
Abstract
BACKGROUND:
Near-miss analysis is an effective method for preventing serious adverse events, including never events such as wrong-site surgery.
OBJECTIVE:
To analyze all near-miss incidents reported in a large general hospital in southern Brazil between January 2013 and August 2017.
METHOD:
We performed a descriptive retrospective study of near-miss incidents recorded in the hospital’s electronic reporting system in a large non-profit hospital (497 beds). The results are expressed as absolute (n) and relative frequencies (%). Pearson’s chi-square test, Fisher’s exact test (Monte Carlo simulation) and linear regression were used.
RESULTS:
A total of 12,939 near-miss incidents were recorded during the study period, with linear growth in the number of reports. Near-miss incidents were most frequent for medication, followed by processes unspecified in the International Classification for Patient Safety framework, followed by information control (patient chart and fluid balance data), followed by venous/vascular puncture. The highest prevalence of reports was observed in inpatient wards, in adult, pediatric, and neonatal intensive care units, and in the surgical center/post-anesthesia care unit. Pharmacists and nursing personnel recorded most of the reports during the day shift.
CONCLUSION:
The most frequent categories of near-miss incidents were medication processes, other institutional protocols, information control issues, and venous/vascular puncture. The significant number of reported near-miss incidents reflects good adherence to the reporting system.
Introduction
Health care organizations worldwide advocate the use of patient incident reporting systems to support safety practices and programs, a strategy adapted from high-reliability organizations, such as air traffic control centers and nuclear power plants, in which operation is nearly error-free despite the potential for catastrophic failure [1,2]. In these industries, near-miss analysis is systematically performed to mitigate risk and improve safety [3].
In aviation, a major incident is frequently followed up by simulating the causes and adding them to training processes. In addition, equipment design, procedures, and training are often revised to reflect what has been learned. However, a gap remains in healthcare between error occurrence/reporting and the materialization of learning, since few strategies focus on implementing the necessary changes to prevent error recurrence [3].
A patient safety incident is defined as any event or circumstance that could have resulted, or did result, in unnecessary harm to a patient [4]. Thus, a near-miss incident is an incident that did not cause harm only because the error was detected and corrected prior to reaching the patient [4]. Therefore, near-miss analysis could be highly effective in preventing never events such as wrong-site surgery [5].
However, incident detection is not a simple matter. The literature describes two broad strategies that can be used to track early signs of error. The first relies on collective intelligence for detecting and reporting problems, while the second involves ubiquitous technology, such as airplane black boxes that automatically monitor and identify uncommon events. Some of such technologies have already been tested in surgical centers [6,7]. Both approaches are complex and difficult to implement, since they depend on a culture of safety in which professionals are unafraid to report error [7]. Organizational learning, no punitive response to error, and teamwork within units have also been described as contributing factors to a culture of safety and incident reporting [8–10]. Although there is consensus in the literature about the benefits of such a culture, many healthcare institutions have not been able to achieve it [11].
Learning from patient safety incidents is a crucial step toward developing mechanisms and processes that can prevent similar events and contribute to a culture of safety.
No information is available regarding near-miss incidents in Brazilian hospitals. Therefore, we deemed it important, as a first step, to focus on our own workplace, a hospital with an electronic reporting system (implemented in 2013). Thus, the aim of this study was to analyze all near-miss incidents reported from January 2013 to August 2017 in a large general hospital in southern Brazil.
Method
A descriptive, retrospective study was performed at Hospital Moinhos de Vento (HMV), a large non-profit hospital (497 beds) in southern Brazil (Fig. 1). The study was approved by the HMV Research Ethics Committee (CAAE: 57679316.9.0000.5330, approval report 1.833.572).
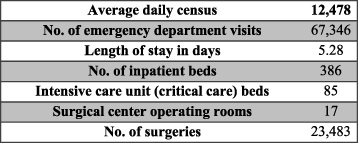
Characteristics of Hospital Moinhos de Vento, 2018.
In 2013, HMV implemented a commercially available Hospital Information System, which was developed in Brazil by a specialized information technology company. This system is used in similar hospitals throughout Brazil and features a set of default tools, including an area for near-miss reporting. All types of near-miss incidents can be reported, and a predefined list of events is also provided. In its first year of operation at HMV, near-miss reporting was introduced only to pharmacy staff. In the following years, as an iterative process, all hospital staff were trained to perform an anonymous incident report. These instructions were routinely reviewed in subsequent years by department heads and their staff, along with a number of other patient safety initiatives. The purpose of such initiatives was to foster a culture of safety and improve overall quality of care and patient outcomes.
Health care in hospital settings involves multiple encounters with the patient and a variety of procedures, such as drug preparation and administration, tests, wound dressings, tube placement, venous puncture, glucose testing, fall prevention, and recording information on the patient’s chart. In the HMV system, safety incidents that could have but did not result in unnecessary harm to the patient are classified as patient-care related near misses. The types and categories of incidents recorded in the system were determined according to the International Classification for Patient Safety framework [12].
Retrospective review of near-miss incidents
The HMV Office of Risk Management routinely reviews all reported incidents as a routine safety practice. According to the severity of the incident, specific safety strategies are implemented to improve work processes to help prevent new events, in particular adverse events and serious adverse events.
To help foster a culture of safety, the hospital has also implemented strategies such as the Green Cross method to encourage near-miss reporting. This method, which originated in the manufacturing industry, has been adapted for use in health care environments to recognize risk and prevent avoidable injury in real time on a daily basis. At HMV, it is used as a quality improvement action as part of the Productive Ward Program [13,14].
In practical terms, the method is a calendar that displays the days of the month in the format of a cross. Each day is divided into three parts corresponding to work shifts. At the end of each shift, the team colors the portion corresponding to their shift: red if a serious adverse event occurred, orange if an adverse event occurred, yellow if a near miss occurred, and green if no incidents occurred. This tool provides a basis for the systematic daily implementation of safety improvement actions suggested by team members and strengthens the institution’s safety culture.
Data collection and analysis
Data collection was performed on 25 August 2017 by the authors (with support from the information technology staff), who extracted the electronic data and generated Microsoft Excel spreadsheets.
The inclusion criteria were near-miss incidents related to medication and patient care processes recorded between 1 January 2013 and 24 August 2017. Data was collected on the following variables: type of near miss, year of event, professional category of the individual who reported it, shift, and hospital ward.
Types of near misses included non-compliance with institutional protocols for procedures, such as standards of care or guidelines regarding: venous/vascular access, sterile materials, communication, fall prevention/restraint measures, wound dressing, drains/tubes, gas therapy, glucose testing, hygiene/comfort, patient identification, isolation precautions, maintenance, miscellaneous materials, other (i.e., related to institutional protocols but not clearly specified in the International Classification for Patient Safety framework [12]), information control (i.e., erroneous or missing data in spreadsheets or patient charts, including fluid balance), vital signs/thermotherapy, and medication processes.
SPSS 20.0 (SPSS Inc., Chicago, IL, USA, 2010) was used for all analyses. The results were expressed as absolute (n) and relative frequencies (%). Pearson’s chi-square test, Fisher’s exact test (Monte Carlo simulation) and linear regression were used to analyze the relationship between the number of near misses and the year, as well as the shift, professional category, and sector of the worker who filed the report. Statistical significance was set at 5% (𝛼 = 0.05).
Results
We analyzed 12,939 near-miss incidents recorded in the HMV reporting system between 1 January 2013 and 24 August 2017. Most reports refer to medication processes, (50.5%, n = 6,537), followed by other institutional protocols (18.7%, n = 2,418), information control (6.0%, n = 775), venous/vascular access (5.1%, n = 662), patient identification (3.7%, n = 480), and miscellaneous materials (3.5%, n = 450) (Table 1).
Distribution of near miss incidents according to year of report
Distribution of near miss incidents according to year of report
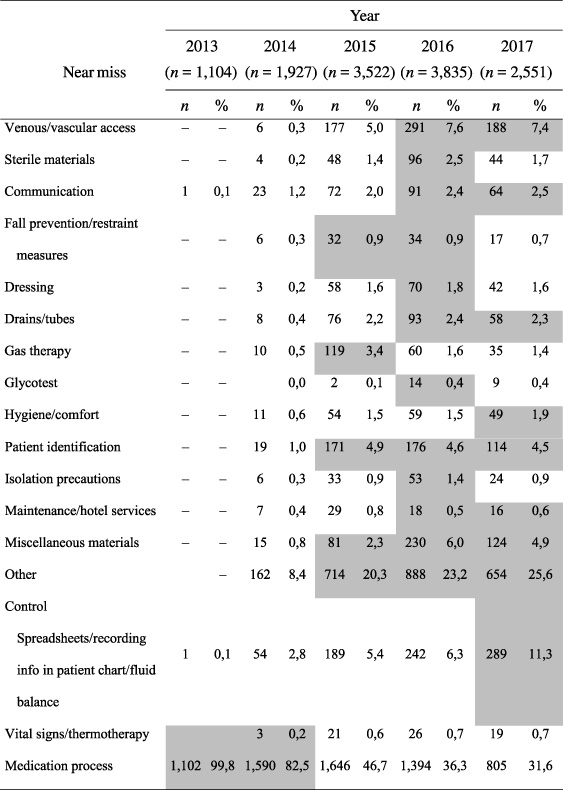
Shaded cells indicate statistical association between year and number of near miss incidents reported during the year. Fisher’s chi square test; (p < 0.001).
A significant association was detected between the type of near-miss incident and the year of occurrence (p < 0.001): 2013 and 2014 were significantly associated with medication processes, while 2015 was associated with fall prevention, miscellaneous materials, other institutional protocols, gas therapy, and patient identification (Table 1).
There was a growth trend in reporting frequency between 2013 (n = 1,104) and 2016 (n = 3,835). Simple linear regression was used to estimate the number of occurrences for the final quarter of 2017 based on the actual data recorded until 24 August 2017. The results suggest that the growth trend in reporting frequency will continue (Fig. 2).

Number of near miss incidents recorded from 2013 to 2017 at HMV.
The most frequently reported near-miss incident type was medication processes (50.5%, n = 6,537). Of these, 86.6% (n = 5,661) were related to medical prescriptions, which encompasses all errors made by a physician during the prescription phase, followed by dose (3.6%, n = 234), medication type (3.3%,n = 217), schedule (2.7%, n = 179), and checking (1.9%, n = 126) (Fig. 3). Incidents regarding dose, type, schedule, and checking involved the nursing staff and were detected prior to reaching the patient.
According to hospital wards, the highest frequency of reported near-miss incidents occurred in the inpatient wards (48.1%, n = 6,229), followed by the Intensive Care Unit (ICU), the Pediatric Intensive Care Unit (PICU) and the Neonatal Intensive Care Unit (NICU) (15.3%, n = 1,991), followed by the Dialysis/Oncology and Emergency Department (12.8%, n = 1,667) (Table 2).
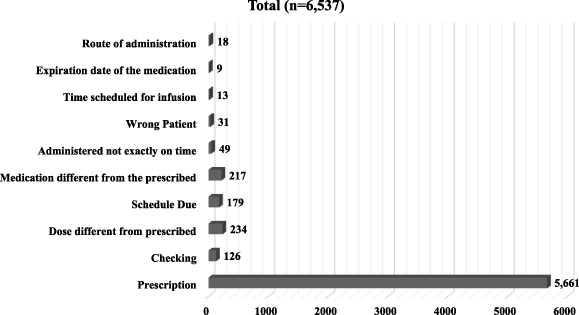
Distribution of near misses related to the medication process.
Distribution of near misses according to hospital sector
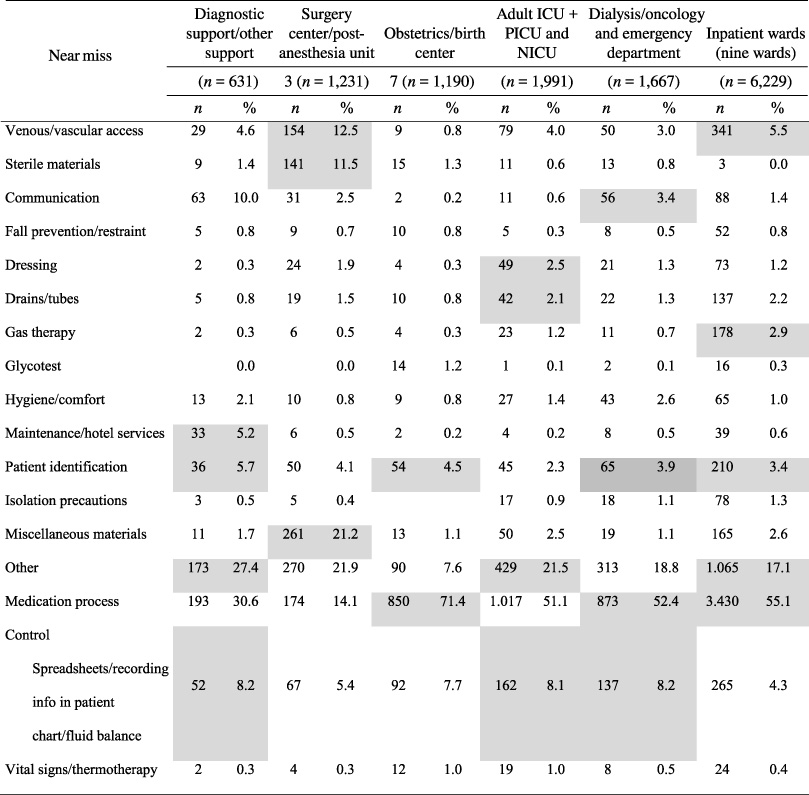
Shaded cells indicate statistical association between hospital sector and number of near miss incidents reported. Fisher’s exact chi-square test (p < 0.001).
Most near misses were reported during the day shift (58.9%, n = 7,624). In terms of occupation, the highest number of near-miss incidents were reported by dieticians, physical therapists, and pharmacists (37.1%, n = 4,797), followed by nurses (29.1%, n = 3,766) and nursing technicians (19.8%, n = 2,562) (Fig. 4).
A significant association (p < 0.0001) was observed between being a nurse and reporting the following type of incidents: venous/vascular access (8.8%, n = 330), information control (8.4%, n = 317), sterile materials (2.7%, n = 103), communication (2.6%, n = 97), and drains/tubes (2.9%, n = 109). An association was also observed between being a pharmacist and reporting incidents related to medication processes (99.3%, n = 4,765).
Analyzing near-miss incidents provides an opportunity to improve processes and routines, developing safer practices by detecting and preventing situations that can cause serious harm. However, little is known about how health care professionals perceive the reporting and analysis of near-miss incidents in their daily practice [15–17]. There is also evidence that professionals tend to correct near-miss incidents as soon as they are perceived (quick fixes) without further action – which is a loss in terms of organizational learning [15–18]. This explains, at least to a certain extent, the scarcity of Brazilian publications on this theme.
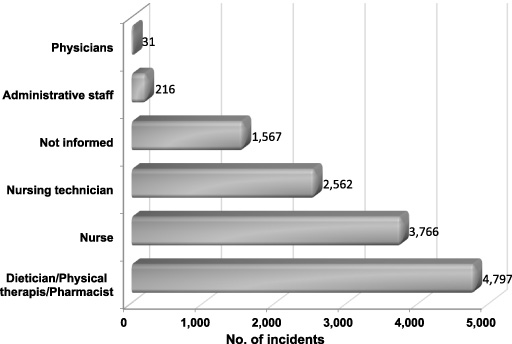
Absolute number of near miss incidents according to occupation.
Our study describes the type and frequency of near-miss incidents reported in a large Brazilian hospital. The steady growth in the number of events reported since implementation of the reporting system shows a trend, which is an expected effect of the visual method used to encourage the reporting of near misses. According to the literature, incident reporting can be a powerful tool for developing and maintaining risk awareness in health care practice [19]. Increased incident reporting may be a result of organizational efforts to develop a culture of safety. Indeed, our results agree with a National Health System Report that the number of incidents reported to the National Reporting and Learning System has continued to increase since the incident report system was implemented in October 2003 [20]. Previous experience from other industries has shown that as an organizational culture matures, the staff become more likely to report incidents. Thus, an increase in incident reporting should not be understood as an indication of patient safety failures, but rather of increased awareness of safety issues among workers and a sign of a more open and transparent organizational culture [20,21]. In other words, staff adherence to reporting tools and processes depends directly on how familiar they are with such processes, their acceptance of best safety practices, and on how comfortable they feel with reporting incidents [22,23]. The results we describe reflect HMV’s efforts to advance organizational learning. HMV was the first hospital in southern Brazil to be accredited by the Joint Commission International (2002).
The most frequent type of near-miss incident observed in this study involved medication processes. Most of these events were detected by pharmacists when reviewing electronic prescriptions, which indicates that reviewing physician prescriptions is a routine part of the work of pharmacists. This is consistent with the results of other studies in hospital settings that identified medication-related incidents as the second most important source of safety events [24,25]. An electronic prescription system is used at HMV, and paper prescriptions are no longer accepted, which is not always the case in other hospitals [26,27]. Medication management has important consequences for patient outcomes [28]. Measures such as daily prescription review by pharmacists, including communication with physicians for clarification, have been described in the literature as an important step in promoting patient safety [29].
At HMV, near-miss incidents can be reported by any hospital worker, regardless of occupation. The sole purpose of analyzing these safety incidents is to plan and implement improvements. Reports, such as never event cases, are discussed in monthly management committee meetings by hospital leadership to define priorities or in weekly risk management meetings with inpatient ward managers. Incidents are not necessarily discussed on the same day they occur. In inpatient wards, teams are directly involved in proposing interventions, implementing safety actions, and developing educational activities for the staff, including guidance for physicians about prescription problems. These teams also define mandatory changes in electronic prescription software when necessary.
Analyses of near-miss incidents in each sector revealed some significant associations. For example, incidents related to venous/vascular access, as well as to sterile material, were significantly more frequent in the surgical center and post-anesthesia care unit, whereas fluid balance-related incidents were significantly associated with ICUs and the dialysis unit. Therefore, the reported incident types reflected the procedures performed in each sector. This suggests that critical analysis of near-miss incidents may be useful for developing customized strategies for specific hospital sectors. It should also be pointed out that the majority of near-miss incidents are job-specific, i.e., to nurses, pharmacists or physicians. This could explain the association we found between ICUs and reports of fluid balance incidents, while other analyses showed that near-miss incidents identified by anesthesia providers in ICUs were more likely to be associated with airway management [30].
As described in other Brazilian studies, the highest prevalence of reports was observed in inpatient wards, in the ICU, PICU and NICU, and in surgical center/post-anesthesia care units [25–29]. This could be explained by the higher number of procedures and patients admitted to these units vs. other sectors, as well as to the large number of prescriptions made on a daily basis in these areas. It should be noted analyzing near-miss incidents in these sectors is very important for establishing prevention strategies, since the occurrence of preventable serious adverse events is still common [29–33].
We observed that most near-miss incidents were reported during the day shift. Reporting more than doubled during the four-year study period, and the proportion of medication-related incidents decreased >60%. This reflects aspects such as pharmacist review of prescriptions during the day shift and the fact that incident report training was first implemented in the pharmacy sector. Moreover, night shift workers have less interaction with patients and, thus, fewer opportunities for near-miss incidents. In addition, the electronic prescription system was adjusted to decrease medical errors and prescription phase near-miss incidents, such as duplicate prescriptions for the same patient.
The low adherence of night shift workers to the reporting system could be related to a lack of training programs for them. Thus, we argue that specific strategies are needed to improve night shift worker awareness of the need to report near-miss incidents. In general, night shift workers have less contact with leadership and do not always engage in continuing education programs [34]. Night shift staff also frequently complain of feeling slighted regarding education: they frequently ask to come in early or stay late to participate in educational programs. However, they would prefer specific programs during their work hours. Thus, commitment to and innovation in learning opportunities for night shift workers are a necessity.
It is also worth pointing out that most of the reports were made by pharmacists, nurses, and nursing technicians. These data agree with a previous study, which reported that physicians are the least engaged staff in error reporting, perhaps for fear of legal disputes or professional embarrassment [23]. A systematic review has shown that, among nurses, the main barriers to reporting are organizational, such as organizational culture and type of reporting system [22]. Personal barriers, such as fear of being held responsible still exist. To overcome these obstacles, it is important to implement anonymous, easy-to-use reporting systems that are effective and efficient, as well as to promote a positive attitude in managers and leaders, who should support workers and provide continuing education and feedback. Additionally, near-miss incident reports can be measured quantitatively and provide qualitative data about less evident processes and rationalizations across a range of procedures and settings. These insights provide opportunities to learn about the cause of incidents and support decision-making to prevent their recurrence.
A final strategy for improving practice is to establish risk management processes and initiatives of adequate quality. Every facility should promote a culture of safety that encourages discussing errors and near-miss incidents in a nonpunitive manner. In doing so, effective solutions for specific systems can be identified and implemented.
As a final thought, we argue that near-miss incidents are difficult to research because classification can be subjective. Perceptions about patient danger may change over time and with repeated exposure to hazardous circumstances [35]. In other words, recognition of and experience with near-miss incidents involves a normalization process. Human judgement and hesitation may also play a role in individual decision-making about what is considered a near miss and about the need to report it.
Classifying some near-miss incidents into a general category (“other institutional protocols”) is a limitation, since there was no in-depth analysis of these items. However, we believe the present results were not affected by this limitation due to the large number of events involved, which provided a good overall picture of the phenomenon. It should also be pointed out that the study was performed in an institution with specific characteristics, e.g. being one of only five hospitals in Brazil classified as “excellent” by the Ministry of Health. Thus, the present findings cannot be generalized to all national contexts. Additional research should be conducted in various hospital settings to facilitate strategies to prevent patient harm.
Conclusions
We analyzed 12,939 near-miss incidents reported in a general hospital from 1 January 2013 to 24 August 2017. We observed a linear increase in the number of notifications during the study period. The highest prevalence of reports was observed in inpatient wards, in the ICU, the PICU and the NICU, and in surgical center/post-anesthesia care unit. Pharmacists and nursing personnel made most of the reports during the day shift.
The frequency of reported near-miss incidents was highest for medication processes, followed by “other institutional processes” (i.e., unspecified the International Classification for Patient Safety framework), followed by information control in patient charts/fluid balance, followed by venous/vascular puncture.
The high number of near-miss incident reports reflects good staff adherence to the reporting system. We argue that improving safety culture is not necessarily an antecedent to or a consequence of incident reporting. Rather, there is a dynamic relationship that contributes to the establishment of a safety culture with emphasis on organizational learning. In addition, the safety culture (or more specifically, the safety climate) was not evaluated in this study and could be considered in further research. The present findings also suggest the current existence of an environment in which professionals feel comfortable discussing safety incidents, and where they are engaged in designing and implementing strategies to improve safety based on reports of near-miss incidents.
Footnotes
Conflict of interest
None to report.