
Abstract
This article presents optimal drug scheduling in chemotherapeutic treatment for eradication of cancerous cells while maintaining tolerable toxicity for the complete period of treatment. For this purpose a cascade control technique is designed wherein individual 2DOF FOPID controllers are employed to regulate drug concentration and toxicity. Conventional schemes fail to address the needs of divergent objectives of cancer chemotherapy which motivates the authors to employ a multi-objective optimization technique, NSGA-II to optimally tune the controller parameters. 2DOF FOPID, its integer order counterpart and PID control schemes are tested on cancer patient model for comparative analysis. The performance of proposed controller is evaluated on the basis of number of cancer cells and normal cells remaining at the end of treatment. Further robustness of the controller is analysed for parametric uncertainty in patient model and disturbance in infusion pump which affects the input drug dosages. The results reveal that proposed control scheme provides optimal drug scheduling and is significantly robust in the presence of uncertainty and disturbances.
Keywords
Introduction
Cancer is a disease in which abnormal growth of cells takes place and has the potential of spreading to other organs of the body. The proliferation in cancerous cells is exponential in nature and is generally measured in terms of number of cancer cells. Cancer informatics is an interdisciplinary science which utilizes biological data to understand the behavior and growth of tumor. It also includes but is not limited to mathematical modeling, design of optimal treatment protocol and management. Cancer informatics has acquired the growing interest of researchers as it presents the challenges in clinical implementation of technology. The requirement of advanced automation and optimization has inspired the engineers to apply control theory principles in this field.
Chemotherapy is an essential method often used by clinicians for treatment of cancer. It involves deployment of drugs that destroy cancer cells in a pre-programmed way known as apoptosis, with the ideal goal of complete elimination of cancerous cells and minimum harm to rest of the body. It is of primitive importance to find optimum drug dose that offers effective treatment with minimum side effects. Thus drug concentration is maintained such that total toxicity is below threshold values during the treatment. This problem may be solved by drug scheduling with the help of optimal control strategy. The chemotherapy regimen defines the drugs to be used, its frequency and dosage, and the period of treatment along with other considerations. In general, these chemotherapeutic drugs are toxic in nature and work on mechanism of impairing cell division. The current scenario for treatment of cancer by chemotherapy is based on the information acquired from clinical trials performed during the process of drug development [1, 2].
The mathematical model of cancer patient relates population of cancer cells, normal cells, and toxicity to drug dose & concentration. Different models of tumor behavior are proposed in literature and the most commonly used are Gompertz model, exponential model and models based on metabolic considerations. Swan [3] discussed various models such as miscellaneous growth kinetic models, cell cycle models, physiological models etc. The unperturbed growth of cancer cells is also described in [4] by considering constrained cumulative toxicity. The control parameterization technique was established for optimal control of drug scheduling. The results obtained claim that minimum initial drug dose followed by high intensity chemotherapy at the end of treatment is more effective. Athanassios et al. [5] described the dynamic relationship between administered drug and its concentration at cellular level by pharmacokinetic- pharmacodynamics modeling. Open loop control is used while considering constrained plasma concentrations, drug exposure and toxicity limits. The quasi-Newton constrained method was employed for optimization. Various authors have also discussed closed loop control strategy for chemotherapeutic treatment. A recent research by Alam et al. [6] implemented a closed loop I-PD control for multi-compartment model of tumor tissues comprising proliferating, quiescent and dead cells. A multi objective genetic algorithm is used for controller tuning. Khadraoui et al. [7] presented a measurement-based control to address the problem of cancer treatment using a set of frequency-domain data. A GA optimized cascade PID is proposed to find optimal drug schedule with constraints on drug concentration and toxic side-effects.
It is revealed from literature that PID controller has evolved with time, and more advanced techniques like intelligent PID, fuzzy PID, fractional order PID and hybrid techniques are now available which enhance the capabilities of conventional PID controller in various aspects [8–15]. The degree of freedom of controller plays an important role in the design of an efficient control scheme for multi-directional problem, [16]. Single DOF controller is not capable enough to deal with multiple problems simultaneously which motivates researchers to utilize 2DOF PID controller. Recently, Mohan et al. [17] proposed analytically derived two-degree-of-freedom fractional order fuzzy PI-D controller for complex nonlinear systems. It utilizes formula based fuzzy design which proved to be more robust and efficient as compared to the conventional techniques. Extensive research is carried out to incorporate fractional calculus in the field of control so as to provide more flexibility to design and increase its potential as well as scope of utilization. In some studies the integer order differ-integral operator in simple PID are directly replaced by fractional operators and results claim that FO techniques perform superior as compared to their integer order counterpart [18, 19].
In chemotherapy, the cytotoxic agents do not provide selective toxicity and hence kill cancerous cells as well as fast dividing normal cells such as blood cells, hair follicles etc. This motivates the utilization of advance control practices in the field of clinical sciences for optimization of chemotherapeutic treatment by manipulating drug dosage so as to limit the toxic side effects. Further, to obtain a compromising solution between conflicting targets, various researchers incorporate multi-objective evolutionary optimization algorithms like, MODA, MOMVO, MOCSA, NSGA II, MOWCA [20–24].
The mathematical models help in analysing, testing new technology and its effects before actual clinical trials. A treatment involving low dosage, may not be effective enough to deal with malignant cell population. Whereas, a treatment protocol administering high initial drug dosages needs regulated interruption plan to restrain the side effects and toxicity level. Simulated model of tumor provides secure alternative to clinical experimentation in such cases, as it is immoral to examine new combination and regimen of drug on patient during trials. Thousands of drug combinations and chemotherapy regimen could be tested on simulated patient model and few best selected solutions could be clinically examined which increases the prospects of patient survival [25–27].
Therefore present study extends the concept of fractional calculus to design Two Degree of Freedom-Fractional Order Proportional Integral Derivative (2DOF FOPID) controller based cascade control scheme to achieve effective regulation of drug concentration and cumulative toxicity. In this work, normal cell population is also taken into account and various constraints are applied so that chemo-drugs cause minimum harm to normal cells. A multi-objective optimization technique NSGA-II is used to estimate the controller parameters, to trade-off cell killing and toxic side effects. The effectiveness of proposed controller is examined on a simulated patient model in terms of number of cancerous cells and normal cells remaining at the end of treatment. Further to demonstrate the efficacy and robustness of the proposed optimal drug scheduling, parametric uncertainty and disturbance are introduced in chemo-model.
The major contributions of this paper can be recapitulated as follows: An advanced cascade control scheme utilizing 2DOF FOPID controller to manipulate drug dose for cancer chemotherapy regimen is proposed. The FO differ-integral operator is designed in discrete time domain by binomial expansion of backward difference transformation. A constrained Pareto-based multi objective optimization i.e. NSGA II algorithm minimizes toxic side effects and maximizes cancerous cell killing, which allows oncologists to choose from a set of good solutions as per patient’s condition. The robustness of controller is analyzed for disturbance in the input drug dose due to infusion pump and uncertainty in the parameters of tumor growth. The most important benefit of the proposed technique is that it kills maximum cancerous cells while satisfying various constraints on toxicity, drug concentration and drug dosages.
The paper is organized as follows. The mathematical model describing tumor behavior and effect of chemo-drugs are presented in Section 2. The proposed control method for cancer chemotherapy along with tuning of PID controllers is discussed in Section 3. In Section 4, the simulation results are presented and compared with results of existing techniques. Finally, concluding remarks are given in Section 5.
Mathematical model of cancerchemotherapy
Chemotherapy is a course of treatment involving the use of one or more anti-cancer drugs delivered to the patient by following a standard regimen. The amount of drug delivered and its duration both are crucial in this therapy. These drugs specifically kill fast dividing cells or damage the DNA structure thus preventing further replication of cancer cells [28]. The success of treatment may depend on physiological state of patient, location of tumor, interaction of drugs, duration of therapy etc.
It is important to have basic knowledge of the tumor growth to understand the actions of chemotherapeutic agents on cancerous cells. The main difference between cancerous cell and normal cell lies in the growth pattern rather than rate of growth. Normal cells generally have regulated growth with a balance in number of cells being produced and number of cells dying. Depending upon the type of cells, they have slow or fast dividing rate according to a pre-programmed function [29] for example, blood cells are rapidly dividing cells. On the other hand, cancer cells exhibit unregulated growth with very high cell division rate and there is no balance between cell production and cell death. Specific mathematical models of tumor growth that fit clinical data are available in literature which describe the increase in malignant cell population per unit time. The growth of tumor is given by exponential model, when the doubling time is assumed constant and is expressed below:
A tumor within clinical detectable capability having 2cm diameter may contain 109 cells. In this work, initial number of cancerous cells at tumor site in the beginning of treatment is assumed to be N (0) =1010 cells [7]. Clinical studies also show that most of the cytotoxic drugs kill cancerous cells by first order kinetics and cell killing does not depend on the size of tumor. Therefore, a logistic equation is used to mathematically describe the effect of anti-cancer drugs on tumor growth during the treatment and is expressed as
The anti-cancer drug infused to patient’s body not only kills the cancerous cells, but also affects normal cells. Limited growth rate is assumed for normal cells as cancer cells proliferate in uncontrolled manner. The growth of normal cell population and the effect of drug may be expressed by the following equations
T (t) and η are toxicity level in the patient’s body and elimination rate constant of toxicity respectively. As these drugs are toxic in nature, a constraint is imposed to restrict toxicity level such that toxic effect is enough to kill cancerous cells with minimum side effects. Minimum drug concentration level is also considered as a constraint, so as to maintain lower level of toxicity for effective cell killing. Another constraint considered is on the minimum acceptable normal cell population so as to avoid severe physiological damage to the patient.
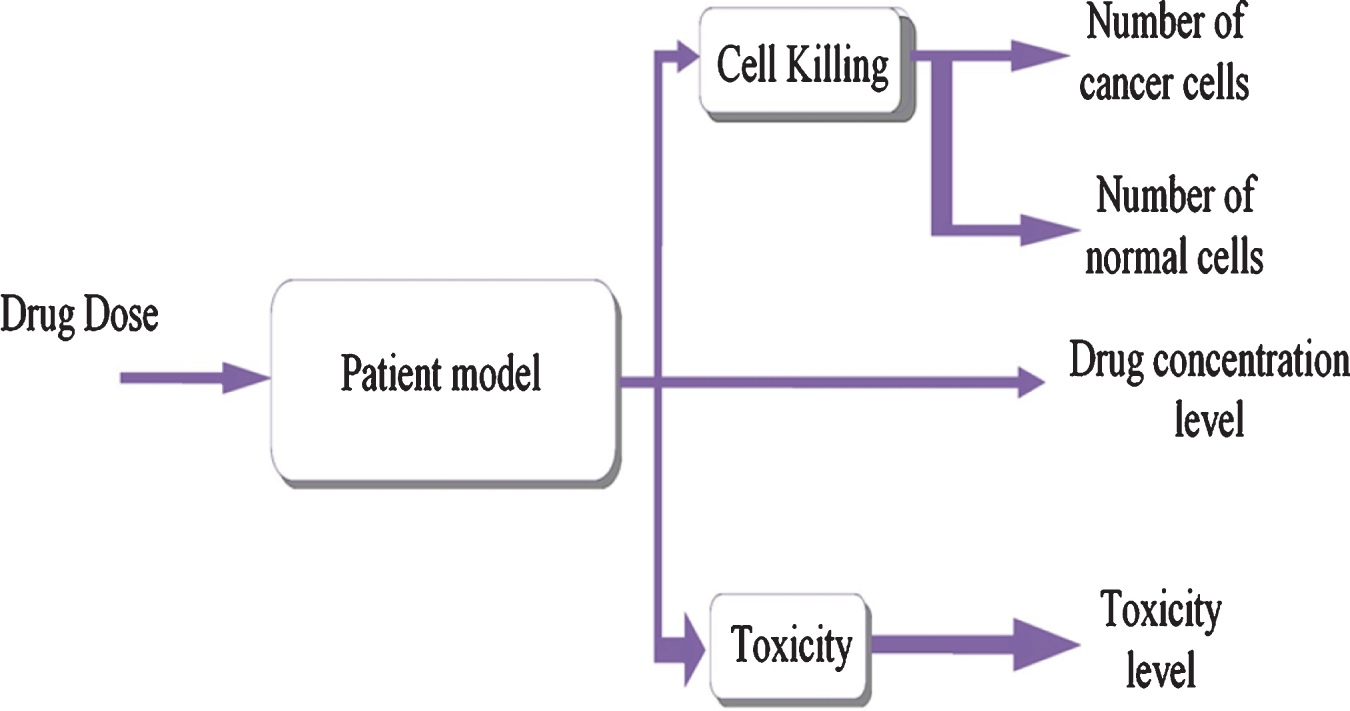
Figure 1 shows the block diagram of chemotherapy treatment model, which has one input variable ‘drug dose’ infused into patient’s body and four output variables i.e. toxicity, number of cancer cells at tumor site, normal cell population, and drug concentration level. Utilizing the above differential equations a model for chemotherapy treatment is simulated in MATLAB Simulink to test and quantify the proposed control strategy for optimization of drug scheduling. Parameter values used in the above equations are given in Table 1. Initial values of drug concentration level, toxicity level, and initial drug dose are considered to be 0.

Block diagram of cancer chemotherapy system.
Parameters of chemotherapy model
In chemotherapy, higher drug concentration causes increased cancer cell killing, which in turn increases toxicity level as well and harms normal cells too. These constraints on drug concentration and toxicity are conflicting in nature and hence a cascade control strategy with individual controller for manipulation of drug concentration level ‘C1’ and regulation of toxicity ‘C2’ (Fig. 2) is designed.
Schematic diagram of cascade control scheme.
The controller C1, in inner loop maintains a specified drug concentration level in the range (10, 50) i.e. greater than threshold 10 and smaller than the limiting value of 50, for effective cell killing. The cumulative drug toxicity for complete duration of treatment is obtained by integrating drug concentration level. Therefore, outer loop controller C2 keeps the toxicity at a predefined level of 100 for efficient chemotherapy. The drug infused to the patient is obtained through controller C1. In the designed control scheme both C1 and C2 controllers are considered to be same. The performance comparison is made by considering three cases using 2DOF FOPID, 2DOF PID and PID controllers.
A two degree of freedom fractional order PID control technique can efficiently address the issue of multiple constraints in chemotherapy system. The 2DOF control structure consists of two closed loops to regulate the set point and reject disturbance thus providing robustness to the system [30]. The proposed controller is mathematically defined as:
The Equation (8) can be simplified as
Substituting, ‘E = R - Y’ and writing the Equation (11) in the form of error and output,
Equation (13) describes the final control action U2DOF FOPID, generated by the proposed 2DOF FOPID scheme and is used to manipulate the drug dose along with regulation of toxicity level. The complete time span of chemotherapeutic treatment is considered to be 84 days as recommended by various researchers in literature. The block diagram of 2DOF FOPID controller is shown in Fig. 3. The basic arrangement of 2DOF FOPID is obtained in the form of serial compensator and feed-forward compensator, which are tuned independently. Sudden changes in drug dosages due to derivative action are dealt using a filter to completely avoid the derivative kick. The integer order counterpart 2DOF PID is also designed by taking order of fractional operators as unity.
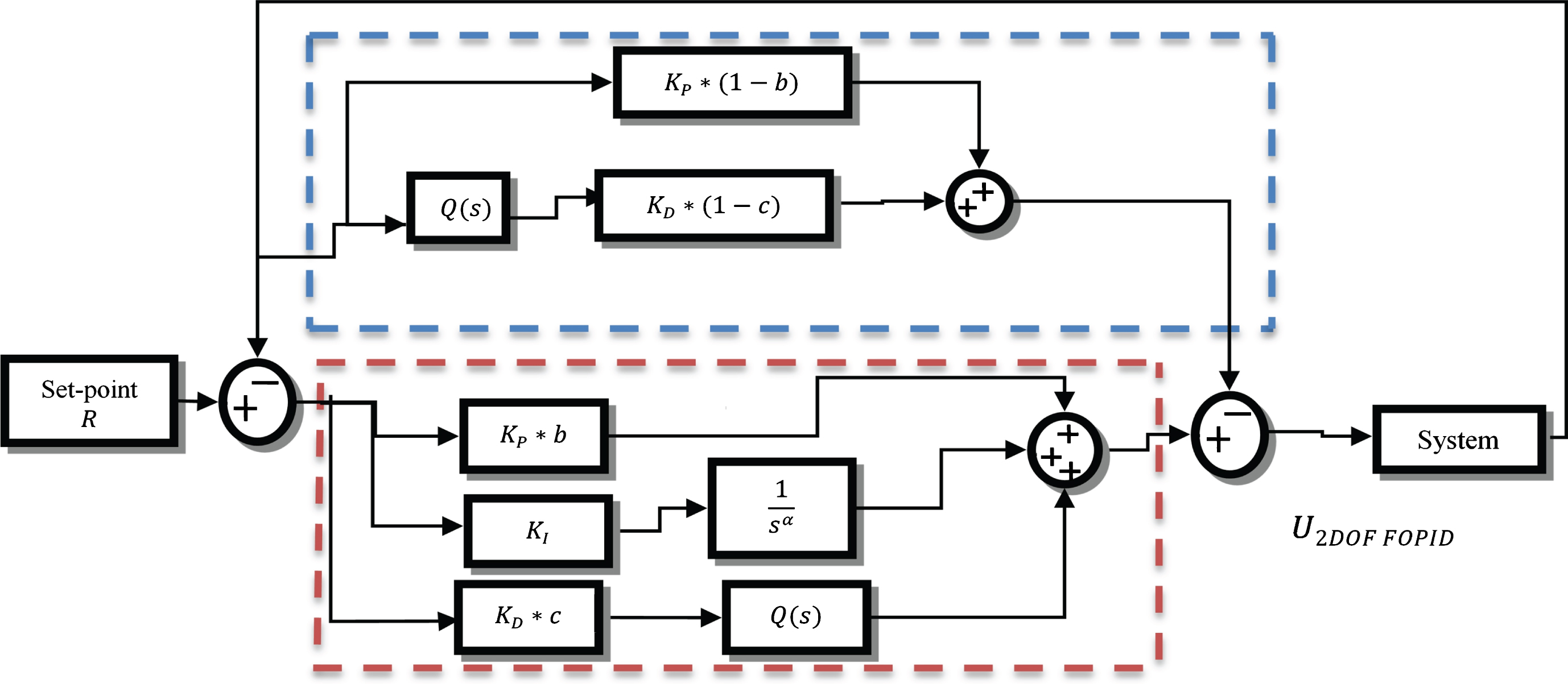
Block diagram of 2DOF FOPID controller.
In conventional PID control scheme, the error e (t) = r (t) - y (t) is minimized by integer order integral and differential actions. Application of fractional order calculus in PID controller provides extra flexibility to conventional design. Various methods are reported in literature to implement fractional operators [31]. In the present work, fractional order differ-integral is designed in discrete time domain by binomial expansion of backward difference transformation [17] as
In order to realize Equation (16) the number of coefficients and delay units to be computed is extremely large. So, principle of short memory is employed to devise a practically viable fractional order operator.
Evolutionary multi-objective optimization algorithms provide several satisfying solutions by trading off amongst various conflicting objectives [23]. This feature makes it apt for the purpose of tuning a controller with large number of parameters. The goal values, constraints and objectives of optimization problem are framed prior to the execution of algorithm. The goal is to attain minimum number of cancer cells and maximum number of normal cells at the end of treatment. As the drug infused in the patient body regulates the drug concentration and toxicity, it needs to be carefully administered to avoid side effects. Therefore, few constraints are imposed on cumulative toxicity level, drug concentration level and minimum number of normal cells as discussed in Section 2.
The multi-objective optimization NSGA-II is utilized to find parameters of designed control scheme while optimizing the conflicting objectives subject to the mentioned constraints. The sum of absolute error (e1) in toxicity level at tumor site (Z1) and sum of absolute error (e2) between desired and actual drug concentration (Z2) are the two objective functions considered for optimization.
The aim is to improve the adaptive fit of population of solutions to Pareto front constrained by objective functions on the basis of non-dominated sorting and crowding distance. The design steps for implementing NSGA-II are described below [32] The first generation of size P is randomlygenerated. The objective functions are evaluated for 1st generation. The population is then sorted by providing a rank according to non-dominance level. Select parent population by binary tournament selection. Two solutions are randomly selected and their non-dominance ranks are compared, the better solution is retained as parent. The solutions with same rank at same non-dominance front are then sorted by crowding distance technique. The off-spring population of size P is generated by genetic operators, crossover and mutation from selected parent population. The objective function for off-spring solutions is calculated. The parent and off-spring solutions are combined to form a population of size 2P and assign rank on the basis of non-dominance. Select P best solutions as next generation population by elitism and discard other solutions. Check if stopping criterion is met or if maximum number of generations is reached. If stopping criteria are not satisfied, repeat steps 4 to 10 otherwise stop further generation.
NSGA-II tuned 2DOF FOPID controller in cascade control scheme is proposed for optimal drug scheduling in cancer chemotherapeutic treatment. Exponential model of tumor growth is considered and normal cell population is also taken in account to analyse the effect of drugs on fast dividing cancer and normal cells. The integer order 2DOF PID and cascaded PID controllers are also designed for comparison purpose.
Reduction of cancerous cells
Simulations are performed in MATLAB with sampling time of 100 samples per day. The value of input drug dose is limited to the range [10–50]. The parameters of proposed 2DOF FOPID and 2DOF PID are tuned optimally by NSGA II, whereas the parameters of PID controller are taken from [7] and recorded in Table 3. The parameters of NSGA-II and bounds for controller parameters are recorded in Table 2. NSGA-II algorithm provides multiple non-dominated solutions instead of a unique optimal solution, which are plotted in multi-dimensional objective’s space to form the Pareto front. The plot helps to address the problem of trade-off, by characterizing the fact that a solution cannot be improved in one dimension without worsening in others. The Pareto front, representing set of optimal solutions for tuning 2DOF FOPID and 2DOF PID controllers are shown in Fig. 4 (a) and (b) respectively. Although any point from this set would provide satisfactory results, optimum solution is obtained when both the objectives are simultaneously minimized. Therefore, solutions close to origin in objective space are considered. In this work three solutions closer to origin are selected and controllers are tuned accordingly. The best solution out of the three is finally used for the desired control and highlighted with red color in Fig. 4. The corresponding controller parameters and objective values for 2DOF FOPID, 2DOF PID are listed in Table 3.
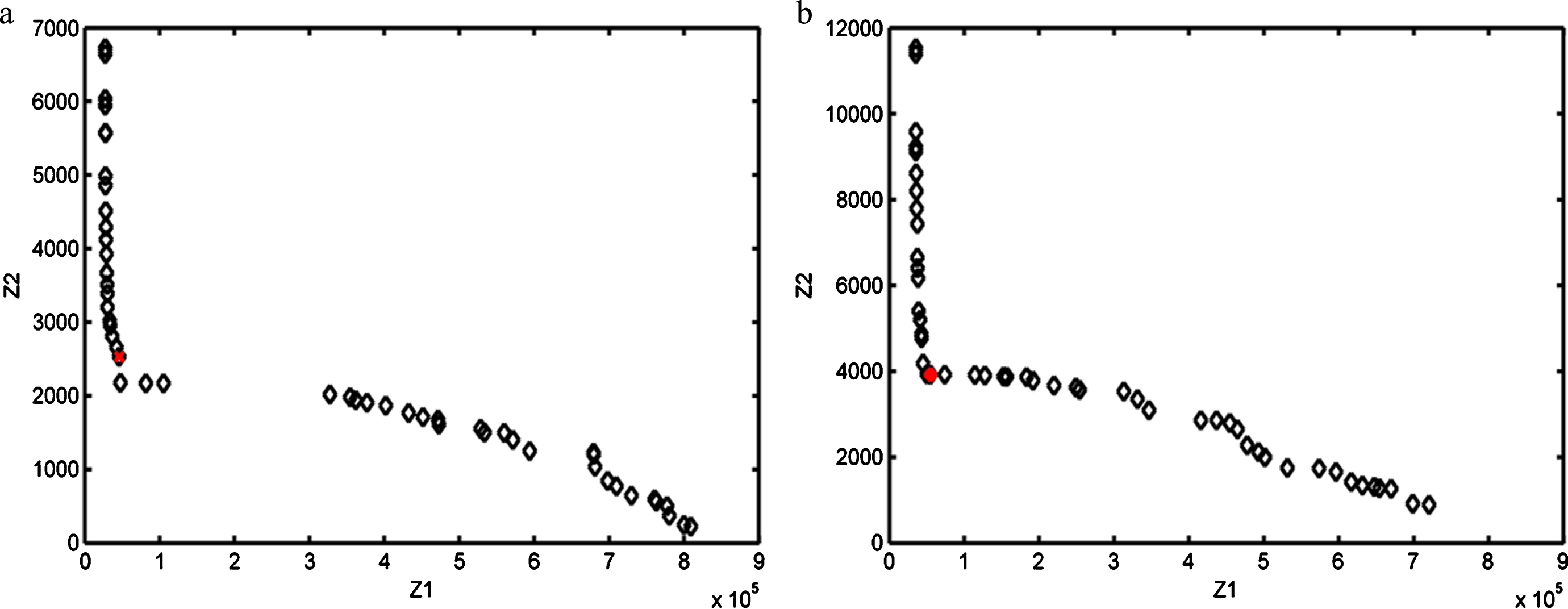
Pareto front for (a) 2DOF FOPID (b) 2DOF PID controllers.
NSGA-II parameters and search space of controller gains
Optimized parameter values of designed controllers
The tracking response for desired drug concentration at tumor site using the designed controllers is shown in Fig. 5. The performance comparison of controllers is made on the basis of number of cancer cells and normal cell population remaining at the end of treatment. After 84 days of treatment the number of cancer cells remaining for 2DOF FOPID is 0.41, with 2DOF PID it is 0.58 whereas 1.21 for PID. The number of normal cells at the end of treatment for 2DOF FOPID is 2.23*108, for 2DOF PID is 2.08*108, and for PID it is 1.83*108. It is also revealed that normal cell population is greater than 1*108 in each case which signifies minimum toxic side-effects and good physiological condition of patient.
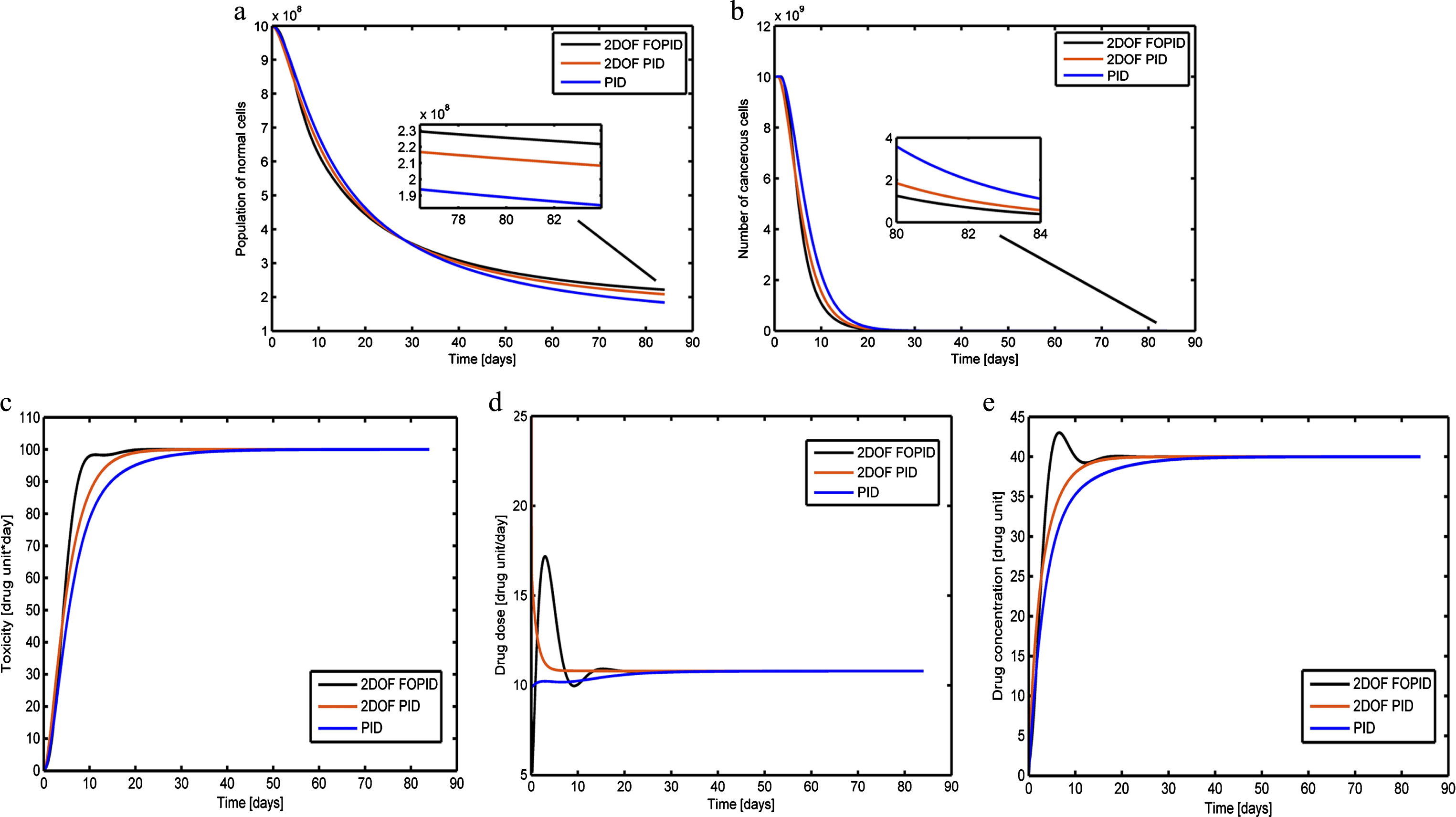
Performance comparison of designed controllers (a) No. of normal cells (b) No. of cancer cells (c) Toxicity level (d) Drug Dose (e) Drug concentration at tumor site.
Various performance measures obtained using designed controllers are listed in Table 4. The peak toxicity level, average drug dosages and concentration level at tumor site are within the specified limits. It is observed that 2DOF FOPID has minimum peak toxicity level and hence brings about minimum harm to patient’s health. 2DOF FOPID provides efficient control because the first term in control action takes into account the error in toxicity level and drug concentration. Whereas the second term in control action considers the actual output as both the pattern & magnitude of drug concentration are crucial for maximum cell killing. It is thus revealed that 2DOF FOPID controller achieves maximum reduction in cancer cells with minimum harm to normal cell, thus performs better as compared to other techniques.
Performance measures for drug scheduling by various controllers
The proposed controllers are designed for a patient specific model and effect of chemotherapy on it. However practically it is difficult to model the tumor growth due to various approximations and different physiological conditions of patient. Thus a control strategy must be capable enough to deal with parametric variations in model and produce desired response. Therefore important parameters in tumor growth and drug response model are perturbed from their nominal values. The parameters considered for the purpose are ρ, k, γ, δ, k1 and η. The number of cancer cells and normal cells at the end of treatment cycle for each case of uncertainty are recorded in Table 5. The quantitative comparison for designed controllers for different cases of uncertainty is depicted in Fig. 6. It is observed from the table that number of cancer cells is low for 2DOF FOPID as compared to other designed controllers. On other hand number of normal cells is higher for 2DOF FOPID in each case of uncertainty. Thus, proposed 2DOF FOPID controller is capable of handling parametric uncertainty more effectively as compared to 2DOF PID and PID.
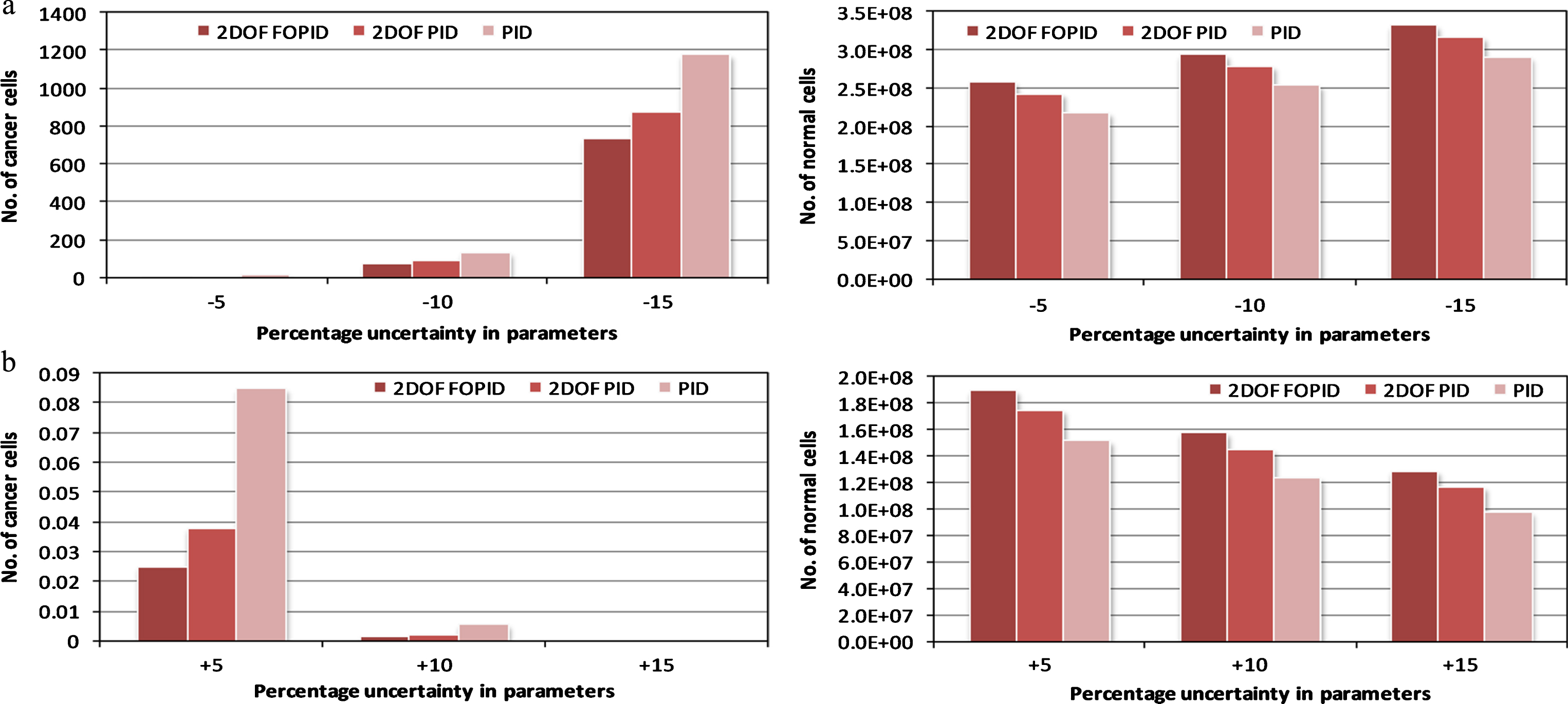
Quantitative comparison of cancer and normal cells for designed controllers (a) Decrease in parameter values (b) Increase in parameter values.
Number of cancer cells and normal cells remaining at the end of treatment with parametric uncertainty
A robust controller also has the ability to reject the effects of disturbance and achieve the desired response. In case of cancer chemotherapy, drugs are generally infused in patient body through infusion pumps which utilize dc servomotors. Although highly efficient motors are available now-a-days, these motors are still susceptible to sinusoidal disturbances of low frequency due to cogging and eccentricity [33]. Therefore disturbance is added in drug dosage of patient model during 45 to 55 days to test the efficiency of proposed controllers under such adverse conditions. Different cases are considered by varying the frequency of disturbance from 5 rad/sec to 20 rad/sec at an interval of 5. It is found that during each case of disturbance no significant change in number of cancer cells is observed but peak toxicity level changes. Table 6 shows the record of peak toxicity level obtained by various controllers for all cases of disturbance. It is obvious from the results that even in the presence of disturbance in drug dosages, the 2DOF FOPID controller is capable of limiting the toxicity below threshold level hence avoiding any harm to patient’s physiological condition. Figure 7 shows regulation of toxicity in the presence of disturbance by various controllers.
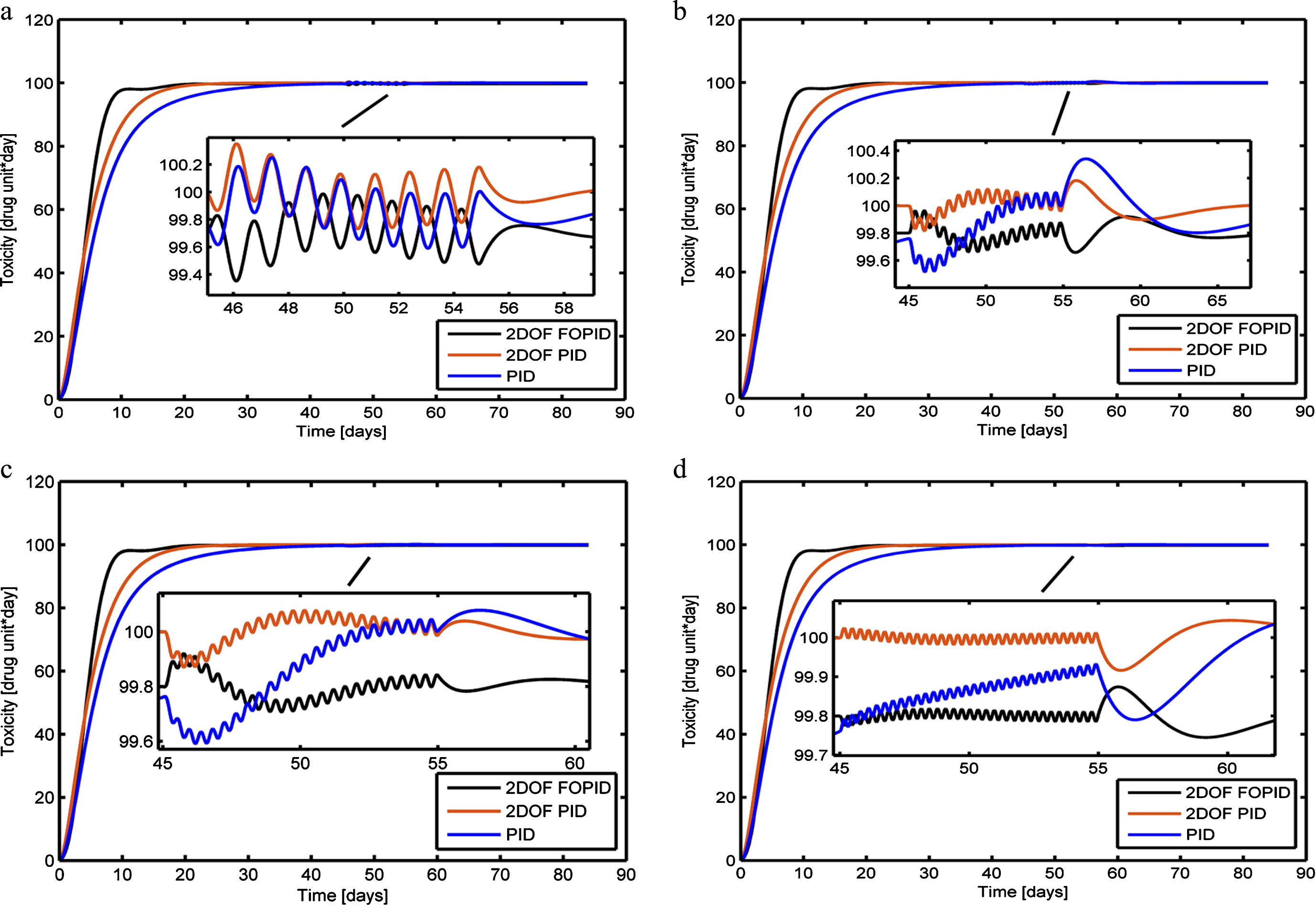
Regulation of toxicity by designed controllers for disturbance of (a) 5sin5t (b) 5sin10t (c) 5sin15t (d) 5sin20t.
Peak toxicity level during treatment in presence of disturbances
Hence it can be perceived from the above analysis that proposed NSGA-II tuned 2DOF FOPID controllers performs better for optimal drug scheduling of cancer chemotherapy as compared to 2DOF PID and PID techniques.
In this article, a closed loop control strategy for optimal drug scheduling of cancer chemotherapy is proposed. A 2DOF FOPID controller for drug regulation and toxicity control is designed. 2DOF PID and PID controllers are also designed for comparative analysis. Multi-objective optimization technique NSGA-II is employed for tuning of designed 2DOF FOPID and 2DOF PID controllers. The 2DOF FOPID controller achieves maximum cancer cell killing with minimum harm to normal cells while satisfying the constraints on cumulative toxicity and drug concentration at tumor site. The presented 2DOF FOPID control scheme also performs better in the instances of disturbance in input drug dose and uncertainty in system parameters. Hence it is concluded that optimal 2DOF FOPID controller provides highly efficient and robust control for drug scheduling in chemotherapeutic treatment of cancer. Further, intelligent and hybrid techniques may be designed in future so as to deal with problems regarding accurate mathematical model of chemotherapy treatment.