
Abstract
Tuberculosis (TB) bacteria may develop resistance to the drugs, which are used in TB treatment. Multidrug-resistant TB (MDR-TB) is a type of TB that does not respond to at least rifampicin and isoniazid, the 2 most powerful anti-TB drugs. MDR-TB requires a more compelling treatment and it is more difficult to diagnose. The experience of physician is the key factor in the success of MDR-TB diagnose. The existence of TB bacteria in the body can be observed relatively faster with a standard sputum smear however, drug-susceptibility tests require nearly 45 days. To cope with this infectious disease, it is vital to estimate the resistance in a newly diagnosed TB patient to plan the initialization of the treatment in the testing period. Herein, the purpose of this study is to build a framework and establish a mathematical model that will help decision makers (physicians) while estimating the risk of multidrug resistance when a new tuberculosis patient arrives, using intuitionistic fuzzy cognitive maps (IFCM). Intuitionistic fuzzy sets are utilized to reflect the decision makers’ hesitancy degrees in the model.
Keywords
Introduction
Tuberculosis (TB) is a global burden and one of the leading causes of morbidity and mortality [46]. It is one of the top 10 causes of death worldwide. TB is known for centuries, has a vaccine, also a standard treatment that takes six months. The medicine solved the problem of TB decades ago by finding the cure; it is not a problem of medicine anymore, it is a problem of management. TB is not just a disease, but also an issue of social inequality and poverty. Contagiousness and mismanagement of TB treatment are the most important reasons why MDR-TB is continuously emerging and spreading around the world. Utilization of incorrect or low quality medications, poor healthcare conditions, poor quality of life, and dropping the treatment prematurely may lead to drug resistance, which is transmitted especially in crowded areas as hospitals and prisons.
MDR-TB is a type of TB that does not respond to the two most powerful first-line anti-TB drugs: rifampicin and isoniazid. MDR-TB can be treated with second-line TB drugs with an extensive treatment up to two years. About 480,000 people worldwide developed MDR-TB in 2015 [46]. When a new TB case is diagnosed, it is vital to capture the drug resistance risk. This study is a risk assessment model for MDR-TB using IFCM which is an effective decision-making tool in medical problems considering the hesitation degrees of decision makers.
The aim of the study is to determine the factors that are important for the development of resistance in TB and establish a framework that will form the basis of subsequent statistical research in Turkey as recently driven in Ethiopia [22] and India [5]. Today, the factors that play a role in the occurrence of MDR-TB are known as basic concepts, however due to the lack of statistical data, the contribution of these factors to the development of resistance cannot be measured. After a patient is diagnosed with TB, a number of drug-susceptibility tests are performed to determine whether it is TB or MDR-TB and the test results are completed in approximately 45 days. Since the prevalence of TB is higher than the prevalence of MDR-TB, standard TB treatment is given to the patient during this process. If the patient is MDR-TB, it is a waste of time and also an unnecessary load of chemicals to the patient’s body, especially to the liver. The treatment of MDR-TB is longer, and requires more expensive (≥US$ 1000 per person), more toxic drugs and the latest data reported to World Health Organization (WHO) show a treatment success rate for MDR-TB of 55%, globally [48]. Considering that liver health is essential to the effectiveness of the rest of the treatment, it is vital for the patient to quickly predict resistance in a TB patient. This study will be the first step in constructing a decision support system to forecast the resistance status of a TB patient before the drug-susceptibility tests.
The remainder of this paper is as follows: Section 2 summarizes the use of cognitive mapping in medical decision making and explains IFCM method in detail. Section 3 shows the numerical application of IFCM. Section 4 observes the system in different scenarios and Section 5 concludes the study.
Cognitive mapping in medicine and IFCM method
Cognitive mapping in medical decisions
Cognitive mapping (CM) is a structuring tool, which can be used for a better understanding of complex systems. It constructs a conceptual map of the system that already exists in the expert’s mind. In the last two decades, CM has been widely used in medical decision-making especially accompanied by fuzzy logic. Since medical decisions involve vagueness, ambiguity, and fuzziness, Fuzzy Cognitive Map (FCM) and its extensions as IFCM are used in detection, diagnosis and treatment planning as listed in Table 1.
The applications of FCM in the recent literature
The applications of FCM in the recent literature
In 2005, CM is used for important communication skills that physicians need over the course of caring for a person with cancer [6]. In 2008, CM is applied for reshaping the diagnostic process and improving the management of digital imaging [27]. Lastly, in 2010, CM is used again for medical diagnosis support [18]. Apart from these, conventional CM has not been used in the last five years in medical problems.
FCM is proposed by Kosko [25] as an expert-based and causal methodology aiming to structure complex decision systems. FCM is a directed graph with nodes as system concepts and edges as causal relations. Each concept represents a variable / a factor of the system and each arrow represents the cause-and-effect relationship between two concepts.
Let C i and C j be two different concepts of a system, then the arrow with a direction from C j to C i is called w j i and it shows the degree of causality between C j and C i as shown in Fig. 1. The presence of w j i makes C j and C i the cause variable and the effect variable, respectively. In conventional CM, w j i takes only the crisp values – 1,0 and 1 which represents a decrease, no relation and an increase. In FCM, w j i values can be linguistic terms which are represented by fuzzy sets.
Concept nodes and relation edges of FCM.
In FCM, the final value of each concept in other words, the strength of each variable in the system is calculated with an algorithm of iterative steps using Equation (1) where si (k) is the value of concept i at iteration k, w
j
i is the weight of connection from C
j
to C
i
, si (k + 1) is the value of concept i at iteration k+1, and f is the threshold function.
IFCM [24] is an extension of FCM with Atanassov’s intuitionistic fuzzy sets (IFS) [4]. IFS differ from fuzzy sets with their ability of representing hesitation degrees of decision makers in the mathematical model. IFCM is a relatively new and attractive method with its recently developed versions by integrating TOPSIS [23], by using evidential reasoning [49] and by implementing synergy effect [14].
Let X = {x1, x2, …, x n } be a finite universal set. An IF set A in X is defined as:
A ={ 〈 x l , μ A (x l ) , υ A (x l ) 〉 |x l ∈ X } with the functions;
μ
A
: X → [0, 1] , x
l
∈ X → μ
A
(x
l
) ∈ [0, 1] and
π A (x l ) =1 - μ A (x l ) - υ A (x l ) is Atanassov’s intuitionistic fuzzy index, the degree of indeterminacy membership, of the element x l in the set A and for every x l ∈ X, 0 ≤ π A (x l ) ≤1.
In IFCM method, Equation (1) is updated using IFS hence, in Equation (2) of IFCM, instead of wji, there are two weight values namely the influence weight
TB is an infectious disease caused by the bacillus Mycobacterium tuberculosis. It is one of the top 10 causes of death worldwide and the leading cause from a single infectious agent (above HIV/AIDS) [48]. A preventive treatment is available with vaccination of children with the bacille Calmette-Guérin (BCG). The risk factors of the disease, shown in Fig. 2, are known and investigated continuously in various countries with high TB rates. In the scope of the project “End TB Strategy” of WHO, all TB data is collected from countries (usually by The Health Ministry), driven by WHO, and reported annually as “Global Tuberculosis Report”. In addition, according to the latest research, “Treatment Guidelines” are also prepared and published each year by WHO as a key reference for TB healthcare practitioners, experts, physicians and patients (www.who.int/tb/en).
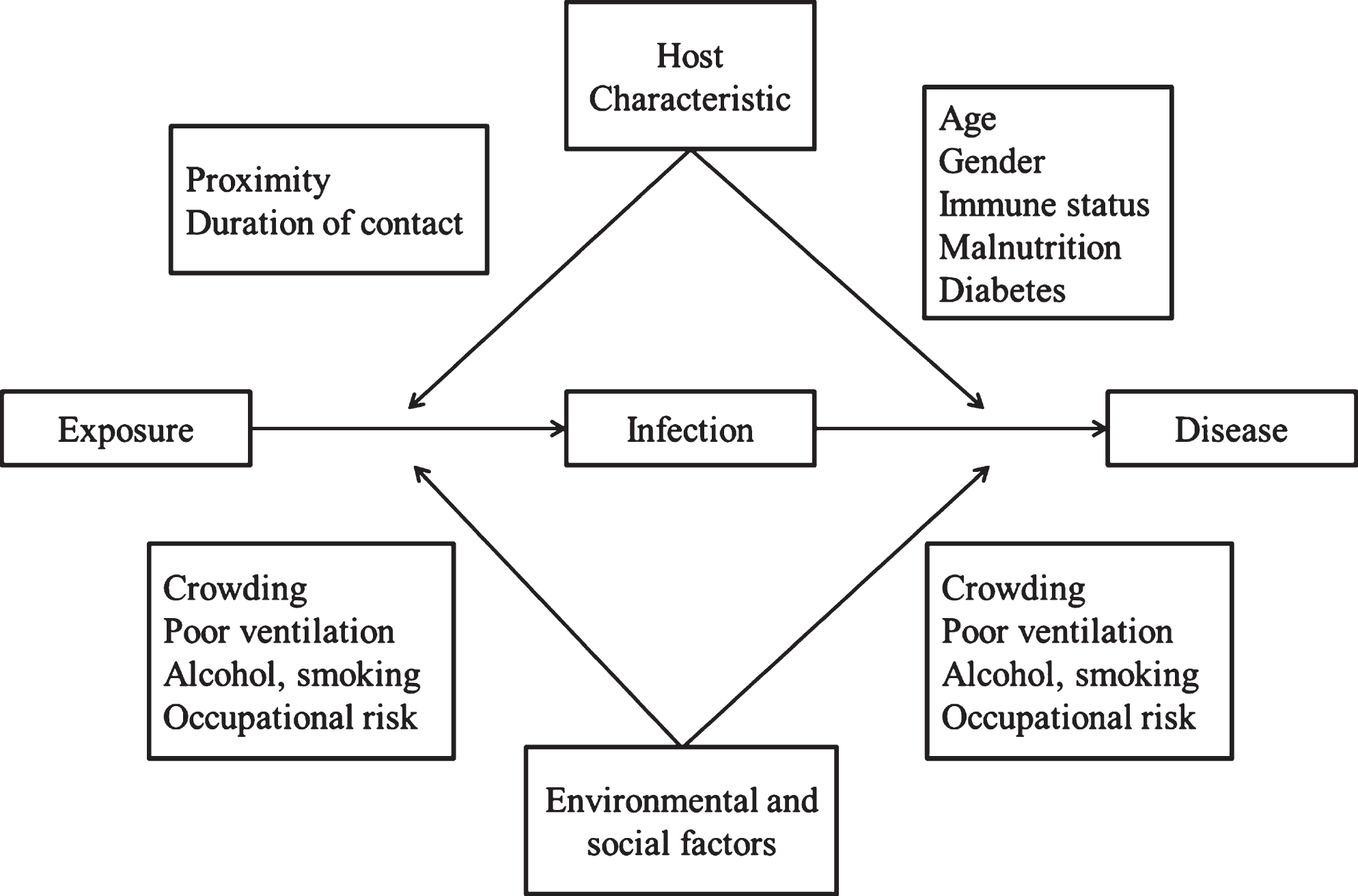
Risk factors of TB [28].
The types of TB are defined by the drug-susceptibility condition of bacteria causing the disease. There are two types of anti-TB drugs that are currently in use: First-line drugs and second-line drugs. The five first-line anti-TB drugs are [47]: Isoniazid (H/Inh) Rifampicin (R/Rif) Pyrazinamide (Z/Pza) Ethambutol (E/Emb) Streptomycin (S/Stm)
The first-line antitubercular drugs provide the most powerful and effective treatment of TB. These are cost-efficient drugs with few side-effects. Drug-susceptible TB has a standard treatment regimen of 6 months with high intensity phase (Inh, Rif, Ebm and Pza) of 2 months and continuity phase (Inh and Rif) of 4 months. Standard regimen has shown high efficacy rates (90% –95%) [41], and low toxicity in TB patients. The second-line antitubercular drugs are shown in Table 2. Groups A, B and C are the core second-line drugs and Group D is additional drugs that cannot be used without core second-line drugs in a treatment plan.
Second-line anti-TB drugs [46]
If the TB bacteria are only resistant to Rifampicin, the type of TB is called Rifampicin Resistant-TB (RR-TB). If the TB bacteria are resistant to Rifampicin and Isoniazid, the two most effective anti-TB drugs, the type of TB is called Multidrug-Resistant TB (MDR-TB). If the TB bacteria have, in addition to MDR-TB, resistance to at least one drug in both of the two most important classes of medicines in an MDR-TB regimen; fluoroquinolones (Group A) and second-line injectable agents (Group B), the type of TB is named as Extensively Drug Resistant TB (XDR-TB). Average treatment success rate of these resistant TB cases is 55% globally [48].
In RR-TB and MDR-TB, recommended treatment is a bundle of five effective TB drugs during the intensive phase: pyrazinamide and four core second-line drugs – one from Group A, one from Group B, and at least two from Group C. If the minimum number of effective drugs cannot be reached as given, one additional drug from Group D2 and other drugs from Group D3 is included to bring the total to five [46]. Recommended total treatment duration is 18 months and more, up to two years. In XDR-TB, according to drug-susceptibility test results of the bacteria, the most effective treatment bundle is constructed by using the drugs to which the bacteria are not resistant. High-dose of first line drugs can be used also when there is no other chance of completing the treatment bundle.
A patient with tuberculosis may have resistance in two main ways; by contacting a resistant TB patient (i.e. Primary Resistance) or by failing in the previous TB treatment (i.e. Secondary Resistance). Globally, 3.5% of new TB cases and 18% of previously treated cases have MDR/XDR/RR-TB [48]. If a patient has the history of previous TB treatment, it is relatively uncomplicated to foresee the current drug-resistance pattern since the drugs of the previous treatment are known. However, the diagnosis of primary resistant TB is highly challenging. Considering the primary resistant cases are only 3.5% of the total, until the drug-susceptibility test results are ready (in nearly 45 days), all new TB cases start with the standard TB treatment regimen. If the patient has primary resistance in the test results, the treatment is re-organized using second-line drugs and the patient returns to the beginning with 45 days of loss and a fatigued liver.
Determining the risk factors of resistance development in a TB patient is important to detect a patient with primary resistance without waiting for the results of the drug-susceptibility test. When the risk factors are detected, a decision support system can be constructed as a predictive model.
In order to assess the risk of multidrug resistance, the factors that influence the resistance development are determined. These factors are not the risk factors of being infected with TB, but the risk factors of having primary resistance in a newly diagnosed TB patient. First, an in-depth literature research is conducted to find all the risk factors that have been investigated previously, and then three chest diseases experts are interviewed, risk factors are classified and defined. Nine factors are determined as system concepts: Age [10, 43]: The patient’s age in years. The resistance is more likely to develop in younger ages. Substandard housing conditions [1, 16]: Substandard means homelessness, excessive household crowding etc. Housing conditions can be related to strength of immune system. BMI [10, 16]: Low Body-Mass Index represents potential risk for many diseases. History of MDR-TB Exposure [21, 40]: MDR-TB is reported as an infectious disease. Presence of comorbidities [7, 44]: All comorbid diseases as diabetes, hypertension etc., especially HIV, is associated with TB resistance risk. Previous use of TB antibiotics [7]: There exist the risk of resistance development for each antibiotic previously used. Being an immigrant [15]: Migration represent many risks like low income, poor health-care, etc. History of imprisonment [1, 40]: Prisons are dangerous in terms of infectious diseases. History of travel to high-risk country [13]: The 30 high MDR-TB burden countries are determined by WHO [45] to provide a focus for global action on the MDR-TB crisis in the countries where progress is most needed. The 20 countries with the highest estimated numbers of incident MDR-TB cases are: Bangladesh, China, DPR Korea, DR Congo, Ethiopia, India, Kazakhstan, Kenya, Indonesia, Mozambique, Myanmar, Nigeria, Pakistan, Philippines, Russian Federation, South Africa, Thailand, Ukraine, Uzbekistan, and Viet Nam. The additional 10 countries by estimated rate per 100 000 population and with a minimum number of 1000 cases per year are: Angola, Azerbaijan, Belarus, Kyrgyzstan, Papua New Guinea, Peru, Republic of Moldova, Somalia, Tajikistan, and Zimbabwe.
Numerical application
To obtain a conceptual map of the system and calculate the final values of the factors, three chest disease specialists of Yedikule Chest Diseases and Thoracic Surgery Training and Research Hospital are interviewed. Relation and hesitation matrices of each expert are constructed as 9×9 matrices for pair-wise causal relations between each of the 9 concepts.
4 questions are asked to decision makers to define each causal relationship: With respect to resistance development in a TB patient, does a positive change in Concept 1 create a change in Concept 2? (Yes or No) Is this change positive or negative? What is the strength of this change? (Low, Fair, High, Very High) How much hesitation do you have on this information that you give? (Low, Fair, High, Very High)
The first three questions are common with FCM. In IFCM, an additional question is asked in order to represent hesitation degrees of the decision makers in the model.
Relation and hesitation degrees of Decision Maker 1 are given in Table 3. The diagonal elements of the matrix is zero, by definition, to avoid creating reinforce loops in the algorithm. For example, Decision Maker 1 responded that, a positive change in Age creates a positively fair change in Substandard Housing Conditions with respect to resistance development in a TB patient, and that she has high level of hesitation on this information. Linguistic terms of decision makers’ responses are represented with intuitionistic fuzzy scales given in Figs. 3 and 4.
Relation and hesitation degrees matrix of Decision Maker 1 (NVH: Negatively Very High, NH: Negatively High, NF: Negatively Fair, NL: Negatively Low, Z: Zero, PL: Positively Low, PF: Positively Fair, PH: Positively High, PVH: Positively Very High)
Relation and hesitation degrees matrix of Decision Maker 1 (NVH: Negatively Very High, NH: Negatively High, NF: Negatively Fair, NL: Negatively Low, Z: Zero, PL: Positively Low, PF: Positively Fair, PH: Positively High, PVH: Positively Very High)
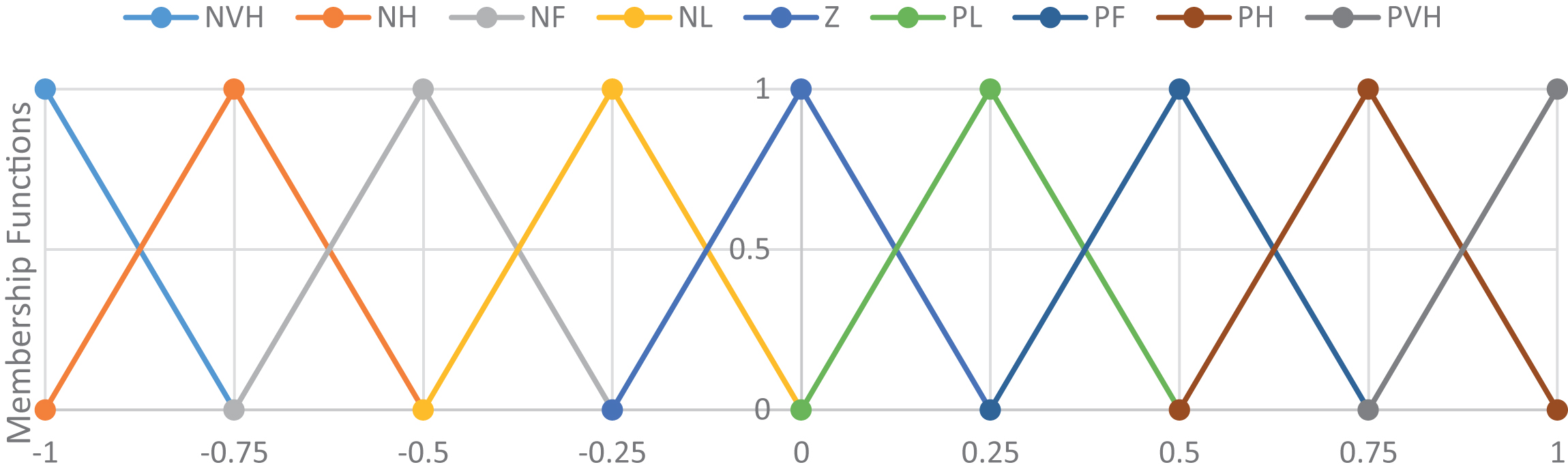
Linguistic variables of relation degrees (NVH: Negatively Very High, NH: Negatively High, NF: Negatively Fair, NL: Negatively Low, Z: Zero, PL: Positively Low, PF: Positively Fair, PH: Positively High, PVH: Positively Very High).
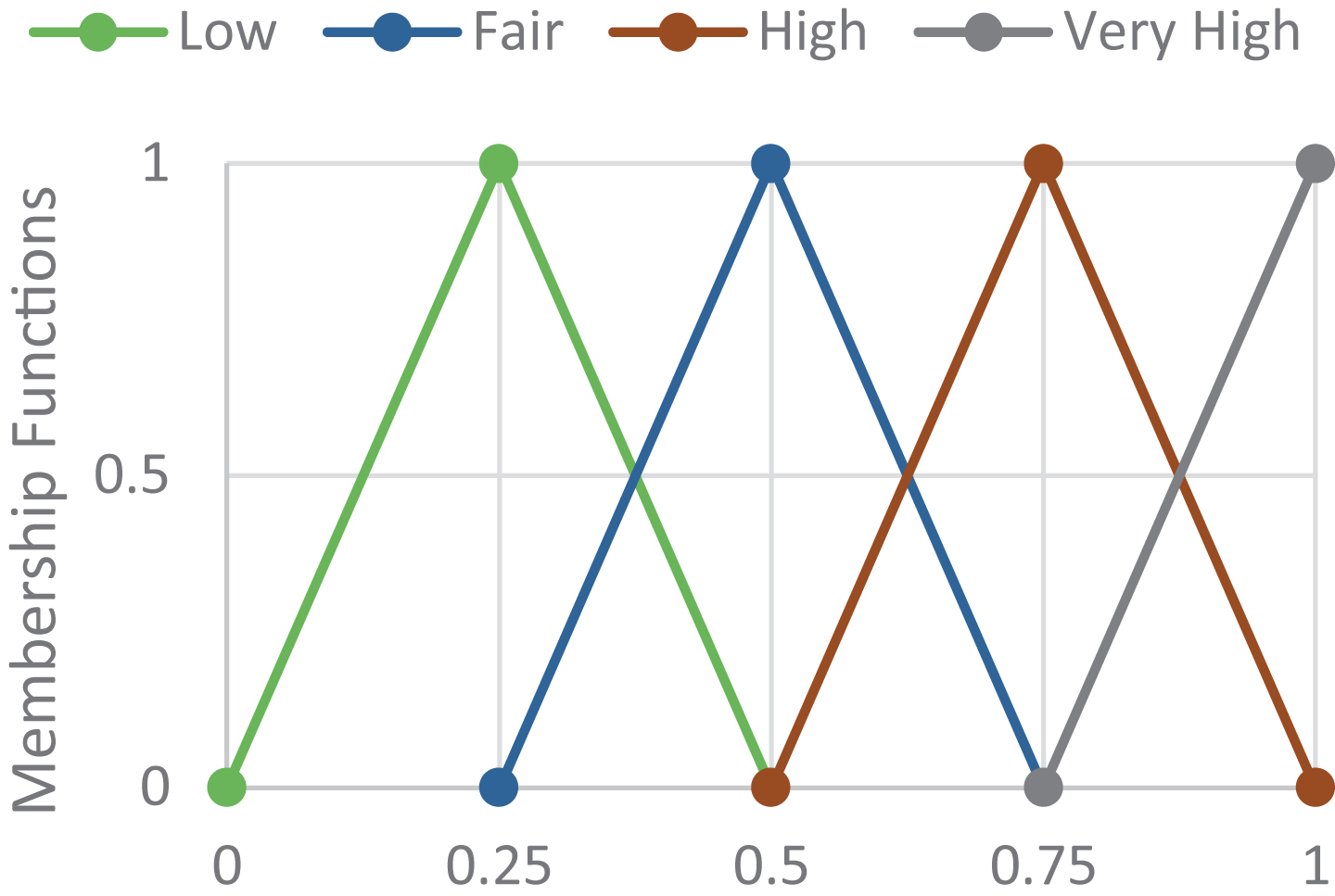
Linguistic variables of hesitation degrees.
Three relation matrices and three hesitation matrices of three decision makers (DMs) are aggregated and defuzzified using max aggregation and centroid defuzzification methods. For example for the row “Age” and the column “BMI”, DMs responses are: DM1: Positively Fair Relation, Fair Hesitation DM2: Positively Fair Relation, Fair Hesitation DM3: Positively Low Relation, High Hesitation
The aggregated and defuzzified relation and hesitation values for the causal relationship of these two factors are 0.3750 and 0.6250, respectively.
For the row “Immig.” and the column “BMI”, DMs responses are: DM1: Negatively Fair Relation, Low Hesitation DM2: Negatively Low Relation, Fair Hesitation DM3: Negatively High Relation, Low Hesitation
The aggregated and defuzzified relation and hesitation values for the causal relationship of these two factors are – 0.5000 and 0.3750, respectively. Hence, the influence weight and hesitancy weight matrices are obtained with aggregated and defuzzified values.
The weights of the map are calculated considering the concept weights defined in Equation (2) as
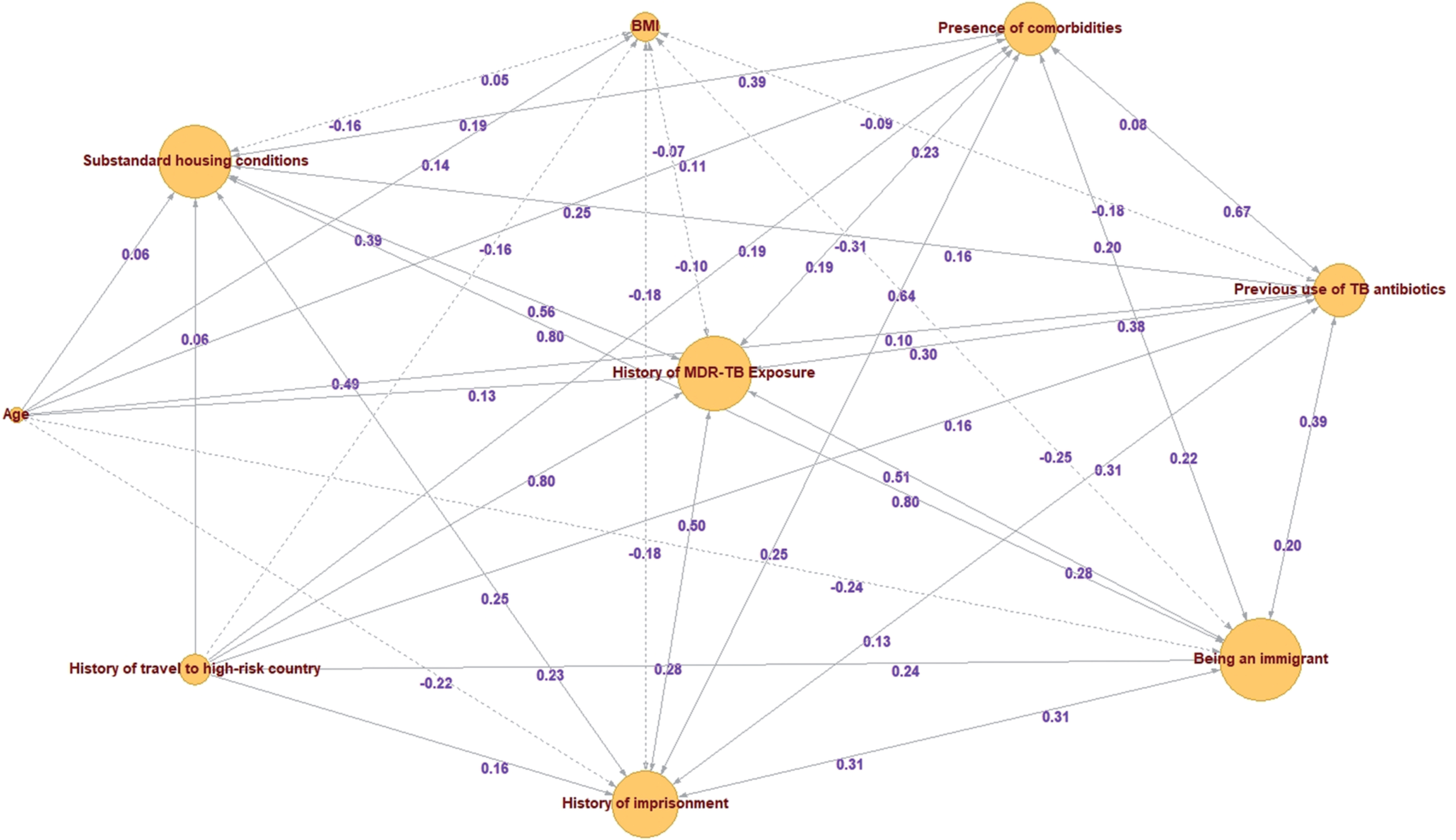
IFCM of MDR-TB risk factors.
Outdegree, indegree and centrality values of the concepts
Briefly, in directed graphs, indegree is the number of arrows arriving to the node, outdegree is the number of those departing from the node, and centrality is the total number of edges that a node possesses. Centrality can be interpreted as the popularity of a concept in the system. In Fig. 5, the sizes of concept nodes are adjusted by their centrality degrees.
“Being an immigrant” has the greatest centrality degree, 5.29, which shows that it is the most interacting node with other system concepts. Migration is one of the most important factors in the spread of infectious diseases. Migration brings poor living conditions and puts immigrants in a vulnerable position in terms of contagious diseases. Migration creates every kind of reason that will expose a person to the infection by weakening his/her immune system. In this respect, it is expected that this factor has the highest centrality in this system.
“Age” has the lowest centrality degree, 0.99. It is mostly because its indegree equals to zero, by definition. “Age” is a scale variable that only changes with time. None of the factors in the system can make any change to the age of a person. “Age” is a transmitter variable in the system that affects other concepts but not affected by them. It is predictable that the factor “Age” has a low degree of popularity in the network because of its constant increase in years.
Centrality degree should not be confused with node influence in the network. Centrality is calculated using influence weights and hesitancy weights of the edges. However, node influences are calculated using Equation (2) and the weights of the edges. It is an iterative process which is terminated by the convergence of final values of all the nodes in the system.
For the iterations, the initial state vector is chosen as the vector of ones, assuming each concept is on-state in the system, which means all the factors are equally active in the initial state of the network. The threshold function is chosen as tanh(x) providing an output interval of [–1, 1], which allows to observe positive and negative effects of the factors in the resistance development system. All the iterations are operated using MATLAB Software and the final values are converged in 20 iterations, as shown in Table 5 with the ranking order of absolute values.
Final values of the concepts and the ranking order
“History of MDR-TB Exposure” has the greatest final value, and hence the greatest influence in the resistance development system. MDR-TB exposure means that the body recognizes resistant bacteria. If the body’s immunity is powerful when exposure occurs, resistant bacteria are inactivated in the lung but not excreted. Resistant bacteria may remain in the lung for many years asleep. When the immunity of the body, especially of the lungs, decreases due to weight loss, stress, pneumonia etc. these bacteria become active and start to multiply. Thus, if a patient with TB diagnosis has previously encountered resistant bacteria, it is highly likely to be MDR-TB. It is the most influencing factor of the resistance. However, it is challenging to determine the occurrence of MDR-TB exposure if the patient has not exact information on a MDR-TB infected relative, colleague or acquaintance. In tuberculosis disease, a contact is defined as breathing the same air in a closed area for a long time with an active, infected and non-treated patient. If the patient does not reveal his/her condition, it is not possible to notice the exposure in the daily life. Since tuberculosis is an infectious disease, patients tend to hide their medical condition at work in order not to lose their jobs. According to chest disease specialists, if a TB patient knows exactly an acquaintance previously infected with MDR-TB, they usually have similar resistance conditions. If there is not a known case, then it is unlikely to estimate whether there is history of MDR-TB exposure or not. It is the most effective factor in the system and also the most problematic to determine. On the other hand, it creates a critical advantage in estimating the resistance pattern, if there is a pre-determined case of exposure.
“Substandard housing conditions” has the second greatest influence in the system because it gathers many components that might weaken the immune system. Substandard housing conditions represent homelessness, excessive household crowding, lack of heating system, coldness, humidity, lack of hygiene and poverty. Homelessness, where housing conditions are considered the worst, makes a person vulnerable to all kind of diseases. In addition, homeless people are more likely to drink alcohol to stay warm outside, which yields more serious problems as comorbid diseases by damaging the liver. Excessive household crowding increases the likelihood of disease transmission and decreases hygiene. Lack of heating system and humidity creates an environment that allows the bacteria to multiply easily. And poverty is usually the essential reason for not reaching proper healthcare. “Substandard housing conditions” has an extensive influence in the system by depressing the immune system and also it is very simple to detect. The presence of this factor might be an advantage for the physician in predicting resistance with its power in the system and its simplicity in detection.
“Previous use of TB antibiotics” has the third rank of influence. Some of anti-TB drugs are commonly used is the treatment of other lung diseases, especially in chronic and recurrent pneumonia. There is a probability of resistance development in the body, for each type of antibiotic previously used. Hence, if the patient has a history of treatment of a lung disease with TB antibiotics in his/her medical records, then the physician considers the probability of resistance to that group of antibiotics. Previous use of TB antibiotics is vital information for the TB patient’s resistance pattern. Since antibiotics are not sold without prescription, the patients usually have the list of previously used antibiotics in their medical records. The existence of this factor in a patient is relatively effortless to notice.
“Being an immigrant”, “presence of comorbidities” and “history of imprisonment” are following factors by means of influence. These three factors have relatively more indirect effects than the first group of three factors. Being an immigrant increases the probability of having substandard housing conditions. Presence of comorbidities, especially HIV, weakens the immune system of the body. History of imprisonment provides an environment for MDR-TB exposure. The effects of these three factors are less direct in the resistance development system however, they should not be eliminated from the conceptual map because their final values are greater than 0.98. An indirect effect is still an effect.
“BMI” is the only factor that has negative effect on resistance development. As the BMI falls below normal values, the body’s immunity decreases, which makes the person vulnerable to development of resistance. In other words, when the BMI is reduced, the probability of resistance development increases. This situation creates an opposite influence of BMI in the system. The negative final value of BMI is a marker of the reliability of the numerical application.
“Travel to high risk country” is also related to the most influencing factor, MDR-TB exposure. Since it does not guarantee the occurrence of exposure, it has a smaller influence in the system.
“Age” has the smallest influence. 0.2616 is not a negligible value however it is relatively very small when compared to other factors of the system. If the aim is to conduct a new statistical study with these factors, the presence of “Age” factor can be questioned.
Scenario analysis is one of the most important advantages of cognitive mapping methods. Once the map is constructed and the final values are calculated, one or more concepts can be set as off-state (to the value zero) to observe the rest of the system. Setting a concept as off-state can be interpreted as elimination of the factor from the system by cancelling its influence. If only one factor is set as off-state, more information about the system can be obtained by examining how the final values of the remaining factors change. Scenario analysis allows decision makers to ask “What if?” questions about the system.
Scenario analyses in this study are performed using FCMapper software which is an Excel based mapping & modelling program freely available online at www.fcmappers.net.
Since “Age” has the smallest influence in the system, the first scenario is on its elimination from the map. Changes in other factors are shown in Table 6.
Changes of Scenario 1 (1:Strong, 2:Medium, 3:Weak, 4:Very Weak)
Changes of Scenario 1 (1:Strong, 2:Medium, 3:Weak, 4:Very Weak)
According to Table 6, none of the factors showed a strong change after the elimination of “Age”. The factors which have interactions with “Age” have lost little influence which the others have gained. “History of imprisonment” and “BMI” had positive medium change in their influence. “Age” has more effect on other factors than “History of imprisonment”, therefore it gains most of the power that the others factors lose by interacting with “Age”. “BMI” gains importance because “Age” and “BMI” change in parallel direction in time. With elimination of “Age”, “BMI” gains power because it starts to represent two of them together. However, apart from these minor changes, the ranking order of the final values did not change. Hence according to Scenario 1, the elimination of the factor “Age” does not affect the system significantly.
What if the most influencing factor in the system is eliminated? This question is important for the chest disease specialists because in addition to resistance development, this factor has a certain influence on other factors too. Which one of the remaining factors will gain or lose power is valuable to understand the system thoroughly. Table 7 shows the changes in other factors in the absence of “History of MDR-TB Exposure”
Changes of Scenario 2 (1:Strong, 2:Medium, 3:Weak, 4:Very Weak)
When “History of MDR-TB Exposure” is off-state, all the other factors lose power with mostly strong and medium strength. Being exposed to resistant bacteria means the body can recognize and reproduce resistance, hence it is a pillar of the resistance development system. It is a reinforcing concept. In its absence, the ranking order of the remaining concepts does not change however their final values decrease dramatically.
Apart from elimination of the concepts, cognitive mapping allows for the individual analysis of each patient’s condition in medical decision making. For example, if a patient claims that he/she has never used any of the anti-TB drugs and has never been in prison, these two factors can be set as off-state and the most influencing factors for this patient can be determined for a customized treatment planning. Scenarios 3 and 4 are two examples based on previous patient stories given by chest disease specialists.
For the patients in Scenarios 3 and 4, the final values and the ranking orders of the remaining concepts are given in Table 8. At first glance, it is observed that final values of the concepts are smaller than those given in Table 5. The factors of the system empower each other. When some of the factors are eliminated, the influence of the other factors on resistance development decreases.
Final values of the concepts and the ranking order
The most noticeable change in Scenario 3 is that “MDR-TB Exp.” has regressed to second rank. The eliminated factors in Scenario 3 are all the most affecting factors of “MDR-TB Exp.”. In their absence, “MDR-TB Exp.” loses its power on the resistance development system and “Prev. use of TB anti.” becomes stronger. Hence for the patients with these conditions, “Prev. use of TB anti.” might be the reason of having primary resistance. The drugs previously used, should not be included in the new treatment.
In Scenario 4, “MDR-TB Exp” is still the most influencing factor however its final value is decreased. The patient in Scenario 4 is more difficult to diagnose than the patient in Scenario 3 because of the difficulty in determining the occurrence of exposure in a patient’s life.
Tuberculosis is a growing problem of the world, especially with increasing rates of antibiotic resistance. There are two types of resistance in TB: primary resistance and secondary resistance. Primary resistance is developed by contacting an active, non-treated and resistant TB patient. Secondary resistance is developed by failing in a previous TB treatment. Diagnosing primary resistance in a new TB patient, which is only 3.5% of the total, is difficult for the physicians. The problem challenges are (i) the time required by the drug-susceptibility tests, (ii) the minority of the primary resistant cases, and (iii) the lack of certain information on the patients’ previous exposure to the resistant bacteria. In this study, an intuitionistic fuzzy cognitive map model is suggested as a decision support system in order to assess the risk factors of primary resistance in a newly diagnosed TB patient.
By means of an in-depth literature survey and many interviews with three chest disease specialists, 9 factors are determined and defined as the concepts of resistance development system: Age, substandard housing conditions, BMI, history of MDR-TB exposure, presence of comorbidities, previous use of TB antibiotics, being an immigrant, history of imprisonment and history of travel to high risk country. Using linguistic terms, the relation and hesitation degrees of the causal relationships among these concepts are identified by the decision makers. The degrees are represented by Atanassov’s intuitionistic fuzzy numbers in the numerical application and three matrices are formed for three decision makers. For each element of the matrix, in other words for each causal relationship, the relation and hesitation degrees are aggregated and defuzzified. A conceptual map of the resistance development system is obtained. To find the influences of the concepts, the iterative procedure of IFCM is initiated and the final values of the concepts are calculated. History of MDR-TB exposure, substandard housing conditions, and previous use of TB antibiotics had the greatest influence values in the system.
The IFCM method is chosen in this study because it is a structuring tool which has previously shown successful applications in complex systems and it is highly useful in putting the information that exists in human brain on paper. The decision makers not only reflect their experience on the system but also they can express their hesitations on the information that they give. Especially in medical decision making, the physicians are used to work with statistical information. Since no data is required in IFCM, the physicians feel more comfortable when hesitation degrees are considered in the model.
The IFCM method is advantageous in structuring human knowledge however its limitations are twofold; it is subjective and its results cannot be validated if it remains at this stage. Statistical data should be collected in order to demonstrate the influences of the factors and to construct predictive models.
When the results are discussed with the decision makers, they stated their total agreement with the results. The final values and the ranking order were expected however the ability of analyzing new scenarios for each patient was unexpected. They pointed out the usefulness of the model in daily decisions of newly diagnosed TB patients. Therefore, the contributions of this study can be summarized as A decision support framework is constructed for the risk assessment of MDR-TB cases, The risk factors of primary resistance in TB patients are determined and evaluated in different scenarios, The usefulness of the IFCM method in medical decision-making is indicated.
Cognitive mapping is extended using intuitionistic fuzzy sets in this study to give the decision makers the flexibility of expressing their hesitations on the information that they give. In the literature, there exist various techniques featuring hesitation degrees as hesitant fuzzy sets, interval-valued fuzzy sets, pythagorean fuzzy sets, neutrosophic fuzzy sets etc. The future research directions are the use of cognitive mapping with these sets and the use of other IFCM extensions with temporal parameters and integrated techniques.
Footnotes
Acknowledgments
The authors would like to thank to chest disease specialists, Assoc. Prof. Gülfidan Aras MD and Tuğba Mandal MD, who contributed the study with their valuable expertise. This study is supported by Galatasaray University Research Fund.