placebo) are equal. Binomial test results were reported with 95% confidence intervals (CIs), and statistical significance was considered at p < 0.05. If the p-value from the binomial test result is less than 0.05, then the null hypothesis is rejected in favor of the alternative hypothesis. Meanwhile, if the p-value is greater than 0.05, then the null hypothesis is accepted.
Correlation analysis of dapagliflozin doses
All studies with gender information were collected. Then, we divided these studies into the placebo and dapagliflozin groups. We applied z-test to determine whether the male and female participants from each group significantly differ in UTI%. Software R was used for statistical computing and graphics. The results were described with 95% CI. In addition, odds ratios (ORs) were used to measure the association between males and females with UTI% while taking dapagliflozin. We calculated ORs using a two-by-two frequency table.
After calculating the UTI% in different dapagliflozin doses, we performed three analyses to determine their correlation. First, considering the sample size difference, we performed two-tailed t-test to analyze the differences in UTI% at different doses of dapagliflozin compared with placebo. Moreover, we analyzed the differences in UTI% between different doses (p < 0.05 considered statistically significant). Second, ORs were determined to identify the correlation between different dapagliflozin doses and UTI%. UTI% was weighted according to the population size of source data. Furthermore, factors are modeled as dummy variables. The dummy variable result indicates the correlation between different dapagliflozin doses and UTI%.
We also perform correlation analysis of dapagliflozin with other diabetes drugs. The designate dummy variables are able to describe the correlation between different dapagliflozin doses, add-on drugs gender effect, and UTI%.
Results and discussion
Study characteristics
From 308 identified studies, we excluded non-human, non-English or Chinese studies, finally leaving 12 studies for full-text assessment. Reference lists of eligible studies, as well as the therapy design, sample size, and other information, were also considered (Table 1). The number of participants differed in each dosing group (Fig. 1). From these 12 studies published between 2009 and 2015, 5805 (range 71–1246) participants were included. Study duration ranged from 2 weeks to 102 weeks. Six studies out of 12 were placebo versus dapagliflozin, whereas others were dapagliflozin plus other hypoglycemic agents. All trials were conducted in accordance with the guidelines of Good Clinical Practice. All participants provided informed consent prior to engaging in their respective clinical trials.
Baseline characteristics of the included studies
Baseline characteristics of the included studies
Dapa: dapagliflozin.
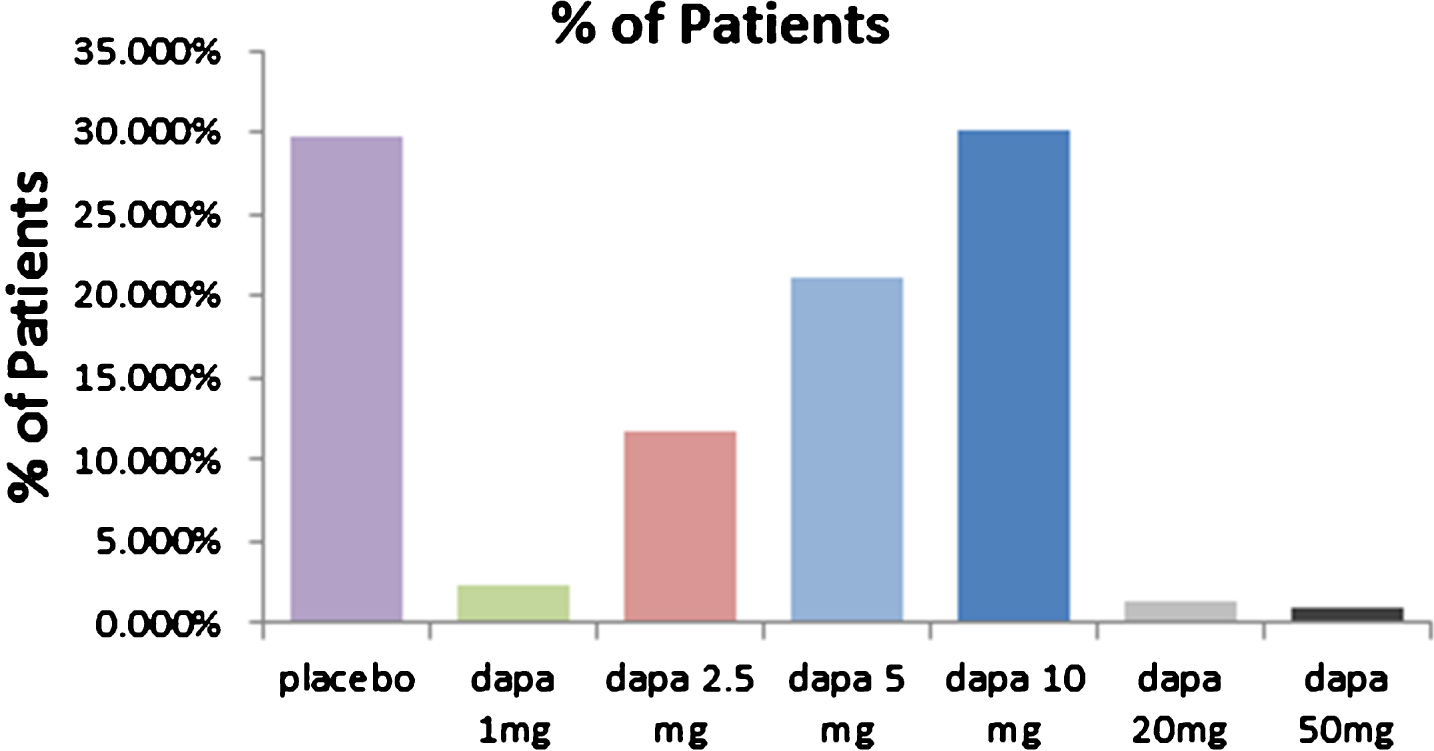
Sample size comparison of dose-related trends in the dapagliflozin trials.
The numbers of patients with UTI in the dapagliflozin and placebo groups are shown in Fig. 2. The incidence rates of UTI in the dapagliflozin and placebo groups were 5.743% (standard deviation: 2.455–9.032) and 4.333% (standard deviation: 0.333–8.332), respectively. On the basis of the binomial test result, the null hypothesis was rejected with 95% CI (p < 0.001). The UTI proportion in the dapagliflozin group was significantly greater than that in the placebo group (Fig. 2).

UTI patient number in the dapagliflozin and placebo groups.
The numbers of male and female patients with UTI in three studies with gender information are shown in Table 1. In these three studies, there were 475 males and 507 females (Fig. 3). In the placebo group, the UTI% values in the males and females were 1.596% and 11.561%, respectively. In the dapagliflozin group, the UTI% values in the males and females were 4.530% and 8.683%, respectively. With 95% CI, the z-test results showed that the two null hypotheses were rejected in the placebo and dapagliflozin groups. Infection was more common in females than that in males in both groups. Furthermore, the OR was 2.02 with dapagliflozin exposure. The UTI% in women was 2.02 times greater than that in men (Table 2).

Numbers of male and female patients with UTI in studies with gender information.
Two-by-two frequency table of OR
The incidence of UTI between different dapagliflozin doses is shown in Fig. 4 (the 50 mg group cannot be calculated because of only one data of UTI incidence). A t-test result showed that among the different dapagliflozin doses, 5, 10, and 20 mg significantly increased the UTI risk compared with placebo (Table 3). The OR values are shown in Table 4.
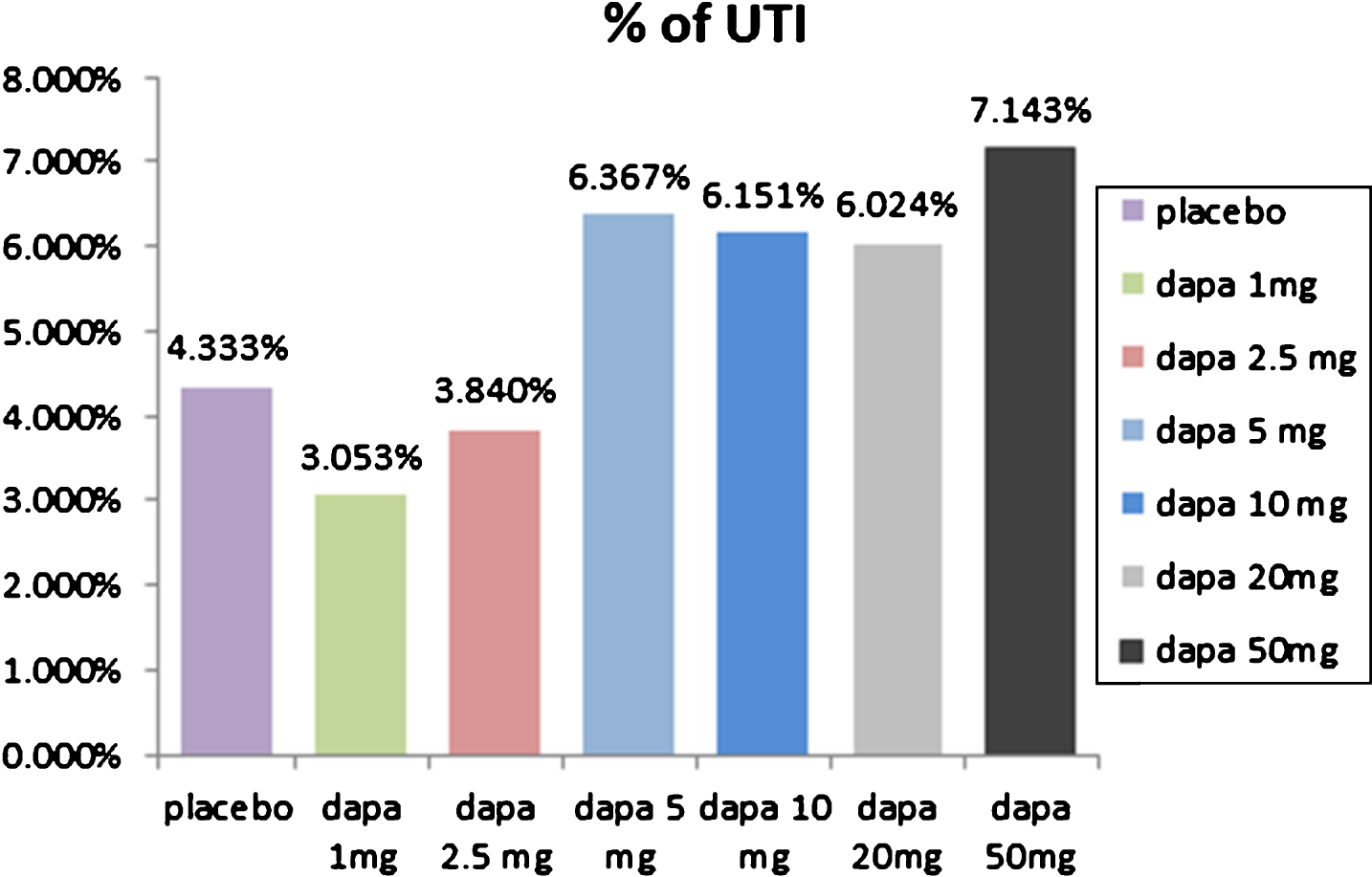
Percentage of UTI in patients treated with different dapagliflozin doses.
Statistically significant result from t-test. *: significant
Dapa: dapagliflozin.
Odds ratio comparisons of UTI% between dapagliflozin doses and placebo (i.e., UTI% was 1.641 times higher with 10 mg than with 2.5 mg dapagliflozin)
Dapa: dapagliflozin.
We model the dose prescribed as dummy variables. Let x1: 1 mg; x2: 2.5 mg; x3: 5 mg; x4: 10 mg; x5: 20 mg; and x6: 50 mg. The regression yielded:
UTI% = 0.049 – 0.016x1 – 0.010x2 + 0.016x3 + 0.017x4+0.012x5+0.021x6.
All coefficients were significant with p-values less than 0.001. The goodness of fit value R2 = 0.034 and CI was 99.9%. The result demonstrated a positive correlation between dapagliflozin dose and UTI incidence.
All dose groups significantly affected UTI probability. The 1 and 2.5 mg groups showed reduced UTI incidence.
We cannot reveal the correlation between dapagliflozin as an add-on therapy to sitagliptin (CI: 0%), pioglitazone (CI: 0%), or insulin (CI: 90%) and the chance-experienced UTI. UTI% was reduced when dapagliflozin was added with metformin and glimepiride (CI: 95%) (Table 5). As seen in dummy results, the P value of sitagliptin, pioglitazone and insulin were too large meaning that we could not tell their effect to UTI. P value of metformin and glimepiride, however, were significantly small. The coefficients of metformin and glimepiride were negative, resulting in the UTI% become lower when dapagliflozin add to these two drugs.
Dummy variable result using dapagliflozin as an add-on therapy to hypoglycemic agents
Dummy variable result using dapagliflozin as an add-on therapy to hypoglycemic agents
Dapa: dapagliflozin.
Comparison of dose-related trends in male and female patients with UTI in dapagliflozin trials with gender information was showed in Fig. 5. The data has been divided by two groups: male and female. The dummy variable result still showed a positive correlation between dapagliflozin dose and UTI incidence.
UTI% = 0.095 – .058x1 – .028x2 – .013x3 + 0.016x4 – 058x5.

Comparison of dose-related trends in male and female patients with UTI in dapagliflozin trials with gender information.
The 20 mg and 50 mg of dapagliflozin studies had no gender information so that their dummy variable cannot be calculated for the dapagliflozin doses and gender correlation. The 2.5, 5, 10 mg, and gender groups significantly affected UTI% (p-values were small). The overall goodness of fit value R2 = 0.360. Females showed more chance of acquiring UTI than males (coefficient of x5 was negative).
Within the language limitation, we collected original studies only in English and Chinese. We may ignore some relevant publications written in other languages, resulting in bias.
Our study showed that the UTI incidence in the dapagliflozin group (5.743%) was significantly greater than that in the placebo group (4.333%). SGLT2 inhibitors accumulated glucose in the urine, which increases the risk for UTI. The result was close to the incidence data according to the original dapagliflozin manufacturer (4.3% –5.7%) [23]. The FDA released a warning on May 15, 2015. In this warning, 19 cases of life-threatening blood infections (urosepsis) and kidney infections (pyelonephritis) that started as UTI with the SGLT2 inhibitors were reported to the FDA Adverse Event Reporting System from March 2013 to October 2014. Therefore, patients should be cautioned for signs and symptoms of UTI when doctors prescribe dapagliflozin to avoid severe adverse drug reaction.
Our review shows that not all 12 trials had gender information, causing not enough number of male or female patients to calculate (six studies). Furthermore, studies displayed that UTI is more common in females than in males in the dapagliflozin group and placebo group with 95% CI. The UTI% in women with dapagliflozin exposure is 2.021 times greater than that in men with dapagliflozin exposure. In the reference, UTI prevalence varies with gender (pharmacotherapy). Approximately one in five women will suffer a symptomatic UTI at some point in their lives. By contrast, the prevalence in adult men is low (<0.1%) [24]. However, the rates reduced to 8.683% after taking dapagliflozin compared with taking placebo (11.561%). The result may be affected the most by one of the six trials, i.e., the one conducted by Matthaei et al. in 2015 [12]. The other five trials had higher UTI% in the dapagliflozin group than in the placebo group. In addition, the UTI% in the placebo group was almost twice that in the dapagliflozin group. Although different outcomes were observed from these six studies, we still confirmed that females have a higher chance of acquiring UTI compared with males whether in the placebo group or the dapagliflozin group. Females and their physicians must be aware of this fact.
All doses (1, 2.5, 5, 10, and 20 mg) except 50 mg significantly affected UTI%. Low doses (1 and 2.5 mg) can decrease UTI%, whereas high doses (5, 10, and 20 mg) can elevate UTI%. Increasing glucose in the urinary tract provides conducive environment for bacteria. The doses were not continuous variables; thus, the linear relationship between dose and UTI cannot be confirmed. The sample size was relatively small in the 1, 20, and 50 mg groups (less than 30). The results may be not accurate because we simulated the normal distribution using a statistical method during calculation, which could reduce the credibility of the results.
UTI incidence is reduced when dapagliflozin is added to metformin and glimepiride. The pharmacological explanation remains unknown but can be attributed to the good glycemic control of the two drugs. However, in all studies on dapagliflozin as add-on drug, the sample size was very small (less than 30), which reduces the credibility of the results. Thus, the results could only be used for reference.
We should consider some limitations of the present studies. First, we did not determine if the females experiencing UTI after taking dapagliflozin are menopausal. Females have a high chance of acquiring UTI during menopause. We suggested that some UTI incidences are due to the physical mechanical change in the bladder rather than the intake of dapagliflozin [1]. Second, we did not identify if the patients had other UTI risk factors during clinical trials. For example, a significant proportion of females with a history of childhood infections are prone to recurrent infections. Therefore, UTI% can be partly attributed to other UTI risk factors aside from taking dapagliflozin. Finally, data on 1, 20, and 50 mg dapagliflozin have been reported only in 3, 2, and 1 studies, respectively, thereby limiting the possibility of performing a complete analysis. The results of these three groups may decrease the credibility of our findings. Additional studies should be published in the future to minimize the influence of these biases.
Conclusions
This pooled meta-analysis revealed some risk factors of patients taking dapagliflozin as glycemic control. UTI% can be predicted on the basis of different factors, such gender, dose, and other add-on hypoglycemic agents. The UTI incidence was higher in the dapagliflozin group than in the placebo group. Increased dose corresponded to increased UTI incidence. Considering the minimized risk of contracting UTI and the maximized control of blood glucose, the results showed that the best dosage is at 1 mg or 2.5 mg. Females had a greater chance of acquiring UTI than males. Dapagliflozin as an add-on therapy to sitagliptin, pioglitazone, or insulin did not affect the chance of acquiring UTI. UTI% reduced when dapagliflozin was added with metformin or glimepiride. When available, patients are advised to use dapagliflozin as an add-on drug to metformin or glimepiride and use low-dose dapagliflozin to reduce UTI incidence. Ongoing clinical trials with UTI outcome will clarify whether UTI incidence is influenced by other factors.
Footnotes
Acknowledgments
This work was supported in part by grants from the Ministry of Science and Technology, Taiwan (MOST 104-2410-H-327-018-MY3, 106-2221-E-037-001, 106-2622-E-037-005-CC3, 106-2218-E-327-001, 107-2221-E-037-006, 107-2218-E-992-308), and the “Intelligent Manufacturing Research Center” (iMRC) from the Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan.