
Abstract
Background:
Parkinson’s disease (PD), a degenerative disease with irreversible motor dysfunction, impacts patients’ quality of life (QoL). Spirituality can provide a sense of hope and meaning when individuals are faced with adverse life events, such as a diagnosis of PD. However, few studies have examined the relationship between spiritual well-being and QoL for persons with PD.
Objective:
To explore the relationships between the disease characteristics, spirituality and QoL for persons with PD, and verify the mediating effects of spirituality on the relationship.
Methods:
This cross-sectional study recruited patients with PD (n = 110) by convenience sampling from a neurological clinic in northern Taiwan. Variables were measured using the Spirituality Index of Well-Being Chinese version (SIWB-C) and the 39-item Parkinson’s disease Quality of Life Questionnaire Chinese version (PDQ-39-C) self-report questionnaires. Descriptive analysis and linear hierarchical regression were conducted to examine the studied variables and explore the mediating effect of spiritual wellbeing.
Results:
Those whose scores were significantly better in PDQ-39 were younger, employed, with shorter disease duration and less severe condition with better functioning on their early stages and lower LEDD; additionally, those who had better quality of life also experienced better spiritual wellbeing than the counterparts. The regression model demonstrated spiritual self-efficacy had mediating effects between disease characteristics and QoL, explaining 69.8%of the variance (adjusted R2 = 65.3%).
Conclusion:
The results can be the references for future strategies and interventions, focusing on increasing spiritual self-efficacy and reducing the impact of disease severity to improve QoL for persons with PD.
INTRODUCTION
The increase in global aging populations will result in a worldwide doubling of the number of persons with Parkinson’s disease (PD) by 2030, including Asian regions [1, 2]. Compared with Alzheimer’s disease, PD is the second most common neurodegenerative disorder. Although treatments are available for the symptoms of PD, there is no cure for PD, which is a debilitating chronic disease [3] with high medical costs [4]. The average age of PD onset ranges from 55 to 65 years, and compared with many other chronic neurological diseases, the disease trajectory of PD can lead to early retirement, a loss of productivity, and the direct and indirect costs of care can be a significant burden for society and families of persons with PD [5].
Those who are diagnosed with PD face disease-related stresses due to loss of mobility, reductions in activities of daily living (ADLs), and ongoing deterioration in physical and social functions, which significantly impacts their quality of life (QoL) [6]. When an individual with PD attempts to cope with the reality of this debilitating disease, spiritual wellbeing, acting as a buffer, can help mitigate disease-related stresses and provide a source of strength [7, 8]. In other words, spirituality may act as a mediator between disease characteristics as independent variables or predictors and QoL as the dependent variable or outcome for persons with PD. The function of identifying mediators is to examine the effects of predictors on an outcome mediated by various transformation processes internal to the persons with PD [9].
What is spirituality?
Daaleman et al. (2002) suggested spirituality is a dynamic and changeable process, which is highly related to a person’s psychological wellbeing [8]. Dhar et al. (2013) described spirituality as an integrated meaning-giving and purpose-making aspect of human existence, tapping the universal human needs [10]. Spirituality differs from religion or religiosity, in which an individual gains strength from a divine, mystical, or transcendent source, which is incorporated into their daily life [11]. Whereas spirituality is a more subjective experience [12] by focusing on being deeply involved in day-to-day activities in this world, while being detached. In addition, there is a continuous effort for developing universal love, compassion, and equanimity to replace negative emotions such as anger, jealousy, arrogant ego, and hatred. Therefore, individuals can use spirituality to develop one’ abilities to the fullest and even transcending beyond that [10]. Daaleman et al. described two domains of spirituality that were related to subjective well-being for older patients or those with chronic disease: life scheme and self-efficacy [8]. Life scheme is a way that allows individuals to view their world, which provides a sense of order and purpose, while self-efficacy is task specific, which allows an individual to overcome changes in function, both threatening and actual [8]. For individuals with a chronic disease, such as PD, the domains of life scheme and self-efficacy can trigger positive intentionality, allowing an individual to be motivated to recognize resources and actions when facing pressures and dilemmas.
Strong empirical evidence has demonstrated that spirituality is an essential resource for patients during treatment, which can affect QoL [13–15]. With a higher level of spirituality being associated with lower levels of anxiety and depression, the patients can have a better quality of life, fewer non-motor symptoms, reduced palliative symptoms, and less prolonged grief [16]. However, within the trending theoretical framework of successful aging, there is no spiritual dimension [17]. A spirituality index of well-being (SIWB) was, thus, developed as the first step to assess spirituality in an older patient population [8]. Yet, there is little empirical evidence to support the buffering or mediating effect of spiritual well-being on the relationship between disease-related stresses and QoL in persons with PD.
Currently, the availability of national health insurance and implementation of the Long-Term Care Policy, Version 2 (2020) in Taiwan [18], provides multiple resources for persons with PD to maintain or enhance their QoL; however, there are no services available to assess and support spiritual well-being of persons with PD. Given the differences in societal, cultural and health care systems in Western and Asian countries, it is important to examine the relationship between spiritual well-being and QoL of persons with PD in northern Taiwan. Therefore, the purpose of this study was to examine the mediating effects of spiritual well-being on the relationship between PD related stress or disease characteristics and QoL, while controlling for the demographic factors.
We developed a conceptual framework for spiritual well-being and QoL for persons with PD (Fig. 1) based on the spirituality framework of Daaleman et al. [8]. Our framework includes demographics and disease characteristics, spirituality well-being, and QoL for persons with PD. We treated spiritual wellbeing as a mediator for the relationships between disease characteristic related stresses and QoL for those with PD and examined two hypotheses: 1) Disease characteristics and spirituality would be related to QoL for persons with PD, while controlling for demographic factors, and 2) Spiritual wellbeing would mediate the relationship between disease characteristics and QoL for persons with PD.
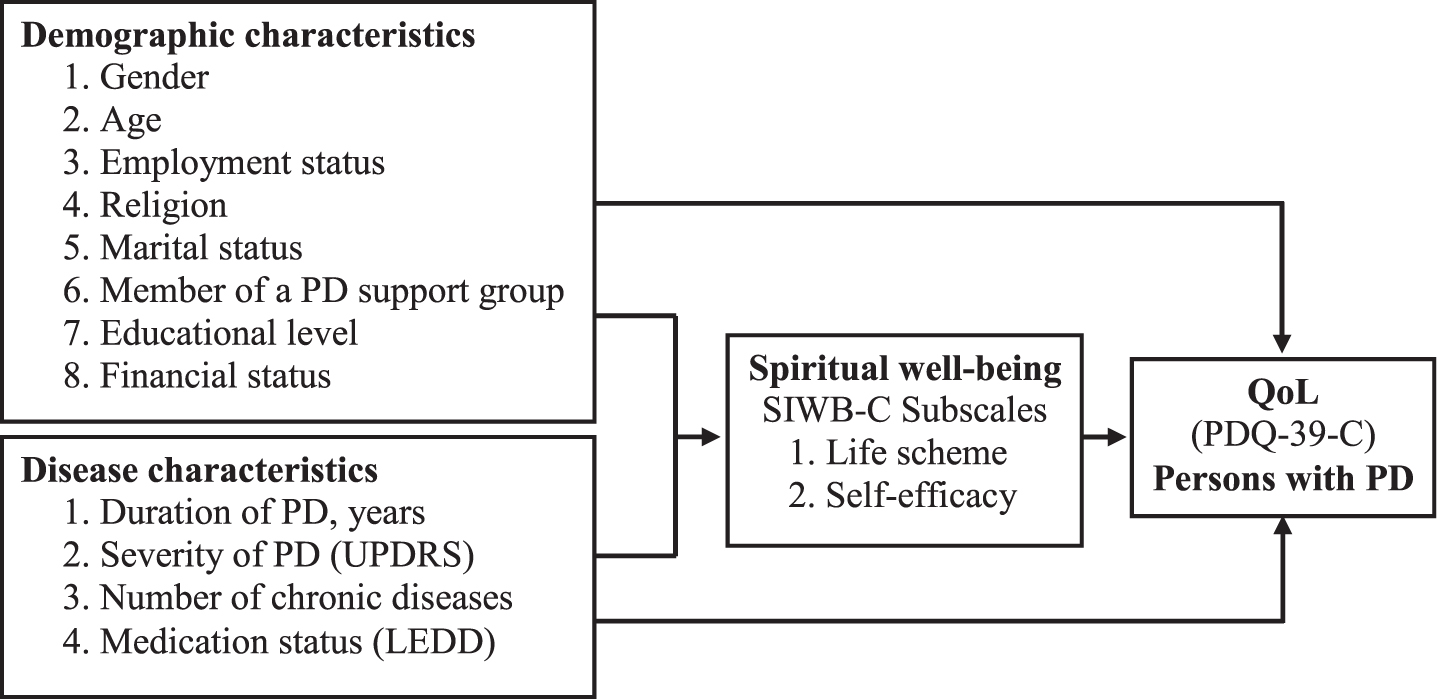
The conceptual framework of the relationship between spiritual well-being and quality of life (QoL) for persons with Parkinson’s disease (PD). UPRDS, Unified Parkinson’s Disease Rating Scale; LEDD, Levodopa equivalent daily dose; SIWB-C, Spirituality Index of Well-Being Scale-Chinese version; PDQ-39-C, Parkinson’s Disease Questionnaire, Chinese version.
MATERIALS AND METHODS
Study design and participants
This cross-sectional design recruited persons with PD by convenience sampling from an out-patient clinic of a neurological department in a teaching hospital in northern Taiwan. Patients meeting the following criteria were eligible to participate: a diagnosis of PD without dementia based on Mini-Mental State Examination (MMSE) scores: cut-off point of ≥16 for those with less than a high school education; ≥24 for those who completed at least high school. Exclusion criteria were secondary Parkinsonism, stroke, brain tumor, or an alternative cause for parkinsonism symptoms. Eligible patients were referred to a research team member who explained the design and purpose of the study. All patients who agreed to participate provided written informed consent. The flowchart for the selection of patients to participate in the study is shown in Fig. 2. The study was approved by the Institutional Review Board of the participating hospital (#201600054B0).
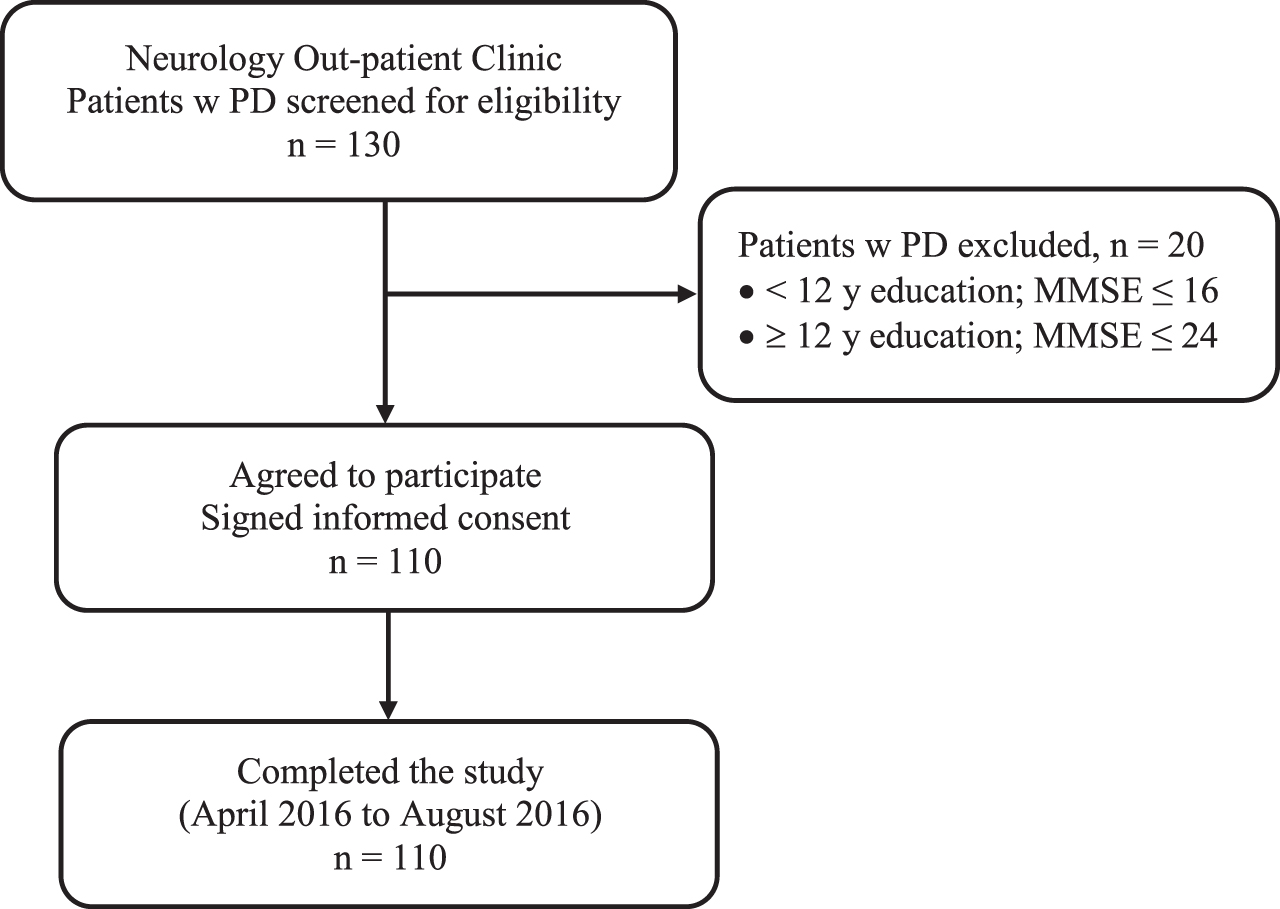
Flowchart for patients with Parkinson’s disease (PD) who participated in the study.
The sample size was estimated using G power software based on the following parameters for linear multiple regression with fixed model to estimate the increase in R2: effect size = 0.15, α=0.05, power = 0.95, two predictors for spirituality (life schema and self-efficacy) and 14 predictors in total. Estimation indicated that 107 participants were required. Therefore, the sample size of 110 participants in our study was sufficient for our analyses.
Questionnaires and assessments
A questionnaire was used to collected demographic characteristics, such as age, gender, and marital status, as well as whether they were a member of a support group, the Parkinson’s Disease Association (yes/no). Data for clinical characteristics were collected from patient’s charts with their permission, including number of comorbidities and duration of PD. The impact of PD on participants was measured by the following scales: severity of PD with the Unified Parkinson’s Disease Rating Scale (UPDRS); stage of PD with the modified Hoehn and Yahr Staging Scale (H&Y scale); and daily activities with the Schwab and England Activities of Daily Living Scale (SE-ADL).
The UPDRS measures the severity and progression of the PD by evaluating four aspects: 1) mentation, behavior, and mood; 2) ADLs; 3) motor function; and 4) complications of therapy in the past week [19]. Patients are evaluated with interviews and clinical observations; higher scores on the UPDRS indicate greater symptom severity.
The modified H&Y staging scale is a 5-point ordinal scale that provides a global assessment of the progression of PD based on clinical findings and functional disability [20]. The modified H&Y staging scale is commonly used to describe the progression of PD by how much of the body is involved for each stage: 1 = unilateral; 1.5 = unilateral and axial; 2 = bilateral without impaired balance; 2.5 = mild bilateral disease with recovery on pull test; 3 = mild to moderate bilateral disease; physically independent; 4 = severe disability; still able to walk or stand unassisted; 5 = wheelchair bound or bedridden unless aided. Martin et al. (1994) reported an internal consistency value as high as Cronbach’s alpha = 0.96 [21].
The SE-ADL estimates the abilities of patients with PD to complete daily activities or chores relative to completely independent and healthy individuals; a score of 100%indicates a completely independent patient, while a score of 0%indicates a completely disabled individual. The convergent validity of the H&Y staging scale with the SE-ADL is high (r = 0.71; p < 0.001) [21]. In this study, clinical data were collected within 3 months from participants’ charts with their permission. Therefore, no Cronbach’s α values were calculated for this study.
The outcome variable of spiritual well-being was measured with the Chinese version of the SIWB (SIWB-C), which was translated and revised by Hsu (2012) [22]. The 12-item SIWB-C consists of two subscales: life scheme, which is having a sense of order and purpose (6 items) and self-efficacy, which is the ability to overcome changes in functioning (6 items). Each item is a negative statement, which is scored on a 5-point Likert scale from 0 (strongly agree) to 4 (strongly disagree), with a midpoint of neither agree nor disagree. The total score ranges from 0 to 48 with higher scores indicating higher levels of spiritual well-being. The Cronbach’s α of the SIWB-C was 0.92, compared with α=0.89 for the original SIWB [22]. In this study, the overall Cronbach’s α was 0.89.
The outcome variable for QoL was measured with the 39-item Parkinson’s Disease Questionnaire (PDQ-39), which is a well-validated instrument for measuring the impact of PD on QoL and daily activities [23]. The PDQ-39 is comprised of eight subscales: mobility (10 items), activities of daily life (6 items), emotional status (6 items), stigma (4 items), social support (4 items), recognition (3 items), communication (3 items) and physical discomfort (3 items). Items are scored on a 5-point Likert scale from 0 –4 : 0 = never, 1 = occasionally, 2 = sometimes, 3 = often, and 4 = always. The total score is expressed as a percentage from 0 to 100, with 0%indicating no impact and 100%the maximum negative impact on QoL. The Cronbach’s α of these subscales ranged from 0.71 to 0.923 [23–25]. We used the Chinese version of the scale, the PDQ-39-C, which was developed by Lin [26] with an overall Cronbach’s α of 0.96. In this study, the overall Cronbach’s α was 0.74.
Statistical analysis
Data were analyzed with SPSS for Windows (Version 22.0). We conducted descriptive statistics (frequency, percentage, mean, and standard deviation [SD]) to describe participants’ demographics, disease characteristics, scores on the SIWB-C and outcome- the variable of PDQ-39-C scores, as well as the rank orders for SIWB-C, and PDQ-39-C item scores. For Hypothesis 1, the relationships between demographic factors, disease characteristics, scores on the SIWB-C and PDQ-39-C were examined by inferential statistics which included t-tests one-way analysis of variance (ANOVA) for discontinuous variables and Pearson Moment Product correlation coefficient analysis for continuous variables. Post-hoc tests following one-way ANOVA were performed with Scheffe’s or Dunnett’s T3 analyses, depending on the Levene test for homogeneity of variance. This allowed us to avoid type I errors which can result from multiple paired comparisons. Finally, we examined Hypothesis 2 by conducting linear hierarchical regression analysis with collinearity diagnostics using the criteria of variance inflation factor (VIF) being higher than 5–10. All linear hierarchical regression analysis results indicated no multicollinearity among independent variables or predictors.
RESULTS
A total of 110 eligible participants with PD agreed to participate in this study. The mean age of participants was 65.75 years (SD = 8.91); slightly more than half were male (58.2%); and 78.2%were married. Participants who received elementary school education or less was 40%, and 55.5%did not participate in any PD support groups. The mean duration of PD was 9.03 years (SD = 7.03), mean UPDRS score for disease severity was 41.65 (SD = 18.89). The mean H&Y staging scale for PD was 1.93 (SD = 1.03), indicating minor unilateral to bilateral symptoms. The mean number of chronic diseases was 1.74 (SD = 1.49). The mean SE-ADL score was 79.36%(SD = 15.22), indicating most participants were able to handle most daily activities independently. The mean LEDD was 705.95 mg (SD = 454.13). Details of demographics and disease characteristics of participants are shown in Table 1.
Demographic and disease characteristics of participants (N = 110)
SD, standard deviation; NTD, New Taiwanese Dollars; UPDRS, Unified Parkinson’s Disease Rating Scale; H&Y scale, modified Hoehn and Yahr Staging Scale; SE-ADL, Schwab and England Activities of Daily Living Scale; LEDD, Levodopa equivalent daily dose.
Scores for the SIWB-C scale are shown in Table 2. The mean total score for spiritual well-being was 29.01 (SD = 6.99), indicating participants had a moderate level of overall spiritual well-being. The mean subscale scores for self-efficacy were 12.49 (SD = 4.09), lower than the mean subscale scores of 16.52 (SD = 3.67) for life scheme. Mean scores for two items of the self-efficacy subscale were identical (mean = 1.78, SD = 1.05) and the lowest of all items: 1) “There is not much I can do to help myself” and 2) “There is no way that I can complete what I have started.” These results highlighted the most declined self-efficacy areas due to PD.
Spirituality Index of Spiritual Wellbeing-Chinese version item scores and rank order of subscales for participants (N = 110)
SD, standard deviation. 1Rank = rank order from 1 (best) to 11 (worst).
The mean scores for participants on the PDQ-39-C are shown in Table 3. The mean summary score was 32.00 (SD = 16.68), indicating participants perceived a mild to moderate impact of PD on overall QoL. The subscale for social support had the lowest mean score (0.58, SD = 1.42), suggesting the persons with PD in our study did not experience a significant impact of their disease on this dimension of QoL. The highest subscale score was mobility (16.47, SD = 10.79), indicating their disease had the greatest negative impact on their mobility.
Mean scores on the 39-item Parkinson’s disease questionnaire for Health-related Quality of Life-Chinese version item scores; rank order of subscales for participants (N = 110)
SD, standard deviation. 1Rank = Rank order from 1 (worst) to 8 (best).
Bivariate analyses explored the relationships among demographic factors, disease characteristics, spirituality measured by scores on the SIWB-C and the outcome of QoL measured by PDQ-39-C. There was a positive association between age and PDQ-39-C (r = 0.25, p < 0.01); the older the persons with PD were, the worse their experiences of overall QoL were. On the other hand, the number of chronic diseases was only associated with the PDQ-39-C subscale scores for recognition (r = 0.23, p < 0.05). With the exception of Stigma, disease characteristics were associated with the total scale scores and the most subscale scores of PDQ-39-C (r ranged from –0.73 to 0.80, p < 0.01), indicating that worse disease characteristics were associated with lower levels of QoL in persons with PD: duration of the disease (r = 0.45, p < 0.01), UPDRS scores for disease severity (r = 0.80, p < 0.01) and SE-ADL scores (r = –0.71, p < 0.01) for daily life activities. The LEDD (mg/day) was significantly and positively associated with PDQ-39-C scores (r = 0.46, p < 0.01), indicating a higher dosage of LEDD was related to higher QoL scores for persons with PD, indicating perceived QoL was poor.
Consequently, there was a significant negative association between the total scores of SIWB-C and the overall PDQ-39-C (r = –0.53, p < 0.01), as well as for the subscales of the SIWB-C, life scheme and self-efficacy (r = –0.38, p < 0.01 and r =&thinsp-0.57, p < 0.01, respectively). These findings suggest persons with PD who had lower levels of spiritual well-being were more likely to experience a lower level of QoL. Life scheme and self-efficacy were negatively associated with the UPDRS for disease severity (r = –0.43, –0.52, respectively, p < 0.01) and were positively associated with functioning of the participants (SE-AD) (r = 0.40, 0.47, respectively, p < 0.01). Finally, self-efficacy was negatively associated with duration of disease (r= –0.31, p < 0.01) and dosage of LEDD (r = –0.38, p < 0.01). In summary, disease characteristics had a negative impact on life scheme and self-efficacy for spiritual well-being in persons with PD. Details of the analysis results are shown in Table 4.
Relationship between variables of age, disease characteristics, and SIWB-C and outcomes for QoL (PDQ-39-C scores) and Spirituality (SWIB-C scores) for persons with PD (N = 110)
PDQ-39-C, 39-item Parkinson’s disease questionnaire-Chinese version; ADL, Activities of Daily Living; SOC, social support; RECOG, recognition; COM, communication, PD, physical discomfort; chronic diseases (n), number of chronic diseases; UPDRS, Unified Parkinson’s Disease Rating Scale; SE-ADL, Schwab and England Activities of Daily Living Scale; LEDD, Levodopa equivalent daily dose; SIWB-C, Spirituality Index of Well-Being Scale-Chinese version; LS, life scheme; SE, self-efficacy; *p < 0.05; **p < 0.01.
We also examined if any discontinuous variables of demographics or stage of PD, assessed with the H&Y scale, were associated with scores on the PDQ-39-C and the two subscales of SIWB-C for persons with PD (Table 5). The results showed that lack of employment negatively impacted PDQ-39-C (t = –4.78, p < 0.01), and positively influenced life scheme (t = 2.19, p < 0.05) and self-efficacy (t = 2.46, p < 0.05). In other words, persons with PD who were unemployed had worse QoL experiences, lower levels of life scheme and self-efficacy than those who were employed. However, being a member of a PD support group was not associated with the PDQ-39-C or SIWB-C subscores, suggesting PD support groups showed no impact on overall QoL and spiritual well-being. Educational levels and marital status were also not associated with total scores on the PDQ-39-C or subscales scores on the SIWB-C. However, the more severe the HY-stage, the higher the mean PDQ-39-C scores, indicating the severity of the disease stages was associated with worse experiences of overall QoL (F = 37.09, p < 0.01). Post hoc analysis by Scheffe’s test showed that mean scores for PDQ-39 among participants at stage 4 to 5 were significantly higher than those at stage 2–2.5; and mean scores for the PDQ-39 among participants at stage 3 were significantly higher than those at stage 0–1.5. Similarly, the later stages, based on the HY-score, were related to lower mean subscale scores on the SIWB-C, indicating later disease stages were associated with worse experiences of life scheme and self-efficacy for spirituality (F = 7.48 and 6.09, respectively, p < 0.01). Post hoc analysis by Scheffe’s test showed that mean subscale scores for life scheme among participants at stage 0 to 1.5 > were significantly higher than those at stage 2–2.5, and those participants had higher scores those at stage 4–5. Subscale scores among participants at stage 3 were significantly higher than those at stage 4–5. Post hoc analysis by Scheffe’s test showed that mean scores for the subscale of self-efficacy among participants at stage 0 to 1.5 were higher than participants at stage 2–2.5, who had higher scores than participants at stage 4–5 (Table 5).
Relationships between discontinuous variables and outcome variables for total score on the PDQ-39-C and subscale scores for life scheme and self-efficacy on the SIWB-C
SD, standard deviation; PDQ-39-C, 39-item Parkinson’s disease questionnaire-Chinese version; SIWB-C, Spirituality Index of Well-Being Scale-Chinese version; QoL, quality of life; ADL, Activities of Daily Living; SOC, social support; COM, communication; PD, physical discomfort; PD group, member of a PD support group; NTD, New Taiwan Dollar; HY-stage, modified Hoehn and Yahr Staging Scale. #Post Hoc Test: Scheffe’s test and Dunnett’s T3 test. *p < 0.05; **p < 0.01.
Variables from the bivariate analyses that were significantly associated with the outcome of scores on the PDQ-39-C in persons with PD were entered into linear hierarchical regression models using the enter method for SPSS regression models (Table 6). In the first step, we entered employment status (yes or no), variables of financial status, and age. Although Model I was significant (F = 3.774, p < 0.05) and explained 15.4%of the variance in scores for PDQ-39-C (adjusted R2 = 11.3%), there were no significant predictors.
Regression analysis for correlations between variables of demographics, disease characteristics, spiritual well-being (scores on the SWIB-C) and quality of life (scores on the PDQ-3) for persons with Parkinson’s disease (N = 110)
β, standardized regression coefficient; NTD, New Taiwanese Dollars; PD, Parkinson’s disease; HY-stage, modified Hoehn and Yahr Staging Scale; UPDRS, Unified Parkinson’s Disease Rating Scale; SE-ADL, Schwab and England Activities of Daily Living Scale; LEDD, Levodopa equivalent daily dose. 1Reference group = no income. 2Reference group = H&Y scale, stage 1.0–1.5. *p < 0.05; **p < 0.01.
In the second step, we entered significant disease characteristics (H&Y stage, UPDRS, SE-ADL, duration of PD, and LEDD) for Model II. Only UPDRS was a significant predictor (β= 0.503, p < 0.01), which increased the explained variance to 51%. The entire Model II explained 66.3%of the PDQ-39-C variance (adjusted R2 = 62.2%, F = 16.908, p < 0.01).
In the third step, we added the subscale scores of the SIBW-C subscores, (life scheme and self-efficacy) for Model III. UPDRS continued to be a significant predictor for the outcome of PDQ-39-C (β= 0.424, p < 0.01); and the subscale scores for self-efficacy were added as a significant predictor (β= –0.246, p < 0.05), with an increase of 3.5%in explained variance. The entire Model III explained 69.8%of the total variance (adjusted R2 = 65.3%; F = 16.230; p < 0.01). Therefore, the Spiritual Well-Being subscale scores of self-efficacy was could alter the relationship between disease characteristics (UPDRS) and PDQ-39-C. However, self-efficacy was not the dominant predictor of PDQ-39-C. Therefore, we determined that self-efficacy was a mediator and partially influenced the relationships between disease characteristics (UPDRS) and PDQ-39-C for persons with PD.
DISCUSSION
In this study, we investigated the relationships between demographic factors, disease characteristics, spirituality and QoL and verified the mediating effect of spirituality in persons with PD at their early stages. Our study was guided by the spirituality framework of Daaleman et al. [8]. The results of our study partially supported the two hypotheses derived from our theoretical framework: 1) When controlling for demographic factors (i.e., age, employment status, financial categories), the disease characteristics of duration of disease, disease severity measured by UPDRS, functioning measured by SE-ADL, and LEDD, we found that spirituality, measured by SIWB-C, were significantly associated with QoL measured by the PDQ-39-C; and 2) Spiritual self-efficacy acted as a significant but partial mediator between disease characteristics of UPDRS and outcomes of PDQ-39-C for persons with PD.
Results from the bivariate analysis indicated if the persons with PD were employed, they reported better QoL than those who were unemployed (t = 4.78, p < 0.001). It has been suggested that a longer duration of illness, high medication costs, unemployment, and a lack of available social services for patients has a negative impact on QoL [28, 29]. However, employment status is not a significant predictor for QoL for participants in our study, while it was significantly associated with spirituality regarding life scheme and self-efficacy. As a result, our findings merit additional research to better understand the meaning and importance of occupation/employment and its relationship with spirituality and QoL in persons with PD.
The subdomain of mobility problems for PDQ-39-C was ranked number 1 by participants, suggesting this have the greatest impact on QoL. Mobility problems also had high correlation coefficients with disease severity (UPDRS) and functioning (SE-ADL) (r = 0.78, –0.73, respectively, p < 0.01). Thus, even at the early disease stages, QoL was significantly impacted by mobility for persons with PD. Mobility problems, observed as bradykinetic gait features, such as reduced trunk rotation, decreased arm swing and slow turns, maybe present in newly diagnosed persons with PD, even when walking speed is normal [27]. A recent study by Johansson et al. (2020) found that persons with PD in their early stages suffered from a decline in mobility measured by the Timed Up and Go Test and Postural Stability Test [27]. The consequences of mobility problems include increased risks of falls and a decline in QoL. Therefore, older adults with PD should be closely monitored if they are experiencing problems with mobility [27].
In Model II, the disease severity measured by the UPDRS score was not only a predictor of QoL in persons with PD, but also the most critical one, accounting for 53.1%of the variance. He et al. (2016) [30] reported the importance of symptoms of PD contributing to quality of life. These symptoms, however, are often treated as outcomes rather than predictors in many clinical trials. In this study, we treated disease severity as one of the predictors for overall quality of life for persons with PD because the concept of QoL widens the horizon of understanding the impact of PD on an individuals’ life. Therefore, clinical treatment and nursing care should be guided by improving or maintaining quality of life based on patient preferences [31–35].
As hypothesized, Model 3 demonstrated self-efficacy, one of the subscales of spiritual well-being, was a significant and partial mediator between disease related stress and quality of life, supported by the results that the values of β (0.503, p < 0.01) between UPDRS and PDQ-39-C in model II was shared by β (–0.246, p < 0.05) between SIWB-C and PDQ-39-C in Model III. Spirituality has been proposed as a mediator, which is a characteristic related to psychological health in the following four ways: it ensures social support and integration within a community, establishes personal relationships with a divine other, promotes a salubrious personal lifestyle that is congruent with a traditional personal faith, and provides systems of meaning and existential coherence. Patients associate spirituality with well-being largely through the provision of meaning systems and coherence. This is especially true for positive intentionality, which shares characteristics with self-efficacy, an individual belief in the capacity to organize and perform activities required for a prescribed goal. Self-efficacy beliefs are domain and task specific; therefore, within the context of overcoming threatened or actual changes to their functioning when suffering from symptoms of PD, patients who report high self-efficacy beliefs regarding their functioning and who view their lives as purposeful and meaningful, scored higher on measures of subjective well-being than those who do not hold such beliefs or attitudes [8]. This may explain why self-efficacy of spiritual well-being mediated interference of the effects of symptoms of PD, which then positively impacted QoL. However, self-efficacy is not a dominant mediator for quality of life experienced by persons with PD. It is possible that some important variables may be left out. Future research should include mixed methods for the collection of qualitative and quantitative data to explore the cultural influence on illness and spiritual experiences of persons with PD and how these experiences are related to their quality of life.
There was no significant effect of gender on QoL for persons with PD, which is supported by the findings of Lawrence et al. [36] and Moreira et al. [33]. Moreover, in contrast to a previous study [6], we found no evidence that marital status was associated with QoL in persons with PD. More details need to be explored in this regard, such as examining the quality of the marriage, rather than marital status. Finally, no significant differences were found in QoL and spirituality between those with and without religious beliefs. Nevertheless, there was a negatively correlated relationship between the two subscales for spiritual wellbeing: life scheme and self-efficacy, and QoL. It indicated that a higher level of spiritual wellbeing is associated with better QoL in persons with PD. These results supported the notion that religion and spirituality are two different concepts. Further research is required to understand how nurses can use spirituality as a resource to assist persons with PD to cope with disease related stresses and to maintain or improve their quality of life.
Limitations, strengths, and summary
There were three limitations in this study. First, a cross-sectional study design prevents analysis of causal relationships between spiritual wellbeing and QoL for persons with PD. However, this study was guided by a theoretical framework and the results were verified and supported by empirical evidence. Therefore, future longitudinal studies will be conducted to monitor symptom changes and trajectories, spiritual wellbeing and QoL for persons with PD. In addition, a qualitative approach can be applied to fully understand the cultural influence on illness and spiritual experiences of persons with PD, including spiritual distress or religious struggles, such as being punished by God or psychosocial strains due to failing to live up to high religious standards [37]. Some individuals with PD often become increasingly involved in spiritual activities as an escape from dealing with family problems, or delay diagnosis and even refuse medical treatments due to religious beliefs [37]. Therefore, both objective and subjective reports that include positive and negative effects of spirituality or religion should be included in future studies. Second, studies have found that lateralization in persons with PD impacts spiritual acceptance and spiritual wellbeing [7]. Although we did not collect the brain imaging data in this study, future research directions could include lateralization of PD or comparison of pre-and-post surgical treatment of PD and levels of spiritual well-being [7] while controlling for religious distress or other negative effects of spirituality [37]. Third, the effects of participating in disease associations were different from previous reports [38]. A more detailed investigation combining qualitative interviews may reveal the inner experiences of persons with PD who attend or not attend the PD associations or other support groups. Our study recruited persons with PD in their early stages, while similar approaches have been applied in a study which focused on PD persons in their late stages [38]. This study found that enhanced spirituality was associated with reduced anxiety and depression [38]. Therefore, spirituality could be a possible coping resource for persons with PD in their late stages to deal with prolonged grief and non-motor symptoms [38]. Future research can recruit persons with PD in both early and late stages and deeply examine the complex relationships between positive and negative aspects of spirituality, brain imaging and palliative care as well as quality of life in these populations.
Despite above mentioned limitations, the findings of our study support the use of the conceptual framework derived from the spirituality framework of Daaleman et al. [8] and partially validate our hypotheses. Our results contribute to the understanding of spiritual wellbeing and its relationships with quality of life in persons with PD in northern Taiwan. These relationships have important clinical applications for assessing the spiritual needs of persons with PD, assisting health professionals in the development of spiritual related interventions, and improving the quality of patient care. Our research outcomes can also be a reference for providing education and training courses to health professional students and healthcare professionals on assessing spiritual needs and providing spiritual care for persons with PD and evaluate the broaden outcomes such as quality of life.
Footnotes
ACKNOWLEDGMENTS
We thank all patients who participated in this research. We are grateful to all who provided support and assistance for this study.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.