
Abstract
Background:
Orthostatic hypotension (OH) may antedate Parkinson’s disease (PD) or be found in early stages of the disease. OH may induce a PD brain to chronic hypotensive insults. 18F-Florbetaben (18F-FBB) tracer has a high first-pass influx rate and can be used with positron emission tomography (PET) as a surrogate marker for early- and late-phase evaluation of cerebral perfusion and cerebral amyloidosis, respectively.
Objective:
In this study, we evaluated whether 18F-FBB uptake in the early- and late-phases of PD was related to OH. This study manipulated the imaging modality to illustrate the physiology of cerebral flow with OH in PD (PD + OH).
Methods:
A group of 73 early-stage PD patients was evaluated with a head-up tilt-test and 18F-FBB PET imaging. The cognitive status was assessed by a comprehensive battery of neuropsychological tests. PET images were normalized, and both early- and late-phase standardized uptake value ratios (SUVRs) of pre-specified regions were obtained. The associations between regional SUVRs and OH and cognitive status were analyzed.
Results:
Twenty (27.4%) participants had OH. Thirteen (17.8%) patients were interpreted as having amyloid pathology based on regional 18F-FBB uptake. Early-phase SUVRs were higher in specific brain regions of PD + OH patients than those without OH. However, late-phase SUVRs did not differ between the groups. The early-phase SUVRs were not influenced by amyloid burden or by interaction between amyloid and orthostatic hypotension. Cognitive functions were not disparate when PD + OH patients were contrasted with non-OH patients in this study.
Conclusion:
Cerebral blood flow was elevated in patients with early PD + OH. This finding suggests augmented cerebral perfusion in PD + OH might be a compensatory regulation in response to chronic OH.
Keywords
INTRODUCTION
Orthostatic hypotension (OH) is not uncommon in the early stage of Parkinson’s disease (PD) [1] and may be found in the prodromal period of disease [2], exposing the PD patient to chronic hypotensive insult. It has been postulated that cerebral autoregulation modifies its range to accommodate the blood pressure (BP) drop in PD [3]. PD is also related to concomitant amyloid-β (Aβ) pathology, the presence of which is observed to influence clinical expression [4].
Application of imaging biomarkers has been extended to predict or anticipate clinical progression in neurodegenerative diseases such as Alzheimer’s disease, and perfusion imaging has been utilized to reflect functional integrity, including synaptic dysfunction and neuronal injury [5]. However, metabolic imaging has been of limited use for PD. PD-related patterns have been used to differentiate PD from other atypical Parkinsonian disorders, and the features of binary division of PD-tremor-related patterns have been correlated with motor dominance [6, 7]. Functional imaging has been seldom employed to study the neurophysiology of PD with OH (PD + OH).
18F-Florbetaben (18F-FBB) is a lipophilic amyloid tracer. It has a high first pass influx rate that correlates with cerebral blood flow, which allows it to be a surrogate of cerebral perfusion when measured early (post-injection) and a marker of cerebral amyloidosis when delayed [5, 9].
The main hypothesis in this research was that, in early PD with cardiovascular dysautonomia, compensatory changes of cerebral autoregulation regulate regional cerebral flow in response to chronic orthostatic insult to maintain functions relevant to brain regions, irrespective of amyloid burden. Dual-phase 18F-FBB positron emission tomography (PET) imaging was suitable to evaluate contemporary cerebral flow (early-phase) and brain amyloidosis (late-phase) of PD + OH, allowing simultaneous characterization of hemodynamic status and amyloid accumulation.
METHODS
Participants
This study was approved by the Institutional Review at Seoul St. Mary’s Hospital, and all subjects provided written informed consent to participate. All experiments were performed in accordance with relevant guidelines and regulations. This study was registered (Identification Number: KCT0005552) in the Clinical Research Information Service (CRIS; http://cris.nih.go.kr), which is an online clinical trial registration system established by the Korea Centers for Disease Control and Prevention (KCDC) with support from the Korea Ministry of Health and Welfare (KMOHW) and embodied as a part of the Primary Registries in the World Health Organization (WHO) Registry Network.
Seventy-three drug-naïve, de novo PD patients who visited our institution between June 1, 2018 and December 10, 2020 were enrolled. Participants were diagnosed with idiopathic PD according to the criteria of the UK PD Society Brain Bank [10]. All subjects underwent PET using 18F-N-(3-fluoropropyl)-2β-carbon ethoxy-3β-(4-iodophenyl) nortropane, and every patient had decreased presynaptic dopamine transporter uptake, predominantly in the posterior striatum [11]. Clinical characteristics of age, sex, motor symptom duration, body mass index, education status, smoking status, and history of hypertension, diabetes mellitus, dyslipidemia and stroke were obtained by interviews or medical records. Disease severity was assessed with the Unified Parkinson’s Disease Rating Scale (UPDRS) and modified Hoehn and Yahr (H&Y) stages [12, 13]. Apolipoprotein E (APOE) polymorphism was evaluated, and the subjects were categorized based on the presence of the APOE ɛ4 allele. Patients with the following indications were excluded: (1) symptoms or signs of atypical PD and secondary Parkinsonism; (2) history of heart problems such as heart failure or atrial fibrillation that could influence BP; (3) history of autonomic neuropathy; (4) history of symptomatic stroke or other brain lesions that affect cognition; and (5) clinical suspicion of dementia screened by a comprehensive neuropsychological battery [14], when available.
Neuropsychological evaluation
The neuropsychological evaluations were performed in drug-naïve state and the tests were rated by experienced psychologists who were blinded to patient clinical and neuroimaging data. Information about memory problems and other subjective cognitive deficits was obtained from caregiver interviews. Global cognitive efficiency was investigated by a Mini-Mental Status Examination and Clinical Dementia Rating (CDR). Five cognitive domains were assessed by a comprehensive neuropsychological battery [14]. Attention/Working memory was examined with the Digit Span Forward Test and the Korean-Color Word Stroop Test (K-CWST). Executive domain was evaluated with the Digit Span Backward Test, and phonemic fluency was estimated with the Controlled Oral Word Association Test (COWAT). Language and visuospatial domains were assessed by the Korean-Boston Naming Test and the Rey Complex Figure Test (RCFT), respectively. Verbal and visual memory domains were investigated separately, with subdomains of immediate recall, delayed recall, and recognition, with the Seoul Verbal Learning Test (SVLT) and the RCFT, respectively. The z-scores of each subtest were extracted for analysis [15]. Of the 73 PD patients, those who did not complete a full battery of neuropsychological tests because of illiteracy or other physical and/or neuropsychological problems, were excluded from the cognitive function analysis (n = 13).
Head-up tilt test
All participants were in a fully resting state before the procedure and were in drug-naïve state. Continuous electrocardiograph leads and non-invasive BP monitoring equipment were applied to the patients (YM6000, Mediana Tech, Redmond, WA, USA). A supine position was maintained for 20 minutes before tilting to 60 degrees (ENRAF NONIUS, Rotterdam, The Netherlands). BP and heart rate were measured every 5 minutes for 20 minutes in the supine position. In a tilted position, BP and heart rate were recorded at 0, 3, 5, 10, 15, and 20 minutes. The supine BP at 0 minutes was excluded, and the average supine systolic and diastolic BPs were calculated with the measurements at 5, 10, 15, and 20 minutes. The lowest systolic and diastolic BP at 3 or 5 minutes during the tilted position were selected, and the orthostatic BP changes of systole (ΔSBP) and diastole (ΔDBP) were calculated. OH was defined as orthostatic ΔSBP≥20 mmHg and/or ΔDBP≥10 mmHg [16].
123I-metaiodobenzylguanidine (123I-MIBG) scintigraphy
123I-MIBG scintigraphy was performed using a dual-head camera equipped with a low-energy, high-resolution collimator (Siemens), and data were collected at 30-minute (early) and 2-hour (late) intervals after a 111 MBq 123I-MIBG injection. A static image was obtained with a 128×128 matrix. Regions of interest were manually drawn around the heart and mediastinum. Tracer uptake was measured within each region of interest to calculate the heart-to-mediastinum (H/M) ratio. The lower limit of the reference value for delayed H/M ratio was calculated to be 1.78 [17].
18F-Florbetaben positron emission tomography imaging acquisition, processing, and interpretation
Dual-phase 18F-FBB PET-computed tomography (PET/CT) images were acquired on a dedicated PET/CT scanner (Discovery PET/CT 710, General Electric Healthcare, Waukesha, USA). Early-phase PET data were obtained 10 minutes after intravenous injection of 296 MBq of 18F-FBB. Ninety minutes after 18F-FBB injection, delayed-phase PET data were obtained. A low dose CT scan for attenuation correction was obtained immediately before PET imaging. Both early and delayed static PET data were reconstructed using a fully 3D ordered subset-expectation maximization algorithm (VUE Point HD) with 4 iterations and 16 subsets, with a 3 mm filter and a 256×256 matrix size. Individual structural T1 magnetic resonance imaging (MRI) acquisitions were used for spatial normalization of PET data. The mean interval between MRI and 18F-FBB PET acquisitions was 14.9±62.1 days.
Statistical Parametric Mapping version 8 (University College of London, London, UK, http://www.fil.ion.ucl.ac.uk/spm) was used for PET image preprocessing. Individual PET images were coregistered to the corresponding T1 MRI images using a rigid transformation. The individual MRI scans were spatially normalized into MNI space via the T1 MRI template using non-linear registration. The automated anatomical atlas 3 (AAL3), consisting of 170 regions-of-interest (ROIs), was used to parcellate the ROIs [18]. The central white matter area was chosen as a reference area to calculate the standardized-uptake-value-ratio (SUVR) for semi-quantification of perfusion from early-phase 18F-FBB PET images [8, 19], which was extracted from the SPM12 white matter probability map using a threshold of 75%probability. The cerebellar gray template presented by the Centiloid Project was chosen as a reference ROI to calculate SUVR for semi-quantification of amyloid β plaque from the delayed-phase 18F-FBB PET images [20]. Delayed-phase 18F-FBB PET imaging was visually interpreted by two nuclear medicine physicians (S.H. and H.Y.) as either positive or negative based on regional 18F-FBB uptake assessment of the lateral temporal cortex, frontal cortex, posterior cingulate cortex/precuneus, and parietal cortex, as previously described [21]. The images were acquired in in drug-naïve state.
Regions of interest
Among parcellated regions of AAL atlas 3, 29 related to five cognitive domains [22, 23] and motor behavior [23, 24] were pre-specified and used for investigation (Supplementary Table 1).
Statistical analyses
All statistical analyses were performed with jamovi software (version 1.2, Retrieved from https://www.jamovi.org/, 2020) with additional R software (version 3.6, Retrieved from https://cran.r-project.org/, 2019) car and emmeans packages (Retrieved from https://cran.r-project.org/package = car., 2018, and Retrieved from https://cran.r-project.org/package = emmeans., 2018). Descriptive analyses and independent or Welch’s t-test, Mann-Whitney U test, or Fisher’s exact test were applied as appropriate to describe baseline characteristics of the PD patients. Subgroups of participants were examined by a general linear model, adjusted for age, disease duration, and disease severity, with additional covariates when needed. Multiple comparisons were corrected with a Benjamini-Hochberg procedure at a defined significant two-tailed p-value < 0.05.
RESULTS
The mean age of participants was 70.8±8.7 years, and 36 (49.3%) were female. Median disease duration was one year (interquartile range, IQR, 1.4). The total sum of the UPDRS was 29.9±16.8, with a median modified H&Y value of 2.5 (IQR, 0.5). Of the patients evaluated, 13 (17.8%) had positive Aβ based on visual analysis of the 18F-FBB PET scan, and 14 (19.2%) had at least one APOE ɛ4 allele. Amyloid positivity and APOE ɛ4 status did not have any association (McNemar test, χ2 = 0.077, p = 0.78).
Twenty (27.4%) subjects had OH. Motor functions were not different between groups when adjusted for age, sex, and disease duration (PD non-OH vs. PD + OH: UPDRS Part II, 6.8±0.7 vs. 8.1±1.1, p = 0.35; UPDRS Part III, 20.6±1.4 vs. 21.2±2.4, p = 0.82; not shown in the table). PD + OH had a lower delayed H/M ratio and a higher supine BP than those without OH (PD non-OH vs. PD + OH: delayed H/M ratio, 1.62±0.45 vs. 1.40±0.34, p = 0.04; supine SBP, 122.2±18.3 mmHg vs. 135.0±18.5 mmHg, p = 0.01, Table 1).
Clinical characteristics
OH, orthostatic hypotension; BMI, body mass index; H&Y, Hoehn and Yahr; UPDRS, Unified Parkinson’s Disease Rating Scale; SBP, systolic blood pressure; DBP, diastolic blood pressure; H/M, heart-to-mediastinum; APOE, apolipoprotein E; SD, standard deviation; IQR, interquantile range. +Blood pressure unit is mmHg. Group differences were compared using independent or Welch’s t-tests, Mann-Whitney U test, or Fisher’s exact test, as appropriate. Statistical significance was defined as a two-tailed p < 0.05.
Table 2 and Fig. 1 summarize the between-group regional SUVR differences at each time point. During the early-phase, the PD + OH group manifested higher uptake ratios than PD non-OH in the regions of precentral gyrus, dorsolateral superior frontal gyrus, inferior frontal gyrus (opercular part), supplementary motor area, medial superior frontal gyrus, middle cingulate/paracingulate gyrus, superior parietal gyrus, and inferior parietal gyrus (supramarginal and angular gyrus excluded). These regions were significant after correction of multiple comparisons. When the 18F-FBB activities in the early-phase were compared according to amyloid pathology positivity, significant regional differences were not found (Supplementary Table 2). The results of Table 2 and Supplementary Table 2 manifested that in regions of increased uptake in early-phase did not coincide with any significant increase of late-phase SUVRs. Interaction between amyloid burden and OH did not exert any influence on cerebral perfusion (Supplementary Table 3). SUVRs acquired during the late-phase also did not differ between groups in the pre-specified areas.
Regional standardized uptake ratios (SUVRs) differences between groups
OH, orthostatic hypotension. Data are presented as means±standard deviation. *Supramarginal and angular gyrus are excluded. Group differences were compared using analysis of covariance (ANCOVA) adjusted for age, disease duration, and total sum of Unified Parkinson’s Disease Rating Scale (UPDRS) and mean supine systolic blood pressures. Multiple comparisons were adjusted using the Benjamini-Hochberg procedure. Statistical significance was defined as a two-tailed p-value < 0.05.
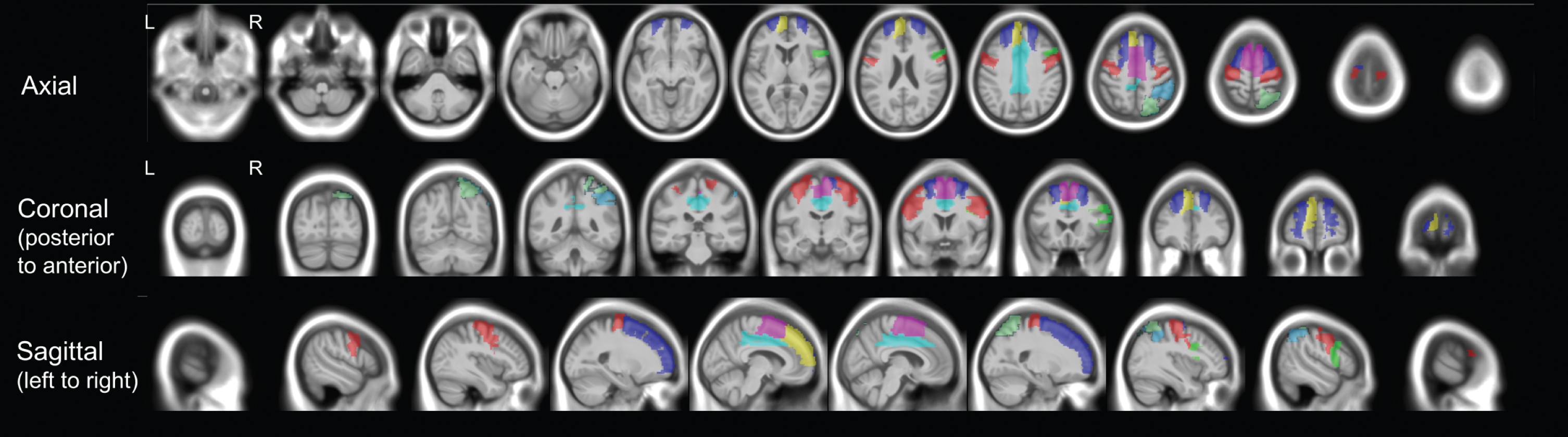
Regions of interest with significantly higher perfusion in the OH group than in the non-OH group. Axial, coronal, and sagittal images were presented with neurological orientation. Red, Precentral Gyrus; Blue, Superior Frontal Gyrus, Dorsolateral; Green, Inferior frontal gyrus, dorsolateral; Purple, Supplementary Motor Area; Yellow, Superior Frontal Gyrus, Medial; Cyan, Middle Cingulate & Paracingulate Gyrus; Mint, Superior Parietal Gyrus; Sky blue, Inferior parietal gyrus. OH, orthostatic hypotension; L, left; R, right.
In a subset of participants, the cognition of 60 patients was analyzed and stratified by OH (Table 3). They were all non-demented, and global cognition did not differ (PD non-OH vs. PD + OH: MMSE, 27.0 vs. 26.0, p = 0.32; CDR, 0.5 vs. 0.5, p = 0.34). Quantifiable neuropsychological tests underlining each cognitive domain were compared between PD non-OH and PD + OH. Between-group comparisons did not reveal any significant differences, adjusted for multiple comparisons. When multiple comparisons were not controlled, the K-CWST and the SVLT recognition z-scores were lower in PD + OH than those in PD non-OH (PD non-OH vs. PD + OH: K-CWST, –0.47±0.16 vs. –1.22±0.28, p = 0.02; SVLT-E: Recognition, –0.30±0.18 vs. –1.10±0.31, p = 0.04; Supplementary Table 4).
Between-group differences of cognitive domains
Z-scores of each neuropsychological test are presented as means±standards. Group differences of global cognition were compared using Mann-Whitney U test, as appropriate and the results are shown as median (interquartile range). Between-group disparities of cognitive tests were done by analysis of covariance (ANCOVA), adjusted for age, disease duration, total sum of Unified Parkinson’s Disease Rating Scale (UPDRS), and education years. Multiple comparisons were corrected by Benjamini-Hochberg procedure. Statistical significance was defined as a two-tailed p-value < 0.05. MMSE, Mini-Mental Status Examination; CDR, Clinical Dementia Rating; K-CWST, Korean-Color Word Stroop Test; COWAT, Controlled Oral Word Association Test; K-BNT, Korean-Boston Naming Test; SVLT-E, Seoul Verbal Learning Test-Elderly’s version; RCFT, Rey Complex Figure Test.
DISCUSSION
In de novo early PD, distinct regional perfusion patterns were observed between those with OH and those without OH. Perfusion, estimated by the early-phase 18F-FBB PET imaging, showed that cerebral blood flow was elevated in specific areas in PD patients with OH. The cerebral blood flow was not affected by Aβ accumulation. Between-group similarities of cognitive efficiency presumably indicated that augmented cerebral perfusion in PD + OH might be a compensatory regulation in response to chronic OH.
The prevalence of OH (27.4%) was comparable to that of early PD in another study [1]. The subjects of this study were in a relatively early stage of disease with mild parkinsonism. Low average H/M ratios substantiated the clinical diagnosis [11], and the neurogenic basis of OH was in line with more severe cardiac sympathetic denervation and higher supine systolic BP in PD + OH [25, 26].
Perfusion imaging is an accepted measure of cerebral blood flow [7]. The early-phase of 18F-FBB PET imaging is known to mirror this hemodynamic [5] and correlates well with 18F-deoxyglucose PET [9]. The early-phase 18F-FBB PET uptake implies cerebral flow and metabolism based on flow-metabolic coupling [27], and the perfusion defects of this modality could be interpreted as a reflection of neurodegeneration and/or synaptopathy [5, 29]. Among areas related to cognition and motor behavior (Supplementary Table 1), certain regions in this study were revealed to have elevated perfusion in PD + OH compared to non-OH. This is an unorthodox finding as chronic cerebral hypoperfusion has been associated with metabolic impairment, Aβ formation, functional deficits, and brain atrophy [30, 31]. The physiology of this result could be explained as an independent adaptive response of cerebral autoregulation (CA) to orthostatic challenge in early PD to sustain functions compromised by synaptic derangement [3]. Findings that OH did not influence motor behavior, cognition, or cerebral amyloidosis (late-phase) are supportive of this assumption.
Aβ was suggested as a possible influence on cerebral flow in Alzheimer’s disease [32]. The finding that extracellular amyloid burden alone and its interaction with OH did not impact cerebral perfusion (Supplementary Tables 2 and 3) in early PD, therefore, enhances the argument of isolated CA compensation.
Up-regulated perfusion in PD + OH was interpreted to be a result of synaptic dysfunction but not of cortical degeneration because the impaired noradrenergic neural network by locus coeruleus (LC) degeneration in early PD could explain both synaptopathy [21, 34] and OH [35], ultimately demanding hemodynamic compensation. Interestingly, LC degeneration might explain the impaired attention (Supplementary Table 4) of the subcortical origin [36], in relevance to the compensatory hyperperfused dorsolateral prefrontal, inferior frontal, middle cingulate, and superior/inferior parietal areas. Defect in verbal memory recognition could also be attributed to LC degeneration which is also involved in memory processing [36].
Concomitant amyloidosis in early stage PD and its relevance to motor features have been suggested [4], but the event is seldom associated with non-motor features. Moreover, its prevalence was similar to that in normal controls [37], which renders the significance of its presence in the early stage controversial. In this study, the molecular marker of Aβ in the late-phase could not be associated with dysautonomia. Longitudinal follow up is required to clarify the association.
The strength of this study is that 18F-FBB PET imaging enables consideration of contemporary cerebral perfusion and the influence of amyloid accumulation on its physiology. This research provides further evidence of cerebral autoregulation adaptation in response to chronic OH, within the context of concomitant amyloidosis, in early stage PD.
This study has several limitations. Its sample size and observatory cross-sectional design limit firm conclusions. A total of 73 early PD patients was analyzed, and 60 patients were included in the between-group comparison of cognition. Longitudinal design with a larger sample is required to determine how perfusion, amyloidosis and the relevant clinical functions change as the disease progresses. Secondly, the study did not include comparisons with normal controls which may depreciate the compensatory differences between PD + OH and non-OH. Recent studies found that different endophenotypes existed within PD population and OH was indicated to act as a prognostic factor [38–40]. Within context of such clinical relevance, this work provides additive understanding of neurophysiology of PD subtypes in the early stage. It helps establish the basis why PD + OH projected a different trajectory in longitudinal studies [40] when it was not evident at the early phase in this study. As mentioned above, a longitudinal design with controls is required but current research may be of value in understanding the phenotypic differences in PD.
In conclusion, the results of this study illustrate that elevated cerebral blood flow may be abnormal compensatory elevations in response to the repetitive orthostatic insults to preserve functions in PD + OH. This research elucidates cerebral perfusion physiology in dysautonomic PD with amyloid tracer imaging that enables simultaneous interpretation of the hemodynamics within the context of the molecular pathology.
Footnotes
ACKNOWLEDGMENTS
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning (NRF-2017R1D1A1B06028086) and by the National Research Foundation of Korea (NRF) grant funded by the Korean Government (NRF-2018R1D1A1A02086383). This study was also supported by Research Fund of Seoul St. Mary’s Hospital, The Catholic University of Korea.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.