
Abstract
Computerized Cognitive Training (CCT) contents used to improve patients’ cognitive ability with Mild Cognitive Impairment (MCI) can provide customized training through individual data collection and analysis. However, studies on transfer effect of improving other untrained cognitive domains while performing the contents are insufficient. The present paper intended to collect literature published by PubMed, EMBASE, Cochrane Library, and Web of Science until December 2019 and analyze the trends of CCT and the transfer effect in each training area. Studies on CCT (82/891) have been increasing each year, and universities (60/82) in the United States (17/82) have published the most. In the literature that reported clinical effect (18/82), the cognitive domain mostly studied was memory (14/18), and the N-Back (3/14) method accounted for most of the training contents. Moreover, the contents that showed the highest degree, closeness, and betweenness centrality (BC) indices were the memory area, and video accounted for the highest among the intervention methods. In particular, the closeness centrality (CC) index of the memory and attention contents showed similar results. It can be interpreted that the possibility of the transfer effect occurring from memory and attention areas is the highest since the semantic distance (i.e. the similarity of the training process) between the attention contents and memory contents was the closest. The effectiveness of the actual transfer effect between the memory and attention should be verified.
Introduction
According to World Population Prospects (United Nations, 2019), one in six people in the world is 65 years or older, and the world population is becoming more aged [1]. Furthermore, among the people 65 years or older, about 15–20% has the symptom of Mild Cognitive Impairment (MCI), and about 15% of them are known to develop dementia [2, 3]. It was predicted that delaying the progression of MCI to dementia by two years can reduce the global incidence rate by 22.8 million cases and thus relieve the economic burden on individuals, families, and societies [4]. MCI is generally caused by decreased cognitive abilities, such as memory, judgment, concentration, and attention, due to aging. It is reported that accurate and appropriate diagnosis and treatment can minimize the damage of the cognitive functions [5]. Treatment of MCI is divided into pharmacological and non-pharmacological methods depending on the drugs administered. Although studies have reported that pharmacological medication alleviates dementia patients’ symptoms, it is known that there is no effect of delaying progression from MCI symptoms to dementia [6]. Cholinesterase is generally used to delay the progression of MCI symptoms to dementia; however, on the other hand, non-pharmacological methods and training have gained broad interest because the high risk of clinical trials’ adverse effects can be eliminated through such approaches [7].
Non-pharmacological methods include cognitive stimulation, cognitive rehabilitation, and cognitive training. They differ in the manner of intervention as the strategy to achieve the goal [8]. Cognitive rehabilitation requires development of a strategy or external auxiliary device to compensate for functional difficulties, while cognitive stimulation uses a series of activities and discussions with the goal of general improvement of the cognitive functions. Moreover, the intervention based on cognitive stimulation and cognitive rehabilitation focuses more on the individuals with dementia to improve the general quality of life by overcoming specific difficulties in their daily living [9]. Since cognitive training is applicable to patients with no cognitive or functional difficulties, it is more appropriate for patients with MCI. The goal of cognitive training is to improve the cognitive ability in a specific area through repetitive learning on designed technique and strategy [10]. The cognitive process is known to occur through the activation of neurons related to brain regions biologically activated during the calculation and processing of specific stimuli from the external environment. In recent years, the distributed and overlapping control architecture in which each brain area that controls cognitive function is in overlapping structures rather than functioning separately and efficiently activates cognitive functions through interaction has been reported. Research on the connectome that analyzes brain connectivity from the viewpoint that cognitive functions execute through complex connections between brain regions of the brain is also actively ongoing [11]. Therefore, to improve cognitive ability, it is very important to use an effective and appropriate intervention strategy and manner according to the patient’s conditions.
Several studies are ongoing on improving cognitive function by using a variety of information technologies, including virtual reality, interactive video gaming, and mobile technology, as intervention manner for cognitive training [12]. Among these technologies, computerized cognitive training (CCT) relies on computers or tablet PCs as the intervention means and thus differs from the conventional face-to-face cognitive training that uses paper and pencil [13]. CCT has the advantage of providing objective data collection and real-time feedback since the cost and time efficiency, accessibility, and training content and difficulties can be specified for each user [14, 15].
Although studies have reported the trend of intervention manners and verifying the effectiveness of CCT through meta-analysis of existing studies [16–18], there are no studies to-date on the analysis of transfer effect of CCT to other cognitive domains. For example, the study by Hill, Nicole TM, et al. (2017) [19] on the effectiveness of CCT discussed the meta-analysis and contents used for each of the various cognitive domains but did not analyze the association between the cognitive domains. Moreover, it has been reported that CCT is not effective on dementia patients, but there is no report that included the relevant data and reason. In another study, Zając-Lamparska, Ludmiła, et al. (2019) [20] performed meta-analysis on the efficacy of cognitive mediation using virtual reality but limited the intervention manner to virtual reality to possibly constrain the scope of studying CCT. Therefore, this study limited participants to patients with MCI based on the study results showing that CCT was not effective in dementia patients. However, it did not limit the computerized tools used by studies to analyze computer tools’ diversity. Literatures published until December 2019 were collected and analyzed for trends by year, journal characteristics, and national trends of the main author and examined the transfer effect of computerized cognitive training contents by using a text network algorithm. While performing cognitive training, the patient trains one or two specific cognitive domains, and there is a possibility of transfer effects in which the cognitive ability of untrained areas is improved due to the adaptive manner [21]. Therefore, this study aimed to analyze the overall trend of CCT and whether the content of CCT targeting a specific cognitive domain is effective in other cognitive areas due to the transfer effect.
Methods and materials
Searching strategy
This study used four databases, viz. PubMed (NCBI), EMBASE, Cochrane Library, and Web of Science, to gather literature and analyzed the published study results up to December 2019. The literature collection used the search strategy by four types: study type, participant type, intervention type, and result measurement type. Three researchers independently reviewed and discussed the collected papers based on whether they should be included in or excluded from this study, and the contents for the study were extracted accordingly.
Inclusion & exclusion criteria
Keywords & study selection
Table 1 lists the keywords used for literature search categorized by each type according to the inclusion and exclusion criteria.
Searching of keywords
Searching of keywords
A total of 888 papers were identified in four databases after the initial literature search, and three additional papers were collected by manually searching for the references in the collected papers related to this study in Google Scholar. Figure 1 shows the literature collection process.
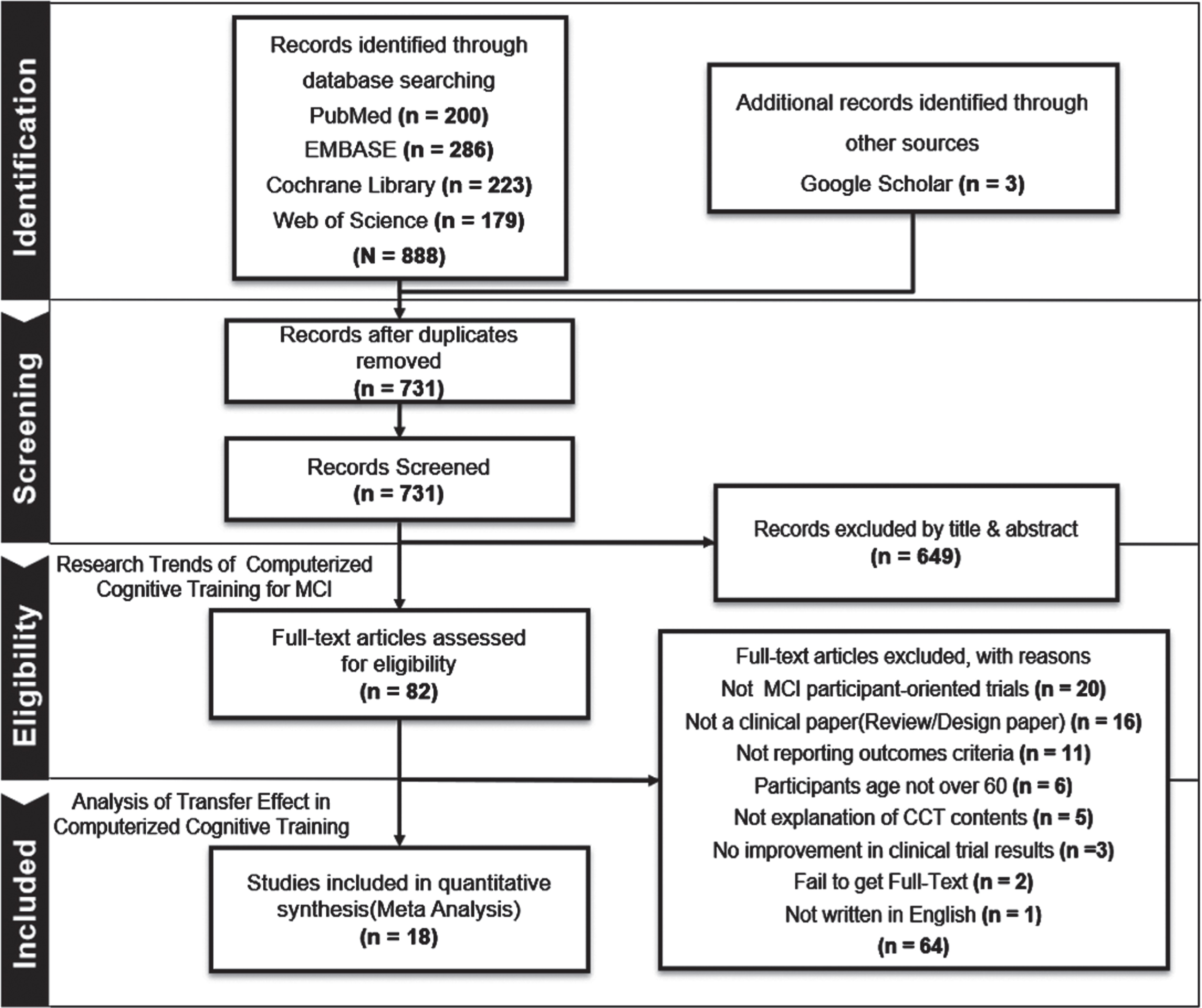
Flow chart of research selection process.
Through the literature identification process, the duplicate papers were removed, while through the eligibility process the subject and abstract were reviewed and those that did not meet the inclusion criteria were removed. In this way, 82 papers were selected via the eligibility process. Those 82 studies used CCT in the treatment of MCI patients. The inclusion process reviewed the main text and removed the papers that did not meet the criteria of the study type, participant type, intervention type, and outcome type. The final 18 papers selected in the inclusion process signified that they used CCT to treat MCI patients and showed positive clinical outcomes. The current study analyzed the trend of CCT using the 82 papers identified via the eligibility process, and performed a meta-analysis using the 18 papers selected through the inclusion process.
Figure 2 shows the 82 papers on the study of CCT for MCI patients selected in the eligibility process and 18 papers on the study with verified clinical effect selected in the inclusion process. They are listed by the published year.
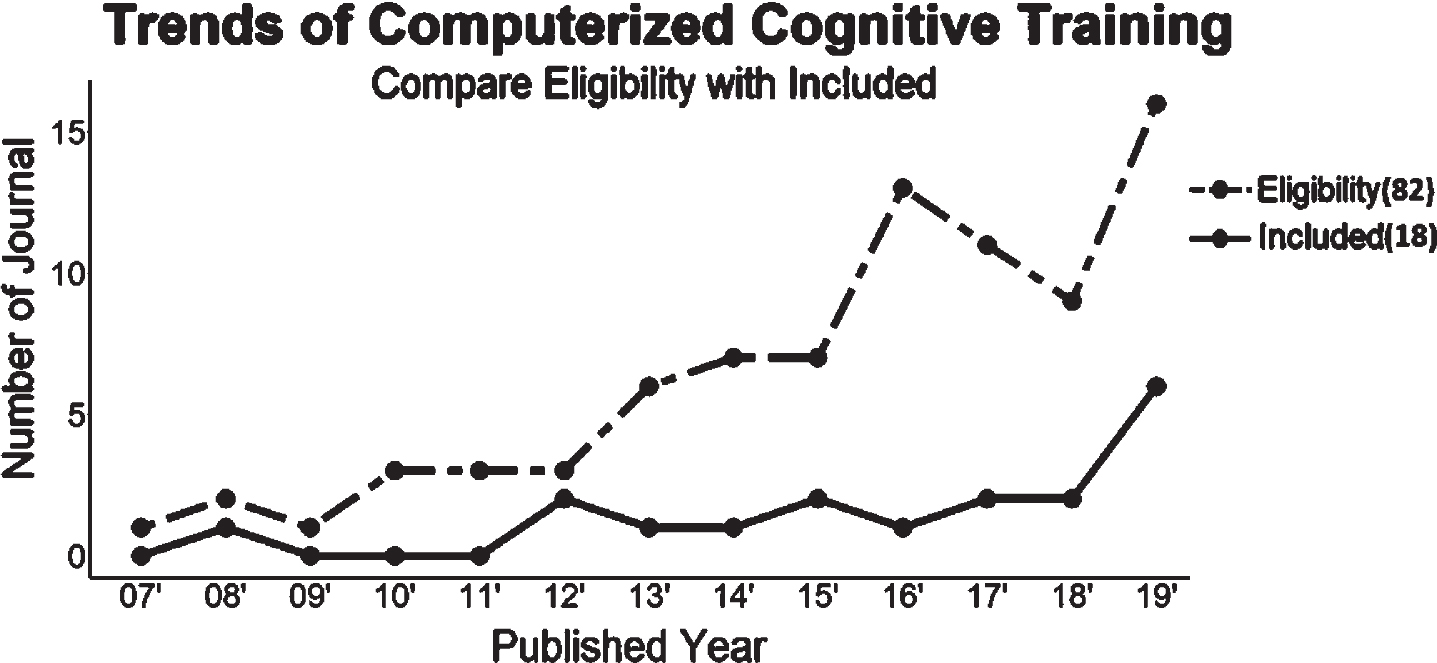
Research trends by year of publication.
The selected 82 papers were all published in journals, and the study type consisted of design, clinical, and review. In the present work, the first identified paper on CCT was the study by Mate-Kole, C. C. et al. (2007) published in 2007, and since then, the interest on CCT is ever increasing. In 2019, in particular, there were 16 studies on CCT, and 6 of them verified the effectiveness of CCT through clinical trials. It showed that the digitalization of cognitive training increased with the advancement of the digital content technology, thereby verifying the effectiveness of CCT. Tables 2 and 3 show the top 10 publishers of papers on the selected 82 CCT cases and the top 10 journals of most cited papers, respectively, for the statistical analysis of journals. Impact Factor (2019), ranked no. 1 in Table 3, scored 7.755 points in the Cochrane database of systematic reviews, and Laver et al. (2017), ranked no. 1 in Table 2 was cited 941 times [28]. In particular, one of the study goals of Laver et al. (2017) was to examine the effect of VR depending on the presence of interventions for global motor function, cognitive function, and activity limitation. The review article analyzed 72 cases of 2,470 stroke patients. Its main result showed that there was a statistically significant difference between the participants when using virtual reality with daily and in ADL also (SMD 0.49, 0.21 to 0.77, 10 studies, 210 participants, low-quality evidence).
Top 10 journals ranked based on the number of publications on this research topic
Top 10 journals ranked based on the number of citations on this research topic
Table 4 lists the countries of the institutions of the principal author of the 82 selected papers to analyze in which countries the studies of CCT are active. In Table 4, if the number of published papers is two or more, the institution that the principal author is affiliated with is categorized, and only the country without the affiliated institution is listed if the number of papers is one. Suppose the institution of the principal author is a college. In that case, it is included in the university category, and the medical institutions, such as hospital, clinical, and rehabilitation center, is included in the medical center category. As Table 4 shows, the United States had the most institutions affiliated with the principal authors, 17 in number, followed by Italy and China, with 6 in number. Of the 82 selected papers on CCT, the universities were the most active institutions, 60 in number, followed by medical centers, 13 in number, and research institutes, 9 in number.
Affiliated country and institution of the first authors
*Notes: Medical center includes hospital, clinical and rehabilitation center; University includes collage; Univ. —university; MC—medical center; RC—research center.
The text network can understand the characteristics of clustered keywords groups through location and relationship analysis using the visual expression of keywords [29]. Network clustering can build networks with various approaches, such as co-citation, bibliographic combination, co-author, and co-word analysis, according to the analysis target and purpose [30]. The analysis based on the simultaneous occurrence of keywords among these network construction methods has an advantage in understanding the conceptual structure and trend of a specific field by measuring the relationship strength between representative keywords in related papers [31, 32]. Therefore, it was used to connect the keywords with edges and links and express the connection relationship between keywords visually. Density, average distance, centrality analysis, and component analysis are widely used to examine the characteristics of connected keywords. The most used index is centrality, which has the advantage of quantifying the frequency and connection strength according to various types of centrality by analyzing keywords that play an important role in the network connection.
This involves text network analysis using Quanteda package of R (version 3.6.2) statistical software to investigate the transfer effect of CCT [33]. The present study calculated the Degree Centrality (DC), Closeness Centrality (CC), and Betweenness Centrality (BC) to analyze the link strength between the keywords [34]. The DC refers to the number of keywords linked with a keyword. A higher centrality indicates that the keyword is linked with many other keywords. The calculation for the DC can be expressed as Equation (1).
Characteristics of included studies
Table 5 shows the number of participants and characteristics of the research methods in the 18 papers needed for the analysis of clinical trials among the collected 82 papers. The number of participants was more than 10. The age of participants in the study by Gagnon et al. (2012) and Ballesteros et al. (2017) was over 60, but the studies did not disclose the number of participants by gender. However, they mentioned that there was no statistical difference between the participants, and we included them in the analysis. The number of participants in the selected papers varied widely from 21 to 271 in number, and there was no statistical difference in gender. There was no restriction on criteria, and the studies used a variety of diagnostic criteria, including Mini-Mental State Examination (MMSE), Montreal cognitive assessment (MOCA), and Saint Louis University Mental Status Exam (SLUMS). In all the studies, the participants had no disease or neurological problem other than MCI and did not take any drug. There were also no clinical ethical problems. The participants had at least six years of education in most of the studies, and the studies stated the selection and study processes. The research design on the selected 18 papers included 14 papers on a randomized single-blinded controlled pilot trial, 2 papers on a single-blinded randomized controlled trial, 1 paper on a randomized controlled pilot trial, and 1 paper on single-blinded randomized controlled pilot trial.
Characteristics of participants and trial design in the included studies
Characteristics of participants and trial design in the included studies
*Notes: RCT—randomized controlled trial; SBRCPT—single-blinded randomized controlled pilot trial; RCPT—randomized controlled pilot trial; SBRCT—single-blinded randomized controlled trial; SD—standard deviation.
Table 6 lists the intervention manner and contents of CCT in the 18 papers that reported the effectiveness of clinical trials. Computer was the most widely used tool for CCT, while video and virtual reality were used as the medium. As Table 6 shows, the comparative experimental studies that used computers and video games together as a training tool accounted for the most, and Nintendo and iPad were used as the media of the video game. All studies stated the process of computerized training to the participants and provided sufficient education and training. The training contents were either available or designed specifically matched with the study objective. Only the studies that reported significant effect of training were included. Memory accounted for most of the cognitive domain targeted by the training, and a variety of contents were performed for it. The most frequent memory training method used by the 18 studies was N-Back, and each study designed their contents based on the different memory areas, viz. occupational memory, short-term memory, and instantaneous memory. Since the lower-level recognition domains were divided according to the cognitive characteristics of the higher-level cognitive domains, the analysis included them in the higher-level cognitive domains of the target cognitive area [35]. The training period varied widely between 1 week and 26 weeks, and most studies compared the participant groups and observed the effect after training of one month or longer. The training on activities of daily living involved activities such as grocery shopping, cooking, and washing, which are routine activities of daily life. All studies performed them in a virtual reality environment. The training was conducted with one or two target cognitive areas to each content, and the training period varied widely between 1 week and 6 months.
Characteristics of CCT contents in the included studies
Characteristics of CCT contents in the included studies
*Notes: CT—computerized cognitive training; ADL—activity of daily living; IT—interventions type; PC—computer; VG—video game; VR—virtual reality; TCA—target cognitive area; M—memory; A—attention, E—executive; LT—Length of Training.
Figure 3 visualizes the text network analysis of digitalization types, training contents, and targeted cognitive domains listed in Table 6. The main keywords in the text network are indicated in bold. Here, CCT_contents were connected to Memory_contents, Attention_contents, executive_contents, and ADL_contents. Separately, the Intention Type (IT) was connected to VR, Computer, and Video, and the Target cognitive domain (TCD) was connected to memory, attention, executive, and ADL. The connecting line between the keywords became thicker as the centrality index became higher, and a thicker line represented a stronger correlation between the keywords.
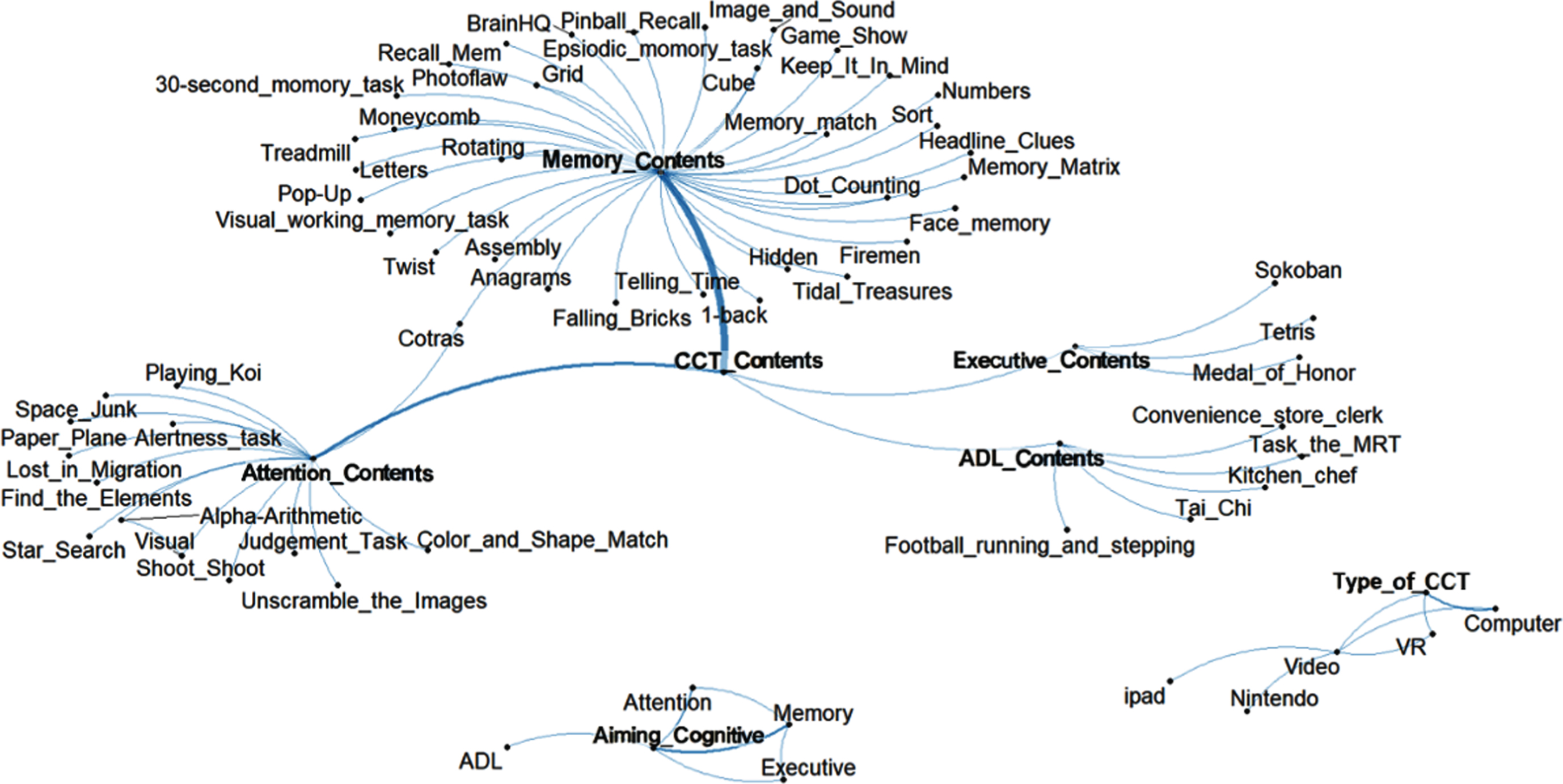
Text network analysis of computerized cognitive training.
Table 7 lists the calculation results of the centrality indices shown in Fig. 3. In the DC index, memory was a CCT content having the highest frequency 33, followed by attention with frequency 16, activities in with frequency 3. Likewise, memory accounted as the largest training target domain with frequency 14, followed by attention with frequency 7, executive ability with frequency 2, and activities in daily living with frequency 1. The indices of the memory contents and the attention contents were relatively high in CC index, indicating that the studies focused more on memory and attention than executive ability and activities of daily living.
Top 10 centrality of keywords
*Notes: CCT—computerized cognitive training; ADL—activity of daily living; TCA—target cognitive area; IT—interventions type. *Notes: DC—degree centrality; CC—closeness centrality; BC—betweenness centrality.
Although the frequency of memory training contents was more than twice that of the attention contents when analyzing only the DC, they showed similar scores of 0.387 and 0.381, respectively, in the CC index. It means that the semantic distance between the memory training contents and attention training contents is short and implied that performing memory training would be effective for the attention domain also. CoTras, which is the training contents targeting memory, is sometimes performed also for attention. However, it is segmented for training of each area and has not been analyzed for transfer effects. In the BC index, the memory training contents were the highest with frequency 64, indicating that it is likely to be used more widely. The BC increases as there are more target cognitive domains of the collected studies and is equal to the number of computerized cognitive training contents if there is only one domain. Moreover, the BC index of the video was higher than the other intervention manners, indicating that many studies tried to verify the effectiveness by comparing video with other intervention manners.
CCT is a method of improving cognitive ability, such as memory, attention, and executive ability, using digital media without intervention of any drugs. It is used to improve the cognitive ability of MCI patients rather than the dementia patients. Most contents of CCT are designed with the expectation of improvement in the cognitive domain targeted by the study. However, there are no studies on the impact of training using the contents designed for the specific study objective on other untrained domain. To investigate the transfer effect of CCT, the current work collected papers that performed CCT and selected the ones that reported clinical effects of performing text network analysis. Out of 888 papers collected initially, 82 were found to study MCI patients’ training for memory, attention, executive ability, and activities in daily living. Out of those 82 papers, 18 papers verified the effectiveness through clinical trials. The 82 selected papers indicated that the number increased each year, beginning with the study by Mate-Kole, C. C. et al. (2007). Mate-Kole’s report showed that studies on efficient training appropriate to patients have steadily increased due to the advancement of digital contents. With 60 out of 82 cases, universities were the most active institutions in studies on CCT, and most of the studies were conducted in the United States.
In the 18 selected papers that reported the clinical effect, the training targeting memory accounted for the most CCT contents with clinical effects. They used computers, video games, and virtual reality environments according to the study objective. Activities of daily living, such as washing, shopping, moving items, and eating, used virtual reality environments to emphasize reality. The studies were mostly designed for randomized controlled trials, and there was no significant statistical difference between the number of participants and gender. The 18 selected papers were investigated for keyword connection related to three-centrality analysis (DC, CC, and BC) and three types (CCT, intervention manner, and training target domain) in the text network. The DC index showed a difference of more than double as there were 33 contents for memory training and 16 contents for attention training, meaning that memory contents were studied more than attention contents. Moreover, it was confirmed that relatively similar scores in CC were derived for the memory and attention domains, 0.387 and 0.381, respectively. It indicates that the two contents’ training processes may be similar and that a transfer effect may appear between the two domains. The attention content generally receives a higher score as more items are processed simultaneously in a shorter period, and the memory content receives a higher score as more items are stored longer in the memory. Therefore, we can consider that the two domains are related because it is necessary to pay more attention to process the items simultaneously in a short period when more items are stored in the memory. In the BC index, the memory contents were the highest with frequency 64, indicating that it is likely to be used more widely. The high BC index of the video game indicated that many studies compared it with other intervention manners (e.g., virtual reality and computer) to verify its effectiveness. However, one of the papers collected for our study reported that the content was effective on memory, but no further studies were done to prove its effectiveness on attention.
As a future work, it is necessary to study on contents that are the most effective in each cognitive domain through effect size analysis of the collected papers, and more samples should be collected to study on domains that showed the transfer effect. They can verify the effectiveness of CCT for treating MCI without using any drug.
Footnotes
Acknowledgments
This work was supported by the National Research Foundation of Korea (NRF-2020R1A2C1011960) grant funded by the Korea government (MSIT), the MSIT (Ministry of Science and ICT), Korea, under the ITRC (Information Technology Research Center) support program (IITP-2020-2018-0-01426) supervised by the IITP (Institute for Information & Communications Technology Planning & Evaluation).