
Abstract
Assessing fetal growth and development requires accurate identification of the fetal area contour and measurement of the Crown-Rump Length (CRL). In this paper, we presented a unique method for autonomously segmenting the fetal region in ultrasound images and calculating the CRL based on the U-Net architecture. Because of its capacity to capture both global and local information, the U-Net model is a popular choice for image segmentation tasks. Our method employs the U-Net model to extract the fetal region contour and measure the CRL, resulting in a dependable and efficient prenatal evaluation solution.
Introduction
Ultrasound imaging is essential in prenatal treatment because it offers important information about the developing fetus. Accurate and automated fetal area segmentation and Crown-Rump Length (CRL) measurement are required for a variety of clinical applications, including gestational age estimate, fetal growth monitoring, and anomaly detection. Manual annotation of fetal features and measurements, on the other hand, is time-consuming and subjective, necessitating the development of efficient and dependable electronic procedures [1, 2]. Deep learning-based techniques have showed encouraging results in medical image segmentation challenges in recent years. With its encoder-decoder structure and skip links, the UNet architecture has emerged as a preferred alternative for precise segmentation [3]. The UNet captures hierarchical features successfully while maintaining fine-grained spatial details, making it suited for fetal region segmentation [4].
This research offers a modified U-Net model for precise fetal area segmentation and Crown-Rump Length (CRL) estimate from ultrasound images. The modified U-Net architecture improves on the original U-Net model by introducing additional convolutional layers and batch normalization, with the goal of improving both segmentation accuracy and predicted boundary quality which illustrated in Fig. 1. The fundamental goal of this study is to solve the difficulties associated with accurate fetal area segmentation and CRL length calculation, such as noise, fetal positional variation, and complicated anatomical components. And to create a reliable and efficient algorithm that can reliably delineate fetal region boundaries and estimate CRL length, allowing for better clinical decision-making.

Block diagram of proposed modified U-Net model segmentation.
To assess the performance of our proposed technique, used a dataset comprised of a wide range of ultrasound images taken at various gestational ages and fetal positions. To measure the accuracy of the segmentation findings, quantitative metrics such as the Dice coefficient, Jaccard index, and Hausdorff distance will be used. In addition, compared this model’s CRL estimations to ground truth measurements with the precision and reliability of our approach. The rest of the paper is structured as follows: Section 2 gives a comprehensive summary of related research and existing methodologies for fetal area segmentation and CRL length estimate. The technique, including the modified U-Net architecture and the training procedure, is described in Section 3. Section 4 offers the experimental results and performance evaluation, and Section 5 discusses them. Finally, Section 6 closes the paper by highlighting our research’s contributions and future directions. Anticipate that the proposed modified UNet model will demonstrate improved accuracy and robustness in fetal region segmentation and CRL length estimation in this study, providing valuable support to clinicians in prenatal care and improving the overall efficiency of fetal ultrasound analysis.
Prenatal healthcare requires accurate segmentation of fetal ultrasound images as well as measurement of the Crown-Rump Length (CRL). Various strategies have been proposed over the years to overcome these difficulties. In this section, will look at some of the recent research on fetal area contour segmentation and CRL length estimation.
The UNet architecture described [5] is a frequently used approach for medical picture segmentation. The UNet model is an encoder-decoder network with skip links that allows for the integration of low-level and high-level data for exact segmentation. This design has demonstrated promising results in a variety of medical imaging applications, including image segmentation of prenatal ultrasounds. Several research have used the UNet model to segment fetal ultrasound images. [6] proposed a modified UNet design with residual connections for fetal head and brain segmentation. The inclusion of residual connections minimizes the vanishing gradient problem and increases segmentation accuracy overall.
[7] suggested a method for estimating fetal CRL that includes fetal ultrasound image segmentation and measuring. Their method extracts the fetal region using a UNet-based segmentation network, followed by CRL length estimation using geometric techniques. Their findings indicated accurate CRL estimation, emphasizing the potential of U Net based methods in fetal biometric measurements. [8] developed a modified UNet with attention gates to segment fetal ultrasound images. The attention gates concentrate interesting regions selectively, improving the model’s capacity to catch small features and segmentation accuracy. investigated various methodologies for fetal area contour segmentation and CRL length estimate. [9] proposed Fetal Ultrasound Image Segmentation with Multi-Scale Fully Convolutional Network a multi-scale fully convolutional network for fetal ultrasound image segmentation. Their network integrates multi-scale features to capture both local and global context, allowing for precise fetal structural segmentation. Furthermore, [10] published Deep Learning for Automatic Fetal Ultrasound Image Analysis in which they described a deep learning-based method for automatic fetal area segmentation. The method captures spatial and temporal connections in fetal ultrasound data using a combination of convolutional neural networks (CNNs) and recurrent neural networks (RNNs), resulting in robust segmentation [11]. While existing research has made important advances to fetal area contour segmentation and CRL length estimate, difficulties such as occlusion, image artifacts, and fetal posture variability remain. To overcome these issues, presented a modified UNet architecture with extra features and architectural advancements suited specifically for accurate fetal area contour segmentation and CRL length estimate. The next section describes our suggested modified U-Net architecture, emphasizing the changes and enhancements made to improve the accuracy and robustness of fetal area contour segmentation and CRL length estimate.
Methodology
Modified U-Net architecture has been designed to improve the accuracy and robustness of fetal area contour segmentation and Crown-Rump Length (CRL) estimate. The changes and enhancements made attempt to solve issues including occlusion, image artifacts, and variability in fetal positions. Our modified U-Net architecture expands on the original U-Net concept by incorporating an encoder-decoder network with skip links. However, to make many crucial changes to improve segmentation performance. To collect both local and global information, incorporated multi-scale context modeling into the U-Net architecture [12]. In particular, this model used dilated convolutions in several layers to expand the receptive field and allow the model to catch more contextual information. This improves the model’s ability to handle fetal size changes and accommodate varied anatomical components.
During the segmentation phase, applied attention methods to selectively emphasize informative regions. The model concentrates on relevant regions while suppressing noise and irrelevant information by assigning higher weights to salient features. This attention mechanism improves segmentation accuracy, especially in difficult circumstances with delicate structures or occlusions. In this model employed residual connections between the encoder and decoder paths to improve information flow and address the vanishing gradient problem. These connections enable the model to better maintain and transfer information across levels of abstraction, allowing for more accurate segmentation [13]. To normalize the feature maps, added batch normalization layers after each convolutional layer. By lowering internal covariate shift, this method helps to stabilize and expedite the training process, resulting in faster convergence and enhanced segmentation performance. In this model used a number of data augmentation strategies to improve the model’s robustness and generalization. Random rotations, translations, scaling, and flipping of the input images, as well as elastic deformations, are among the techniques used. Data augmentation reduces overfitting and increases the model’s capacity to manage a wide range of fetal ultrasound variations.
Our proposed modified U-Net architecture intends to improve the accuracy and robustness of fetal area contour segmentation and CRL length estimation by incorporating these enhancements. These enhancements allow for more precise delineation of fetal features, especially in difficult settings involving occlusions, image artifacts, and fetal posture fluctuations.
Dataset
Collected 1129 two-dimensional ultrasound images of fetal from the database of Mediscan Systems, chennai, India. The size of ultrasound images is (800 * 600).
Data augmentation
For data augmentation transformed each image by horizontal and vertical flipping, width and height shifting with a range of 0.1, shearing 0.1, and also applied Zoom range of 0.1, fill mode. Generated 9032 augmented ultrasound images in total from the augmentation.
Methodology
There are numerous image segmentation networks that use attention processes to increase segmentation accuracy, which enhance the representational accuracy of neural networks by extracting important information relevant to their task and have shown promising advancements. To address the issue of inconsistent features between classes, [14] the discriminative feature network (DFN) included modules such as channel attention and global average pooling. [15] presented a squeeze- and-excitation block (SE) attention module that automatically calculates the weight of each feature channel. Furthermore, it merged features from different phases and improved feature representation. An attention gate and readjusted the encoder’s output features were successfully applied to segmentation before splicing the image features generated by convolution of the encoder with the equivalent features in the decoder [16].
Intend to use a modified U-Net architecture to perform fetal contour segmentation and crown-rump length (CRL) measurement in this paper. The U-Net is a well-known deep learning model that is commonly used for image segmentation tasks. Improved the U-Net model’s performance by incorporating both channel attention and spatial attention mechanisms illustrated in Fig. 2. The U-Net design is made up of an encoder-decoder structure connected by skip links. The encoder extracts high-level characteristics from the input image, which are then up-sampled by the decoder to produce the segmentation mask. Skip connections allow encoder information to travel straight to related decoder layers, assisting in the recovery of fine details.

Architecture of Proposed Modified U-Net Model.
The channel attention mechanism works to prioritize informative channels while suppressing irrelevant ones. It is divided into two stages feature map reduction and feature map augmentation [17]. The reduction step reduces channel dimensionality with 1 × 1 convolutional layers, while the enhancement stage generates channel-wise attention weights with sigmoid activation [18]. Element-by-element multiplication with the original feature map improves informative channels while suppressing less significant ones illustrated in Fig. 3. In this channel attention mechanism the input feature map for channel mechanism, let it say be I
c
, initially the mechanism aggregates the dimensionality of a input feature map by using both max-pooling and average-pooling which generates the descriptors like I
avg
and I
max
for both average pooling and max pooling respectively. Then both the descriptors are applied to shared network FC to produce the Channel attention map O
c
. Channel and spatial attention mechanism.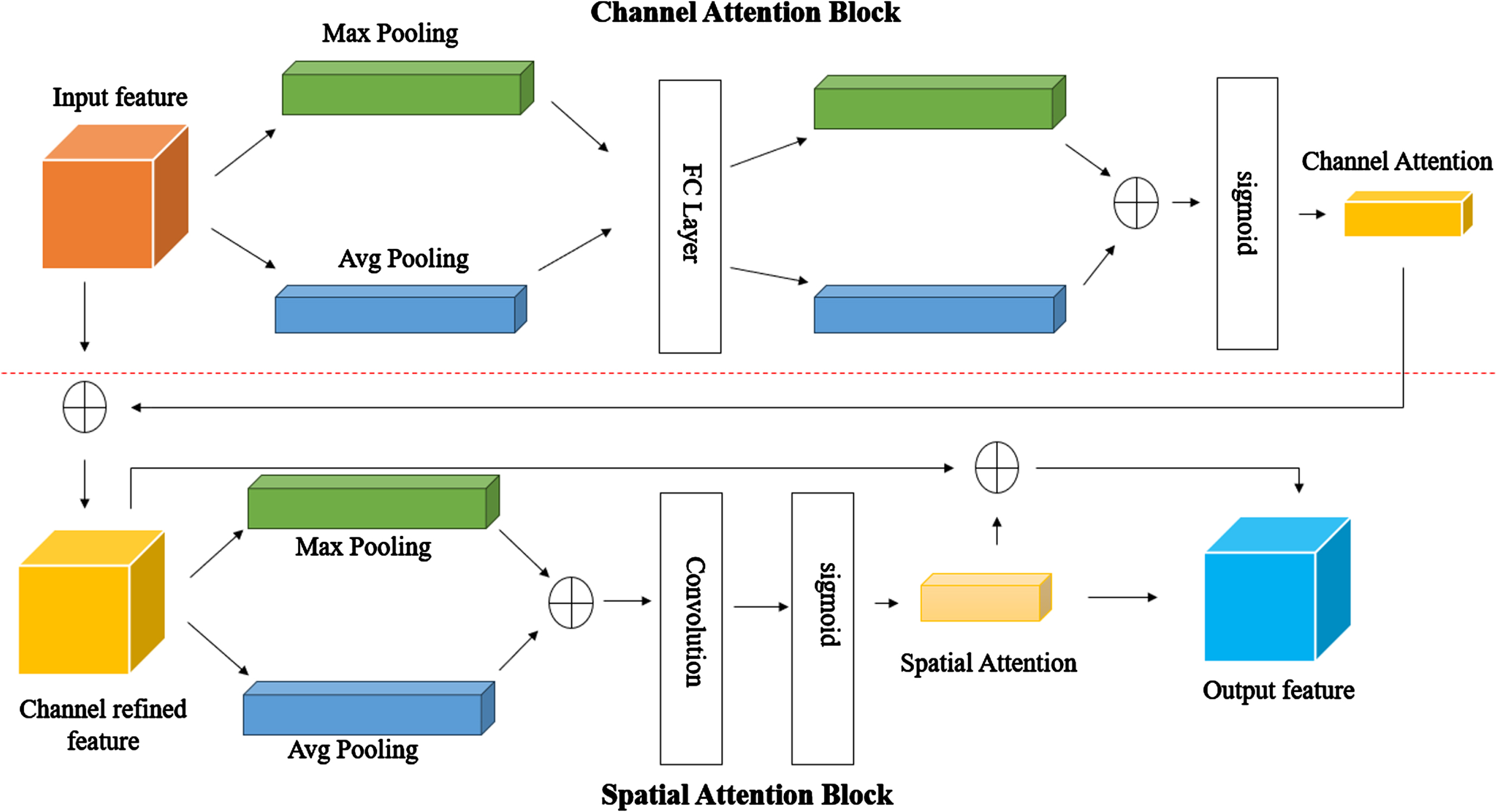
The channel attention technique is used in the U-Net model’s encoder blocks. It enables the model to concentrate on relevant feature channels at each encoding stage, resulting in improved feature representation [19]. The spatial attention mechanism is also applied to the skip connections, assisting the decoder in attending to critical spatial regions and refining the segmentation mask [20].
This model uses a set of fetal ultrasound images paired with manually annotated fetal area contours to train the U-Net algorithm. The dataset is separated into two parts: training and validation. To train the model, the modified U-Net, used Binary Cross-entropy loss and Mean Intersection over Union (IoU) as assessment metrics. Data augmentation approaches during training to improve the model’s generalization capability. And also used L2 regularization on the convolutional layers to prevent overfitting. ReduceLROnPlateau callback to reduce teh learning rate if the validation loss plateaus which helps the model to converge better during training. Performed hyperparameter tuning as grid search by iterating over the different learning rates and dropout rates. Batch normalization also applied for faster convergence and better generalization.
Inference and CRL calculation
In this paper applied the trained U-Net model on unprocessed ultrasound images after training to obtain the segmentation mask representing the fetal region. The segmentation mask is refined and any artifacts are removed once it has been processed and then estimated the CRL using contour information by measuring the maximum distance between contour points which indicates the CRL length.
Experimental results & discussion
On a diverse dataset of fetal ultrasound images, assessed the performance of our suggested technique. Metrics such as IoU, Dice coefficient, and pixel-level accuracy are used to assess segmentation accuracy. The accuracy of CRL estimation is determined by comparing the calculated CRL values to the ground truth measurements achieved through expert annotations. In this experiment compared the fetal contour and estimation of CRl length uisng U-Net with the Modified U-Net proposed method. Figure 4 Illustrates the Resultant Image using U Net with integrated Channel and Spatial Attention Mechanisms which shows Input Image with predicted regions and Fetus region.
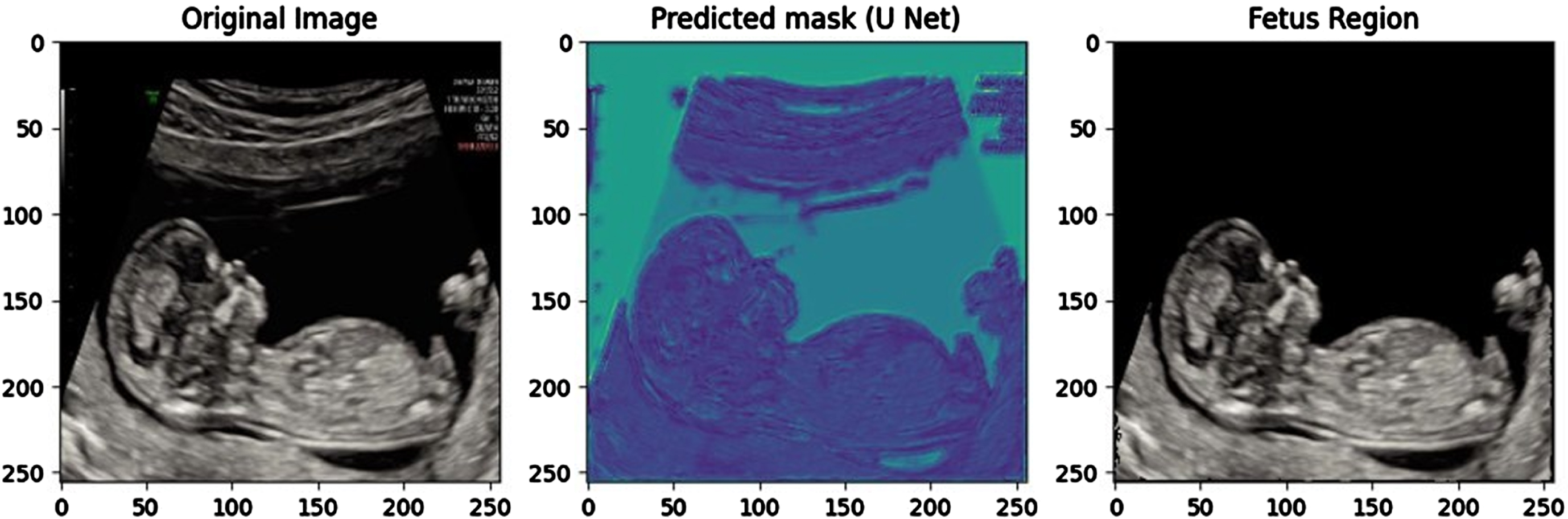
Resultant Input Image, Predicted Regions and Fetus region using Proposed method.
Figure 5 shows Fetus mask, Fetus Contour and CRL estimation using proposed U-Net with Integration of channel & spatial attention mechanisms. The proposed method identifies the fetal contour and estimated the CRL value as 8.77 cm.
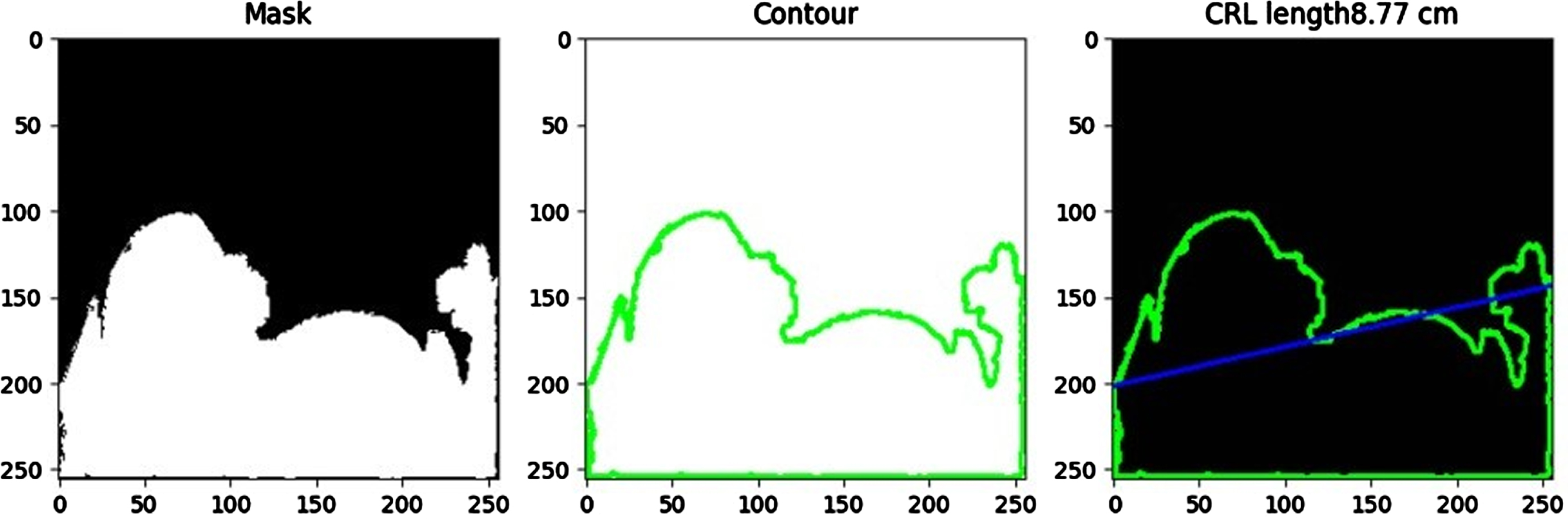
Resultant mask, fetus contour and estimation of CRL length using proposed method.
In this paper evaluated the performance of our proposed approach on a diverse dataset of fetal ultrasound images. To evaluate segmentation accuracy, metrics such as IoU, Dice coefficient, and pixel-level accuracy are used. By using this approach achieved an Accuracy of 77.9 with Dice Coefficient and IoU are 0.50 & 0.33 respectively, which illustrated in Fig. 6. CRL estimation accuracy is measured by comparing calculated CRL values to ground truth measurements obtained through expert annotations.

Performance metrics of proposed method.
This paper provide a novel approach for recognizing the fetal area contour and computing the CRL using the U-Net model in this work. Our technique shows promising results in accurately segmenting the fetal region and determining the CRL, making it a useful tool for prenatal evaluation. Our approach’s automated nature decreases inter-observer variability and increases efficiency in clinical settings. Further study could concentrate on expanding the proposed system to Increase the accuracy of fetal contour detection and to handle more fetal biometry measurements incorporating sophisticated anomaly identification algorithms.
Footnotes
Acknowledgments
This study was supported by funding from the Indian Council of Medical Research (ICMR) under grant AI-Adhoc/03/2022-AI Cell.