
Abstract
In this paper, a bi-objective mixed-integer linear programming model is constructed to manage the pharmaceutical supply chain of a hospital. The proposed model aims to concurrently reduce the overall cost of obtaining drugs from several vendors and choose the best suitable source. The suggested model takes into account supplier distance, inventory management, and multi-product and multi-period. The major assumptions of the proposed model are product storage for future periods of decreased demand and supplier capacity. The results indicate that the ideal approach can minimize hospital supply and pharmaceutical planning expenses. The Best-Worst and TOPSIS methods determine which pharmaceutical supplier should be selected for future orders. The suggested model identifies human resource capability as an essential factor that might significantly affect the system’s total cost. The results of applying the model and the sensitivity analysis validate the efficacy and validity of the suggested mathematical model and solution strategy.
Introduction
The importance of the Pharma Supply Chain (PSC) has become clear to researchers. Recently many studies have been done on different aspects of PSC. Supply Chain Management compass remarkable percentage of hospital expenditures [1–4]. Drugs account for about 30 per cent of Global Health Spending [5]. The PSC faces uncertainty that sometimes makes a difference from other supply chains. Demand for certain medications may increase because of atmospheric conditions [6, 7]. This paper aims to reduce the costs of health care without damage to customer service. The medicines must be available at a scheduled time. The results of surveys show that the distribution strategies are the reason for a 13 per cent lack of inventory causes [8]. A shortage of drugs may lead to financial loss and dangerous problems for the patient. Unfortunately, dissipation in health care systems is more than in other systems. A standardized process can mitigate wasting, and establishing Cooperation between the elements of this system can lead to more efficiency. The efficient PSC cause build a distinguished competitive advantage and mitigate the risks [9].
PSC is one of the most important management issues in sophisticated healthcare systems. The hospitals face various problems that need to mention, such as expensive medicines and others [10]. The managers of hospitals and drugstores are entirely aware of the circumstance of the preparation and maintenance of the drugs and do their best to service the patient at the right time and place [6]. Two risks might face in PSC. The first is the demand being more than the inventory level and might be a loss. The second is ordering more than the needs that cause the drug to spoil. In developed countries, the orders will be available at a specified time then there is no need to keep much inventory. Although this process happens slowly in developing countries [11]. Some emergency suppliers provide the medicines faster but at a higher cost to prevent loss.
This article explores bi-objective mathematical programming—the first aims to minimize the costs of preparing medicines from ordinary suppliers. Ordinary suppliers procure the drugs at a lower price but face the uncertainty that the lead time of orders is more than emergency suppliers. The second target is to propose a model that maximizes the utility of choosing an appropriate supplier for responding to demands.
The main contribution of this paper is the construction of two optimization models that incorporate the evaluation of suppliers for managing medications in hospitals, the capacity for overtime labour in hospitals, emer-gency purchases to avoid loss and the consideration of components of uncertainty.
The remaining sections of the paper are structured as follows: The relevant research literature is reviewed in Section 2, followed by the research technique and mathematical model in Section 3, the results in Section 4, and the conclusion in Section 5.
Literature review
Risk and uncertainty consideration in pharma supply chain (PSC)
Jnandev Kamath, Kamath, Azaruddin, Subrahmanyam, and Shabharaya [12] illustrated the proper actions to mitigate the risks in the pharma supply chain. Outsourcing and insurance are the best actions we can apply to mitigate financial and regulatory risk. It also can be useful for an inventory and counterfeit risks in inventory management. These solutions are based on an Analytical Hierarchy Process Model. Brettler [13] worked on managing pharmaceutical chain risks; He believes that the methodical process can manage those risks and explains that insurance could play a role in raw material supply, manufacturing, Quality Assessment, Stability Testing, final packaging, and Delivery to Customers to reduce the potential losses.
El Mokrini, Dafaoui, Berrado, and El Mhamedi [14] explained which claims risk assessment plays a particular function in outsourcing evaluation. This evaluation method consists of Risk Assessment, Risk Identification, Risk Analysis, and Risk Evaluation, each of which consists of three steps: Criteria utilized in risk categorization, MCDM for risk sorting, and model construction proposal utilizing ELECTRE Tri. Ouabouch and Amri [15] describe the risks in the Pharma Supply Chain and attempt to rank them from many perspectives at three stages: upstream, internal, and downstream. This article recommends focusing on supply- and demand-side risk factors. In addition, enhancing operations like demand forecasting and supplier relationship management was mentioned.
The purpose of this article is to analyze the risks that are associated with the Pharmaceutical Supply Chain. The AHP method was used in the risk assessment that the authors conducted. Using the Delphi Method, the most critical risks and sub-risks were prioritized in order of importance. According to the findings, the four categories of risks listed below are among the most significant: supply risks, organizational risks, financial risks, and demand risks [16].
Torasa and Mekhum [17] provide evidence that the corporate reputation of pharmaceutical businesses is impacted by supply-side risk factors, demand-side risk factors, financial risk factors, and operational risk factors. The results also indicate that it is necessary to address the negative impact of operational failures involving equipment or machines and power outages.
Pharma supply chain and its frameworks
Chen and Yu [18] investigated the optimization of Emergency Medical Service efficacy following a natural catastrophe. It utilized integer programming to enlarge the scope of the challenge. At the end of this article, numerical examples have been provided to substantiate its claims. Yu, Jia, Fang, Lu, and Xu [19] investigated multi-resource and multi-activity scheduling inside the medical procedure. Utilizing mathematical modelling based on a timed coloured Petri net and a dynamic simulation allocation technique, an attempt was made to maximize the utilized resources. The suggested methodology improves resource usage and reduces the cost of allocating multiple resources in terms of time.
Kwon, Kim, and Martin [20] published an article that investigates critical areas in which the healthcare supply chain may increase its efficiency in terms of the cost per patient discharge of healthcare operations while simultaneously improving the quality of treatment by lowering the readmission rate. The management of supplier relationships, the use of logistics operational tools, and the improvement of processes were identified as the three key strategic areas that should be stressed and proposed in order to get the highest value from supply chain operations.
Burinskiene [21] described an essay concerning the effectiveness of the pharmaceutical supply chain. Some suggestions can help reduce costs in the pharma supply chain, such as eliminating the middleman (wholesaler) who does not add value, cutting costs in areas where there is waste and money is not used efficiently, understanding the patterns in customer orders, and implementing a paperless process for supply chain operations.
Franco and Alfonso-Lizarazo [6] studied an optimization model for managing a pharmaceutical supply chain in hospitals under uncertainty. Their findings indicate that the optimal policy can reduce the current hospital supply and medicine management costs by 16% when considering 22 categories of medications.
Nasrollahi and Razmi [22] investigated a mathematical model for designing an integrated pharmaceutical supply chain with maximum expected coverage under uncertainty. Their results show that when different levels of trust for different pharmaceutical substances in different hospitals are taken into account, results are much better in terms of unmet demand without a big rise in costs.
Lee, Lee, and Schniederjans [23] studied the supply chain (SC) innovation for enhancing organizational performance in the healthcare sector. It also demonstrates that material and product delivery are required to support hospitals’ essential operations and plans, as well as supplier collaboration. Hospitals should classify SC activities in order to standardize the materials required for a lean SC that can give the greatest quality care at the lowest cost. Byrnes [24] published an essay on supply chain improvement prospects, such as Disaster Recovery, Supply chain integrity, and Network complexity. Significant developments in the healthcare supply chain have created new management imperatives for hospital and distributor administrators.
Rossetti, Handfield, and Dooley [25] worked on the examination of the Pharma Supply Chain from many perspectives. The results of the interviews from many firms show that compensation, alternative channels, and product forces are three major forces that can be influential. It also mentioned eight trends in evolving forces in PSC.
Mercanoglu and Ozer [26] wrote an essay discussing the significance of supply chain management in the pharmaceutical and radiopharmaceutical sectors, as well as the obstacles they encounter, such as fluctuating market circumstances etc. Finally, they discussed novel SCM methods in the Pharmaceutical and Radiopharmaceutical Industries from a financial and operational perspective.
Zandkarimkhani, Mina, Biuki, and Govindan [27] proposed a bi-objective Mix Integer Linear Programming (MILP) that considers demand uncertainty and inventory-location-routing considerations. This idea aims to save overall costs while simultaneously bringing back lost consumer interest. This bi-objective model is solved by using a one-of-a-kind approach for chance-constrained fuzzy goal programming, and a case study is presented to demonstrate and validate the model.
Tat, Heydari, and Rabbani [28] presented a mechanism that gathers expired pharmaceuticals from pharmacy warehouses for resale on the secondary market. The Pharma Supply Chain plays a vital part in this matter. Statistical analyses demonstrate that it can boost the anticipated profit for pharmacies and pharma suppliers.
Savadkoohi, Mousazadeh, and Torabi [29] created a multi-product, multi-period model for inventory placement. This approach seeks to dilute the expenditures of the pharmaceutical network design challenge that takes perishability into account. In addition, it serves as a case study to demonstrate the model’s capability and volatility handling technique.
Franco and Alfonso-Lizarazo [6] created two mixed integer programming models in order to optimize the strategic and operational decisions made inside the pharmaceutical supply chain (PSC). The first model takes into consideration things like expiration dates, the required service level, perishability, inventory levels based on age, and any purchases that need to be made in an emergency. The second model determines an acceptable expiration date for pharmaceuticals to cut down on the number of medications that have outlived their usefulness.
Uthayakumar and Priyan [10] demonstrate an inventory model to identify the appropriate lot size, lead time, etc., for Pharma Supply Chain (PSC) to reduce costs. It may be utilized to manage medical and pharmaceutical supplies without overstocking or expiry. This approach seeks to obtain the desired CSL at the lowest possible PSC inventory cost. At the conclusion, a numerical example is shown.
Research methodology
The purpose of this study is to develop a bi-objective mathematical model. The first objective aims to minimize the costs of preparing lot sizes of medicines. The medicines procured from ordinary suppliers and emergency suppliers cost more. It is exploited to reach the most efficient and cheapest supplier. The second objective is to maximize medicine orders from the best suppliers. The models focus on primary issues such as perishability, human resource constraints, the maximum number of orders, and the service level.
The elements of the proposed PSC model consist of several different parts. The supplier and the manufacturer or retailer that cooperate between these elements can prevent the waste of medicines. The pharmacy that manages the inventory level should control the safety of drugs that are significant in distribution to the hospital. The hospital is one of the most significant elements that provide medicines to patients and places orders from the pharmacy.
The patients are the reason for this system that requires treatment and medicines.
This article aims to increase service levels, optimize inventory costs, etc. Deficiencies are allowed in this model, but a lack of medicines might face danger for the patients. There is an element of unknown factor involved in each step along the chain: hospital administrators and pharmacies do not know the demand for the medications, and the pharmacy does not know the precise price at which the medicines are sold.
In that order, the selection of an acceptable supplier will be based on financial, quality, and environmental considerations. Financial considerations are among the most appealing criteria for managers when picking suppliers. In this study, this variable includes labour, machinery & equipment, material, and energy expenses. This is an undesired element; thus, the less of it there is, the better. Next on the list of input requirements is quality. Due to its direct influence on supply chain outcomes, quality is an essential aspect. Two sub-criteria comprise quality: materials and certificates. Quality controls and standards are required to avoid issues and mitigate risks. This criterion is highly desired. In recent years, environmental concerns have received a growing amount of attention.
Consequently, we evaluate this factor based on the sub-criteria of Standards, Staff, Technologies, Energy, GHG Emissions, and Materials. Employing environmentally friendly technology for more efficient material and energy use is essential. Next, we consider consumer satisfaction. Customers have a significant role throughout any firm. Consequently, clients are central to the decision-makingprocedure.
Best-worst method
BWM is a technique for making judgments based on several criteria by comparing two criteria simultaneously using pairwise comparisons. Some of the areas in which it has been used include green innovation, technology evaluation and selection, logistics performance evaluation, research and development performance evaluation, SC management, and evaluation of SC logistics [30–32]. Before discussing the processes of this approach, it is crucial first to review its underlying philosophy and goal.
Let’s say there are n criteria, and we want to develop a pairwise comparison matrix so that we can start figuring out how much weight each condition should have. As will become clear in the next illustration, each cell in this matrix is a representation of the relative preference of one criterion over another.
In addition, the decision-maker (DM) is responsible for filling out the pairwise comparison matrix using a scale ranging from 1 to 9. For example, the relative preference of criterion I to criterion j is denoted by the variable a
ij
. If a
ij
is equal to one, it indicates that I and j are of equal value; however, if it is more than one, it indicates that I is viewed as a much more essential one. Let us say that the fact that a
ij
= 9 is evidence of how critically important i to j are to the equation.
Considering the reciprocal property of the matrix, (n-1)/2 pairwise comparisons will be performed to complete the matrix. There is an important consideration surrounding this matrix, and it relates to its consistency. A pairwise comparison matrix is consistent, according to the [33] if:
What was described before were the fundamentals of the pairwise comparison matrix. However, there is still a concern regarding the certainty and dependability of this matrix. To utilize the views of experts, we must ensure that these concepts are not prejudiced and can convey the relative importance of criteria I through j. This approach was proposed to determine the weights of each criterion by comparing them to the best and worst standards. By employing these criteria, the decision-maker can communicate his choices more clearly, facilitating the comparison process.
In this part, we will discuss the BWM stages that can be utilized to determine the weights of the criterion, and they are as follows:
Step 1: Determine decision criteria assets
In this stage, we evaluate the decision-making criteria c1, c2, c3...c n.
Finding the best and worst criteria is the second step. This stage requires DM to choose the most critical and least important criteria.
Step 3: Determine the preference of the best criterion over other criteria by using a value between 1 and 9, which will result in the best-to-others vector.
The others-to-worst vector is constructed in Step 4 by assigning a value between 1 and 9 to the preference of other criteria over the worst one.
Step 5. Finding the optimal weights (w1, w2, w3, … w
n
). The optimal weight for each criterion is the one for which
Maximum absolute differences between
In order to make the model in the linear form equation 6 is obtained:
In 1981, Hwang and Yoon presented the TOPSIS technique, which allows users to rank solutions based on how close they are to the optimal one. TOPSIS is an effective method for solving problems associated with making decisions using several criteria and limited options [35]. Using a distance measure between each option and the ideal and negative ideal solutions, this method attempts to determine which choice is superior.
According to reference [36], here are the steps of the TOPSIS method: determining the decision matrix R = {r
ij
}, in which r
ij
is the value of the j th attribute in i th alternative; i = 1, 2, . . . , m; j = 1, 2, . . . , n. Considering the difference of attributes in dimension and order of magnitude, normalize the decision matrix R and transform it into the normalized matrix Find the weighted normalized decision matrix V = {v
ij
} by the following equation:
Calculate the and by the following equations:
Calculate the relative closeness of each alternative by the following equation:
The value of relative proximity is directly proportional to the alternative’s degree of relative superiority. If the RC i value for alternative I is larger, this implies that it is a comparatively better option, but if it is less, this indicates that it is a significantly lower option.
The following is a list of the primary elements that make up the pharmaceutical supply chain: I the companies that are responsible for the production or distribution of the medicines; ii the hospitals that are accountable for the ordering of medicines from the companies that are responsible for the production or distribution of the medicines; iii the patients who require treatment and medicines; and iii the patients who are responsible for placing orders with the pharmacies. As a result of this, the following presumptions underpin our strategy.
Assumption A1. Every one of the periods in P represents one month.
Assumption A2. For each medicine, the initial stock = 0.
Assumption A3. The demand has to be satisfied at a rate equal to one hundred per cent of the service level. In the case that the stock that is now available is inadequate to satisfy the demand, an emergency buy will be executed at a cost that is higher than the purchase price that is typically used.
Assumption A4. In this strategy, the provided mathematical models concentrated on the choices the managers made for the hospital.
Assumption A5. The inventory level of one period is calculated at the beginning.
Assumption A6. The cost of medicine in a specific period for ordinary suppliers is the same.
Assumption A7. The medicines are added to the warehouse at the beginning of the period.
Assumption A8. The total purchased medicine from a supplier for different types of medicine in a period is calculated in one order.
Assumption A9. The envisioned supply chain consists of three tiers: suppliers, hospitals, and demand zones (patients).
Assumption A10. In addition, the supply chain is viewed as being multi-period and multi-product.
Mathematical model
The proposed model is used for the scheduled horizon that each period is equal to one month. Every month there is a demand D MP for different kinds of medicine m ∈ M. The requirements of mediation are prepared with ordinary and emergency suppliers that Y MSP indicate if the purchase of specific medicine m ∈ M in a period p ∈ P from a set of suppliers is done or not. Mna is responsible for determining the maximum amount of orders that may be placed within each time period.
Three main variables denote a request for medicines, X MPS determine the total number of medicines purchased. The number of medicines gathered from ordinary suppliers shows with MO MP and the ones from emergency suppliers by ME MP . This purchase is made with a cost of C SMP for a unit of medicine. It needs to mention that each supplier has some limitations in preparing the medicine determined with RC MSP . The inventory level in the period p ∈ P determined by I MP and also the reorder point, which impact the number of orders shown with RO M binary variable SE MP decide if the order should be done or not. The medicines that are administered to patients specify with MP MP and while not having enough mediations, the variable B MP shows the amount of backorder of medicine m ∈ M in period p ∈ P and also the penalty of back-ordering defined with the variable BP MP .
An additional category of administrative constraints is represented by taking into account the quantity of human resources that are cap p available throughout each time period as well as the amount of permissible overtime labor by W P . For the purpose of modelling this limitation, the parameter Ut M , which denotes the amount of time needed in hours to manufacture a unit dosage, is used. The overtime working should be less than the GE P and PS P variables which shows the maximum capacity of overtime working in a period and the available percentage of overtime working hours due to capacity of regular time.
Each kind of medicine occupies some space determined with OS
M
and the total occupied space must be less the available storeroom of the hospital shows with SR
P
. The following equations represent the model which minimizes pharmaceutical SC in hospitals.
The objective function minimizes the total cost of preparing the medicines. The model considers the number of medicines ordered, the expense of medications supplied from ordinary and emergency suppliers, the inventory, and the overtime working expenses. It aims to maximize the orders of the ordinary supplier and choose the best supplier in each period.
S.t
Regarding constraint (1) aims to handle the inventory level of different kinds of medicine in periods. It shows that the inventory level of the period comprises medicines purchased from suppliers and drugs from the previous period. The medications were administered to patients, and the backorders of drugs are other factors that need care.
The constraint (2) presented the connection between the binary variable and the number of medicines purchased from ordinary and emergency suppliers. It shows that if the binary variables are confirmed, it will be possible to purchase mediation.
Through constraint (3), the number of medicines administered to patients in one period should be, at most, the medicines purchased from ordinary and emergency suppliers in addition to the ones held and the back order of the previous period.
Constraints (4) and (5) specify the connection between the reorder point and the inventory level of medicines.
The constraint (6) signifies that the number of medicines that must be kept in stores equals the total purchased medications minus the ones that were not administered to patients.
According to constraint (7), human resource capacity is affected by the amount of medicine that can be arranged in a specific time depending on the unitary time for making a unit dose of medicine and the number of ordered medications. Overtime is another option in emergencies that cause high costs for the system.
Constraint (8) cares about the cumulative number of orders from different medicine types prepared by the ordinary and emergency supplier. It should not be more than the maximum number of orders that are allowed.
The constraint (9) illustrates the total number of medicines ordered from ordinary and emergency suppliers in one period.
According to constraint (10), the storeroom constraint present that each kind of medicine occupies a specific space and the number of medicines in the store is limited.
The constraint (11) signifies that the backorder of a specific medicine in a period equals the demand for medicine minus the ones administered to patients.
Through constraint (12), the number of medicines purchased from ordinary suppliers equals the limited number of medicines the suppliers can afford in one period.
According to constraint (13), the reorder point of one medicine should be less than the medicines purchased from ordinary suppliers.
Through constraint (14) and (15), the available overtime must be less than a particular percentage of human resource capacity or the maximum available overtime in hours in a period.
The constraint (16) presents that a certain percentage of medicines purchased from ordinary suppliers should be kept for the next period.
Through constraint (17), the medicines that were purchased from ordinary suppliers should not be more than the demand for that period.
Computational experiment
In this section, the demand for specific medicine equals D. The hospital receives the drug at unit cost c from ordinary and CC from emergency suppliers. The cost of keeping inventory in periods is shown with H, and B presents the backorder penalty. It is crucial to provide a high service level for the hospitals that face the challenge of satisfying the patients’ drug needs.
The proposed model has been reviewed in two scales. The first size problem is related to a clinic with fewer patients and a hospital in the second size. The data which is applied to solve the model is shown in the table below.
Model validation
Demand is one of the main factors that can affect the system’s costs. While increasing it, the orders from emergency suppliers go up. It causes to increment in the available human resource capacity or the use of warehouses and the costs of the whole system. The backorder cost is another which can influence the expenses. While the backorder cost increases, the hospital tries to store the medicines in the warehouses, which causes the growth of inventory costs; inversely, when the costs of maintenance increase hospital try to keep drugs for a short time. The loss is a critical factor that needs to have cared for. Fixed inventory ordering cost of medicine can cause significant changes in the number of orders of specific drugs. While it decreases, the number of orders increases; there is no need to keep much inventory, although the hospital can process limited orders in one period. Reorder points of different kinds of medicine can also impress the number of orders. To prevent loss and risks like delays in delivery, the companies put high reorder points that force the company to order the mediations soon. In some cases, much inventory needs to be stored, and it causes high expenses.
Sensitivity analyses
In this part, we do sensitivity studies on key factors. Given that decision-makers may be in varying circumstances that alter the amount of data and problem factors, the ideal approach must be identified by examining the impact of various model parameters. As part of a precise sensitivity analysis, the impact of changes in the values of two significant factors, such as the cost of medication (C) and Human Resource Capacity (F), on the best values may be determined. Under the same degree of confidence, it is evident that when the parameter C grows, so does the value of the objective function, and vice versa. It should state that ideal values rise as Human Resource Capacity grows.

Interactions throughout the SC of pharmaceuticals.
Here, in order to examine sensitivities, a one-dimensional technique has been employed. In other words, we maintain all the factors constant and merely alter one to determine its effect on the objective function value. As the suggested model incorporates several costs, changing their values would influence the model’s judgments. The cost sensitivity analysis is presented in Figs. 7-8.
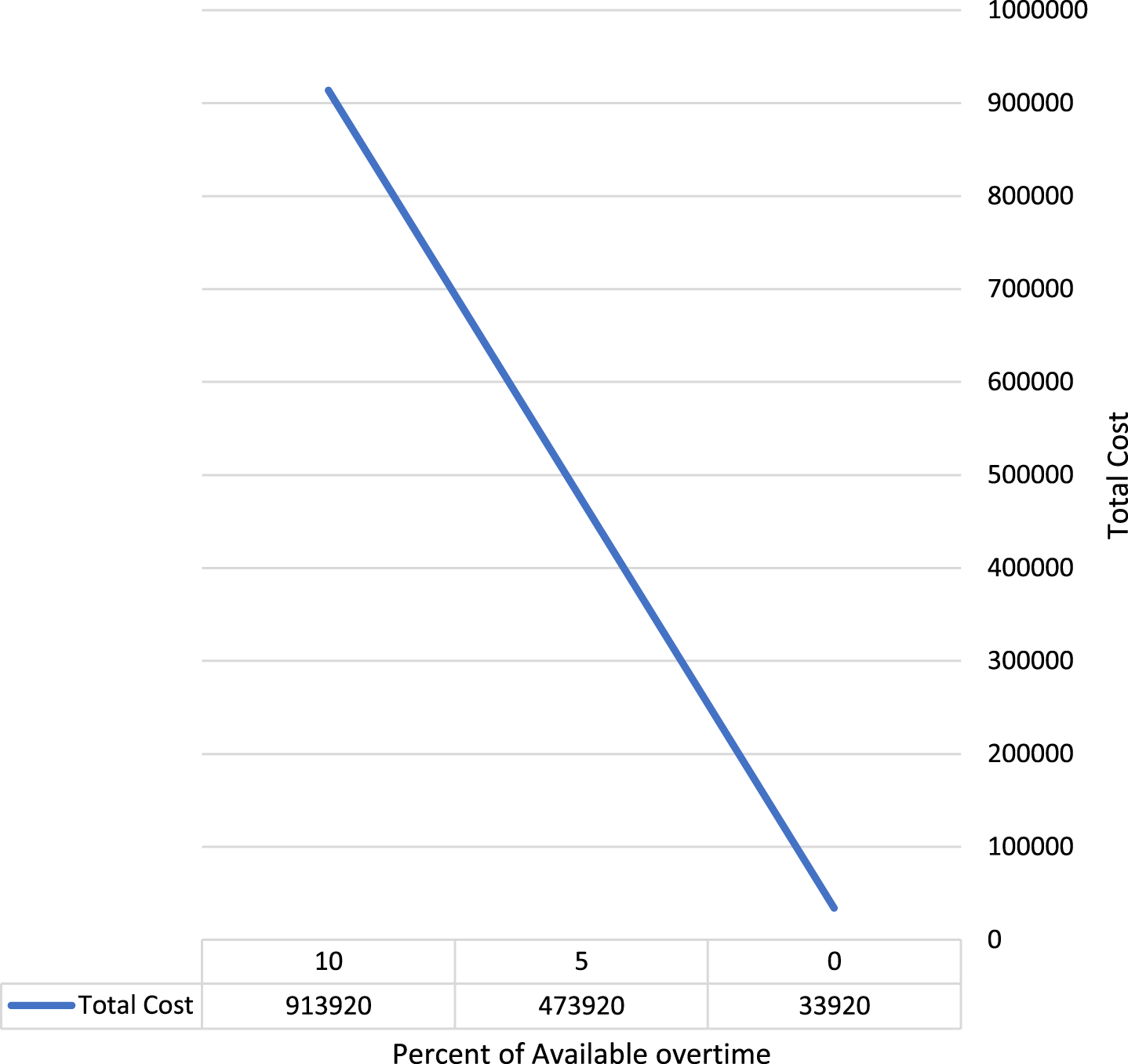
Impact of percent of available overtime.
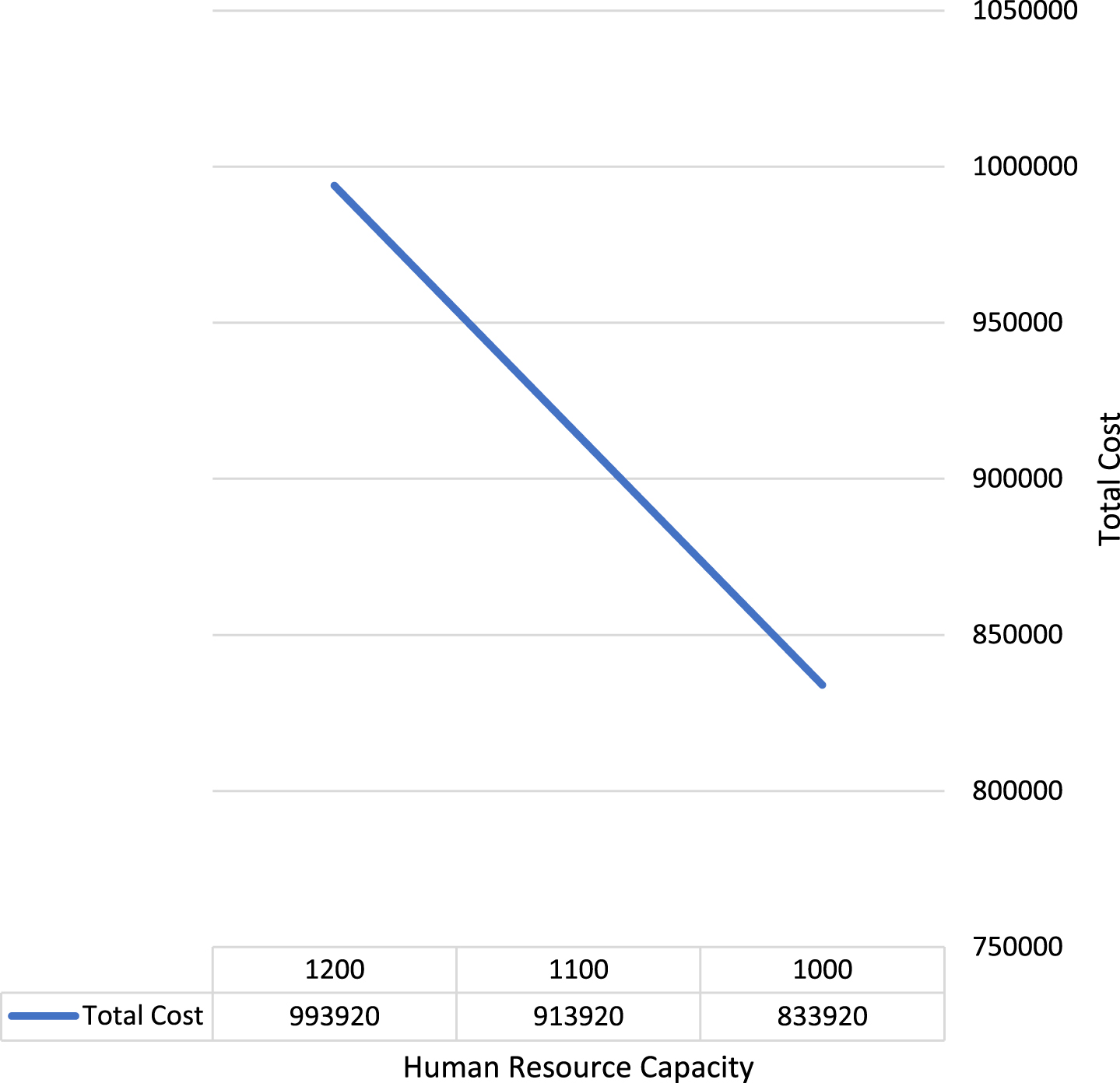
The impact of human resource capacity.
The proposed article helps the managers of the hospitals to optimize the amount of medicine needed to be ordered in a period. It prevents loss and maximizes the service level. The priority of ordering medications in the proposed model is with ordinary suppliers that release the drugs at a lower price. Scheduled demand for medicines in all periods equals the capacity of ordinary suppliers. The regular capacity of ordinary suppliers is one of the main factors determining the amount of allowed medicine to be purchased in one period.
Problem sizes
Problem sizes
In some cases, the uncertainty of demand causes orders from emergency suppliers. This article also distinguishes the suppliers that transport the drugs with delay or present with less quality from other arranged suppliers. This model considered many aspects that many hospitals might face, like the available storeroom or the regular capacity of ordinary suppliers. This innovation of this paper that distinguishes it from previous related articles is considering an increase in human resource capacity that Franco and Alfonso-Lizarazo (2020) just considered the scheduled human resource capacity. However, in this paper, a limited increase for emergencies is allowed. Savadkoohi et al. [29] determine whether the available inventory level is less than the reorder point. Nevertheless, this model shows that the reorder point must be less than the amount of medicine purchased from ordinary suppliers in one period. It also says that a specific percentage of medicines need to be kept in warehouses to prevent loss for the next period.
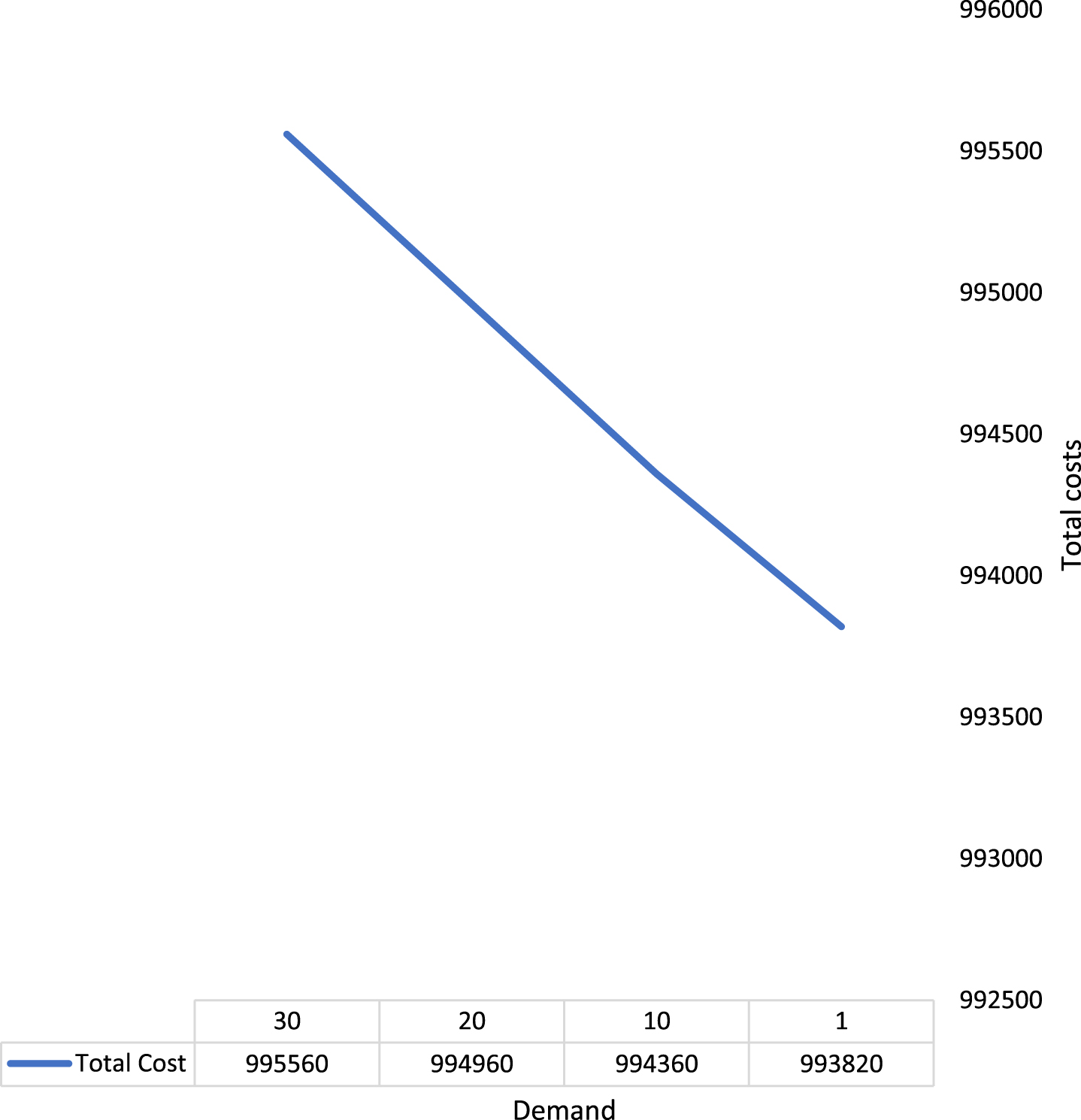
Figure 2 indicates that the total cost will decrease when the demand decreases. Figure 3 shows that the total cost will decrease when the operational costs imposed on stores decrease. Figure 4 depicts that the total cost will decrease when medicine costs decrease. In Fig. 5, we can see that the total cost will decrease when the fixed ordering cost decreases. According to the Figs. 6-8, the impacts of distance of suppliers, percent of available overtime, and human resource capacity on total cost are direct.

Impact of demand.
Impact of cost to store.

Impact of cost of medicine.
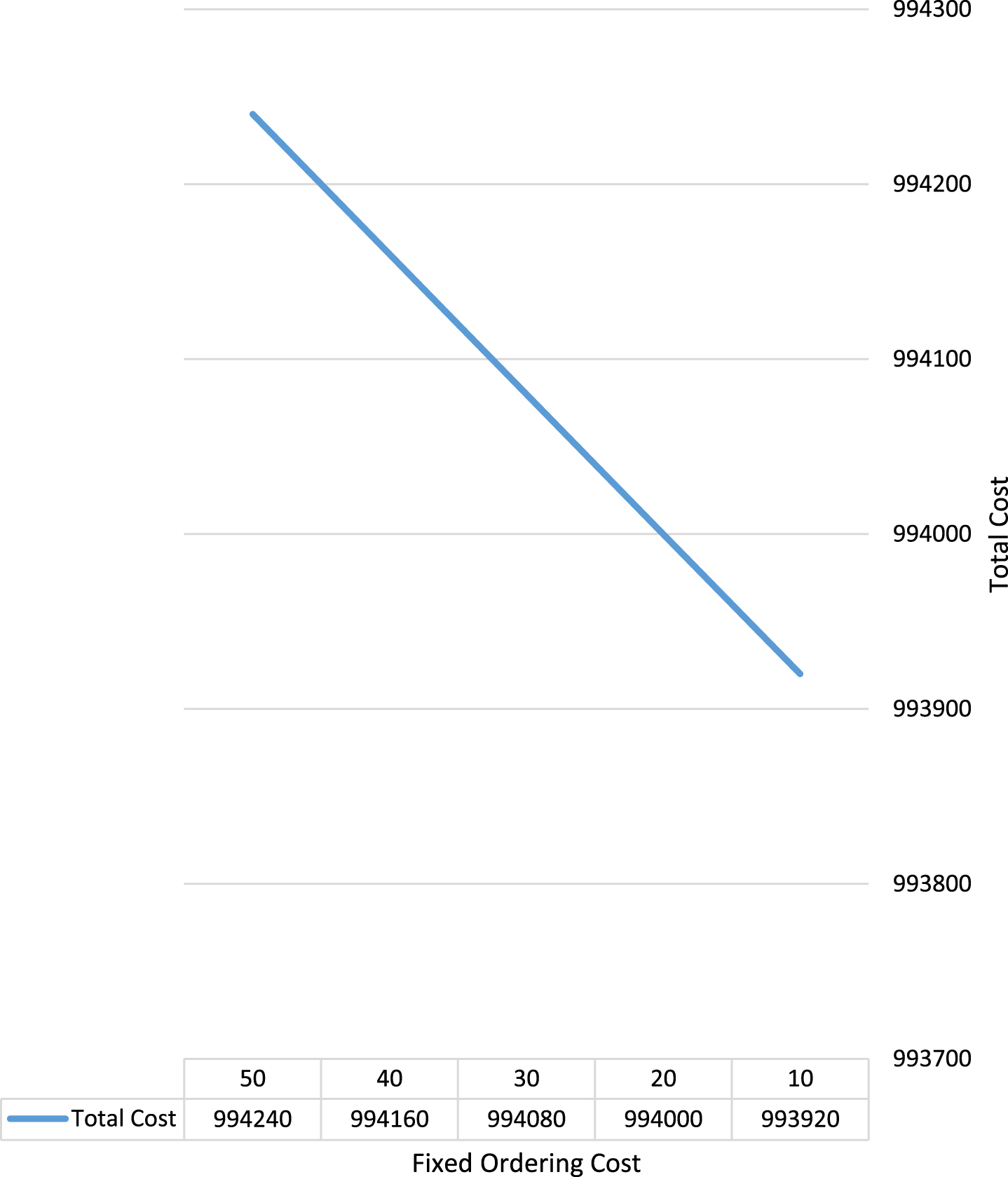
Impact of ordering cost.
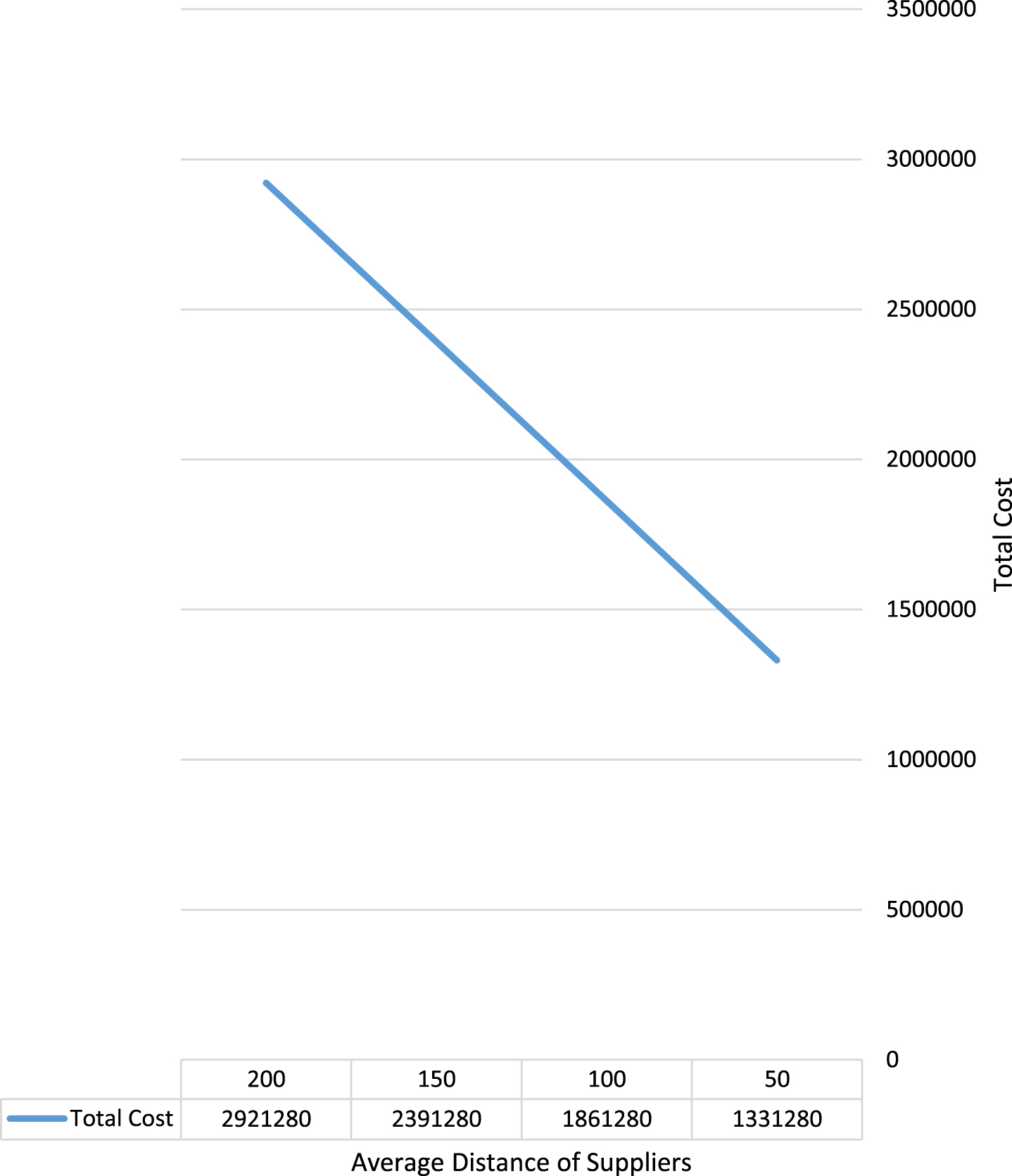
Impact of distance of suppliers.
In this work, a bi-objective MILP model was presented by taking inventory, human resource capacity, supplier distance, and demand uncertainty into account in order to solve uncertain pharmaceutical logistics issues in hospitals. The primary purpose is to reduce the overall cost of purchasing from both standard and emergency suppliers. The second purpose is to choose the best suppliers based on predetermined criteria utilizing the Best-Worst and TOPSIS technique. The suggested model was executed using the GAMS program. A sensitivity analysis approach then validated the validity of the suggested model.
This paper’s contribution is the construction of two optimization models that incorporate the evaluation of suppliers for managing medications in hospitals, the capacity for overtime labour in hospitals, emergency purchases to avoid loss and the consideration of components of uncertainty. The findings of the suggested approach indicate that it may substantially cut buying and inventory costs. In addition to its advantages, any research always has certain limits. Recognizing them may result in future research achievements. In addition, research on drugs that expire in warehouses is required to enhance the pharmaceutical supply chain.
Footnotes
Acknowledgment
The general Project of the Education and Research Project of Young and Middle-aged Teachers of Fujian Provincial Department of Education (Social Science) in 2022, Research on the integration of the industrial chain of Textile Shoes and Clothing in Quanzhou under the background of industrial Transfer (No. JAS22199).